Sociodemographic Inequalities in Outcomes of a Swedish Nationwide Self-Management Program for Osteoarthritis: Results from 22,741 Patients between Years 2008–2017



Abstract
:1. Introduction
Study Aim
2. Method
2.1. Study Design
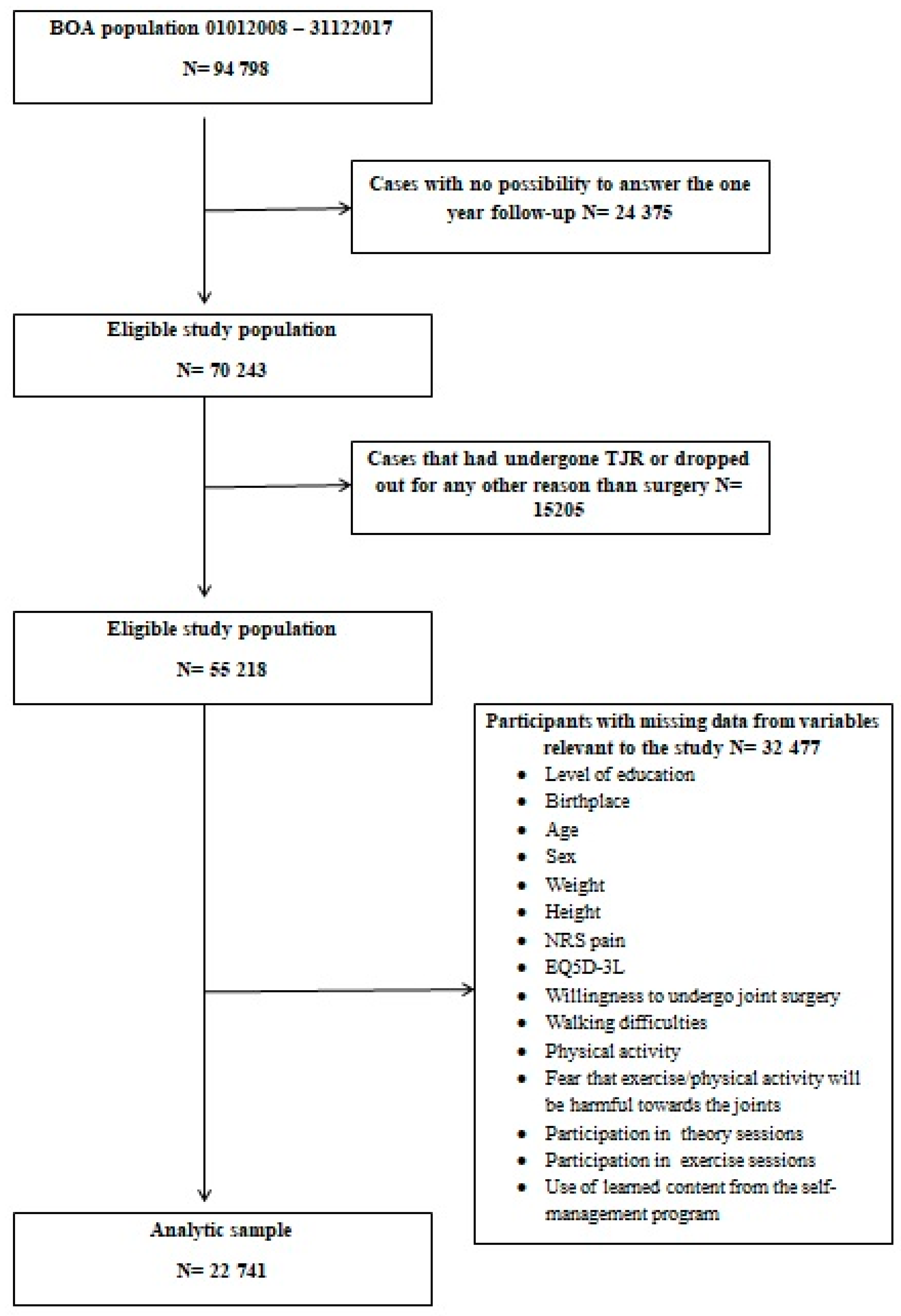
2.2. Sample Selection and Size
2.3. Measures
- Independent Variables
- -
- Which is the highest level of education that you have obtained (compulsory, upper secondary, university)?
