Effects of Elastic Resistance Exercise on Postoperative Outcomes Linked to the ICF Core Sets for Osteoarthritis after Total Knee Replacement in Overweight and Obese Older Women with Sarcopenia Risk: A Randomized Controlled Trial


Abstract
:1. Introduction
2. Methods
2.1. Ethics Approval and Study Design
2.2. Participants
2.3. Sample Size Estimation
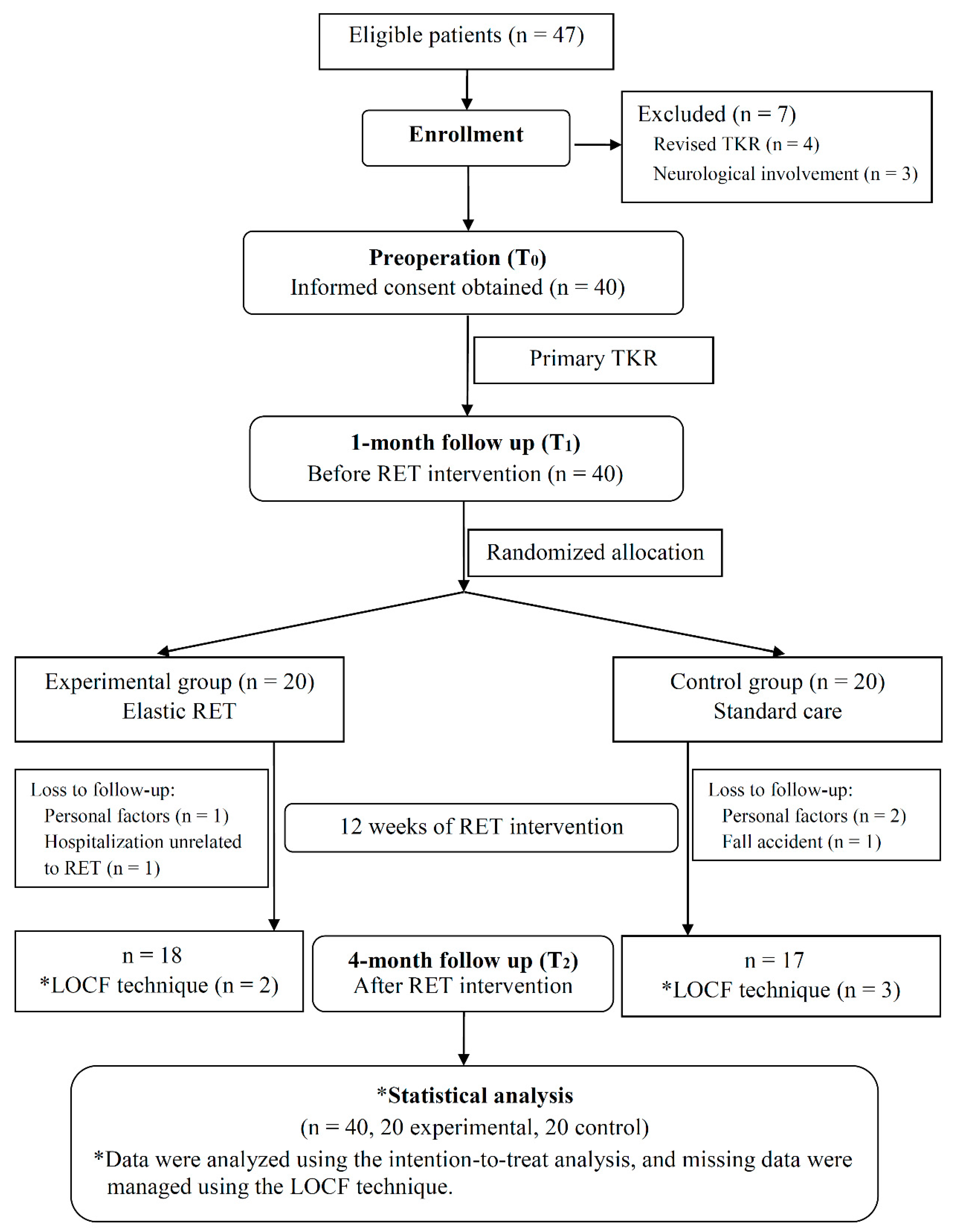
2.4. Randomization
2.5. Interventions
2.5.1. Inpatient Rehabilitation
2.5.2. Elastic Resistance Exercise
2.5.3. Standard Care
2.6. Outcome Measures
2.6.1. Primary Outcome Measures
2.6.2. Secondary Outcome Measures
2.7. Statistical Analysis
3. Results
3.1. Patient Demographics and Clinical Characteristics
3.2. Effects of Elastic RET on Muscle Mass
3.3. Effects on Pain, ROM, Physical Capacity, and WOMAC Outcomes
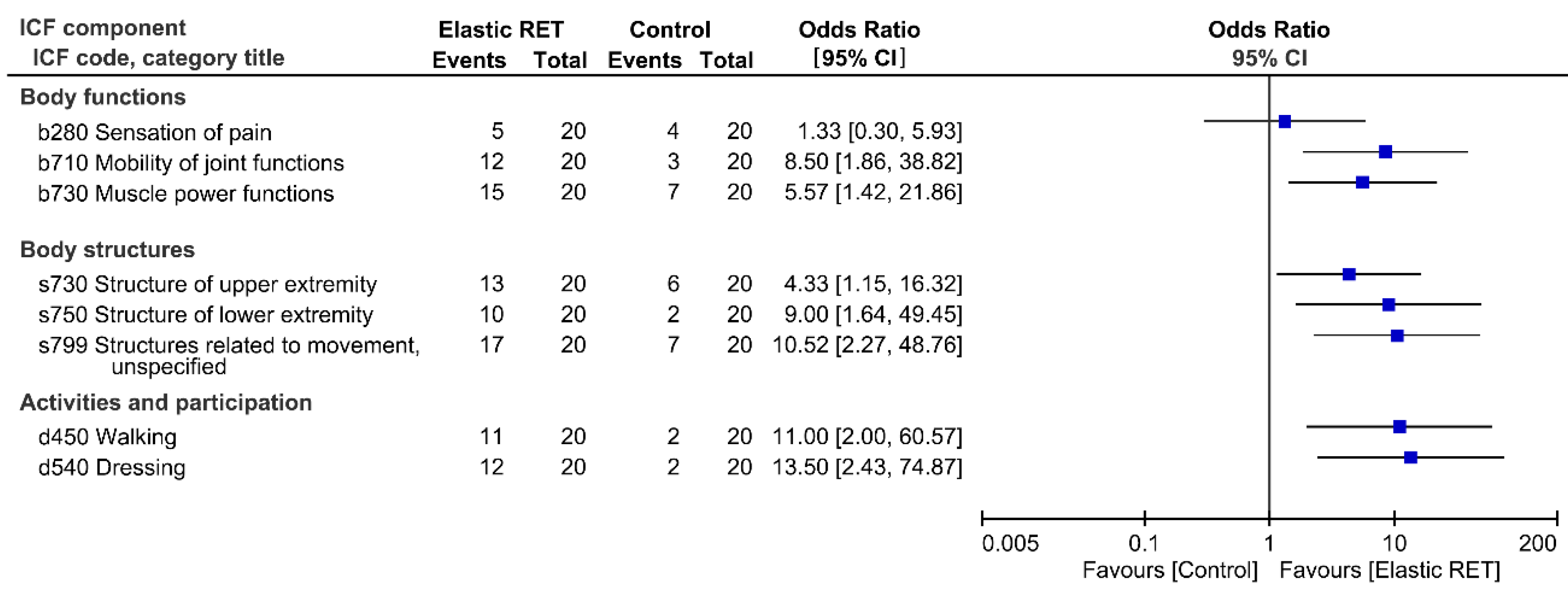
3.4. Results of Function and Disability Based on the Brief-ICF-OA
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bennell, K.L.; Wrigley, T.V.; Hunt, M.A.; Lim, B.W.; Hinman, R.S. Update on the role of muscle in the genesis and management of knee osteoarthritis. Rheum. Dis. Clin. N. Am. 2013, 39, 145–176. [Google Scholar] [CrossRef] [PubMed]
- Masiero, S.; Vittadini, F.; Ferroni, C.; Bosco, A.; Serra, R.; Frigo, A.C.; Frizziero, A. The role of thermal balneotherapy in the treatment of obese patient with knee osteoarthritis. Int. J. Biometeorol. 2018, 62, 243–252. [Google Scholar] [CrossRef]
- Hsu, H.; Siwiec, R.M. Knee Osteoarthritis; StatPearls, Ed.; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2019. [Google Scholar]
- Lee, S.; Kim, T.N.; Kim, S.H. Sarcopenic obesity is more closely associated with knee osteoarthritis than is nonsarcopenic obesity: A cross-sectional study. Arthritis. Rheum. 2012, 64, 3947–3954. [Google Scholar] [CrossRef]
- Papalia, R.; Zampogna, B.; Torre, G.; Lanotte, A.; Vasta, S.; Albo, E.; Tecame, A.; Denaro, V. Sarcopenia and its relationship with osteoarthritis: Risk factor or direct consequence? Musculoskelet Surg. 2014, 98, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Toda, Y.; Segal, N.; Toda, T.; Kato, A.; Toda, F. A decline in lower extremity lean body mass per body weight is characteristic of women with early phase osteoarthritis of the knee. J. Rheumatol. 2000, 27, 2449–2454. [Google Scholar]
- Lee, S.Y.; Ro, H.J.; Chung, S.G.; Kang, S.H.; Seo, K.M.; Kim, D.K. Low Skeletal Muscle Mass in the Lower Limbs Is Independently Associated to Knee Osteoarthritis. PLoS ONE 2016, 11, e0166385. [Google Scholar] [CrossRef] [PubMed]
- Welch, C.; Hassan-Smith, Z.K.; Greig, C.A.; Lord, J.M.; Jackson, T.A. Acute Sarcopenia Secondary to Hospitalisation—An Emerging Condition Affecting Older Adults. Aging Dis. 2018, 9, 151–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verdijk, L.B.; Gleeson, B.G.; Jonkers, R.A.; Meijer, K.; Savelberg, H.H.; Dendale, P.; van Loon, L.J. Skeletal muscle hypertrophy following resistance training is accompanied by a fiber type-specific increase in satellite cell content in elderly men. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Arai, H.; Kritchevsky, S.B.; Guralnik, J.; Bauer, J.M.; Pahor, M.; Clark, B.C.; Cesari, M.; et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef] [PubMed]
