Transcending the Suffering in Cancer: Impact of a Spiritual Life Review Intervention on Spiritual Re-Evaluation, Spiritual Growth and Psycho-Spiritual Wellbeing


Abstract
:1. Introduction
1.1. Cancer as a Limit Situation: Existential Despair, Spiritual Re-Evaluation, and Self-Transcendence
1.2. Transcending the Self and Spirituality
1.3. Spiritual Life Review as a Tool for Spiritual Re-Evaluation
2. Materials and Methods
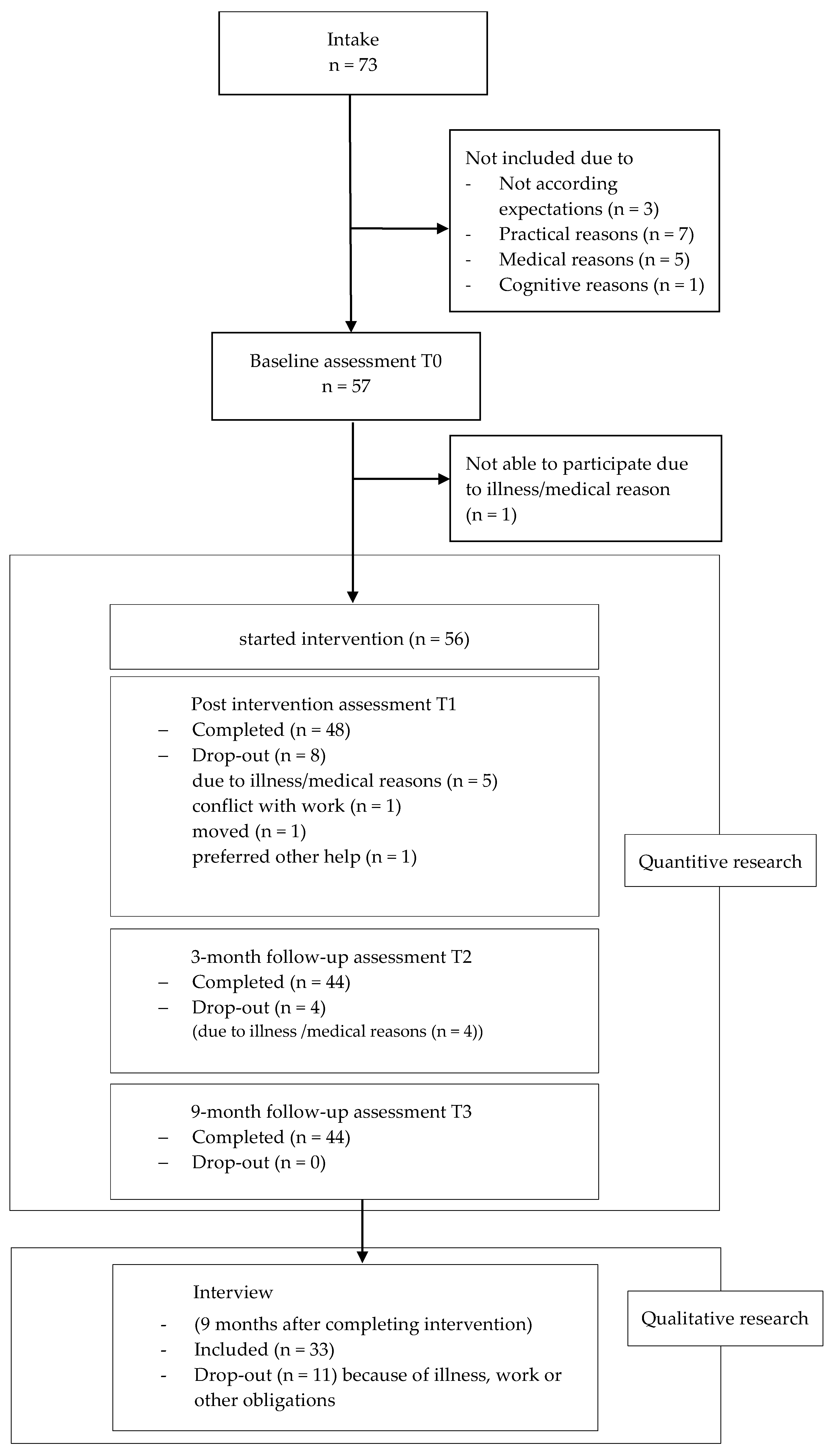
2.1. Study Design and Population
2.2. Intervention
2.3. Outcome Measurements
2.4. Analysis
2.4.1. Qualitative Analysis
2.4.2. Quantitative Analysis
3. Results
3.1. Re-Evaluation before the Intervention
3.1.1. Ontic Reorientation: From Ontic Anxiety to Ontic Affirmation
3.1.2. Moral Reorientation: From Moral Anxiety to Moral Affirmation
3.1.3. Spiritual Re-evaluation: From Spiritual Anxiety to Spiritual Affirmation
3.2. Re-Evaluation after the Intervention
3.2.1. Ontic Reorientation: From Ontic Anxiety to Ontic Affirmation
3.2.2. Moral Reorientation: From Moral Anxiety to Moral Affirmation
3.2.3. Spiritual Re-Evaluation: From Spiritual Anxiety to Spiritual Affirmation
3.3. Impact of the Intervention on Spiritual Growth, Ego-Integrity and Psycho-Spiritual Wellbeing
3.3.1. Spirituality and Spiritual Growth
3.3.2. Psycho-Spiritual Wellbeing
3.3.3. Ego Integrity
4. Discussion
4.1. Limitations
4.2. Implications
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
| Resp. nr: | Re-Evaluation | |||||
|---|---|---|---|---|---|---|
| Content | Witness/Presence of Respondents | Witness/Presence of (O)thers | Finding Meaning/Meaning Making | Attitude | Anxiety vs. Affirmation | |
| What is of ultimate concern? (self, other, other meaning or presence; lived experience; practices) | For whom is resp. receptive/present; whom does resp. hear/see/acknowledge/sustain? | Who is receptive/present; By whom is resp. heard/seen/acknowledged/sustained? | What meaning does resp. find in suffering; in life, in works, creations; in experiences, encounters | Taking a stand to life, conditions of life, illness; fulfillment of self; ultimate concern | - ontic (fate/death) - moral (guilt, condemnation) - spiritual (doubt, estrangement) | |
| in vivo | self, other, other meaning or presence | self, other, other meaning or presence | in vivo | in vivo | in vivo | |
| Before illness | ||||||
| Impact of illness | ||||||
| During intervention | ||||||
| Impact of intervention | ||||||
| General notes/observations | ||||||
References
- Anbeek, Christa. 2013. Aan De Heidenen Overgeleverd: Hoe Theologie De 21ste Eeuw Kan Overleven. Utrecht: Ten Have. [Google Scholar]
- Bauereiß, Natalie, Stefanie Obermaier, Selcuk Erol Özünal, and Harald Baumeister. 2018. Effects of existential interventions on spiritual, psychological, and physical well-being in adult patients with cancer: Systematic review and meta-analysis of randomized controlled trials. Psychooncology 27: 2531–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Best, Megan, Lynley Aldridge, Phyllis Butow, Ian Olver, and Fleur Webster. 2015. Conceptual analysis of suffering in cancer: A systematic review. Psychooncology 24: 977–86. [Google Scholar] [CrossRef] [PubMed]