- -
- Were you born in Sweden (yes/no)?
- CovariatesAll analyses were adjusted for age, sex, and levels of BMI. Age and sex are self-administered variables by the BOA-register, retrieved by the patient’s personal identity number in the baseline questionnaire. BMI (kg/m2) was calculated based on patient’s self-assessed weight (kilograms) and length (centimetres).
- Dependent Variables
- -
- Mean pain intensity from the patient’s most troublesome joint in the past week was self-reported on a numeric rating scale (NRS), ranging from 0–10 (0 = no pain, 10 = maximum pain) [21].
- -
- The EQ-5D-3L is a standardised self-reported generic measurement of health. It covers five aspects of health: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 levels: no problems, some problems, extreme problems, resulting in 243 possible health states. In this study we used the United Kingdom value set, diverging from −0.594 to 1, where a value of 1 means that a person has no problems with any of the five health domains, and value of 0 means that the person has extreme problems with all five health domains [22].
- -
- Do you suffer so much impairment from any joint that you are willing to undergo surgery (yes/no)?
- -
- Does your pain cause you difficulties with walking (yes/no)?
- -
- Being physical active more than 150 min per week (yes/no)? This was originally an ordinal variable with seven answer options (spanning from 0 min to more than 300 min). Categories 150–300 min and more than 300 min were recoded into “yes”, and all other categories into “no”. This because at least 150 min of physical activity weekly is recommended to prevent all-cause mortality and chronic disease [23].
- -
- Fear-avoidance behaviour: Are you afraid that exercise or physical activity will be harmful to your joints (yes/no)?
- -
- Participation in theory lessons was assessed by a single question assessed by the physical or occupational therapist, namely “has the patient participated in the theory sessions” (yes/no)?
- -
- Number of supervised exercise sessions the patient participated in, assessed and reported by the physical or occupational therapist. This variable had five answer categories spanning from no session to more than 12. But to make the variable easier to overview, responses were categorized into: no exercise session, 1–9 sessions, and 10 or more.
- -
- How often do you use knowledge acquired from the self-management program? Originally the variable had six categories but for the purpose of interpretation the variable was recoded into two categories. One category included responses like “every day or several times daily” while the other category included responses like “every week, month, never, or don’t know”.
2.4. Statistical Analyses
2.5. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Reported by | Measurement Point in Time | |||||
|---|---|---|---|---|---|---|
| Variables | Indicator | Patient | PT/OT | Baseline | 3 Months | 12 Months |
| Ind. variable | Level of education | X | X | |||
| Ind. variable | Birthplace | X | X | |||
| Covariate | Age | X | X | |||
| Covariate | Sex | X | X | |||
| Covariate | Weight | X | X | |||
| Covariate | Height | X | X | |||
| Dep. variable | NRS Pain | X | X | X | X | |
| Dep. variable | EQ-5D-3L | X | X | X | X | |
| Dep. variable | Willingness for joint surgery | X | X | X | X | |
| Dep. variable | Walking difficulties | X | X | X | X | |
| Dep. variable | Physical activity | X | X | X | X | |
| Dep. variable | Fear avoidance behaviour: Fear that exercise/physical activity will be harmful towards the joints | X | X | X | X | |
| Dep. variable | Participation in theory sessions | X | X | |||
| Dep. variable | Participation in exercise sessions | X | X | |||
| Dep. variable | Use of learned content from the self-management program | X | X | X | ||
| Total (n = 47,682) | Mean | min, max | SD | ||
|---|---|---|---|---|---|
| Gender | Men | 31.4 (14645) | |||
| Women | 68.6 (31962) | ||||
| Level of education | Compulsory | 34.2 (16316) | |||
| Upper Secondary | 36.5 (17385) | ||||
| University | 26.5 (12612) | ||||
| Country of birth | Foreign | 9.3 (4450) | |||
| Domestic | 88 (41946) | ||||