- Waller, B.; Munukka, M.; Rantalainen, T.; Lammentausta, E.; Nieminen, M.T.; Kiviranta, I.; Kautiainen, H.; Häkkinen, A.; Kujala, U.M.; Heinonen, A. Effects of high intensity resistance aquatic training on body composition and walking speed in women with mild knee osteoarthritis: A 4-month RCT with 12-month follow-up. Osteoarthr. Cartil. 2017, 25, 1238–1246. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.Y.; Tchai, E.; Jang, S.N. Effectiveness of aquatic exercise for obese patients with knee osteoarthritis: A randomized controlled trial. PM R 2010, 2, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Toda, Y. The effect of energy restriction, walking, and exercise on lower extremity lean body mass in obese women with osteoarthritis of the knee. J. Orthop. Sci. 2001, 6, 148–154. [Google Scholar] [CrossRef]
- Franzke, B.; Halper, B.; Hofmann, M.; Oesen, S.; Pierson, B.; Cremer, A.; Bacher, E.; Fuchs, B.; Baierl, A.; Tosevska, A.; et al. The effect of six months of elastic band resistance training, nutritional supplementation or cognitive training on chromosomal damage in institutionalized elderly. Exp. Gerontol. 2015, 65, 16–22. [Google Scholar] [CrossRef]
- Liao, C.D.; Tsauo, J.Y.; Huang, S.W.; Ku, J.W.; Hsiao, D.J.; Liou, T.H. Effects of elastic band exercise on lean mass and physical capacity in older women with sarcopenic obesity: A randomized controlled trial. Sci. Rep. 2018, 8, 2317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiebaud, R.S.; Funk, M.D.; Abe, T. Home-based resistance training for older adults: A systematic review. Geriatr. Gerontol. Int. 2014, 14, 750–757. [Google Scholar] [CrossRef]
- Chou, L.N.; Chen, M.L. Effects of Elastic Band Exercise on Lower Limb Rehabilitation of Elderly Patients Undergoing Total Knee Arthroplasty. Rehabil. Nurs. 2019, 44, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Bade, M.J.; Stevens-Lapsley, J.E. Restoration of physical function in patients following total knee arthroplasty: An update on rehabilitation practices. Curr. Opin. Rheumatol. 2012, 24, 208–214. [Google Scholar] [CrossRef]
- Barrois, B.; Ribinik, P.; Gougeon, F.; Rannou, F.; Revel, M. What is the role of the physical medicine and rehabilitation unit after total knee arthroplasty? Clinical practice recommendations. Ann. Readapt. Med. Phys. 2007, 50, 724–728, 729–733. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. How to Use the ICF: A Practical Manual for Using the International Classification of Functioning, Disability and Health (ICF). Exposure Draft for Comment; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Dreinhofer, K.; Stucki, G.; Ewert, T.; Huber, E.; Ebenbichler, G.; Gutenbrunner, C.; Kostanjsek, N.; Cieza, A. ICF Core Sets for osteoarthritis. J. Rehabil. Med. 2004, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Pisoni, C.; Giardini, A.; Majani, G.; Maini, M. International Classification of Functioning, Disability and Health (ICF) core sets for osteoarthritis. A useful tool in the follow-up of patients after joint arthroplasty. Eur. J. Phys. Rehabil. Med. 2008, 44, 377–385. [Google Scholar] [PubMed]
