Meeting the Spiritual Care Needs of Emerging Adults with Cancer


School of Theology, Philosophical Faculty, University of Eastern Finland, P.O. Box 111, 80101 Joensuu, Finland
Religions 2020, 11(1), 16; https://0-doi-org.brum.beds.ac.uk/10.3390/rel11010016
Submission received: 14 November 2019
/
Revised: 18 December 2019
/
Accepted: 24 December 2019
/
Published: 28 December 2019
(This article belongs to the Special Issue Spiritual Care for People with Cancer)
Abstract
:Every year 90,000 young people in Europe and the USA are newly diagnosed with cancer. The majority of earlier studies have taken a quantitative perspective, rarely focusing on the importance of religiosity and spirituality. From these premises, this narrative study explores the spiritual needs of emerging adults with cancer and suggests spiritual care practices that would benefit them in their shift to the remission stage. The data were obtained from the experiences of 16 emerging adults who took part in autobiographical interviews and drew life-tree drawings. Narrative-thematic and visual-narrative methods were used to interpret the data. The results show that spiritual needs manifest in multiple areas: existential questions, value-based searching, and religious seeking. Spiritual care should be targeted to issues such as identity, self-blame, understanding personal values, and relationship with God. Furthermore, family and partners should be supported and dreams of the future after cancer encouraged. The needs for spiritual care are manifold and these needs remain for years after the treatment ends.
1. Introduction
Cancer is not often considered as affecting young people. Yet, because of the high annual numbers of new diagnoses, it should be understood as a global health issue; every year 70,000 young people in the United States and 20,000 in Europe are diagnosed with cancer. (Vassal et al. 2014; Nass et al. 2015; Docherty et al. 2015) Cure rates are relatively high, with 80 percent of patients being cured (Vassal et al. 2014); still, cancer evokes strong psychosocial challenges and longitudinal distress that can follow decades after treatment (Grinyer 2009). Since the turn of the millennium, a growing body of research has examined the age-specific needs of young patients with cancer. Existing studies tend to focus on either the positive or the negative sides of cancer but only rarely are these aspects combined in one body of research (see Belizzi et al. 2012).
When running a review of existing research on religious/spiritual coping of young people with cancer, only a handful of studies were found (search in various databases for keywords such as “cancer”, “religious coping”, “meaning”, “meaning-making”, “young adults”, “emerging adults”; see Saarelainen 2016, 2017a). Interestingly, the majority of the studies found were quantitative (as noted also by Kent et al. 2012) and conducted in the context of the United States. This indicates the pressing need to strengthen European understanding of the role of religious and spiritual aspects in young people’s experience of cancer.
For those young patients who find spirituality meaningful, it is known that spiritual wellbeing correlates positively with psychological adjustment (Park and Cho 2017; Yanez et al. 2009). Being diagnosed with cancer seems to activate earlier belief systems (Jones et al. 2010); furthermore, some found a personal relationship with God through their cancer process (Saarelainen 2016). A relationship with God and personal faith can provide safety (Saarelainen 2016; Jones et al. 2010; Kyngäs et al. 2000, 2001) and alleviate loneliness (Ragsdale et al. 2014). Young cancer survivors found that cancer happened for a reason (Jones et al. 2010; see also Saarelainen 2017b) and a few believed that God had chosen to give the cancer to them (Saarelainen 2017b; Ragsdale et al. 2014). Young patients have appraised cancer as a meaningful part of personal identity (Saarelainen 2017a, 2017b) and for some, being treated for cancer has affirmed the purpose of life (Grinyer 2009; Ragsdale et al. 2014). Distress levels decrease when cancer is associated with a sense of meaning (Thomsen and Jensen 2007). Further, positive correlations have been found between the health-related behavior of young patients, religiosity, and spirituality (Park et al. 2009).
Religious and spiritual coping can contain an element of struggle. These struggles can lead to difficulties in the adjustment process (Park and Cho 2017) and misuse of alcohol (Park et al. 2009). Existential concerns arise when finding answers to the burning questions of why cancer happened or why God allowed it (Saarelainen 2016). Still it seems that in spiritual struggle, young people turn to God to solve these issues (Ragsdale et al. 2014). Even though the role of religion and spirituality in the cancer process for young people seems obvious, unmet needs for religious and spiritual counseling have been reported (Zebrack et al. 2014).
Earlier studies suggest that religiosity is more likely to appear in contexts where religious expression has space and significance (e.g., Ganzevoort 1998a; Pargament 1997). In Finland, the religious context has been highly homogeneous and the Evangelical Lutheran Church of Finland (ELCF) still holds the status of the majority church, although membership has declined to 69.7 percent of the population (ELCF 2019a). However, the number of young people defining themselves as atheist is growing, and 22 percent of Finns aged 15–29 identify as atheist (Palmu et al. 2012). Still, more than 90 percent of pupils take part in the Lutheran religious education that schools provide as part of their curricula (Vipunen 2019) and 80 percent of 15-year-olds participate in the confirmation schooling of the ELCF (ELCF 2019b). Belonging to the ELCF is still culturally acceptable for young Finns (Klingenberg 2014; Saarelainen 2018).
Based on the knowledge and gaps in earlier research, in this paper the spiritual needs of emerging adults with cancer is analyzed. As cancer and its treatment can impede the cognitive maturation of young people (Docherty et al. 2015), the term “emerging adult” to refer the participants who were between 18 and 35 years old during the study is used. As a concept, emerging adulthood refers to the changes and delays in the maturing process that have occurred in Western, well developed, countries (e.g., Arnette 2004; Parks 2011). It is shown that when spirituality is understood as a broad phenomenon, cancer arouses strong identity-related and value-based spiritual needs, as well as the need for religious support. Based on these findings, implications for spiritual care practices are drawn and it is demonstrated how these practices would benefit the young patients, including forgiveness interventions, supporting patients’ families, coaching for the future, and providing longitudinal support.
2. Data and Methods
2.1. Recruitment of the Participants
The Finnish Cancer Organization assisted in finding participants for the study. The organization granted permission to publish the advertisement in three of the chat rooms which it hosts, all of which were aimed at young people with cancer. As it was considered that chat rooms attract people who are actively seeking discussions, the Finnish Cancer Organization also sent the advertisement through their emailing lists for young patients. The aim was to recruit young people who had had cancer during the previous five years. As in the Finnish system young patients are understood as aged between 18 and 35 (Sonninen 2012), this definition of age was followed in the recruitment. Participants did not need to have any religious or spiritual convictions to be able to participate. People interested in the study were asked to send the author an email or phone in order to find out more or to sign up for the interview.
Altogether, the narratives of 16 participants formed the research data. However, 13 females and four males were interviewed. As one of the interviewees described having a benign tumor, it was considered that her situation was different to that of the others, so her interview was excluded from the main data. After 10 to 12 interviews, repetition and similarities began to appear in the meetings. Yet, it was considered ethical to interview all the volunteers even after saturation was reached. A few people who were willing to share their experiences via email; yet, when the email exchange came to the point of arranging an interview, these correspondents did not reply. It was considered that after two reminders, it was best to give people their privacy and they were not approached again.
As the participants had various types and stages of cancer1, in Table 1 the information about their condition is given in the words that participants used to describe it themselves.
The participants can be categorized into three groups based on the time from the treatment during the interview: one year or less (5), two to three years (5), and four to five years (6). Most of the participants were diagnosed with some type of serious lymphoma. All the participants had undergone curative treatment.
2.2. Data Collection
The one-time interviews were conducted after each interviewee’s treatment period had ended; still, most of them were in remission and attending regular check-ups and doctor’s appointments. One participant was interviewed twice; as she had an urge to talk soon after her diagnosis, she was interviewed both during her treatment and four months after it had ended. Interviews were conducted around Finland, as the interviewees were able to choose the location of the meeting.
As a growing body of literature shows that visual elements are particularly helpful in sensitive research topics, the aim was to identify a suitable visuality for the current study. Visualities are found to encourage verbalization, but also support the participants when words are not enough (e.g., Katz and Liat 2013; Keats 2009; Lev-Wiesel and Revital 2007; Pain 2012; Weber 2008). As several authors (e.g., German 2013; Gunnarson et al. 2006; Gunnarson et al. 2010; Hughes 2014) reported advantages when utilizing the shape of a tree with research interview, a life tree was designed for the purposes of the study.
The semi-structured interviews began with a visual task in which participants were asked “to imagine your life until today as a tree. What would it look like?”. Participants were encouraged to find their personal ways of drawing: they were told that the visualities were not going to be judged on their appearance. After the drawing, participants were probed about the elements, colors, and symbols of the tree. The visual assignment was followed by an autobiographical interview about the past, present, and future, as well as the relevance of spirituality and religiosity. Each interview covered the following main themes: childhood memories, narrative of their youth, narrative of their cancer, religion and worldview during different life stages, and views of the future. The length of the interview was approximately 90 min.
In addition to the interview, the meetings included general discussions on the research topic and goals as well as dialogue about the researcher’s interest in the subject. At the end of each interview, participants were asked how they felt after sharing their personal experiences of life with cancer. The researcher was equipped with phone numbers of local psychosocial support providers to secure the wellbeing of the participants. None of the volunteers expressed their need for this kind of support after the interview.
2.3. Analysis of the Data
As the research material included different types of datasets, it was important to discover analytical tools that would grasp the different layers of data. Qualitative studies have been categorized as providing “large amounts of detailed data”: by employing a thematic approach to the analysis, it is possible “to identify, make sense of and highlight the key themes in a rich qualitative data” (King 2017, p. 219). The research focus was to find out the content of “what” was said and how they made sense of life after cancer; a thematic analysis was employed. As the research setting was designed with narrative approach, it was reasonable to choose a narrative thematic approach to the analysis. The narrative application of thematic analysis aims to keep the stories “intact”, which gives the analysis process specific features (Riessman 2008, pp. 53–76). The analysis path is explained next.
The spoken interview data was analyzed with the method that Riessman (2008) calls “narrative thematic analysis”; it is close to what Lieblich (1998) defines as a “narrative holistic approach”. The interviews provided 414 pages of raw transcription, transcribed by the author. As accurate transcriptions are important when trying to grasp “meaning of what is said” (Mishler 1986, p. 47), laughter, tears, different tones, and pauses were recorded in the transcriptions. Furthermore, the text was divided intuitively into units of meaning: an extra line space was added when the interviewee shifted from one subject to another (see Riessman 2008, pp. 34–37).