| Most painful joint | Knee | 65.1 (23151) | |||
| at baseline | Hip | 32.3 (11491) | |||
| Hand | 2.5 (905) | ||||
| Age | 65.5 | 18, 100 | 9.8 | ||
| BMI | 28.1 | 14, 168 | 5 | ||
References
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; A Salomon, J.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Kingsbury, S.R.; Gross, H.J.; Isherwood, G.; Conaghan, P.G. Osteoarthritis in Europe: Impact on health status, work productivity and use of pharmacotherapies in five European countries. Rheumatology 2014, 53, 937–947. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Moskowitz, R.; Nuki, G.; Abramson, S.; Altman, R.; Arden, N.; Bierma-Zeinstra, S.; Brandt, K.; Croft, P.; Doherty, M.; et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr. Cartil. 2008, 16, 137–162. [Google Scholar] [CrossRef] [Green Version]
- Snijders, G.; den Broeder, A.; van Riel, P. Evidence-based tailored conservative treatment of knee and hip osteoarthritis: Between knowing and doing. Scand. J. Rheumatol. 2011, 40, 225–231. [Google Scholar] [CrossRef]
- Shrier, I.; Feldman, D.; Gaudet, M.-C.; Rossignol, M.; Zukor, D.; Tanzer, M.; Gravel, C.; Newman, N.; Dumais, R. Conservative non-pharmacological treatment options are not frequently used in the management of hip osteoarthritis. J. Sci. Med. Sport 2006, 9, 81–86. [Google Scholar] [CrossRef]
- Thorstensson, C.A.; Garellick, G.; Rystedt, H.; Dahlberg, L.E. Better Management of Patients with Osteoarthritis: Development and Nationwide Implementation of an Evidence-Based supported Osteoarthritis Self-Management Programme. Musculoskelet. Care 2015, 13, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Limbäck-Svensson, G.; Abbott, A.; Wetterling, K. The BOA Registry Annual Report for Year 2018. Available online: https://registercentrum.blob.core.windows.net/boa/r/BOA-arsrapport-2018-B1x6Y3MGwH.pdf (accessed on 29 December 2019).
- Jönsson, T.; Hansson, E.E.; Thorstensson, C.A.; Eek, F.; Bergman, P.; Dahlberg, L.E. The effect of education and supervised exercise on physical activity, pain, quality of life and self-efficacy—An intervention study with a reference group. BMC Musculoskelet. Disord. 2018, 19, 198. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, T.; Eek, F.; Dell’Isola, A.; Dahlberg, L.E.; Hansson, E.E. The Better Management of Patients with Osteoarthritis Program: Outcomes after evidence-based education and exercise delivered nationwide in Sweden. PLoS ONE 2019, 14, e0222657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsson, C.B.; Ekelund, J.; Degerstedt, Å.; Thorstensson, C.A. Change in self-efficacy after participation in a supported self-mangament program for osteoarthritis—An observational study of 11 906 patients. Disabil. Rehabilit. 2019, 27, 1–8. [Google Scholar] [CrossRef] [PubMed]
- A Kiadaliri, A.; De Verdier, M.G.; Turkiewicz, A.; Lohmander, L.; Englund, M.; Lohmander, L. Socioeconomic inequalities in knee pain, knee osteoarthritis, and health-related quality of life: A population-based cohort study in southern Sweden. Scand. J. Rheumatol. 2017, 46, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupic, F.; Eisler, T.; Garellick, G.; Kärrholm, J. Influence of ethnicity and socioeconomic factors on outcome after total hip replacement. Scand. J. Caring Sci. 2013, 27, 139–146. [Google Scholar] [CrossRef]
- Callahan, L.F.; Shreffler, J.; Siaton, B.C.; Helmick, C.G.; Schoster, B.; Schwartz, T.A.; Chen, J.-C.; Renner, J.B.; Jordan, J.M. Limited educational attainment and radiographic and symptomatic knee osteoarthritis: A cross-sectional analysis using data from the Johnston County (North Carolina) Osteoarthritis Project. Arthritis Res. Ther. 2010, 12, R46. [Google Scholar] [CrossRef] [Green Version]
- Hawker, G.; Wright, J.G.; Glazier, R.H.; Coyte, P.C.; Harvey, B.; Williams, J.I.; Badley, E.M. The Effect of Education and Income on Need and Willingness to Undergo Total Joint Arthroplasty. Arthritis Rheum. 2002, 46, 3331–3339. [Google Scholar] [CrossRef]
- Statistics Sweden. Foreign Born in Sweden. Available online: https://www.scb.se/hitta-statistik/sverige-i-siffror/manniskorna-i-sverige/utrikes-fodda/ (accessed on 27 December 2019).