- Visser, A.W.; de Mutsert, R.; Loef, M.; Le Cessie, S.; den Heijer, M.; Bloem, J.L.; Reijnierse, M.; Rosendaal, F.R.; Kloppenburg, M.; NEO Study Group. The role of fat mass and skeletal muscle mass in knee osteoarthritis is different for men and women: The NEO study. Osteoarthr. Cartil. 2014, 22, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Tolk, J.J.; Janssen, R.P.A.; Haanstra, T.M.; van der Steen, M.M.C.; Bierma Zeinstra, S.M.A.; Reijman, M. Outcome Expectations of Total Knee Arthroplasty Patients: The Influence of Demographic Factors, Pain, Personality Traits, Physical and Psychological Status. J. Knee Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Huang, Y.C.; Chiu, Y.S.; Liou, T.H. Effect of body mass index on knee function outcome following continuous passive motion in patients with osteoarthritis after total knee replacement. Physiotherapy 2017, 103, 266–275. [Google Scholar] [CrossRef]
- Abizanda Soler, P.; Paterna Mellinas, G.; Martinez Sanchez, E.; Lopez Jimenez, E. Comorbidity in the elderly: Utility and validity of assessment tools. Rev. Esp. Geriatr. Gerontol. 2010, 45, 219–228. [Google Scholar] [CrossRef]
- Cieza, A.; Fayed, N.; Bickenbach, J.; Prodinger, B. Refinements of the ICF Linking Rules to strengthen their potential for establishing comparability of health information. Disabil. Rehabil. 2019, 41, 574–583. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.W.; Chi, W.C.; Chang, K.H.; Yen, C.F.; Liao, H.F.; Escorpizo, R.; Liou, T.H. World health organization disability assessment schedule 2.0 as an objective assessment tool for predicting return to work after a stroke. Disabil Rehabil. 2018, 40, 2592–2597. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Hazra, A.; Gogtay, N. Biostatistics Series Module 5: Determining Sample Size. Indian J. Dermatol. 2016, 61, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Morishita, S.; Yamauchi, S.; Fujisawa, C.; Domen, K. Rating of perceived exertion for quantification of the intensity of resistance exercise. Int. J. Phys. Med. Rehabil. 2013, 1, 172. [Google Scholar]
- Row, B.S.; Knutzen, K.M.; Skogsberg, N.J. Regulating explosive resistance training intensity using the rating of perceived exertion. J. Strength Cond. Res. 2012, 26, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, S.J.; Toms, A.D.; Brown, M.; Welsman, J.R.; Ukoumunne, O.C.; Knapp, K.M. A study investigating short- and medium-term effects on function, bone mineral density and lean tissue mass post-total knee replacement in a Caucasian female post-menopausal population: Implications for hip fracture risk. Osteoporos. Int. 2016, 27, 2567–2576. [Google Scholar] [CrossRef]