As the unit of analysis was defined as making sense of life with cancer, the data as a whole was coded (see Riessman 2008, p. 53). The analysis was partly theory oriented, as the religious coping theories of Kenneth I. Pargament (Pargament 1997; Pargament et al. 1988, 1998) and Ruard Ganzevoort (1998a, 1998b) guided the understanding; yet, the author was not looking to consolidate a priori assumptions. Rather, these theories supported the analysis. In other areas, analysis was fully data-driven.
Open coding was employed for the analysis (see Benaquisto 2008, pp. 581–82) as follows: colored markers and short codes were used to follow each theme in the text. For example, narrations related to religious coping were underlined with a red pen and the code “RC” was written on the margin of the paper. In the coding process, changes in the storyline, unfinished thoughts, and disturbing matters were marked. The author tracked where the themes began and ended, and how they connected. After the transcript was fully coded, the case was read thematically, following specific characters and changes. The central themes were identified and used to form theme lists from each case. In the lists, the main themes were bolded, and subthemes were listed under each theme. First, the cases were analyzed one by one, and next the shared features were discovered (see Riessman 2008).
The drawings were analyzed after the texts, and the visual-narrative analysis included the following analytical steps (for the details see Saarelainen 2015; Rose 2016). First, the tree-related narration was identified from the transcripts and moved to an individual text folder. A general assessment of the drawing was made (such as “the tree seems healthy” or “there is no color other than black”). Then the coding of the drawings began by comparing the tree-related narration to the actual drawing. Participants’ own ideas about the drawing were coded, recording explanations of the colors, symbols, and spatial use of the paper. When the trees had been coded, the themes within them could be identified. The tree themes were compared with the holistic theme lists. It was found that some themes were accentuated, and other themes were left out. The visual-narrative analysis highlighted some themes: for instance, the significance of relationships became more tangible.
2.4. Ethics, Reflectivity, and Validity
From an ethical perspective, the research proposal was accepted by the board of doctoral studies at the Faculty of Theology, at the University of Helsinki. The interviewees’ rights and authors responsibilities as a researcher were discussed at the beginning of each interview when written consent forms were signed. Interviewees were also given an opportunity to withdraw at any time during the project. All participants were given fictional names, and identifiable items that could jeopardize the anonymity of the participants have been left out. High ethical standards were followed at all stages of the study and the criteria for qualitative health studies were discussed in both a pastoral theology research seminar and a focus group on narrative research methods (see Levitt et al. 2018; Tong et al. 2007).
Based on the email exchange, participants knew that the study was conducted at the faculty of theology; yet, it was highlighted that study was not related to any religious denomination. In addition, beforehand the participants knew that they would be asked to share their life story with cancer. The researcher seriously considered the extent to which participant involvement should be used due to the risk of re-opening old wounds. In order to reduce external stress on participants, it was decided to hold only one meeting. This decision was confirmed when one of participants wrote in their cancer-related blog that the interview was fruitful but they had felt tired for several days due to the intensity of the reflection process. Yet, two participants asked for (and received) their transcriptions in order to remember the interview. Further, as agreed, participants received a PDF copy of the doctoral thesis that was based on the interviews.
To secure the validity of research in all stages, the coding, analysis and formulations of results were shared, discussed, and negotiated with colleagues working in the field of pastoral theology. Although the process was independently led, groups of colleagues provided regular feedback. As it was considered crucial to follow and separate personal thoughts and emotions related to the topic, the researcher kept an in-depth field diary, writing down personal thoughts and reflections after each meeting.
2.5. Theoretical Framework: A Broad Concept of Spirituality
A broad definition of spirituality formulated by the European Association of Palliative Care (EAPC) is utilized in the article. As the EAPC’s main aim was to find a definition of spirituality that is usable in the European context and in healthcare settings, it was expected to be helpful for this study, even though the participants were not dying patients per se. As there are multiple ways of defining spirituality, the EAPC’s definition acknowledges that spirituality is hard to define as it carries multiple elements and angles, but clearly includes three categories.
First, spirituality includes existential questions. Aspects of “identity, meaning, suffering and death, guilt and shame, reconciliation and forgiveness, freedom and responsibility, hope and despair, love and joy” are given as examples of existentially relevant spiritual themes. Second, value-based considerations and attitudes are dealt as part of spirituality as follows: “the things most important to each person, such as relations to oneself, family, friends, work, things, nature, art and culture, ethics and morals, and life itself”. Third, spirituality includes personal religious considerations and attitudes such as “faith, beliefs and practices, one’s relationship with God or the ultimate”. (Nolan et al. 2011, p. 88.)
By following this definition of spirituality, the results section presents how emerging adults described their spiritual needs during their cancer process. The discussion addresses the question of what kind of spiritual care practices could have supported emerging adults in their cancer process.
3. Results
3.1. Existential Concerns Raised by Cancer
Among the interviewed emerging adults with cancer, the majority of spiritual needs were existential. In this section, it is first shown how their identity was challenged in terms of self and body image. Second, it is analyzed how relationships were experienced: on the one hand relations provided significant support, on the other, more worries. Third, it is shown how the fear of relapse and death impacted on participants’ views of the future.
