Antimicrobial Stewardship Program, COVID-19, and Infection Control: Spread of Carbapenem-Resistant Klebsiella Pneumoniae Colonization in ICU COVID-19 Patients. What Did Not Work?

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Infection Control Policy
2.3. COVID-19 Situation in Italy
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Burden of AMR Collaborative Group; et al. Attributable Deaths and Disability-Adjusted Life-Years Caused by Infections with Antibiotic-Resistant Bacteria in the EU and the European Economic Area in 2015: A Population-Level Modelling Analysis. Lancet Infect. Dis. 2019, 1, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Tumbarello, M.; Viale, P.; Viscoli, C.; Trecarichi, E.M.; Tumietto, F.; Marchese, A.; Spanu, T.; Ambretti, S.; Ginocchio, F.; Cristini, F.; et al. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae: Importance of combination therapy. Clin. Infect. Dis. 2012, 55, 943–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacconelli, E.; Cataldo, M.A.; Dancer, S.J.; De Angelis, G.; Falcone, M.; Frank, U.; Kahlmeter, G.; Pan, A.; Petrosillo, N.; Rodríguez-Baño, J.; et al. European Society of Clinical Microbiology. ESCMID Guidelines for the Management of the Infection Control Measures to Reduce Transmission of Multidrug-Resistant Gram-negative Bacteria in Hospitalized Patients. Clin. Microbiol. Infect. 2014, 20 (Suppl. 1), 1–55. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Resistance in Europe 2018; ECDC: Stockholm, Sweden, 2019. [Google Scholar]
- European Centre for Disease Prevention and Control. ECDC Country Visit to Italy to Discuss Antimicrobial Resistance Issues; ECDC: Stockholm, Sweden, 2017. [Google Scholar]
- World Health Organization. Rational Use of Personal Protective Equipment for Coronavirus Disease (COVID-19): Interim Guidance; License: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2020. Available online: https://apps.who.int/iris/handle/10665/331215 (accessed on 27 February 2020).