- Rothney, M.P.; Brychta, R.J.; Schaefer, E.V.; Chen, K.Y.; Skarulis, M.C. Body composition measured by dual-energy X-ray absorptiometry half-body scans in obese adults. Obesity (Silver Spring) 2009, 17, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, M.A.; Nechtow, W.; Schwenke, T.; Moisio, K.C. Knee Flexion and Daily Activities in Patients following Total Knee Replacement: A Comparison with ISO Standard 14243. Biomed. Res. Int. 2015, 2015, 157541. [Google Scholar] [CrossRef] [Green Version]
- Bade, M.J.; Kittelson, J.M.; Kohrt, W.M.; Stevens-Lapsley, J.E. Predicting Functional Performance and Range of Motion Outcomes After Total Knee Arthroplasty. Am. J. Phys. Med. Rehabil. 2014, 93, 579–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kornuijt, A.; de Kort, G.J.L.; Das, D.; Lenssen, A.F.; van der Weegen, W. Recovery of knee range of motion after total knee arthroplasty in the first postoperative weeks: Poor recovery can be detected early. Musculoskelet. Surg. 2019, 103, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Lin, L.F.; Huang, Y.C.; Huang, S.W.; Chou, L.C.; Liou, T.H. Functional outcomes of outpatient balance training following total knee replacement in patients with knee osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2015, 29, 855–867. [Google Scholar] [CrossRef]
- Xie, F.; Li, S.C.; Goeree, R.; Tarride, J.E.; O’Reilly, D.; Lo, N.N.; Yeo, S.J.; Yang, K.Y.; Thumboo, J. Validation of Chinese Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) in patients scheduled for total knee replacement. Qual. Life Res. 2008, 17, 595–601. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Horton, N.J.; Carpenter, J.; Pocock, S.J. Strategy for intention to treat analysis in randomised trials with missing outcome data. BMJ 2011, 342, d40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, D.; Visser, M.; De Meersman, R.E.; Sepúlveda, D.; Baumgartner, R.N.; Pierson, R.N.; Harris, T.; Heymsfield, S.B. Appendicular skeletal muscle mass: Effects of age, gender, and ethnicity. J. Appl. Physiol. (1985) 1997, 83, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Roach, K.E.; Miles, T.P. Normal hip and knee active range of motion: The relationship to age. Phys. Ther. 1991, 71, 656–665. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Williams Andrews, A. Normal walking speed: A descriptive meta-analysis. Physiotherapy 2011, 97, 182–189. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Gelman, A.; Hill, J.; Yajima, M. Why we (usually) don’t have to worry about multiple comparisons. J. Res. Educ. Eff. 2012, 5, 189–211. [Google Scholar] [CrossRef] [Green Version]
- Wada, O.; Kurita, N.; Kamitani, T.; Nakano, N.; Mizuno, K. Influence of the severity of knee osteoarthritis on the association between leg muscle mass and quadriceps strength: The SPSS-OK study. Clin. Rheumatol. 2019, 38, 719–725. [Google Scholar] [CrossRef]