- Breitbart, William, Barry Rosenfeld, Christopher Gibson, Haley Pessin, Shannon Poppito, Christian Nelson, Alexis Tomarken, Anne Kosinski Timm, Amy Berg, Colleen Jacobsen, and et al. 2010. Meaning-Centered Group Psychotherapy for patients with advanced cancer: A pilot randomized controlled trial. Psycho-Oncology 19: 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breitbart, William, Barry Rosenfield, Haley Pessin, Alisson Applebaum, Julia Kulikowski, and Wendy G. Lichtental. 2015. Meaning-Centered Group Psychotherapy: An Effective Intervention for Improving Psychological Well-Being in Patients with Advanced Cancer. Journal of Clinical Oncology 33: 749–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breitbart, William, Haley Pessin, Barry Rosenfeld, Alisson J. Applebaum, Wendy G. Lichtental, Yuelin Li, Rebecca M. Saracino, Allison M. Marziliano, Melissa Masterson, Kristen Tobias, and et al. 2018. Individual meaning-centered psychotherapy for the treatment of psychological and existential distress: A randomized controlled trial in patients with advanced cancer. Cancer 124: 3231–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, Jacob. 1977. Statistical Power Analysis for the behavioral Sciences. San Diego: Academic Press. [Google Scholar]
- Coward, Doris D. 1991. Self-transcendence and emotional well-being in women with advanced breast cancer. Oncology Nursing Forum 18: 857–63. [Google Scholar] [PubMed]
- Coward, Doris D. 2003. Facilitation of self-transcendence in a breast cancer support group: II. Oncology Nursing Forum 30: 291–300. [Google Scholar] [CrossRef]
- Coward, Doris D., and Pamela G. Reed. 1996. Self-transcendence: A resource for healing at the end of life. Issues Ment Health Nursing 17: 275–88. [Google Scholar] [CrossRef]
- Carel, Havi. 2016. Phenomenology of Illness. Oxford: Oxford University Press. [Google Scholar]
- de Jager-Meezenbroek, Eltica, Machteld vd. Berg, Gerwi Tuytel, Adriaan Visser, and Bert Garssen. 2006. Het meten van spiritualiteit als een universeel fenomeen: De ontwikkeling van de Spirituele Attitude en Interesse Lijst (SAIL). Psychosociale Oncologie 14: 14–15. [Google Scholar]
- de Jager Meezenbroek, Eltica, Bert Garssen, Machteld van den Berg, Gerwi Tuytel, Dirk van Dierendonck, Adriaan Visser, and Wilmar B. Schaufeli. 2012. Measuring spirituality as a universal human experience: Development of the Spiritual Attitude and Involvement List (SAIL). Journal of Psychosocial Oncology 30: 141–67. [Google Scholar] [CrossRef] [Green Version]
- Frankl, Viktor E. 1955. The Doctor and the Soul. New York: Knopf. [Google Scholar]
- Frankl, Viktor E. 1988. The Will to Meaning: Foundations and Applications of Logotherapy. New York: Penguin. [Google Scholar]