- Soares, J.J.F.; Grossi, G. Experience of musculoskeletal pain comparison of immigrant and Swedish patients. Scand. J. Caring Sci. 1999, 13, 254–266. [Google Scholar] [CrossRef]
- Luong, M.-L.; Cleveland, R.J.; A Nyrop, K.; Callahan, L.F. Social determinants and osteoarthritis outcomes. Aging Health 2012, 8, 413–437. [Google Scholar] [CrossRef] [Green Version]
- Borkhoff, C.M.; Wieland, M.L.; Myasoedova, E. Reaching those most in need: A scoping review of interventions to improve health care quality for disadvantaged populations with osteoarthritis. Arthr. Care Res. 2011, 63, 39–52. [Google Scholar] [CrossRef]
- Li, L.; Sayre, E.C.; Kopec, J.A. Quality of Nonpharmalogical Care in the Community for People with Knee and Hip Osteoarthritis. J. Rheumatol. 2011, 38, 2230–2237. [Google Scholar] [CrossRef]
- Gelman, A.; Hill, J. Data Analysis Using Regression and Multilevel/Hierarchical Models; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Ferreira-Valente, A.; Pais-Ribeiro, J.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef]
- EuroQol Research Foundation. EQ-5D-3L User Guide. 2018. Available online: https://euroqol.org/publications/user-guides (accessed on 27 December 2019).
- WHO. Available online: http://www.who.int/dietphysicalactivity/physical-activity-recommendations-18-64years.pdf?ua=1 (accessed on 27 December 2019).
- Youm, J.; Chan, V.; Belkora, J.; Bozic, K.J. Impact of socioeconomic factors on informed decision making and treatment choice in patients with hip and knee OA. J. Arthroplast. 2015, 30, 171–175. [Google Scholar] [CrossRef]
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner, E. Barriers to treatment adherence in physiotherapy outpatient clinics: A systematic review. Man. Ther. 2010, 15, 220–228. [Google Scholar] [CrossRef]
- Sweden Statitics. The Swedish Occupational Register with Statistics 2017. Available online: https://www.scb.se/contentassets/1fe7f957920f4eaf97bddcc0270553f2/am0208_2017a01_sm_am33sm1901.pdf (accessed on 10 January 2020).