- Chen, H.T.; Wu, H.J.; Chen, Y.J.; Ho, S.Y.; Chung, Y.C. Effects of 8-week kettlebell training on body composition, muscle strength, pulmonary function, and chronic low-grade inflammation in elderly women with sarcopenia. Exp. Gerontol. 2018, 112, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.C.; Yang, R.S.; Yang, R.J.; Chang, S.F. Effects of resistance training on body composition and functional capacity among sarcopenic obese residents in long-term care facilities: A preliminary study. BMC Geriatr. 2018, 18, 21. [Google Scholar] [CrossRef] [Green Version]
- Gadelha, A.B.; Paiva, F.M.L.; Gauche, R.; de Oliveira, R.J.; Lima, R.M. Effects of resistance training on sarcopenic obesity index in older women: A randomized controlled trial. Arch. Gerontol. Geriatr. 2016, 65, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Torres, M.; Trexler, E.T.; Smith-Ryan, A.E.; Reynolds, A. A mathematical model of the effects of resistance exercise-induced muscle hypertrophy on body composition. Eur. J. Appl. Physiol. 2018, 118, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Borjesson, M.; Weidenhielm, L.; Elfving, B.; Olsson, E. Tests of walking ability at different speeds in patients with knee osteoarthritis. Physiother. Res. Int. 2007, 12, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.A.; Cook, C.E.; Baxter, G.D.; Dockerty, J.D.; Abbott, J.H. A comparison of 3 methodological approaches to defining major clinically important improvement of 4 performance measures in patients with hip osteoarthritis. J. Orthop. Sports Phys. Ther. 2011, 41, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Chen, H.C.; Huang, S.W.; Liou, T.H. The Role of Muscle Mass Gain Following Protein Supplementation Plus Exercise Therapy in Older Adults with Sarcopenia and Frailty Risks: A Systematic Review and Meta-Regression Analysis of Randomized Trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshi, R.N.; White, P.B.; Murray-Weir, M.; Alexiades, M.M.; Sculco, T.P.; Ranawat, A.S. Prospective Randomized Trial of the Efficacy of Continuous Passive Motion Post Total Knee Arthroplasty: Experience of the Hospital for Special Surgery. J. Arthroplast. 2015, 30, 2364–2369. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Tsauo, J.Y.; Huang, S.W.; Chen, H.C.; Chiu, Y.S.; Liou, T.H. Preoperative range of motion and applications of continuous passive motion predict outcomes after knee arthroplasty in patients with arthritis. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1259–1269. [Google Scholar] [CrossRef] [PubMed]
- Reid, K.F.; Naumova, E.N.; Carabello, R.J.; Phillips, E.M.; Fielding, R.A. Lower extremity muscle mass predicts functional performance in mobility-limited elders. J. Nutr. Health Aging 2008, 12, 493–498. [Google Scholar] [CrossRef]