- Interim Guidance for Rational Use of SARS-COV-2 Infection Protections in Health and Socio-Health Activities in the Current SARSCOV-2 Emerging Scenario; Version of May 10, 2020; ISS Working Group COVID-19 Infections Prevention and Control: Rome, Italy, 2020; p. Rapporto ISS COVID-19 n. 2/2020Rev. 2. (In Italian)
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]
- Cingolani, M.; Caraceni, L.; Cannovo, N.; Fedeli, P. The COVID-19 Epidemic and the Prison System in Italy. J. Correct. Health Care 2020. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Guidance COVID-19 Personal Protective Equipment (PPE). Available online: https://www.gov.uk/government/collections/coronavirus-covid-19-personal-protective-equipment-ppe (accessed on 12 June 2020).
- World Health Organization. Implementation Manual to Prevent and Control the Spread of Carbapenem-Resistant Organisms at the National and Health Care Facility Level; (WHO/UHC/SDS/2019.6); Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Pittet, D.; Dharan, S.; Touveneau, S.; Sauvan, V.; Perneger, T.V. Bacterial Contamination of the Hands of Hospital Staff during Routine Patient Care. Arch. Intern. Med. 1999, 159, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Adams, B.G.; Marrie, T.G. Hand Carriage of Aerobic Gram-negative Rods by Health Care Personnel. J. Hyg. (Lond.) 1982, 89, 23–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, D.J.; Liang, S.Y.; Smith, C.L.; Johnson, J.K.; Harris, A.D.; Furuno, J.P.; Thom, K.A.; Snyder, G.M.; Day, H.R.; Perencevich, E.N. Frequent multidrug-resistant Acinetobacter baumannii contamination of gloves, gowns, and hands of healthcare workers. Infect. Control Hosp. Epidemiol. 2010, 31, 716–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grice, E.A.; Segre, J.A. The Skin Microbiome. Rev. Nat. Rev. Microbiol. 2011, 9, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.P. Normal Flora. In Medical Microbiology, 4th ed.; Baron, S., Ed.; University of Texas Medical Branch at Galveston: Galveston, TX, USA, 1996; Chapter 6. [Google Scholar]