- Tuakli-Wosornu, Y.A.; Selzer, F.; Losina, E.; Katz, J.N. Predictors of Exercise Adherence in Patients with Meniscal Tear and Osteoarthritis. Arch. Phys. Med. Rehabil. 2016, 97, 1945–1952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farin, E.; Ullrich, A.; Nagl, M. Health education literacy in patients with chronic musculoskeletal diseases: Development of a new questionnaire and sociodemographic predictors. Health Educ. Res. 2013, 28, 1080–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marks, R. Health Literacy and Osteoarthritis Self-Management. J. Aging Res. Healthc. 2018, 2, 32–45. [Google Scholar] [CrossRef] [Green Version]
- Weigl, M.; Angst, F.; Aeschlimann, A.; Lehmann, S.; Stucki, G. Predictors for response to rehabilitation in patients with hip or knee osteoarthritis: A comparison of logistic regression models with three different definitions of responder. Osteoarthr. Cartil. 2006, 14, 641–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Total (n = 22,741) | % (N) | Mean | min, max | SD | |
|---|---|---|---|---|---|
| Sex | Men | 29.3 (6664) | |||
| Women | 70.7 (16,077) | ||||
| Educational level | Compulsory | 32.2 (7328) | |||
| Upper Secondary | 37.2 (8467) | ||||
| University | 30.5 (6946) | ||||
| Country of birth | Foreign | 7.7 (1744) | |||
| Domestic | 92.3 (20,997) | ||||
| Most painful joint | Knee | 68.8 (15,677) | |||
| at baseline | Hip | 28.5 (6477) | |||
| Hand | 2.7 (607) | ||||
| Age | 66.3 | 27, 95 | 9 | ||
| BMI | 27.8 | 13, 71 | 4.7 |
| NRS Pain (0–10 Scale) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Level of Education or Country of Birth | Baseline | 3 Months | Difference at 3 Months vs. Baseline | 12 Months | Difference at 12 Months vs. Baseline | |||
| Mean | SD | Mean | SD | Mean | SD | |||
| Compulsory | 5.2 | 1.8 | 4.1 | 2.0 | −1.1 | 4.6 | 2.2 | −0.6 |
| Upper Secondary | 5.2 | 1.9 | 4.0 | 2.0 | −1.2 | 4.4 | 2.3 | −0.8 |
| University | 4.8 | 1.9 | 3.6 | 2.0 | −1.2 | 4.0 | 2.3 | −0.8 |
| Foreign born | 5.5 | 1.9 | 4.2 | 2.0 | −1.2 | 4.8 | 2.3 | −0.7 |
| Domestic born | 5.1 | 1.9 | 3.9 | 2.2 | −1.2 | 4.3 | 2.3 | −0.8 |
| Total group | 5.1 | 1.9 | 3.9 | 2.0 | −1.2 | 4.3 | 2.3 | −0.8 |
| EQ-5D-3L | ||||||||
| Level of education or country of birth | Baseline | 3 months | Difference at 3 months vs. baseline | 12 months | Difference at 12 months vs. baseline | |||
| Mean | SD | Mean | SD | Mean | SD | |||
| Compulsory | 0.64 | 0.20 | 0.70 | 0.18 | +0.06 | 0.66 | 0.20 | +0.02 |
| Upper Secondary | 0.64 | 0.21 | 0.70 | 0.18 | +0.06 | 0.67 | 0.20 | +0.03 |
| University | 0.67 | 0.19 | 0.72 | 0.16 | +0.05 | 0.70 | 0.19 | +0.03 |
| Foreign born | 0.58 | 0.24 | 0.67 | 0.21 | +0.09 | 0.63 | 0.22 | +0.05 |
| Domestic born | 0.65 | 0.20 | 0.71 | 0.17 | +0.06 | 0.68 | 0.19 | +0.03 |
| Total group | 0.65 | 0.20 | 0.71 | 0.19 | +0.06 | 0.68 | 0.26 | +0.03 |
| Do you suffer that much impairment from any joint that you are willing to undergo surgery? Yes/No | ||||||||