- Rastogi, R.; Chesworth, B.M.; Davis, A.M. Change in patient concerns following total knee arthroplasty described with the International Classification of Functioning, Disability and Health: A repeated measures design. Health Qual. Life Outcomes 2008, 6, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oesen, S.; Halper, B.; Hofmann, M.; Jandrasits, W.; Franzke, B.; Strasser, E.M.; Graf, A.; Tschan, H.; Bachl, N.; Quittan, M.; et al. Effects of elastic band resistance training and nutritional supplementation on physical performance of institutionalised elderly—A randomized controlled trial. Exp. Gerontol. 2015, 72, 99–108. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Experimental (n = 20) | Control (n = 20) | ||
|---|---|---|---|---|
| Mean | (SD) | Mean | (SD) | |
| Sociodemographic | ||||
| Age (year) | 72.22 | (7.75) | 69.79 | (6.72) |
| Education, n (%) | ||||
| Primary | 12 | (60) | 13 | (65) |
| Secondary | 4 | (20) | 2 | (10) |
| University | 4 | (20) | 5 | (25) |
| Living status, n (%) | ||||
| Alone | 3 | (15) | 4 | (20) |
| Family/Spouse | 17 | (85) | 16 | (80) |
| Smokers, n (%) | 2 | (10) | 3 | (15) |
| Alcohol consumption, n (%) | 3 | (15) | 2 | (10) |
| Clinical characteristics | ||||
| Operated leg, Right, n (%) | 17 | (85) | 15 | (75) |
| K&L grade (Non-TKR leg), n (%) | ||||
| I | 9 | (45) | 7 | (35) |
| II | 8 | (40) | 9 | (45) |
| III | 3 | (15) | 4 | (20) |
| Use walking aids, n (%) | 7 | (35) | 6 | (30) |
| Number of comorbidities, n (%) | ||||
| 1 | 8 | (40) | 8 | (40) |
| 2 | 6 | (30) | 5 | (25) |
| 3 | 3 | (15) | 5 | (25) |
| ≥4 | 3 | (15) | 2 | (10) |
| Low muscle mass, n (%) a | 10 | (50) | 11 | (55) |
| Acute hospital stay (day) | 8.3 | (1.60) | 7.9 | (2.10) |
| BMI (kg/m2) | 28.27 | (3.25) | 27.60 | (3.64) |
| AMI (kg/m2) | 6.22 | (1.10) | 5.95 | (0.99) |
| Preoperative PA | ||||
| Moderate PA (h/week) | 0.97 | (1.49) | 1.11 | (2.24) |
| Walk time (h/week) | 6.79 | (6.26) | 7.11 | (6.31) |
| ICF Component ICF Code, ICF Category Title (Measure) | Experimental (n = 20) * | Control (n = 20) * | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1−T0 | T2−T0 | T0 | T1−T0 | T2−T0 | |||||||
| Mean | (SD) | Mean | (SD) | Mean | (SD) | Mean | (SD) | Mean | (SD) | Mean | (SD) | |
| Body functions | ||||||||||||
| b280 Sensation of pain (WOMAC−Pain) | 12.50 | (3.23) | −9.49 | (3.09) | −6.95 | (2.55) | 10.28 | ±3.32 | −8.60 | (1.96) | −5.55 | (1.23) |
| b710 Mobility of joint functions (ROM, degree) | 87.37 | (20.14) | 4.25 | (4.39) | 28.08 | (12.4) | 81.80 | ±21.16 | 7.41 | (6.64) | 20.58 | (11.75) |
| b730 Muscle power functions (TCR, repetition) | 10.50 | (3.69) | −1.05 | (5.91) | 9.05 | (6.74) † | 11.25 | ±3.13 | −1.80 | (4.57) | 2.25 | (5.81) |
| Body structures | ||||||||||||
| s730 Structure of upper extremity (arm lean mass, kg) | 3.69 | (1.19) | 0.24 | (1.13) | 3.41 | ±1.26 | 0.01 | (1.02) | ||||
| s750 Structure of lower extremity (leg lean mass, kg) | 10.69 | (1.80) | 0.84 | (0.91) † | 10.67 | ±1.75 | −0.02 | (0.89) | ||||