- Frank, Arthur W. 1991. The Wounded Storyteller. Chicago: University of Chicago Press. [Google Scholar]
- Frank, Arthur W. 1998. Stories of illness as care of the self: A Foucauldian dialogue. Health 2: 329–48. [Google Scholar] [CrossRef]
- Ganzevoort, R. Ruard. 2001. Chronische aandoeningen en zingeving. TvZ. Tijdschift voor Verpleegkundigen 18/111: 686–89. [Google Scholar]
- Ganzevoort, R. Ruard. 2006. The social construction of revelation. International Journal of Practical Theology 8: 1–14. [Google Scholar] [CrossRef]
- Ganzevoort, R. Ruard, and Jan Visser. 2007. Zorg voor Het Verhaal. Achtergronden, Methode en Inhoud van Pastorale Zorg. Zoetermeer: Meinema. [Google Scholar]
- Hill, Peter C., Kenneth I. Pargament, Ralph W. Hood Jr., Michael E. McCullough, James P. Swyers, David B. Larson, and Brian J. Zinnbauer. 2000. Conceptualizing religion and spirituality: Points of commonality, points of departure. Journal for the Theory of Social Behaviour 30: 51–77. [Google Scholar] [CrossRef]
- Hefferon, Kate, Madeleine Grealy, and Nanette Mutrie. 2009. Post-traumatic growth and life threatening physical illness: A systematic review of the qualitative literature. British Journal of Health Psychology 14: 343–78. [Google Scholar] [CrossRef] [Green Version]
- Jaspers, Karl. 1919. Psychologie der Weltanschauungen. Berlijn: Springer. [Google Scholar]
- Jaspers, Karl. 1938. Existenzphilosophie. Drei Vorlesungen. Berlijn: Springer. [Google Scholar]
- Jaspers, Karl. 1951. Inleiding tot De philosophie. Assen: Born. [Google Scholar]
- Jeong, HyeSun, and HyunSoo Oh. 2015. Evaluating the Compehensive Model of Ego Integrity for Senior Patients in Convalescent Hospitals: Influence Factors and Outcome Variables. International Journal of Bioscience and Bio-Technology 7: 317–26. [Google Scholar] [CrossRef]
- Kissane, David W. 2012. The relief of existential suffering. Archives of Internal Medicine 172: 1501–5. [Google Scholar] [CrossRef]
- Kleijn, Gitta, Lenneke Post, Birgit I. Witte, Ernst T. Bohlmeijer, Gerben J. Westerhof, Pim Cuijpers, and Irma I. Verdonck-de Leeuw. 2016. Psychometric Characteristics of a Patient Reported Outcome Measure on Ego-Integrity and Despair among Cancer Patients. PLoS ONE 11: e0156003. [Google Scholar] [CrossRef]
- Kleijn, Gitta, Birgit I. Lissenberg-Witte, Ernst T. Bohlmeijer, Bas Steunenberg, Kitty Knipscheer-Kuijpers, Vincent Willemsen, Annemarie Becker, Egbert F. Smit, Corien M. Eeltink, Anna M. E. Bruijnzeel, and et al. 2018. The efficacy of Life Review Therapy combined with Memory Specificity Training (LRT-MST) targeting cancer patients in palliative care: A randomized controlled trial. PLoS ONE 13: e0197277. [Google Scholar] [CrossRef]
- Lee, Virginia. 2008. The existential plight of cancer: Meaning making as a concrete approach to the intangible search for meaning. Support Care Cancer 16: 779–85. [Google Scholar] [CrossRef]