3.1.1. Challenged Self and Body Image
Cancer affected emerging adults’ personal experience of self and body image. On the level of mind, being diagnosed with cancer challenged participants’ views of life. Cancer made many of the participants ask questions such as: Why? Why me? Why now? What does it mean to have cancer at this age? After the diagnosis, participants were often driven into a process of reasoning and searching for meaning for cancer. For some, this search included elements of self-accusation: reasons for cancer were found in their own actions as Anna described:
In Anna’s narrative she leaves a few words out of the description but leads the interviewer to understand that she had been drinking and kissing a stranger. Anna had been reading about possible biological causes of her cancer and found a study showing correlation between mononucleosis and her cancer type. Therefore, she found that her illness was an outcome of her behavior. Anna explains that she does not think actively about the relationship of her actions and cancer. However, it can be interpreted that her expression still includes personal guilt and a sense of shame reviles in her words “haven’t even told mom”. Like Anna, some participants were looking for a reason for cancer in their own actions and felt themselves responsible; a few participants found that their actions led to God’s punishment, as it is shown in Section 3.3.I haven’t even told mom about this… I’d just turned 18 and me and my friends had these nights in bars. So I’m guessing that from one of these nights I caught mononucleosis [after kissing a stranger], kissing disease… so one of these drunken nights led me to have cancer.
Furthermore, issues of body image challenged the experience of knowing oneself: losing hair, all the body hair, undergoing changes in weight, having physical scars that would never heal, all made it difficult to identify one’s own image in the mirror. In Sophia’s narrative, questions related to identity were made visible as she drew a tree only half-covered in leaves and explained (Figure 1):
The time with cancer was somehow rough. Still, it [cancer] doesn’t fully cover the tree. It is there but it doesn’t master the tree. And there is a fruit, an apple that shows that something new is mellowing there and new life. It [cancer] doesn’t master [the tree], it is with it, but it doesn’t interfere with the growth otherwise.
Four years after treatment, Sophia described how cancer had become a part of her without negatively impacting on her way of life. As Sophia’s cancer was found in her knee, she had to undergo a long period of living with fear of losing her leg and limping. Sophia, and other participants who had had surgery that changed their physical abilities permanently, shared the experience of the long process of accepting their changed body image. Further, both Sophia and Chloe stated that the cancer diagnosis was like “end of a fairytale”. By this they meant that life before cancer was smooth and childlike; cancer forced them to become adults and made them see their personal vulnerability and limitations.
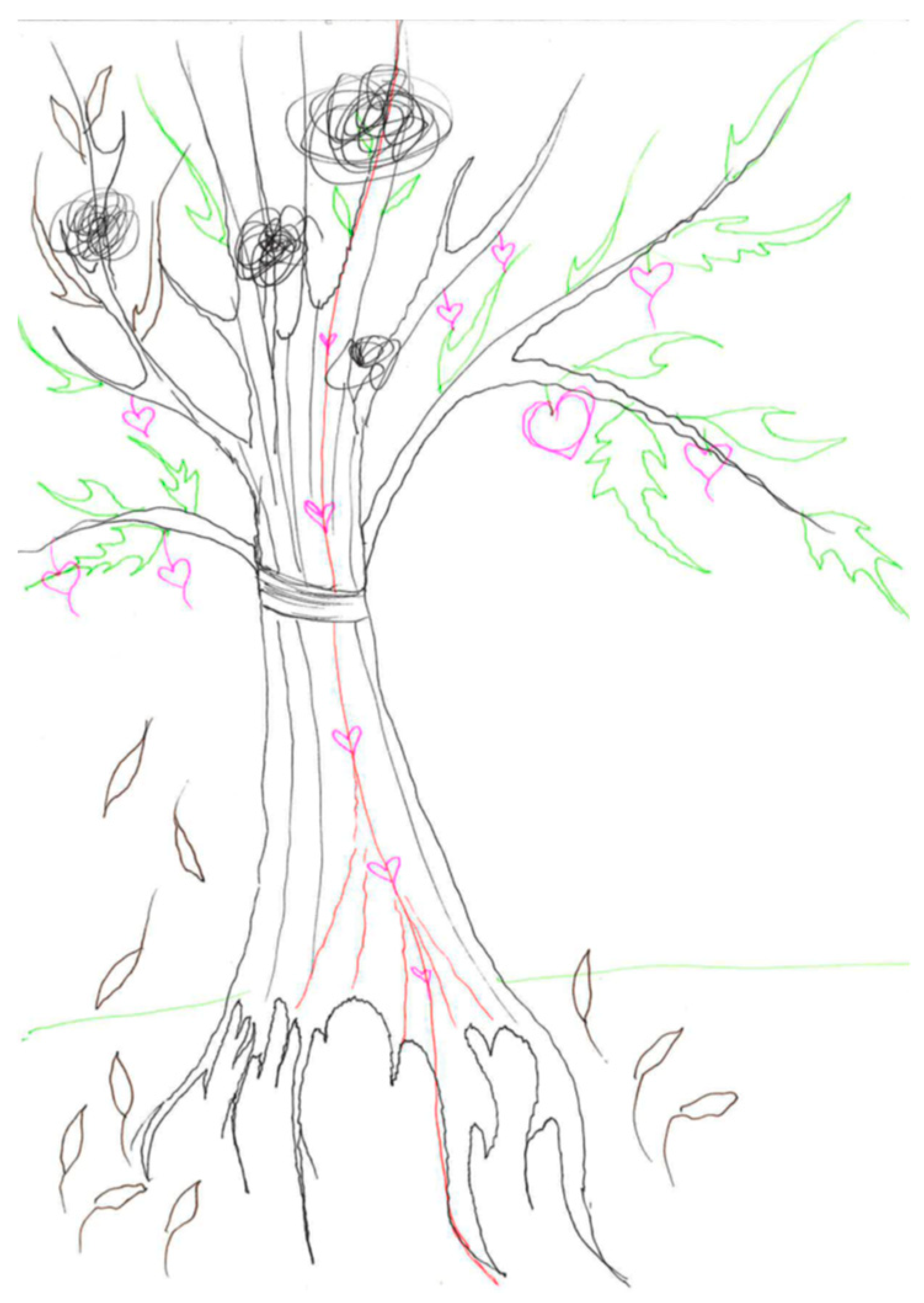
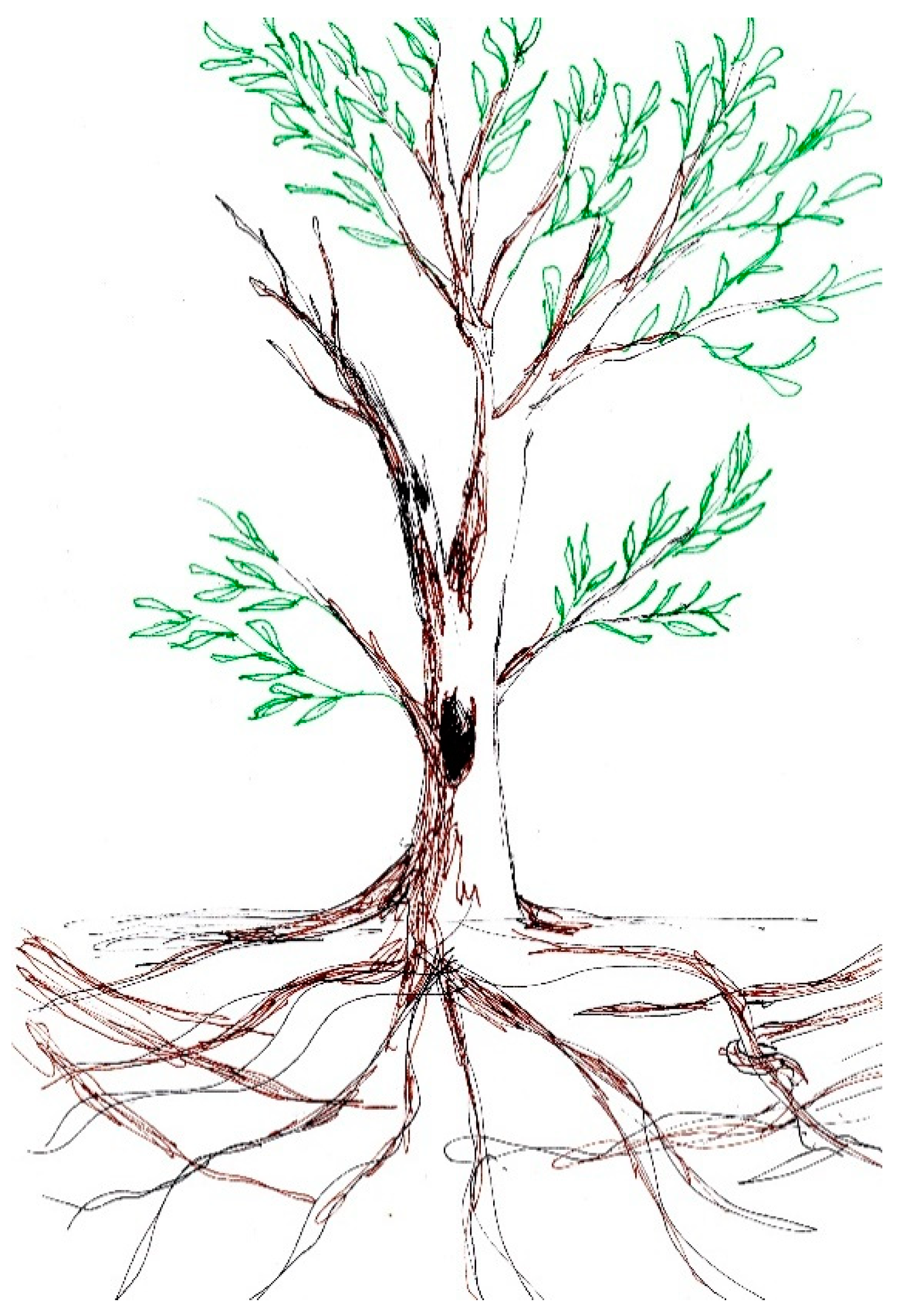
As noted, cancer holistically challenged experiences of self; yet, cancer was often found to have benefits. For instance, Sarah said that “it [cancer] is the worst thing that has happened to me, but on the other hand, it is the best. Would I be me without this experience? As pearls are ground in the sand, so was I”. In Sarah’s drawing (Figure 2), this dualism of cancer is made visible: green leaves and new growth symbolize the growth followed by the cancer; however, scars in the tree trunk and black leaves point to the long-term wounds caused by cancer.
Sarah seems to have found her cancer empowering as, because of it, she reconsidered her values and found her true self. Sarah and a few others stated that they found explicit meaning for cancer in self-growth; cancer gave the emerging adults a chance to reconsider their personal values and ways of life. Often the participants who found identity-related changes meaningful found the courage to live life the way they truly wanted.
3.1.2. Relationships as (Dis)Encouragement
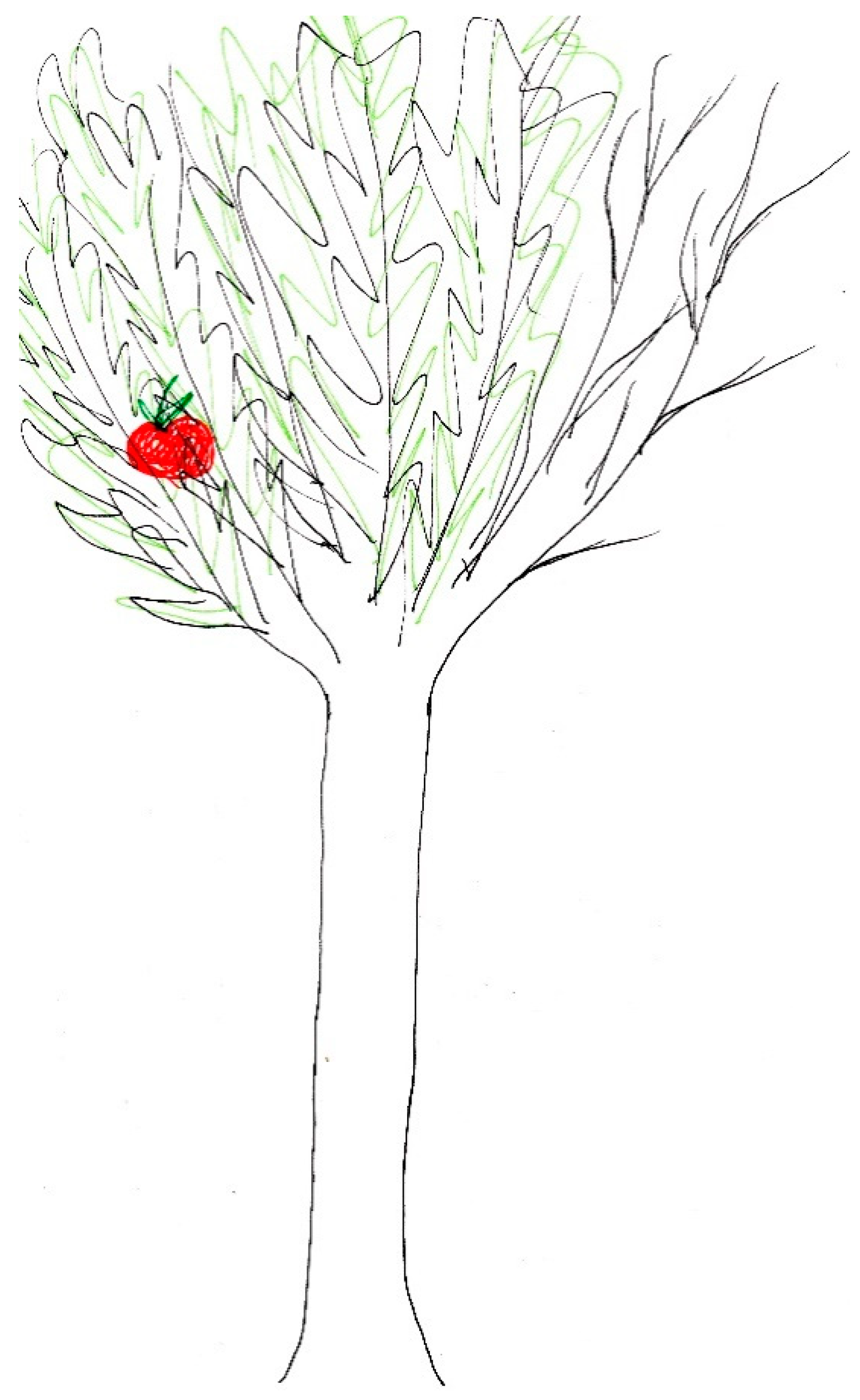
Close relations provided much needed hope in the form of love and acceptance during the cancer process. With families, partners, and close friends it was possible to choose when to discuss and process cancer and when to take a break from ongoing cancer thoughts. For some, cancer brought new people into their lives, so it was difficult to consider what life would have been like if cancer had not happened. For instance, Emily depicted the importance of new relationships by saying: “without the cancer I wouldn’t have met my best friends or my boyfriend… It is really hard to imagine what [it would have been like] if it hadn’t happened”. Tom found relationships with his girlfriend and family important. In Tom’s drawing (Figure 3) the roots are particularly strong.
Tom explained the significance of the roots by saying “the tree is not alone” and a close look at the drawing shows how the roots of the nearby trees hold the tree up. In the midst of challenges, close relations brought the comfort of facing difficulties together. For many, this comfort and strengthened relations provided meaningfulness for cancer.
Yet, the close relationships were narrated in another tone: one of protection and the need to maintain a certain distance. Many of the emerging adults felt that cancer was such a heavy burden on their family members that they felt the need to keep their most painful thoughts to themselves. It seemed that the most difficult questions were faced in romantic relationships, as Olivia described:
Olivia’s quotation shows how strongly cancer impacted on the couple; it also illustrates how people go through cancer thoughts at different paces and the spouse could not handle Olivia’s fear of death. During her treatment, her spouse left for a couple of weeks in order to clear his head. Meanwhile, Olivia was confronted with the thought of being abandoned by her spouse while being terrified of cancer. When they sought couple counseling, the counselor dismissed their issues by saying: “you are young, you’ll sort this out as [you have sorted] all other problems”. Still, for Olivia close relations, including her spouse and his mother as well as her own mother, formed the most important source of mental support.Cancer is not good for your relationship. Somehow it is really hard… my spouse has panicked. A few times he has been ready to take off… Somehow, he believes that I’ll get through this. But no one can speed up my journey.