| s799 Structures related to movement, unspecified (AMI, kg/cm2) | 6.22 | (1.10) | 0.17 | (0.32) | 5.95 | ±0.99 | −0.07 | (0.34) | ||||
| Activities and participation | ||||||||||||
| d450 Walking (gait speed, m/s) | 0.75 | (0.31) | −0.17 | (0.31) | 0.30 | (0.28) † | 0.79 | ±0.37 | −0.22 | (0.35) | 0.04 | (0.27) |
| d540 Dressing (WOMAC−PF) a | 4.50 | (1.82) | 1.65 | (0.88) | −0.95 | (1.76) | 3.45 | ±2.11 | 2.55 | (2.44) | 0.60 | (2.09) |
| ICF Component ICF Code, ICF Category Title | Experimental (n = 20) | Control (n = 20) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1−T0 | T2−T0 | T0 | T1−T0 | T2−T0 | |||||||
| Mean | ±SD | Mean | ±SD | Mean | ±SD | Mean | ±SD | Mean | ±SD | Mean | ±SD | |
| Body functions | ||||||||||||
| b280 Sensation of pain | 3.30 | (0.80) | −1.35 | ±0.59 | −2.15 | (0.88) | 2.90 | (0.85) | −1.20 | (0.52) | −1.80 | (1.06) |
| b710 Mobility of joint functions | 1.85 | (0.75) | −0.20 | ±0.41 | −1.10 | (0.64) | 2.15 | (0.67) | −0.50 | (0.51) | −0.80 | (0.41) |
| b730 Muscle power functions | 1.60 | (1.10) | 0.30 | ±1.72 | −1.75 | (0.12) * | 1.35 | (0.99) | 0.60 | (1.50) | −0.25 | (1.52) |
| Body structures | ||||||||||||
| s730 Structure of upper extremity | 0.50 | (0.69) | 0.00 | (0.56) | 0.90 | (0.79) | 0.30 | (1.03) | ||||
| s750 Structure of lower extremity | 1.30 | (0.66) | −0.60 | (0.94) | 1.50 | (0.61) | −0.10 | (0.79) | ||||
| s799 Structures related to movement, unspecified | 0.40 | (0.68) | −0.25 | (0.85) | 0.48 | (1.09) | 0.25 | (1.16) | ||||
| Activities and participation | ||||||||||||
| d450 Walking | 2.00 | (0.92) | 0.45 | ±1.10 | −1.75 | (1.12) * | 1.80 | (0.89) | 0.70 | (0.98) | −0.25 | (1.52) |
| d540 Dressing | 2.30 | (0.87) | 0.35 | ±1.39 | −1.50 | (1.24) * | 1.95 | (1.00) | 0.75 | (1.37) | −0.40 | (1.05) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, C.-D.; Chiu, Y.-S.; Ku, J.-W.; Huang, S.-W.; Liou, T.-H. Effects of Elastic Resistance Exercise on Postoperative Outcomes Linked to the ICF Core Sets for Osteoarthritis after Total Knee Replacement in Overweight and Obese Older Women with Sarcopenia Risk: A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2194. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072194
Liao C-D, Chiu Y-S, Ku J-W, Huang S-W, Liou T-H. Effects of Elastic Resistance Exercise on Postoperative Outcomes Linked to the ICF Core Sets for Osteoarthritis after Total Knee Replacement in Overweight and Obese Older Women with Sarcopenia Risk: A Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(7):2194. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072194
Chicago/Turabian StyleLiao, Chun-De, Yen-Shuo Chiu, Jan-Wen Ku, Shih-Wei Huang, and Tsan-Hon Liou. 2020. "Effects of Elastic Resistance Exercise on Postoperative Outcomes Linked to the ICF Core Sets for Osteoarthritis after Total Knee Replacement in Overweight and Obese Older Women with Sarcopenia Risk: A Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 7: 2194. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072194