- Maslow, Abraham. H. 1971. The Farther Reaches of Human Nature. New York: Penguin. [Google Scholar]
- McAdams, Dan P. 1996. Personality, Modernity, and the Storied Self: A Contemporary Framework for Studying Persons. Psychological Inquiry 5: 295–321. [Google Scholar] [CrossRef]
- McAdams, Dan P. 2001. The psychology of life stories. Review of General Psychology 5: 100–22. [Google Scholar] [CrossRef]
- McAdams, Dan P. 2009. The Person: An Introduction to the Science of Personality Psychology, 5th ed. New York: Wiley. [Google Scholar]
- Oh, Pok-Ja, and Soo H. Kim. 2014. The effects of spiritual interventions in patients with cancer: A meta-analysis. Oncology Nursing Forum 41: E290–E301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pargament, Kenneth I. 1997. The Psychology of Religion and Coping; Theory, Research, Practice. New York: Guildford. [Google Scholar]
- Pargament, Kenneth I. 2013. Spirituality as an Irreducible Human Motivation and Process. International Journal for the Psychology of Religion 23: 271–81. [Google Scholar] [CrossRef]
- Park, Crystal L. 2010. Making sense of the meaning literature: An integrative review of meaning making and its effects on adjustment to stressful life events. Psychol. Bull. 136: 257–301. [Google Scholar] [CrossRef]
- Park, Crystal L. 2013. Spirituality and meaning making in cancer survivorship. In The Psychology of Meaning. Edited by Keith D. Markman, Travis Proulx and Matthew J. Lindberg. Washington, DC: American Psychological Association, pp. 257–77. [Google Scholar]
- Park, Crystal L, Sherman Allen C., Heather S. L. Jim, and John M. Salsman. 2015. Religion/spirituality and health in the context of cancer: Cross-domain integration, unresolved issues, and future directions. Cancer 121: 3789–94. [Google Scholar] [CrossRef] [Green Version]
- Pinquart, Martin, and Forstmeier Simon. 2012. Effects of reminiscence interventions on psychosocial outcomes: A meta-analysis. Aging Ment Health 16: 541–58. [Google Scholar] [CrossRef] [Green Version]
- Pool, Grieteke. 2009. Kanker: Een existentiële opgave. In Psychologische Patiëntenzorg in de Oncologie. Edited by Hanneke deHaes, Leo G. van Wezel and Robbert Sanderman. Assen: van Gorcum, pp. 134–52. [Google Scholar]
- Puchalski, Christina, Betty Ferrell, Rose Virani, Shirley Otis-Green, Pamela Baird, Janet Bull, Harvey Chochinov, George Handzo, Holly Nelson-Becker, Maryo Prince-Paul, and et al. 2009. Improving the quality of spiritual care as a dimension of palliative care: The report of the Consensus Conference. J. Palliat. Med. 12: 885–904. [Google Scholar] [CrossRef] [Green Version]
- Puchalski, Christina M., Robert Vitillo, Sharon K. Hull, and Nancy Reller. 2014. Improving the Spiritual Dimension of Whole Person Care: Reaching National and International Consensus. J. Palliat. Med. 17: 642–656. [Google Scholar] [CrossRef]
- Ricœur, Paul. 1984. Time and Narrative. Chicago: University of Chicago Press, Volume 3. [Google Scholar]