Fear of social exclusion was described in more formal relationships. For instance, Macy regretted telling her work colleagues about her cancer: “If it is possible, I’m not going to tell [anyone] about this [cancer] at the new workplace”. Macy preferred to keep the information to herself as she did not want to be “the girl with cancer”. Macy’s thought can be interpreted as including shame and fear of social exclusion. Similar thoughts and fears were found among those patients who went back to school after being treated for cancer; the fear of being bullied at school provoked distress.
3.1.3. Fear of Relapse and Death
The fear of death was particularly strong during the treatment period, as for some, the probability of cancer leading to death was high. Still for most interviewees, only after treatment did the reality that “I could have died” hit, as during treatment, all the energy had to go into getting better. It was confusing that when the remission period began, participants were expecting joy and return to their daily life; yet, at this point, new crises emerged as the existential concerns about death and dying had to be faced.
Many of the participants described their views of the future as dualistic as they felt that it was highly likely that their cancer would relapse. For instance, Emma said: “I am not sure if it makes any sense to stress about studying if it [the cancer] relapses”. She would love to focus only on time with friends and family and not worry about her studies in case of a relapse. At the same time, she was hoping to stay cancer free and continue planning further ahead into the future. A year after her treatment, Emma was puzzled about how to organize her daily life and what kind of attitude she should have to her cancer. Still, distance in time from the treatment did not explain the dualism for everyone. For instance, Sarah found her future very unpredictable, and five years after treatment she concluded:
Sarah’s hesitation about the future is also made vivid in her drawing (Figure 2), in which she leaves the top of the tree undrawn. Even though Sarah found cancer to be an important factor that shaped her identity, the illness impacted strongly on her views of the future where death is somehow present. Around half of the participants found that cancer yielded this dualism about the future. The emerging adults found that they could have a happy and fulfilled life; yet, they were concerned about relapse or secondary disease, and early death because of it. Often the fear of relapse and despair peaked when heading for doctor’s appointments and remission check-ups.I am afraid to think about [the future]. So at this point, if I consider all the things my body has gone through …even if there were no relapse… In some scenarios I go earlier than in others. In some scenarios I’ll have a relapse, and in other scenarios I’ll have these unpleasant secondary diseases.
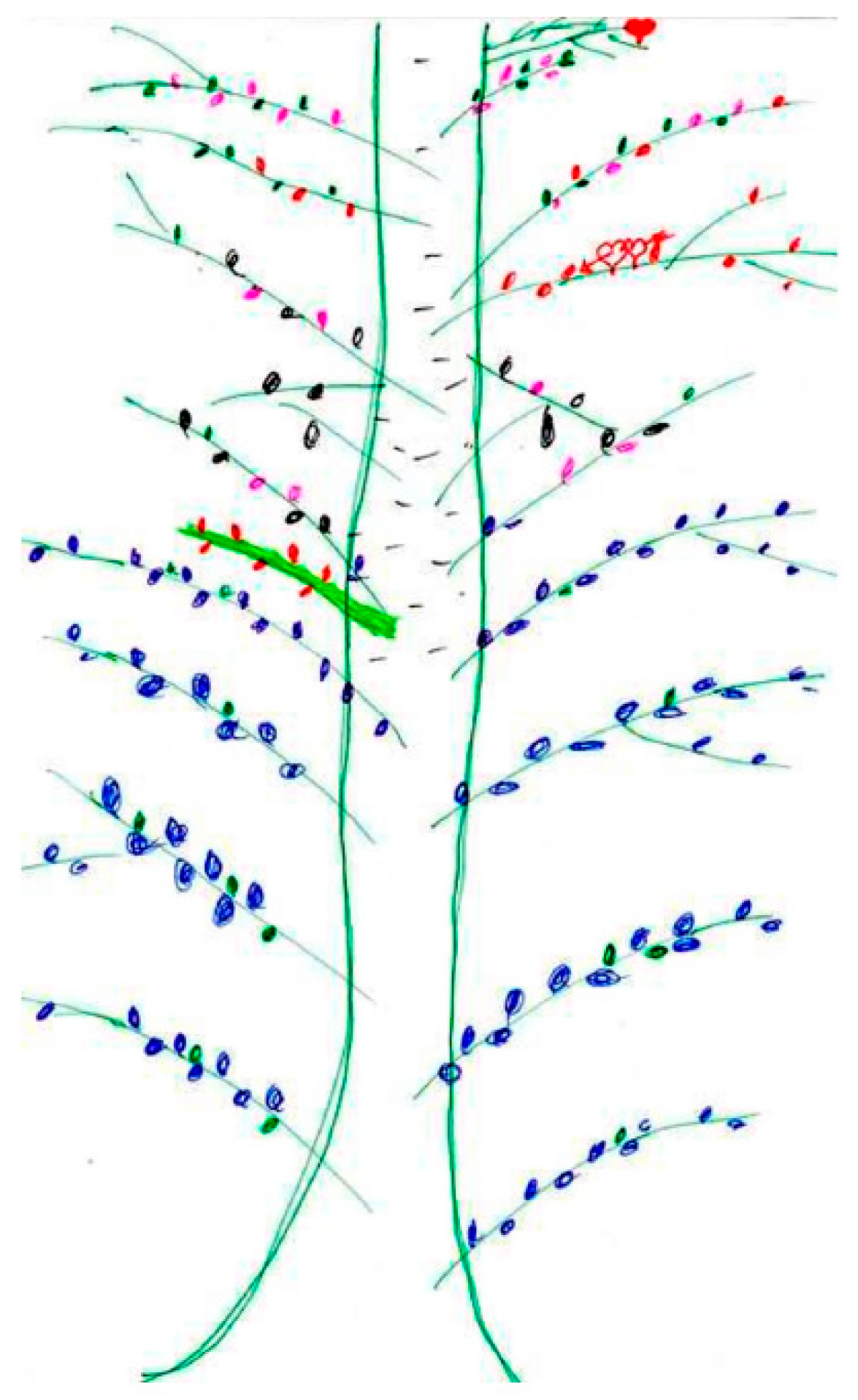
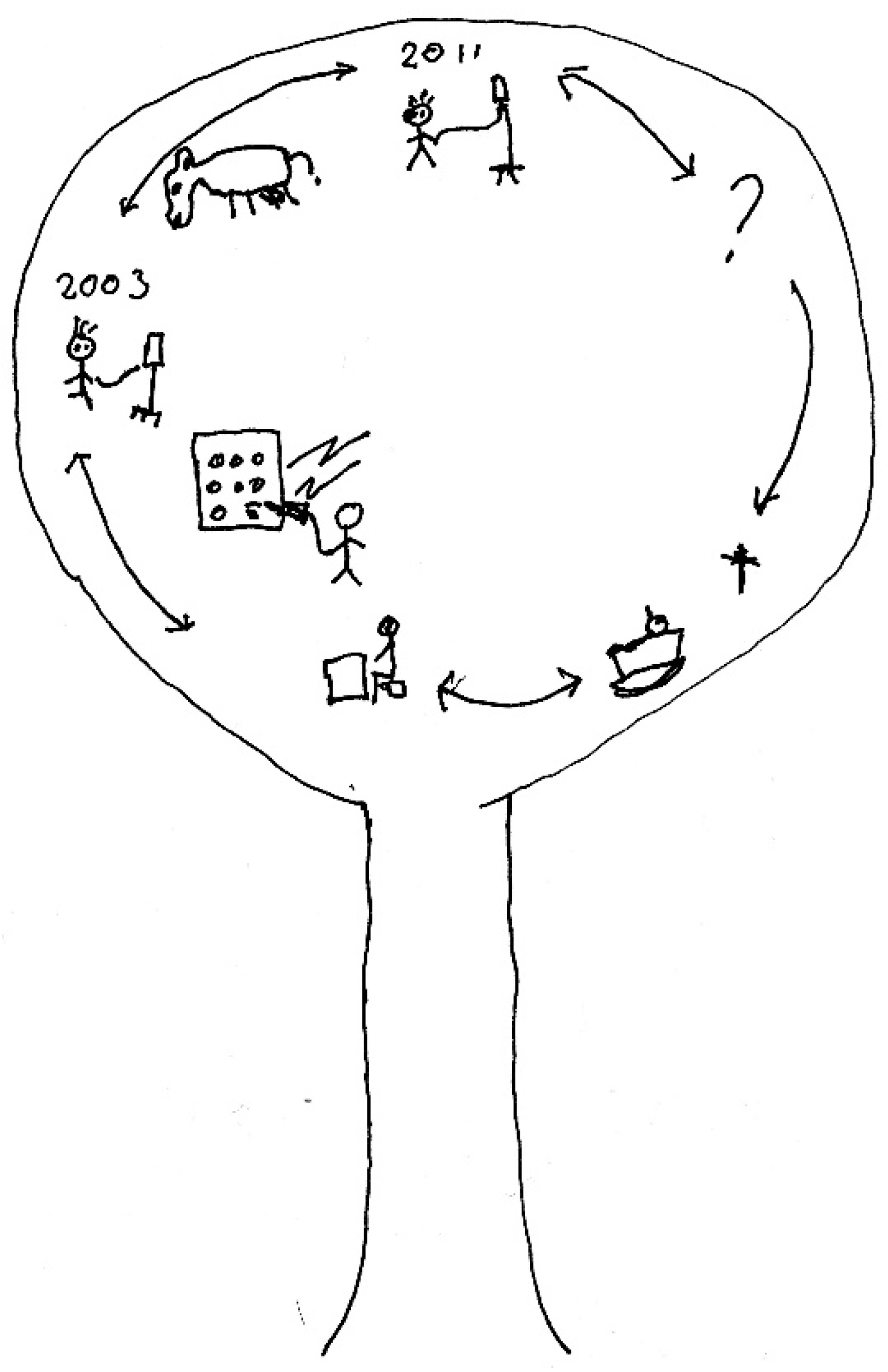
A few interviewees whose treatment had recently ended found it difficult to discuss the future as they were trying to portray their situation with cancer. This is vividly expressed in John’s drawing (Figure 4) and narrative, as he explains that the only thing he knows for sure is that at some point people will die, and no one knows the number of days they have left.