| Level of education or country of birth | Baseline Yes | 3 months Yes | Difference at 3 months vs. baseline | 12 months Yes | difference at 12 months vs. baseline | |||
| Compulsory | 22.7 (1662) | 16.0 (1172) | −6.7 | 24.6 (1801) | +1.9 | |||
| Upper Secondary | 19.2 (1694) | 13.7 (1153) | −5.5 | 22.0 (1860) | +2.8 | |||
| University | 14.7 (1019) | 9.7 (674) | −5 | 17.4 (1210) | +2.7 | |||
| Foreign born | 23.3 (406) | 15.6 (271) | −7.7 | 24.1 (420) | +0.8 | |||
| Domestic born | 18.9 (3969) | 13.0 (2728) | −5.9 | 21.2 (4451) | +2.3 | |||
| Total group | 19.2 (4375) | 13.2 (2999) | −6 | 21.4 (4871) | +2.2 | |||
| Does your pain cause you difficulties with walking? Yes/No | ||||||||
| Level of education or country of birth | Baseline Yes | 3 months Yes | Difference at 3 months vs. baseline | 12 months Yes | difference at 12 months vs. baseline | |||
| Compulsory | 79.5 (5824) | 60.9 (4460) | −18.6 | 63.4 (4644) | −16.1 | |||
| Upper Secondary | 78.5 (6650) | 57.4 (4864) | −21.1 | 59.5 (5042) | −19 | |||
| University | 76.1 (5287) | 54.9 (3810) | −21.2 | 56.1 (3896) | −20 | |||
| Foreign born | 80.6 (1406) | 61.7 (1076) | −18.9 | 63.8 (1113) | −16.8 | |||
| Domestic born | 77.9 (16,355) | 57.4 (12,058) | −20.5 | 59.4 (12,469) | −18.5 | |||
| Total group | 78.1 (17,761) | 57.8 (12,134) | −20.3 | 59.7 (13,582) | −18.4 | |||
| Physical Active more than 150 min Per Week Yes/No | |||||
|---|---|---|---|---|---|
| Level of Education or Country of Birth | Baseline Yes | 3 Months Yes | Difference at 3 Months vs. Baseline | 12 Months Yes | Difference at 12 Months vs. Baseline |
| Compulsory | 40.8 (2987) | 42.2 (3092) | +1.4 | 37.6 (2753) | −3.2 |
| Upper Secondary | 44.9 (3803) | 47.7 (4042) | +2.8 | 44.5 (3764) | −0.4 |
| University | 49.8 (3456) | 52.6 (3652) | +2.8 | 50.2 (3487) | +0.3 |
| Foreign born | 37.7 (657) | 42.4 (740) | +4.7 | 38.7 (675) | +1 |
| Domestic born | 45.7 (9589) | 47.8 (10,046) | +2.1 | 44.4 (9329) | −1.3 |
| Total group | 45.1 (10,246) | 47.4 (10,786) | +2.3 | 44.0 (10,004) | −1.1 |
| Fear avoidance: Are you afraid that exercise or physical activity will be harmful to your joints? Yes/No | |||||
| Level of Education or Country of Birth | Baseline Yes | 3 months Yes | Difference at 3 months vs. baseline | 12 months Yes | Difference at 12 months vs. baseline |
| Compulsory | 14.3 (1048) | 5.5 (402) | −8.8 | 9.4 (688) | −4.9 |
| Upper Secondary | 16.4 (1385) | 5.2 (441) | −11.2 | 8.7 (739) | −7.7 |
| University | 15.0 (1043) | 4.2 (292) | −10.8 | 5.7 (393) | −9.3 |
| Foreign born | 23.3 (407) | 10.8 (189) | −12.5 | 17.0 (297) | −6.3 |
| Domestic born | 14.6 (3069) | 4.5 (946) | −10.1 | 7.3 (1523) | −7.3 |
| Total group | 15.3 (3476) | 5.0 (1135) | −10.3 | 8.0 (1820) | −7.3 |
| Number of supervised exercise sessions the patient participated in | |||||
| Level of education or country of birth | None | 1–9 Times | 10 Times or more | ||