- Ricœur, Paul. 1991. From Text to Action, Essays in Hermeneutics. Evanston: Northwestern University Press. [Google Scholar]
- Ricœur, Paul. 1992. Oneself as Another. Chicago: University of Chicago Press. [Google Scholar]
- Reed, Pamela. G. 2009. Demystifying self-transcendence for mental health nursing practice and research. Archives of Psychiatric Nursing 23: 397–400. [Google Scholar] [CrossRef]
- Staude, John-Raphael. 2005. Autobiography as a spiritual practice. Journal of Gerontological Social Work 45: 249–69. [Google Scholar] [CrossRef]
- Taylor, Charles. 2007. A Secular Age. Cambridge: Belknap Press of Harvard University Press. [Google Scholar]
- ter Borg, Meerten. 2010. Vrijzinnigen Hebben de Toekomst. Zoetermeer: Meinema. [Google Scholar]
- Thomas, Jeani C., Mattie Burton, Mary T. Quin Griffin, and Joyce J. Fitzpatrick. 2010. Self-transcendence, spiritual well-being, and spiritual practices of women with breast cancer. Journal of Holistic Nursing 28: 115–22. [Google Scholar] [CrossRef] [PubMed]
- Tillich, Paul. 2000. The Courage to be. New Haven: Yale University Press. First published 1952. [Google Scholar]
- Tillich, Paul. 1956. Dynamics of Faith. New York: Harper. [Google Scholar]
- van Dierendonck, Dirk. 2004. The construct validity of Ryff’s Scales of Psychological Well- being and its extension with spiritual well-being. Personality and Individual Differences 36: 629–43. [Google Scholar] [CrossRef]
- van den Brink, Gabriel. 2012. De Lagere Landen en het Hogere. De betekenis van Geestelijke Beginselen in Het Moderne Bestaan. Amsterdam: Amsterdam University Press. [Google Scholar]
- Visser, Anja, Nicoline Uwland, and Bert Garssen. 2013. De rol van spiritualiteit bij het omgaan met kanker: Gemengde-methodenstudie. Psyche & Geloof 24: 171–83. [Google Scholar]
- Vehling, Sigrun, and David W. Kissane. 2018. Existential distress in cancer: Alleviating suffering from fundamental loss and change. Psychooncology 27: 2525–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waaijman, Kees. 2000. Spiritualiteit: Vormen, Grondslagen, Methoden. Gent: Carmelitana. [Google Scholar]
- Wakefield, Dan. 1990. The Story of your life. In Writing a Spiritual Autobiography. A Step to Step Approach to Exploring Your Past and Understanding Your Present. Boston: Beacon Press. [Google Scholar]
- Weisman, Avery D., and J. William Worden. 1976. The existential plight in cancer: Significance of the first 100 days. The International Journal of Psychiatry in Medicine 7: 1–15. [Google Scholar] [CrossRef]
- Westerhof, Gerben J., Ernst Bohlmeijer, and Jeffrey D. Webster. 2010. Reminiscence and mental health: A review of recent progress in theory, research and interventions. Ageing & Society 30: 697–721. [Google Scholar] [CrossRef] [Green Version]
- Westerhof, Gerben J., and Ernst T. Bohlmeijer. 2014. Celebrating fifty years of research and applications in reminiscence and life review: State of the art and new directions. The Journal of Aging Studies 29: 107–114. [Google Scholar] [CrossRef]