In his drawing, a cradle which symbolizes birth is placed next to cross that stands for death. The placement of birth and death symbolizes his view that both being born and dying are a natural part of life. Many of the participants described how awareness of death had given them a stronger understanding of the value of life. Death was understood as a natural part of being human.
3.2. Value-Based Spirituality
Many emerging adults described how their values changed after the cancer diagnosis. In this section, change of values is shown in two different terms: as living in the moment and as changing career or study path.
First, the ability and willingness to live in the moment was often expressed as a positive outcome of cancer. For instance, Mark explained that he had been searching and considering what would be the right way to live one’s life. After being diagnosed with cancer, he read Eckhart Tolle’s book The Power of Now: A Guide to Spiritual Enlightenment and felt that he had found the guide to a good life. He said: “My view has changed, and I don’t make plans like I used to. Rather, it is images of being in the present”. His life-tree drawing is extremely reduced as he only draws two clean lines for the trunk and the green foliage part is drawn with one uniform line (Figure 5).
Mark explained that if he had drawn the tree earlier in his life, it would have been different: there would have been shoots and branches for different areas of life. However, he saw that everything in life forms one entity and it would not be appropriate to divide the tree into parts. Mark’s descriptions outline his stronger will and ability to live in the moment. He had found a balance in life itself as well as balance between his personal life goals, family life, and work. Cancer provided many of the emerging adults with calm time for personal reflection. These narratives of halt included experiences of being relieved because participants felt that when discovering personal values, they were released from external pressures to live in a certain mold.
Second, following the contemplative time and self-reflection, there was a strong tendency to find a new career after cancer treatment for many. More than third of the participants narrated that because of their cancer they found their calling or dream career. For instance, Chloe, who was planning to become a professional dancer before cancer, described how the illness impacted on her career selection:
In Chloe’s case, the cancer led to finding a meaningful career. The idea of providing support for others was shared by participants who found a career path related to care work. For some, self-reflection on work provided an opportunity to change the area within their own field. These shifts were made to improve their work-life balance, as Anna narrated: “I know that I’ve been living in a constant hurry... I want to give up that hurry. If I work as a teacher, I don’t have to be available all the time”. The idea of a calm pace at work was linked to participants’ wish to have more time for taking care of themselves and their relationships. More generally, cancer had clarified the value of health for the participants.The credit for finding my study field goes fully to this cancer. I would never have begun to study Occupational therapy if I hadn’t fallen ill. Having this personal experience in the background, being really functional and active in my life and then losing it. It’s like suddenly you are unable to do the stuff that is important to you. So I realized that I want to be in a job in which I can help people in the situation where their physical abilities are restricted.
3.3. Religious Coping and Appearance of Spiritual Seeking
In their narratives, it became clear that the Finnish context impacted on emerging adults’ religious coping with cancer. When discussing their worldviews, values, and self-understanding of personal religiosity, many participants explained their religiosity as the “normal Finnish” way. This expression can be found to include the importance Christian rituals (baptism, confirmation, marriage, funeral) and attending church at Christmas.
The first appearance of religion in the cancer process was negative, as religious struggles often emerged in the beginning of the cancer process. A third of participants encountered why-questions in form of asking “why God allowed” this to happen. For some, these questions included thoughts of doing “evil” deeds. For instance, Beth found that she was given a cancer relapse at the age of 22 so that she would “reconsider her values and way of living”. In contrast Sarah, who defined herself as Christian, could not figure out what she had done wrong in her life, but found an explanation in the thought of doing something wrong in her previous life. She was convinced that “I must have been Hitler’s right hand” in a former life in order to “deserve” cancer. These examples show that religious struggles included the aspect of seeking an answer in one’s own actions.
Religious coping and seeking often became visible in relation to praying. Cancer had triggered a process in which participants turned to God, even if they were not sure who they were turning to, as Olivia explained during her treatment process:
In adolescence, I found myself strongly Christian… now for few years, before the illness, I’ve had this idea that it [faith] grows from inside an individual… this thought was not ready before the illness… but I don’t need a book or religion to define faith, it has to come from inside me… I wouldn’t say I’m particularly Christian… Somehow the illness has made me turn more to my Christianity. More or less, I’ve been praying… It feels really good to know that people have been praying [for me].
Four months after the treatment, she said, “My thoughts are pretty much the same as they were last time we met. So I’m a Christian”. Olivia’s narrative makes visible how her religious process proceeded during the cancer. The beginning of treatment included questioning related to religiosity and Christianity; after the treatment some questions were raised, yet she is much more convinced of her Christianity. For many, the cancer impacted on their willingness to clarify their personal relationship with God. Altogether, few participants identified as Christian and more than half believed in a higher power or universal God that brings all the world religions together. A few of the participants did not know what to believe or identified as atheist. For Anna, seeing and going through suffering with cancer intensified her unbelief.
Even though religious seeking was common among the participants, they rarely portrayed religious experiences in their life trees. The only religious symbols can be found in the drawings of John (Figure 4) and Ava (Figure 6). Ava captured her worldview in the drawing in the form of a red thread. The thread runs through the tree and mainly symbolizes her self-confidence and inner power. Later in the interview she adds that the thread also stands for “the trust that life will take care of you… it could be defined as faith. The thread is some sort of faith”. Ava’s search for faith is a process of construction and in the interview, she is trying to find words to grasp her worldview by explaining: [I believe in] some kind of divinity… whether it is life itself or nature… I don’t think it is any person. I’m not going to define what it is or isn’t. It is something bigger, something that brings all the people and animals together”. John’s drawing, in which the cross symbolizes death, can also be seen as related to his Christianity when he defines himself as a “more secularized Christian”.
More than half of the participants described that praying brought security and consolation. Praying and intercession were the most-often described religious coping rituals. Thea described frequent praying: “I had my evening prayer and then several prayers during the day”. Prayers were often said at nighttime or before treatment if one was feeling scared. As Olivia expressed, many participants experienced affection and comfort in the knowledge that their friends and family were praying for them. Personalized religious rituals which took the form of tactile elements were described by a few. For instance, Chole and Thea had small angel figures and Sophia had a blessed linen cloth; they carried these items to treatment and kept them in safe places at home. These participants found that God’s guidance and protection was concrete through these artifacts.
Even though religious activation and seeking can be seen as intense among the interviewed emerging adults, only a few received pastoral care or spoke to a hospital chaplain. For instance, John, who was going through bone marrow transplantation after his cancer relapsed, explained that the chaplain came to visit him regularly to discuss “ordinary matters” and by this John meant that they did not discuss religious or spiritual matters, or the possibility of death. Thea, whose condition was extremely serious, also reported having pastoral care and realized in the interview that she “would have needed much more” of that kind of support.
4. Discussion: Multilayered Needs for Spiritual Care Require Manifold Practices
This paper shows that being diagnosed with cancer raises multiple spiritual questions and the call for spiritual care is multilayered. In this section, the results are discussed in relation to the findings of earlier studies, demonstrating what kind of spiritual care practices could have been beneficial for emerging adults living with cancer. As the results are based on limited data, the clinical implications rather form a hypothesis of what could be improved. These results cannot be generalized; yet, further quantitative studies are needed to establish consensus on the multilayered needs for spiritual care.
The participants often raised identity-related issues: being diagnosed with cancer challenged their images of self and body. Furthermore, their future dreams were often shaken. Even though many of the participants reported meetings with psychological support, individuals often found that they actively needed to seek out such support for themselves. As studies indicate that the age-specific needs of young patients are rarely met, spiritual and holistic care should target issues such as self-esteem, emotions, and social challenges, and comprehending changed body image and physical legacy, as well as supporting the experience of control over one’s life (see Grinyer 2007, 2009; Park et al. 2014; Nass et al. 2015; Warner et al. 2016; Walker and Lewis 2016). One basic improvement would be providing this type of care automatically: when coming to hospital for cancer treatment, one could have a scheduled appointment with psychological and/or spiritual support provider. As these participants described, they had to conserve energy to go from one cancer treatment to another; their minds were too busy to consider other options. In the Finnish system, support is often provided with a leaflet of phone numbers one can contact if needed. Is this really a task for a patient in crisis or should the first suggestion for support come from a professional?
When looking a reason for cancer in their own deeds, it can be suggested that the participants could have benefited from dealing with their self-blame and religious struggles more directly. Self-blame is often strongest in the beginning of the cancer process. As self-blame may be expressed in self-accusations and self-hate, the appearance of blame lowers the experience of quality of life and increases psychological stress. (e.g., Toussaint et al. 2017, 2014; Friedman et al. 2010; Romero et al. 2006.) Forgiveness interventions have been shown to impact on quality of life among cancer patients. If one is unable to face difficult questions, negative emotions can intensify and cause various unwanted outcomes such as shaken physical and mental balance. (e.g., Worthington 2014, pp. 7, 8, 17, 43; Hook et al. 2012, p. 687.) Further, participants needed spiritual support to understand the religious side of cancer. In theoretical terms, participants described spiritual discontent and error of religious explaining when trying to interpret their personal actions as a source of cancer (Pargament 1997, p. 328; Pargament et al. 1998, p. 523; see also Saarelainen 2016, p. 80). Yet in pleasant situations, religion offers a channel to increase cancer patients’ quality of life and decrease their levels of stress (e.g., Friedman et al. 2010, pp. 343, 345–47). Therefore, support to face religious struggles would have been needed. Often the participants in this study experienced religious and spiritual seeking but only a few discussed this with a chaplain. Perhaps participants were not aware that the ELFC’s hospital chaplains are trained to meet the needs of people with a range of worldviews (see Saarelainen et al. 2019). In all cases, there should have been open discussion of religious and spiritual issues at the hospital. Yet, often the participants reported that the interview was one of the first more formal discussions of the topic.
Challenges and special meaning were entangled in the close relationships of emerging adults with cancer. These phenomena were largely identified in previous studies that show how cancer challenges a young patient’s social network; at the same time, relationships are needed to experience of wellbeing. Supporting the relational network of young patients is crucial to their holistic wellbeing, as social isolation seems to promote behavioral problems in terms of smoking, alcohol misuse, and risky sexual behavior (Patterson et al. 2015). Overprotectiveness of parents or partners have been reported, as well as abandonment by friends. Romantic relationships are especially on the line, as intimate and sexual relationships are found to be challenging and divorce rates among young cancer survivors are higher than in the average population. (Kent et al. 2012; Docherty et al. 2015; Warner et al. 2016.) Therefore, spiritual care should always include support for families and partners. Based on the participants’ needs to protect their nearest and dearest, separate counseling sessions for patients and family members should be considered.