| Compulsory | 40.6 (2972) | 26.9 (1974) | 32.5 (2382) | ||
| Upper Secondary | 42.8 (3625) | 28.2 (2391) | 28.9 (2451) | ||
| University | 40.3 (2800) | 30.6 (2125) | 29.1 (2021) | ||
| Foreign born | 36.1 (629) | 31.8 (554) | 32.2 (561) | ||
| Domestic born | 41.8 (8768) | 28.3 (5936) | 30.0 (6293) | ||
| Total group | 41.3 (9397) | 28.5 (6490) | 30.1 (6854) | ||
| How often do you use acquired knowledge from the self-management program? Every day or several times daily (compared to those who answered: Every week, month, never, or don’t know) | |||||
| Level of education or country of birth | 3 months Yes | 12 months Yes | Difference at 12 months vs. baseline | ||
| Compulsory | 60.7 (4450) | 36.8 (2700) | −23.9 | ||
| Upper Secondary | 61.3 (5188) | 37.4 (3170) | −23.9 | ||
| University | 63.0 (4375) | 40.7 (2824) | −22.3 | ||
| Foreign born | 65.1 (1135) | 43.2 (753) | −21.9 | ||
| Domestic born | 61.3 (12878) | 37.8 (7941) | −23.5 | ||
| Total group | 61.6 (14013) | 38.2 (8694) | −23.4 | ||
| NRS Pain (0–10 Scale) Mean Values | ||||||
|---|---|---|---|---|---|---|
| Education or Country of Birth | Baseline | 3 Months | 12 Months | |||
| Mean | CI | Mean | CI | Mean | CI | |
| Compulsory | 5.2 | 5.2–5.3 | 4.0 | 4.0–4.1 | 4.5 | 4.4–4.5 |
| Upper Secondary | 5.2 | 5.1–5.2 | 4.0 | 3.9–4.0 | 4.3 | 4.3–4.4 |
| University | 4.8 | 4.8–4.9 | 3.8 | 3.8–3.8 | 4.1 | 4.1–4.2 |
| Foreign | 5.5 | 5.4–5.5 | 4.0 | 3.9–4.1 | 4.5 | 4.4–4.6 |
| Domestic | 5.1 | 5.0–5.1 | 3.9 | 3.9–4.0 | 4.3 | 4.3–4.3 |
| EQ-5D-3L Mean values | ||||||
| Education or country of birth | Baseline | 3 months | 12 months | |||
| Mean | CI | Mean | CI | Mean | CI | |
| Compulsory | 0.63 | 0.63–0.64 | 0.70 | 0.70–0.70 | 0.67 | 0.67–0.67 |
| Upper Secondary | 0.64 | 0.64–0.65 | 0.71 | 0.71–0.71 | 0.67 | 0.67–0.68 |
| University | 0.66 | 0.66–0.67 | 0.72 | 0.71–0.72 | 0.68 | 0.68–0.69 |
| Foreign | 0.59 | 0.58–0.60 | 0.69 | 0.69–0.70 | 0.66 | 0.65–0.66 |
| Domestic | 0.65 | 0.65–0.65 | 0.71 | 0.71–0.71 | 0.68 | 0.68–0.68 |
| Do you suffer that much impairment from any joint that you are willing to undergo surgery? Yes/No | ||||||
| Education or country of birth | Baseline | 3 months | 12 months | |||
| OR | CI | OR | CI | OR | CI | |
| Compulsory | 1.65 | 1.51–1.81 | 1.36 | 1.21–1.52 | 1.23 | 1.12–1.35 |
| Upper Secondary | 1.27 | 1.16–1.39 | 1.20 | 1.07–1.35 | 1.12 | 1.03–1.23 |
| University | 1 | 1 | 1 | |||
| Foreign | 1.34 | 1.19–1.51 | 1.09 | 0.93–1.27 | 1.07 | 0.94–1.22 |
| Domestic | 1 | 1 | 1 | |||
| Does your pain cause you difficulties with walking? Yes/No | ||||||
| Education or country of birth | Baseline | 3 months | 12 months | |||
| OR | CI | OR | CI | OR | CI | |
| Compulsory | 1.05 | 0.97–1.15 | 1.12 | 1.03–1.20 | 1.16 | 1.03–1.20 |
| Upper Secondary | 1.05 | 0.98–1.15 | 1.02 | 0.95–1.10 | 1.06 | 0.99–1.14 |
| University | 1 | 1 | 1 | |||
| Foreign | 1.13 | 1.0–1.28 | 1.14 | 1.02–1.27 | 1.16 | 1.04–1.30 |
| Domestic | 1 | 1 | 1 | |||