- Wiener-Well, Y.; Galuty, M.; Rudensky, B.; Schlesinger, Y.; Attias, D.; Yinnon, A.M. Nursing and physician attire as possible source of nosocomial infections. Am. J. Infect. Control 2011, 39, 555–559. [Google Scholar] [CrossRef]
- Perry, C.; Marshall, R.; Jones, E. Bacterial contamination of uniforms. J. Hosp. Infect. 2001, 48, 238–241. [Google Scholar] [CrossRef]
- Wilson, J.A.; Loveday, H.P.; Hoffman, P.N.; Pratt, R.J. Uniform: An evidence review of the microbiological significance of uniforms and uniform policy in the prevention and control of healthcare-associated infections. Report to the Department of Health (England). J. Hosp. Infect. 2007, 66, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Babb, J.R.; Davies, J.G.; Ayliffe, G.A. Contamination of protective clothing and nurses’ uniforms in an isolation ward. J. Hosp. Infect. 1983, 4, 149–157. [Google Scholar] [CrossRef]
- Wong, D.; Nye, K.; Hollis, P. Microbial flora on doctors’ white coats. Br. Med. J. 1991, 303, 1602–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speers, R., Jr.; Shooter, R.A.; Gaya, H.; Patel, N. Contamination of nurses’ uniforms with Staphylococcus aureus. Lancet 1969, 2, 233–235. [Google Scholar] [CrossRef]
- Morgan, D.J.; Rogawski, E.; Thom, K.A.; Johnson, J.K.; Perencevich, E.N.; Shardell, M.; Leekha, S.; Harris, A.D. Transfer of multidrug-resistant bacteria to healthcare workers’ gloves and gowns after patient contact increases with environmental contamination. Crit. Care Med. 2012, 40, 1045–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casewell, M.; Phillips, I. Hands as route of transmission for Klebsiella species. Br. Med. J. 1977, 2, 1315–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
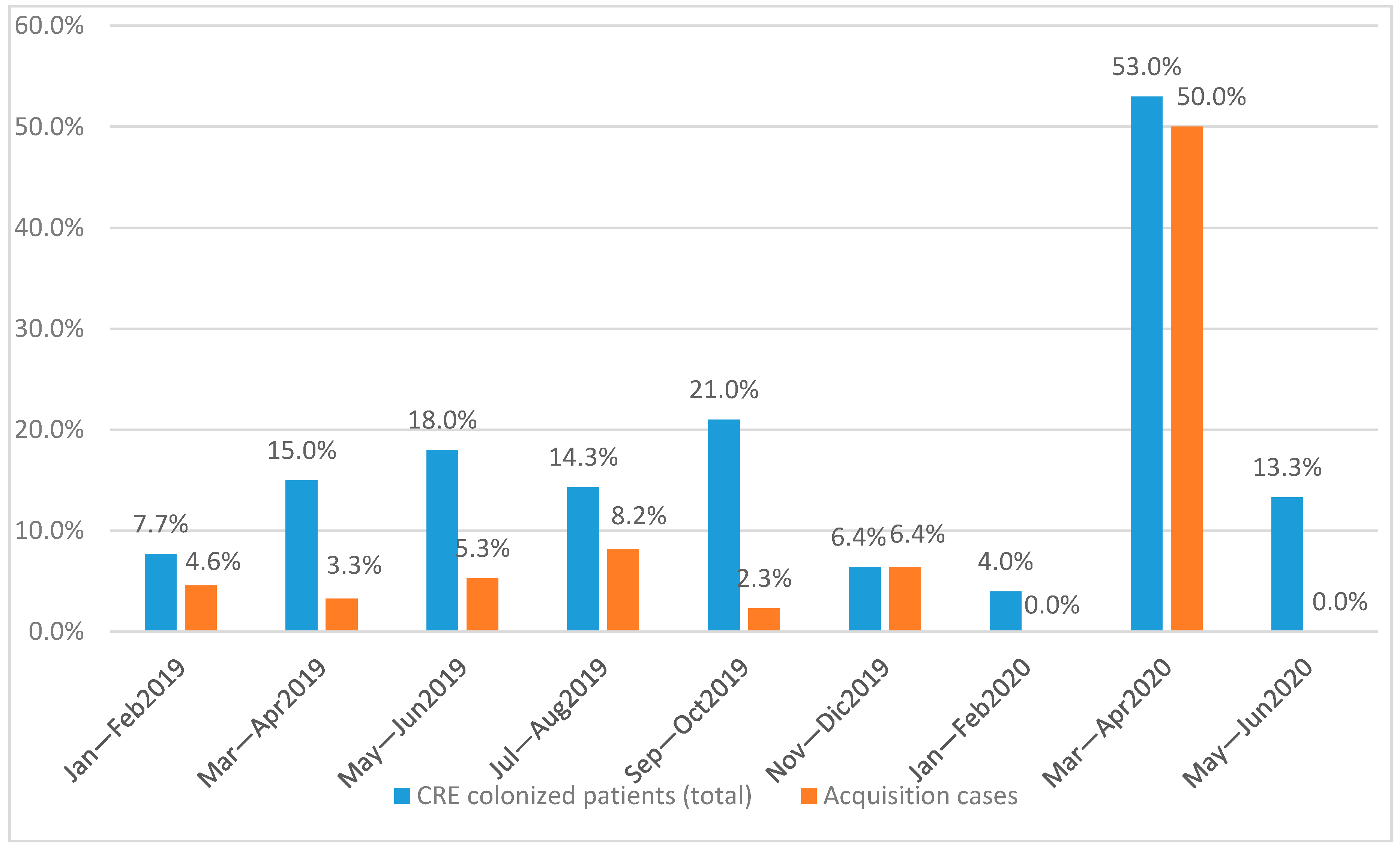
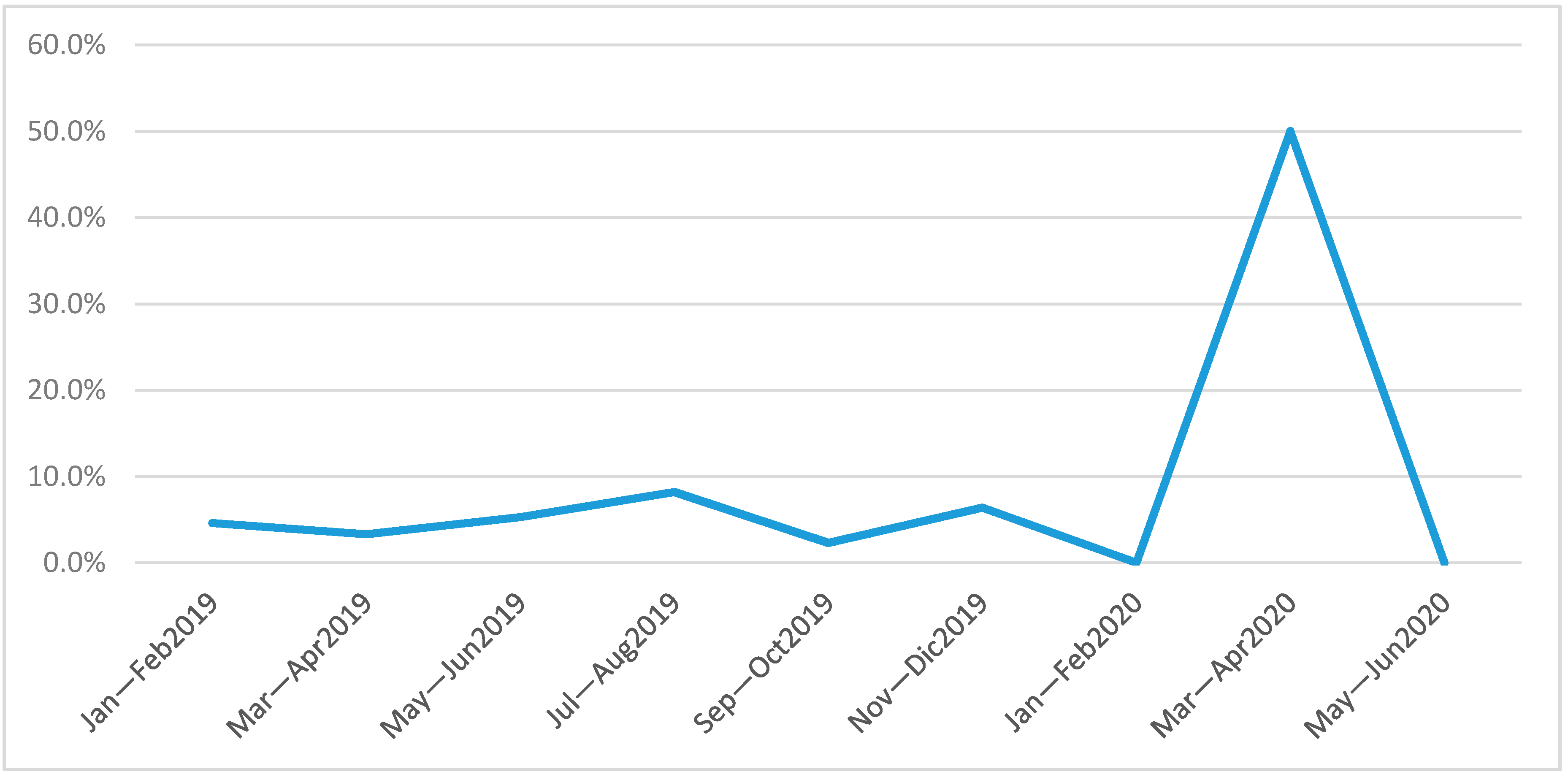