Education was described from two perspectives; participants expressed hesitation about going back to school and eagerness to discover a meaningful career path. These findings echo studies showing that young patients find returning to school education challenging (Patterson et al. 2015); yet, the majority of young patients discover positive changes after cancer (85% in Barakat et al. 2006; 88.5% in Yi et al. 2015). As these experiences are partly conflicting, young patients might find ease if their change of values and wishes for the future can be processed. For instance, at the counseling sessions, the value compass method provides an opportunity to identify, review, and reflect on personal values as well as to plan the steps to take so as to be able to live according to one’s personal values. The value compass is also one way to move thoughts and discussions toward perspectives on the future. (e.g., Hayes et al. 2012; Dahl et al. 2009.) If the dimension of the future is neglected in spiritual care, an individual’s experience cannot be fully understood: if one stays frightened about the future, despair is likely to arise. Therefore, spiritual care should address fears for the future and buffer dreams of the future. (Lester 1995; see also Saarelainen 2019.) If values, future views, and goals were explicitly processed at counseling or with a support provider, hypothetically this should support patients in forming positive views of the future.
Often, it was only after treatment that the emerging adults felt ready to face the seriousness of their situation; yet, at this point they had returned home and the support networks of hospital were not available. As the salience of death demands a long process of reflection, spiritual care and counseling about thoughts of death and dying should be timed for the remission period. It is suggested that young people take at least a year to form an understanding of the salience of death (Little and Sayers 2004). As also reported by the participants in this study, Grinyer (2009) found that people who saw death as a natural part of life appreciated life in general more and were more aware of the value of their current lives. Yet, the key to successful support lies in its continuation. The support offered by the hospital should extend into the remission period. If trust for a support provider is gained during the treatment period, the individual should be entitled to continue counseling and discussions with the same person after changing status from inpatient to follow-up patient. If no support contacts are made during the treatment, the beginning of remission is a crucial opportunity to re-suggest counseling support.
The centricity of long-term support can be seen from two perspectives. First, the emerging adults interviewed for this study described how the crises of the remission period took them by surprise. Second, even five years after treatment, fears of relapse existed. Studies indicate that transition to survivorship is a significant crisis for young patients and that this shift is often neglected by care facilitators (Kwak et al. 2013); the experiences of being abandoned and feeling unsafe arise in the transition to remission (Patterson et al. 2015; Walker and Lewis 2016). To support wellbeing, counseling meetings should be regular, at least once every six months for the first five years of survivorhood (Thomas et al. 2010). Clinical distress has been shown to peak one to two years after treatment; yet the distress can occur even 20 years afterwards (Sansom-Daly and Wakefield 2013) and other long-term negative effects have been reported more than 30 years later (Grinyer 2009). In sum, for young patients with cancer, multilayered needs for spiritual care begin from the first brush with cancer and are likely to continue decades after treatment. Therefore, the counseling meetings would need to address the personal needs of each individual. As religion and spirituality are in flux and go through changes during one’s life span (e.g., Ganzevoort 1998a, 1998b), cancer-related spiritual questions are likely to vary over the years in response to personal life events.
5. Summary
When spirituality was understood as a broad concept defined by the EAPC, multiple needs for spiritual care were identified among emerging adults with cancer. On the level of existential issues, they had questions related to experience of self and body image; in the relational sphere, they found relationships both encouragement and burden. When encountering fear of relapse and death, the interviewees were confronted with personal mortality. These needs which interviewees identified are related to nearly all the aspects defined by the EAPC as existential considerations: spirituality from the viewpoint of identity, meaning, suffering and death, guilt and shame, reconciliation and forgiveness, as well as hope and despair, love, and joy. Thus, the cancer process is deeply existentially moving. Value-based considerations of spirituality can be defined as “the things most important” to an individual, including elements such as oneself, family, and work. This paper focused on important changes reported by the participants: the key issues for them were the ability to live in the moment and finding a new career path. Both these expressions, living in the moment and discovering a new career path, can be viewed as a new understanding of what is important in life, which changed values and everyday living. Participants expressed religious considerations of spirituality as activation of religious coping and spiritual seeking. God or a higher power was often turned to in their search for peace and security.
The EAPC’s broad definition of spirituality made it possible to comprehend the many forms of spirituality aroused by cancer. Spirituality among the interviewed emerging adults with cancer was a truly manifold phenomenon. Yet, each aspect of spirituality that the interviewees presented was linked to other aspects. Sometimes, religious considerations were entangled with why-questions and self-blame. Relationships were found to have existential relevance; as they became more central in the value system of an individual, relationships were also linked to value-based spirituality. These notions show that spirituality is both complex and in flux.
6. Limitations
It is acknowledged that the discussion is based on a limited set of qualitative data and therefore generalizations should not be made. The value of the presented narrative descriptions lies in the insights into the cancer experience and everyday life with the disease which they offer readers (see Flyvberg 2004). Based on the findings, it can be suggested that further mixed-methods studies are needed in order to measure spiritual care needs and to be able to make more extensive policy recommendations.
Funding
This research was funded by the Finnish Cultural Foundation under grant numbers 00120807; 00131822; 00160024, the Church Research Institute, the Olvi Foundation, and the Olga and Vilho Linnamo Foundation.
Acknowledgments
Auli Vähäkangas and Heikki Ruismäki for support in the project. Kate Sotejeff-Wilson for the language editing. Finnish Cancer Association and Sylva Ry for co-operation.
Conflicts of Interest
The author declares no conflict of interest.
References
- Arnette, Jeffrey Jensen. 2004. Emerging Adulthood. The Winding Road from the Late Teens through the Twenties. New York: Oxford University Press. [Google Scholar]
- Barakat, Lamia P., Melissa A. Alderfer, and Anne E. Kazak. 2006. Posttraumatic growth in adolescent survivors of cancer and their mothers and fathers. Journal of Pediatric Psychology 31: 413–19. [Google Scholar] [CrossRef] [PubMed]
- Belizzi, Keith M., Ashley Smith, Steven Schmidt, Theresa H. Keegan, Brad Zebrack, Charlie F. Lynch, Dennis Deapen, Margarett Shnorhavorian, Bradley J. Tompkins, and Michael Simon. 2012. Positive and negative psychological impact of being diagnosed with cancer as an adolescent or young adult. Cancer 118: 5155–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benaquisto, Lucia. 2008. Open coding. In The Sage Encyclopedia of Qualitative Research Methods. Edited by Lisa M. Given. Thousand Oaks: Sage E-Books, pp. 581–82. [Google Scholar] [CrossRef]
- Dahl, JoAnne, Jennifer Plumb-Vilardaga, Ian Stewart, and Tobias Lundgren. 2009. The Art and Science of Valuing in Psychotherapy: Helping Clients Discover, Explore, and Commit to Valued Action Using Acceptance and Commitment Therapy. Oakland: New Harbinger Publications. [Google Scholar]
- Docherty, Sharron L., Mariam Kayle, Gary R. Maslow, and Sheila Judge Santacroce. 2015. The adolescent and young adult with cancer: A developmental life course perspective. Seminars in Oncology Nursing 31: 186–96. [Google Scholar] [CrossRef]
- ELCF. 2019a. Available online: https://evl.fi/tietoa-kirkosta/tilastotietoa/jasenet#2cbf3cda (accessed on 18 December 2019).
- ELCF. 2019b. Available online: https://evl.fi/plus/seurakuntaelama/kasvatus/rippikoulu/tiesitko- (accessed on 18 December 2019).
- Flyvberg, Bent. 2004. Five misunderstandings about case-study research. In Qualitative Research Practice. Edited by Clive Seale, Giampietro Gobo, Jaber F. Gubrium and David Silverman. London: Sage, pp. 390–405. [Google Scholar] [CrossRef]
- Friedman, Lois C., Catherine R. Barber, Jenny Chang, Yee Tham, Mamata Kalidas, Mothaffar Rimawi, Maria Dulay, and Richard Elledge. 2010. Self-blame, self-forgiveness, and spirituality in breast cancer survivors in a public sector setting. Journal of Cancer Education 25: 343–48. [Google Scholar] [CrossRef]
- Ganzevoort, Ruard. 1998a. Religious coping reconsidered part one: An integrated approach. Journal of Psychology and Theology 26: 260–75. [Google Scholar] [CrossRef]
- Ganzevoort, Ruard. 1998b. Religious coping reconsidered part two: A narrative formulation. Journal of Psychology and Theology 26: 276–86. [Google Scholar] [CrossRef]
- German, Mala. 2013. Developing our cultural strengths: Using the “Tree of Life” strength-based, narrative therapy intervention in schools, to enhance self- esteem, cultural understanding and to challenge racism. Educational and Child Psychology 30: 75–99. [Google Scholar]
- Grinyer, Anne. 2007. Young People Living with Cancer: Implications for Policy and Practice. Buckingham: Open University Press. [Google Scholar]
- Grinyer, Anne. 2009. Life after Cancer in Adolescence and Young Adulthood: The Experience of Survivorship. New York: Routledge. [Google Scholar]
- Gunnarson, A. Birgitta, Jansson Jan-Åke, and Eklund Mona. 2006. The Tree Theme Method in psychosocial occupational therapy: A case study. Scandinavian Journal of Occupational Therapy 13: 229–40. [Google Scholar] [CrossRef]
- Gunnarson, A. Birgitta, Peterson Kerstin, Leufstadius Christel, Jansson Jan-Åke, and Eklund Mona. 2010. Client perceptions of the Tree Theme Method: A structured intervention based on storytelling and creative activities. Scandinavian Journal of Occupational Therapy 17: 200–8. [Google Scholar] [CrossRef]
- Hayes, Steven C., Kirk D. Strosahl, and Kelly G. Wilson. 2012. Acceptance and Commitment Therapy. The Process and Practice of Mindful Change, 2nd ed. New York: The Guilford Press. [Google Scholar]