| Odds for Being Physical Active more than 150 min Per Week Yes/No | ||||||
|---|---|---|---|---|---|---|
| Education or Country of Birth | Baseline | 3 Months | 12 Months | |||
| OR | CI | OR | CI | OR | CI | |
| Compulsory | 0.79 | 0.74–0.85 | 0.79 | 0.74–0.90 | 0.71 | 0.66–0.77 |
| Upper Secondary | 0.87 | 0.82–0.93 | 0.88 | 0.82–0.95 | 0.85 | 0.79–0.91 |
| University | 1 | 1 | 1 | |||
| Foreign | 0.74 | 0.66–0.82 | 0.90 | 0.90–1.00 | 0.88 | 0.78–0.98 |
| Domestic | 1 | 1 | 1 | |||
| Fear avoidance behaviour: Are you afraid that exercise or physical activity will be harmful to your joints? | ||||||
| Education or country of birth | Baseline | 3 months | 12 months | |||
| OR | CI | OR | CI | OR | CI | |
| Compulsory | 1.06 | 0.96–1.17 | 1.40 | 1.19–1.65 | 1.86 | 1.62–2.14 |
| Upper Secondary | 0.97 | 0.89–1.07 | 1.15 | 0.98–1.35 | 1.45 | 1.26–1.65 |
| University | 1 | 1 | 1 | |||
| Foreign | 1.81 | 1.60–2.04 | 2.26 | 1.89–2.69 | 2.50 | 2.16–2.90 |
| Domestic | 1 | 1 | 1 | |||
| Odds for number of supervised exercise sessions the patient participated in compared to none (0 times reference group) | ||||||
| Education or country of birth | 1–9 Times | 10 times or more | ||||
| OR | CI | OR | CI | |||
| Compulsory | 0.82 | 0.76–0.89 | 0.97 | 0.90–1.05 | ||
| Upper Secondary | 0.90 | 0.84–0.98 | 0.99 | 0.92–1.07 | ||
| University | 1 | 1 | ||||
| Foreign | 1.26 | 1.12–1.42 | 1.26 | 1.11–1.42 | ||
| Domestic | 1 | 1 | ||||
| How often do you use acquired knowledge from the self-management program? Every day or several times daily (compared to those who answered: Every week, month, never, or don’t know) | ||||||
| Education or country of birth | 1–9 Times | 10 times or more | ||||
| OR | CI | OR | CI | |||
| Compulsory | 0.84 | 0.78–0.90 | 0.85 | 0.79–0.91 | ||
| Upper Secondary | 0.98 | 0.92–1.05 | 0.91 | 0.85–0.98 | ||
| University | 1 | 1 | ||||
| Foreign | 1.16 | 1.05–1.29 | 1.20 | 1.08–1.33 | ||
| Domestic | 1 | 1 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Unevik, E.; Abbott, A.; Fors, S.; Rolfson, O. Sociodemographic Inequalities in Outcomes of a Swedish Nationwide Self-Management Program for Osteoarthritis: Results from 22,741 Patients between Years 2008–2017. J. Clin. Med. 2020, 9, 2294. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072294
Unevik E, Abbott A, Fors S, Rolfson O. Sociodemographic Inequalities in Outcomes of a Swedish Nationwide Self-Management Program for Osteoarthritis: Results from 22,741 Patients between Years 2008–2017. Journal of Clinical Medicine. 2020; 9(7):2294. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072294
Chicago/Turabian StyleUnevik, Erik, Allan Abbott, Stefan Fors, and Ola Rolfson. 2020. "Sociodemographic Inequalities in Outcomes of a Swedish Nationwide Self-Management Program for Osteoarthritis: Results from 22,741 Patients between Years 2008–2017" Journal of Clinical Medicine 9, no. 7: 2294. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072294