| Patients (Total) | CRE Colonized Patients (N) | CRE Colonized Patients (%) | Primary Cases (Patients) | Acquisition Cases (Patients) | % Acquisition Cases (Patients) | |
|---|---|---|---|---|---|---|
| Jan—Feb 2019 | 65 | 5 | 7.7% | 2 | 3 | 4.6% |
| Mar—Apr 2019 | 60 | 9 | 15.0% | 7 | 2 | 3.3% |
| May—Jun 2019 | 56 | 10 | 18.0% | 7 | 3 | 5.3% |
| Jul—Aug 2019 | 49 | 7 | 14.3% | 3 | 4 | 8.2% |
| Sep—Oct 2019 | 43 | 9 | 21.0% | 8 | 1 | 2.3% |
| Nov—Dec 2019 | 31 | 2 | 6.4% | 2 | 2 | 6.4% |
| Jan—Feb 2020 | 25 | 1 | 4.0% | 1 | 0 | 0.0% |
| Mar—Apr 2020 | 32 | 17 | 53.0% | 1 | 16 | 50.0% |
| May—Jun 2020 | 30 | 4 | 13.3% | 4 | 0 | 0.0% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiri, B.; Sensi, E.; Marsiliani, V.; Cantarini, M.; Priante, G.; Vernelli, C.; Martella, L.A.; Costantini, M.; Mariottini, A.; Andreani, P.; et al. Antimicrobial Stewardship Program, COVID-19, and Infection Control: Spread of Carbapenem-Resistant Klebsiella Pneumoniae Colonization in ICU COVID-19 Patients. What Did Not Work? J. Clin. Med. 2020, 9, 2744. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092744
Tiri B, Sensi E, Marsiliani V, Cantarini M, Priante G, Vernelli C, Martella LA, Costantini M, Mariottini A, Andreani P, et al. Antimicrobial Stewardship Program, COVID-19, and Infection Control: Spread of Carbapenem-Resistant Klebsiella Pneumoniae Colonization in ICU COVID-19 Patients. What Did Not Work? Journal of Clinical Medicine. 2020; 9(9):2744. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092744
Chicago/Turabian StyleTiri, Beatrice, Emanuela Sensi, Viola Marsiliani, Mizar Cantarini, Giulia Priante, Carlo Vernelli, Lucia Assunta Martella, Monya Costantini, Alessandro Mariottini, Paolo Andreani, and et al. 2020. "Antimicrobial Stewardship Program, COVID-19, and Infection Control: Spread of Carbapenem-Resistant Klebsiella Pneumoniae Colonization in ICU COVID-19 Patients. What Did Not Work?" Journal of Clinical Medicine 9, no. 9: 2744. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092744