- Hook, Joshua N., Everett L. Worthington, Shawn O. Utsey, Don E. Davis, Aubrey L. Gartner, David J. Jennis, Daryl R. Can Tongeren, and Al Dueck. 2012. Does forgiveness require interpersonal interactions? Individual differences in conceptualization of forgiveness. Personality and Individual Differences 53: 687–92. [Google Scholar] [CrossRef]
- Hughes, Gillian. 2014. Finding a voice through “The Tree of Life”: A strength-based approach to mental health for refugee children and families in schools. Clinical Child Psychology 19: 139–53. [Google Scholar] [CrossRef] [PubMed]
- Jones, Barbara L., Deborah L. Volker, Yolanda L. Vinajeras, Linda L. Butros, Cynthia L. Fitchpatrick, and Kelly L. Rossetto. 2010. The meaning of surviving cancer for latino adolescents and emerging young adults. Cancer Nursing 33: 74–81. [Google Scholar] [CrossRef] [PubMed]
- Katz, Carmit, and Hamama Liat. 2013. Draw me everything that happened to you: Exploring children’s drawings of sexual abuse. Children and Youth Review 35: 877–82. [Google Scholar] [CrossRef]
- Keats, Patrice A. 2009. Multiple text analysis in narrative research: Visual, written, and spoken stories of experience. Qualitative Research 9: 181–95. [Google Scholar] [CrossRef]
- Kent, Erin E., Carla Parry, Michael J. Montoya, Leonard S. Sender, Rebecca A. Morris, and Hoda Anton-Culver. 2012. “You’re too young for this”: Adolescent and young adults’ perspectives on cancer survivorship. Journal of Psychosocial Oncology 30: 260–79. [Google Scholar] [CrossRef] [Green Version]
- King, Nigel. 2017. Thematic analysis in organisational research. In The Sage Handbook of Qualitative Business and Management Research: Methods and Challenges. Edited by Cathrine Cassell, Ann L. Cunliffe and Gina Grandy. London: SAGE, pp. 219–36. [Google Scholar]
- Klingenberg, Maria. 2014. Conformity and Contrast: Religious Affiliation in a Finland-Swede Youth Context. Doctoral dissertation, University of Helsinki, Helsinki, Finland. [Google Scholar]
- Kwak, Minyoung, Brad J. Zebrack, Katheel A. Meeske, Leanna Embry, Christine Aguilar, Rebecca Block, Brandon Hayes-Lattin, Yun Li, Melissa Butler, and Steven Cole. 2013. Trajectories of psychological distress in adolescent and young adult patients with cancer: A 1-year longitudinal study. Journal of Clinical Oncology 31: 2160–6. [Google Scholar] [CrossRef] [Green Version]
- Kyngäs, Helvi, Toini Jämsä, Raija Mikkonen, Eeva-Maija Nousiainen, Mervi Rytilahti, Pirkko Seppänen, and Ritva Vaittovaara. 2000. Terveys ei ole enää itsestään selvyys. Se on elämän suuri lahja. Tutkimus syöpää Sairastavien Nuoren Selviytymisestä Sairauden Kanssa. [Health Is No Longer Taken for Granted. It Is a Great Gift of Life. Cancer Coping of Young Adults]. Oulu: Pohjois-Pohjanmaan Sairaanhoitopiirin Julkaisuja. [Google Scholar]
- Kyngäs, Helvi, Raija Mikkonen, Eeva-Maija Nousiainen, Mervi Rytilahti, Pirkko Seppänen, Ritva Vaittovaara, and Toimi Jämsä. 2001. Coping with the onset of cancer: Coping strategies and resources of young people with cancer. European Journal of Cancer Care 10: 6–11. [Google Scholar] [CrossRef]
- Lester, Andrew D. 1995. Hope in Pastoral Care and Counseling. Louisville: Westminster John Knox Press. [Google Scholar]
- Levitt, Heidi M., Bamberg Michael, Creswell John W., Frost David M., Josselson Ruthellen, and Suárez-Orozco Carola. 2018. Journal article reporting standards for qualitative primary, qualitative meta-analytic, and mixed methods research in psychology: The APA Publications and Communications Board task force report. American Psychologist 73: 26–46. [Google Scholar] [CrossRef] [Green Version]
- Lev-Wiesel, Rachel, and Liraz Revital. 2007. Drawings vs. narratives: Drawing as a tool to encourage verbalization in children whose fathers are drug abusers. Clinical Child Psychology and Psychiatry 12: 65–75. [Google Scholar] [CrossRef]
- Lieblich, Amia. 1998. The holistic-content perspective. In Narrative Research: Reading, Analysis and Interpretation. Edited by Amia Lieblich, Rivka Tuval-Mashiach and Tamar Zilber. Thousand Oaks: Sage, pp. 62–87. [Google Scholar]
- Little, Miles, and Emma-Jane Sayers. 2004. While there’s life... hope and the experience of cancer. Social Science & Medicine 59: 1329–37. [Google Scholar] [CrossRef]
- Mishler, Elliot G. 1986. Research Interviewing: Context and Narrative. Cambridge: Harvard University Press. [Google Scholar]
- Nass, Sharyl J., Lynda K. Beaupin, Wendy Demark-Wahnefried, Karen Fasciano, Patricia A. Ganz, Brandon Hayes-Lattin, Melissa M. Hudson, Brenda Nevidjon, Kevin C. Oeffinger, Ruth Rechis, and et al. 2015. Identifying and addressing the needs of adolescents and young adults with cancer: Summary of an institute of medicine workshop. Oncologist 20: 186–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolan, Steven, Philip Saltmarsh, and Carlo Leget. 2011. Spiritual care in palliative care: Working towards an EAPC task force. European Journal of Palliative Care 18: 86–89. [Google Scholar]
- Pain, Helen. 2012. A literature review to evaluate the choice and use of visual methods. International Journal of Qualitative Methods 11: 303–19. [Google Scholar] [CrossRef] [Green Version]
- Palmu, Harri, Salomäki Hanna, Ketola Kimmo, and Niemelä Kati. 2012. Haastettu kirkko. Suomen evankelis-luterilainen kirkko vuosina 2008–2011. [Challenged Church. The Evangelical Lutheran Church of Finland in the Years 2008–2011]. Porvoo: Kirjapaja. [Google Scholar]
- Pargament, Kenneth I. 1997. The Psychology of Religion and Coping. Theory, Research, Practice. New York: The Guilford Press. [Google Scholar]
- Pargament, Kenneth I., Kennell Joseph, Hathaway William, Grevengoed Nancy, Newman John, and Jones Wendy. 1988. Religion and the problem-solving process: Three styles of coping. Journal for the Scientific Study of Religion 27: 90–104. [Google Scholar]
- Pargament, Kenneth I., Bruce W. Smith, Harold G. Koenig, and Lisa Perez. 1998. Patterns of positive and negative religious coping with major life stressors. Journal for the Scientific Study of Religion 37: 710–24. [Google Scholar] [CrossRef]
- Park, Crystal L., and Dalnim Cho. 2017. Spiritual well-being and spiritual distress predict adjustment in adolescent and young adult cancer survivors. Psycho-Oncology 26: 1293–300. [Google Scholar] [CrossRef] [PubMed]
- Park, Crystal L., Donald Edmondson, Amy Hale-Smith, and Thomas Blank. 2009. Religiousness/spirituality and health behaviors in younger adult cancer survivors: Does faith promote a healthier lifestyle? Journal of Behavioral Medicine 32: 582–91. [Google Scholar] [CrossRef] [PubMed]
- Park, Crystal L., Jennifer H. Wortmann, Amy E. Hale, Dalmin Cho D., and Thomas O. Blank. 2014. Assessing quality of life in young adult cancer survivors: development of the Survivorship-Related Quality of Life scale. Quality of Life Research 23: 2213–24. [Google Scholar] [CrossRef]
- Parks, Sharon Daloz. 2011. Big Questions Worthy Dreams, 2nd ed. San Francisco: Jossey Bass. [Google Scholar]
- Patterson, Pandora, Fiona E.J. McDonald, Brad Zebrack, and Sharon Medlow. 2015. Emerging issues among adolescent and young adult cancer survivors. Seminars in Oncology Nursing 31: 53–59. [Google Scholar] [CrossRef]
- Ragsdale, Judith R., Mary Ann Hegner, Mark Mueller, and Stella Davies. 2014. Identifying religious and/or spiritual perspectives of adolescents and young adults receiving blood and marrow transplants: A prospective qualitative study. Biology of Blood and Marrow Transplantation 20: 1242–7. [Google Scholar] [CrossRef] [Green Version]
- Riessman, Cathrine K. 2008. Narrative Methods for the Human Sciences. Thousand Oaks: Sage. [Google Scholar]
- Romero, Catherine, Lois C. Friedman, Mamata Kalidas, Richard Elledge, Janny Chang, and Katheel R. Liscum. 2006. Self-Forgiveness, spirituality, and psychological adjustment in women with breast cancer. Journal of Behavioral Medicine 29: 29–36. [Google Scholar] [CrossRef]
- Rose, Gillian. 2016. Visual Methodologies: An Introduction to the Interpretation of Visual Materials, 4th ed. London: Sage. [Google Scholar]
- Saarelainen, Suvi-Maria. 2015. Life tree drawings as a methodological approach in young adults’ life stories during cancer remission. Narrative Works 5: 68–91. [Google Scholar]
- Saarelainen, Suvi-Maria. 2016. Coping-related themes in cancer stories of young Finnish adults. International Journal of Practical Theology 20: 69–96. [Google Scholar] [CrossRef]
- Saarelainen, Suvi-Maria. 2017a. Meaningful Life with(out) Cancer: Coping Narratives of Emerging Finnish Adults. Doctoral dissertation, University of Helsinki, Helsinki, Finland. [Google Scholar]
- Saarelainen, Suvi-Maria. 2017b. Emerging Finnish adults coping with cancer: Religious, spiritual, and secular meanings of the experience. Pastoral Psychology 66: 251–68. [Google Scholar] [CrossRef]
- Saarelainen, Suvi-Maria. 2018. Lack of belonging as disrupting the formation of meaning and faith: Experiences of youth at risk of becoming marginalized. Journal of Youth and Theology 17: 127–49. [Google Scholar] [CrossRef]
- Saarelainen, Suvi-Maria. 2019. Landscapes of hope and despair: Stories of the future of emerging adults in cancer remission. Journal of Pastoral Theology 29: 67–84. [Google Scholar] [CrossRef]
- Saarelainen, Suvi-Maria, Peltomäki Isto, and Auli Vähäkangas. 2019. Healthcare chaplaincy in Finland. Tidsskrift for Praktisk Teologi 2: 22–31. [Google Scholar]
- Sansom-Daly, Ursula M., and Claire E. Wakefield. 2013. Distress and adjustment among adolescents and young adults with cancer: An empirical and conceptual review. Transnational Pediatrics 2: 167–97. [Google Scholar] [CrossRef]
- Sonninen, Susanna, ed. 2012. Nuoren Syöpäpotilaan Selviytymisopas. [Survival Guide for Young Patient]. Redfina: Suomen Syöpäpotilaat ry. [Google Scholar]
- Thomas, David M., Karen H. Albritton, and Andrea Ferrari. 2010. Adolescent and young adult oncology: An emerging field. Journal of Clinical Oncology 28: 4781–2. [Google Scholar] [CrossRef]
- Thomsen, Dorthe K., and Anders Bonde Jensen. 2007. Memories and narratives about breast cancer: Exploring associations between turning points, distress and meaning. Narrative Inquiry 17: 349–70. [Google Scholar] [CrossRef]
- Tong, Allison, Sainsbury Peter, and Craig Jonathan. 2007. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care 19: 349–57. [Google Scholar] [CrossRef] [Green Version]
- Toussaint, Loren, Michael Barry, Lynn Bornfriend, and Maurie Markman. 2014. Restore: The journey toward self-forgiveness: A randomized trial of patient education on self-forgiveness in cancer patients and caregivers. Journal of Health Care Chaplaincy 20: 54–74. [Google Scholar] [CrossRef] [PubMed]
- Toussaint, Loren, Michael Barry, Drew Angus, Lynn Bornfriend, and Maurie Markman. 2017. Self-Forgiveness is associated with reduced psychological distress in cancer patients and unmatched caregivers: Hope and self-blame as mediating mechanisms. Journal of Psychosocial Oncology 35: 544–60. [Google Scholar] [CrossRef] [PubMed]
- Vassal, Gilles, Edel Fitzgerald, Martin Schrappe, Frédéric Arnold, Jerzy Kowalczyk, David Walker, Lars Hjorth, Riccardo Riccardi, Anita Kienesberger, Kathy-Pitchard Jones, and et al. 2014. Challenges for children and adolescents with cancer in Europe: The SIOP-Europe Agenda. Pediatric Blood Cancer 61: 1551–7. [Google Scholar] [CrossRef] [PubMed]
- Vipunen. 2019. Available online: https://vipunen.fi/fi-fi/perus/Sivut/Kieli--ja-muut-ainevalinnat.aspx (accessed on 18 December 2019).