- Weathers, Elizabeth, Geraldine McCarthy, and Alice Coffey. 2016. Concept Analysis of Spirituality: An Evolutionary Approach. Nursing Forum 51: 79–96. [Google Scholar] [CrossRef]
- Xing, Lu, Xiujing Guo, Lu Bai, Jiahui Qian, and Jing Chen. 2018. Are spiritual interventions beneficial to patients with cancer? A meta-analysis of randomized controlled trials following PRISMA. Medicine (Baltimore) 97: e11948. [Google Scholar] [CrossRef]
- Yalom, Irvin D. 2008. Staring at the Sun. Overcoming the Dread of Death. London: Piatkus. [Google Scholar]
| Spiritual Re-Evaluation | ||
|---|---|---|
| Anxiety Over Loss of the Self | Self-Affirmation | Self-Transcendence |
| Ontic anxiety (fate and death) | Ontic affirmation: affirming life (in taking a stand towards the conditions of life; in finding meaning in suffering; in accepting life despite fate and death). | Temporal transcendence (integrating past and future in meaningful present) |
| Moral anxiety (guilt, self-rejection, and condemnation) | Moral affirmation: affirming the self as oneself (in taking a stand towards the fulfillment of oneself and one’s destiny; in finding meaning in one’s works and creations; in accepting the self despite being unacceptable). | Intrapersonal transcendence (self-acceptance, fulfillment in life) |
| Spiritual anxiety: (estrangement from ultimate concern; emptiness and meaninglessness) | Spiritual affirmation: affirming ultimate concern (in taking a stand towards ultimate concern; in finding ultimate meaning in encounters and experiences; in accepting affirmation of one’s ultimate concern, despite doubt and/or estrangement from this ultimate concern). | Intrapersonal transcendence (connectedness with the self); Interpersonal transcendence (connectedness with significant others and environment); and Transpersonal transcendence (connectedness with dimensions beyond the typically discernible world; the significant, the sacred) |
| (n = 57) 1 | (n = 33) 2 | ||||
|---|---|---|---|---|---|
| Scale | Distribution | % | Distribution | % | |
| Sex | Male | 6 | 10.5 | 5 | 15.2 |
| Female | 51 | 89.5 | 28 | 84.8 | |
| Age | Mean (SD) | 56.68 (9.2) | 57.73 (9.1) | ||
| Range | 29–73 | 29–73 | |||
| Marital status | Married/long-term | ||||
| relationship | 24 | 42.1 | 19 | 57.6 | |
| Divorced | 16 | 28.1 | 8 | 24.2 | |
| Widowed | 5 | 8.8 | 2 | 6.1 | |
| Never married | 12 | 21.0 | 4 | 12.1 | |
| Children | Yes | 43 | 75.4 | 26 | 78.8 |
| No | 14 | 24.6 | 7 | 21.2 | |
| Education | High | 31 | 54.39 | 22 | 66.6 |
| Medium | 23 | 40.35 | 10 | 30.4 | |
| Lower | 0 | 0 | 0 | 0 | |
| Different | 3 | 5.26 | 1 | 3.0 | |
| Worldview/religion | Christian | 18 | 31.6 | 10 | 30.3 |
| Humanistic | 3 | 5.3 | 2 | 6.1 | |
| Personal bricolage | 21 | 36.8 | 13 | 39.4 | |
| No religion | 15 | 26.3 | 8 | 24.2 | |