- Walker, Amy J., and Frances Marcus Lewis. 2016. Adolescent and young adult cancer survivorship: A systematic review of end-of-treatment and early posttreatment. Nursing and Palliative Care 1: 1–6. [Google Scholar] [CrossRef] [Green Version]
- Warner, Echo L., Erin E. Kent, Kelly M. Trevino, Helen M. Parsons, Brad J. Zebrack, and Anne C. Kirchhoff. 2016. Social well-being among adolescents and young adults with cancer: A systematic review. Cancer 122: 1029–37. [Google Scholar] [CrossRef] [Green Version]
- Weber, Sandra. 2008. Visual images in research. In Handbook of the Arts on Qualitative Research: Perspectives, Methodologies, Examples, and Issues. Edited by J. Gary Knowles and Ardra L. Cole. Thousand Oaks: Sage, pp. 42–55. [Google Scholar]
- Worthington, Everett L. 2014. Forgiveness and Reconciliation: Theory and Application. New York: Routledge. [Google Scholar]
- Yanez, Bettina, Donald Edmondson, Annette L. Stanton, Crystal L. Park, Lorna Kwan, Patricia A. Ganz, and Thomas O. Blank. 2009. Facets of spirituality as predictors of adjustment to cancer: Relative contributions of having faith and finding meaning. Journal of Consulting and Clinical Psychology 77: 730–41. [Google Scholar] [CrossRef]
- Yi, Jaehee, Brad Zebrack, Min Ah Kim, and Melissa Cousino. 2015. Posttraumatic growth outcomes and their correlates among young adult survivors of childhood cancer. Journal of Pediatric Psychology 40: 981–91. [Google Scholar] [CrossRef]
- Zebrack, Brad, Rebecca Block, Brandon Hayes-Lattin, Leanne Embry, Christine Aguilar, Kathleen A. Meeske, Yun Li, Melissa Butler, and Steven Cole. 2014. Psychosocial service use and unmet need among recently diagnosed adolescent and young adult cancer Patients. Cancer 119: 201–14. [Google Scholar] [CrossRef] [Green Version]
| 1 | See more about the medical descriptions of cancer types and stages: https://www.cancer.org/cancer/all-cancer-types.html#alpha-H. |
Figure 1.
Sophia’s drawing.

Figure 2.
Sarah’s drawing.

Figure 3.
Tom’s drawing.

Figure 4.
John’s drawing.

Figure 5.
Mark’s drawing.
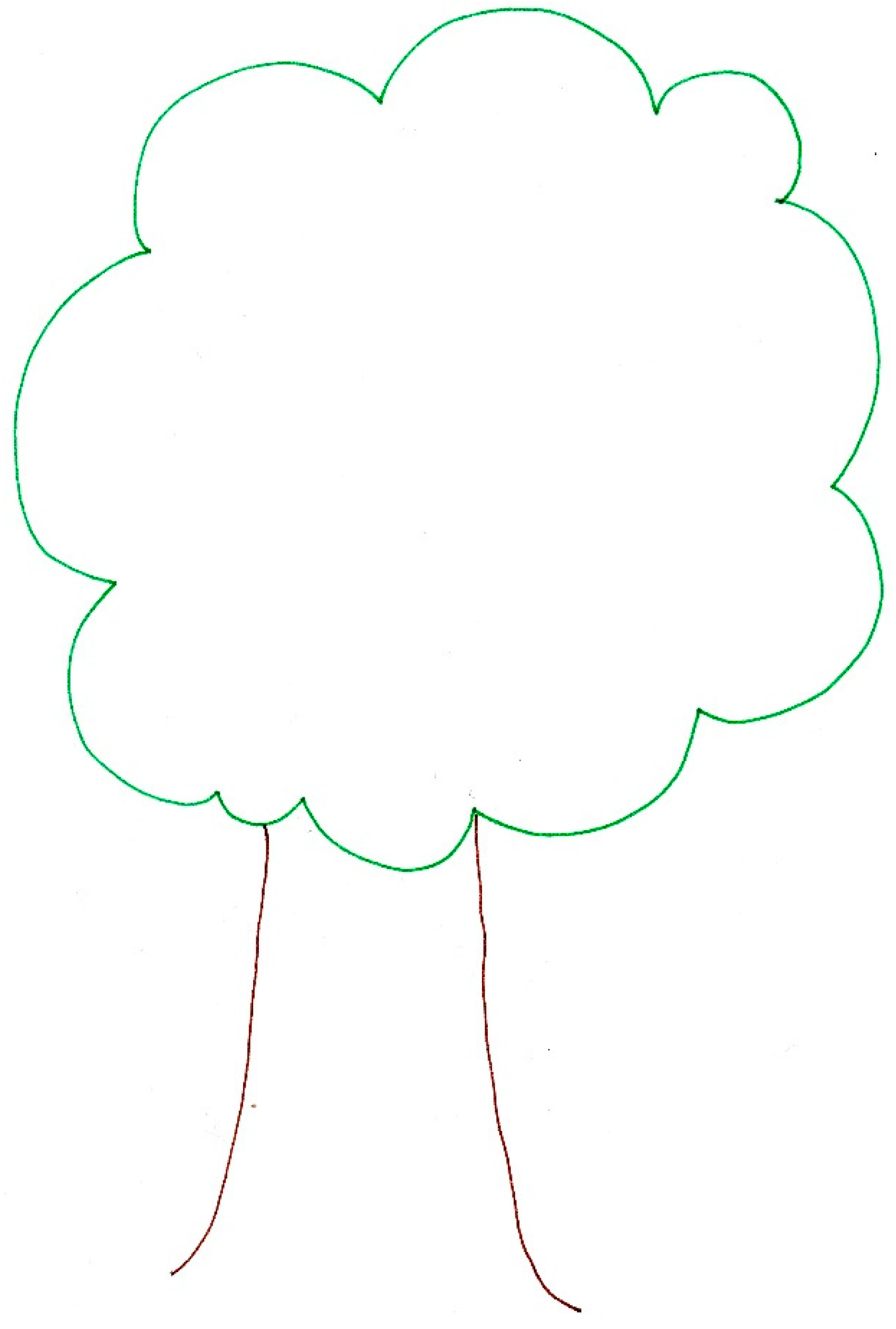
Figure 6.
Ava’s drawing.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Participants and descriptions of their cancer.
| Name * | Cancer | Time since Treatment |
|---|---|---|
| Anna | Hodgkin’s lymphoma, first diagnosis as stage 2A was changed to stage 3 after six months of chemotherapy; because of the changes in spread the treatment was continued for two months. | 5 years |
| Ava | Non-Hodgkin’s lymphoma, more local but made breathing difficult and caused other symptoms. | 2 years |
| Beth | Hodgkin’s lymphoma, stage 4A. Relapse after a couple of years in remission. | 2 years |
| Cain | Testicular cancer, spread to lymph nodes. | 5 years |
| Chloe | Hodgkin’s lymphoma, stage 4B, relapsed during treatment. | 3 years |
| Emily | Non-Hodgkin’s lymphoma, no descriptions of spread. Six months of treatment and no external signs that could refer to more local cancer. | 5 years |
| Emma | Hodgkin’s lymphoma, stage 4B. | 1 year |
| Gina | Lymphoma, with large spread and multiple tumors likely to mean stage 4B. | 3 years |
| John | Hodgkin’s lymphoma, stage 4B. Relapse after seven years in remission. | Right after the treatment |
| Macy | Lymphoma, diagnosis changed during the treatment to spreading stage 4. | 7 months |
| Mark | Hodgkin’s lymphoma, no descriptions of spread. Six months of treatment, this could refer to more local cancer. | 7 months |
| Olivia | Hodgkin’s lymphoma, stage 2A. | During treatment and 4 months after |
| Sarah | Hodgkin’s lymphoma, no notification of exact spread. Symptoms: tumor near the collar bone and tiredness. | 5 years |
| Sophia | Osteosarcoma (knee). Localized cancer; an amputation was not needed. | 5 years |
| Thea | Sarcoma (back), stage 4B. | 4 years |
| Tom | Osteosarcoma (knee), chemotherapy and amputation. Refers to spread to some extent. | 2 years |
* Names are fictional to protect participants’ privacy. All translations from Finnish by the author.
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Saarelainen, S.-M. Meeting the Spiritual Care Needs of Emerging Adults with Cancer. Religions 2020, 11, 16. https://0-doi-org.brum.beds.ac.uk/10.3390/rel11010016
AMA Style
Saarelainen S-M. Meeting the Spiritual Care Needs of Emerging Adults with Cancer. Religions. 2020; 11(1):16. https://0-doi-org.brum.beds.ac.uk/10.3390/rel11010016
Chicago/Turabian StyleSaarelainen, Suvi-Maria. 2020. "Meeting the Spiritual Care Needs of Emerging Adults with Cancer" Religions 11, no. 1: 16. https://0-doi-org.brum.beds.ac.uk/10.3390/rel11010016
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.