| Affinity with writing | Affinity, writing often | 12 | 21.1 | 6 | 18.2 |
| Affinity, not writing often | 36 | 63.2 | 21 | 63.6 | |
| No affinity | 9 | 15.8 | 6 | 18.2 | |
| Tumor type | Breast cancer | 27 | 47.4 | 16 | 48.5 |
| Hematological cancer | 10 | 17.5 | 7 | 21.2 | |
| Different | 10 | 17.5 | 7 | 21.2 | |
| Unknown | 10 | 17.5 | 3 | 9.1 | |
| Key Questions | Aspects |
|---|---|
|
|


| Dependent Variable | Baseline | p (H0:T0 = T1 = T2 = T3) | Treatment Effect | p Bonferroni Correction (p < 0.05/3 = 0.017) | Effect Estimate b | Effect Size Β |
|---|---|---|---|---|---|---|
| Overall spirituality | 4.04 | 0.007 | t0–t2 | 0.001 | 0.204 | 0.397 |
| Meaningfulness | 4.11 | 0.048 | t0–t2 | 0.007 | 0.279 | 0.355 |
| Trust | 4.13 | 0.057 | ||||
| Acceptance | 4.36 | 0.022 | t0–t2 | 0.010 | 0.270 | 0.364 |
| Caring for others | 4.72 | 0.699 | ||||
| Connectedness with nature | 4.99 | 0.406 | ||||
| Transcendent experiences | 3.16 | 0.031 | t0–t2 | 0.004 | 0.291 | 0.286 |
| Spiritual activities | 3.49 | 0.004 | t0–t2 | <0.001 | 0.327 | 0.326 |
| t0–t3 | 0.014 | 0.222 | 0.222 |
| Dependent Variable | Baseline | p (H0:T0 = T1 = T2=T3) | Treatment Effect | p Bonferroni Correction (p < 0.05/3 = 0.017) | Effect Estimate b | Effect Size Β |
|---|---|---|---|---|---|---|
| Positive relations w. others | 4.44 | 0.248 | ||||
| Autonomy | 4.16 | 0.133 | ||||
| Environmental mastery | 4.21 | 0.169 | ||||
| Personal growth | 4.87 | 0.351 | ||||
| Purpose in life | 4.23 | 0.002 | t0–t1 | 0.001 | 0.270 | 0.381 |
| t0–t2 | 0.001 | 0.290 | 0.410 | |||
| Self-acceptance | 4.09 | 0.004 | t0–t1 | 0.002 | 0.240 | 0.305 |
| t0–t2 | 0.002 | 0.254 | 0.323 | |||
| Inner strength | 4.56 | 0.015 | t0–t2 | 0.002 | 0.270 | 0.382 |
| Relationship with a higher power | 3.88 | 0.031 | t0–t2 | 0.005 | 0.265 | 0.213 |
| Dependent Variable | Baseline | p (H0:T0 = T1 = T2 = T3) | Treatment Effect | p Bonferroni Correction (p < 0.05/3 = 0.017) | Effect Estimate b | Effect Size Β |
|---|---|---|---|---|---|---|
| Ego integrity | 4.19 | <0.001 | t0–t1 | <0.001 | 0.481 | 0.606 |
| t0–t2 | <0.001 | 0.375 | 0.473 | |||
| t0–t3 | <0.001 | 0.434 | 0.547 | |||
| Despair | 3.15 | 0.001 | t0–t1 | 0.002 | −0.203 | −0.288 |
| t0–t2 | <0.001 | −0.247 | −0.352 |

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Post, L.; Ganzevoort, R.R.; Verdonck-de Leeuw, I.M. Transcending the Suffering in Cancer: Impact of a Spiritual Life Review Intervention on Spiritual Re-Evaluation, Spiritual Growth and Psycho-Spiritual Wellbeing. Religions 2020, 11, 142. https://0-doi-org.brum.beds.ac.uk/10.3390/rel11030142
Post L, Ganzevoort RR, Verdonck-de Leeuw IM. Transcending the Suffering in Cancer: Impact of a Spiritual Life Review Intervention on Spiritual Re-Evaluation, Spiritual Growth and Psycho-Spiritual Wellbeing. Religions. 2020; 11(3):142. https://0-doi-org.brum.beds.ac.uk/10.3390/rel11030142
Chicago/Turabian StylePost, Lenneke, R. Ruard Ganzevoort, and Irma M. Verdonck-de Leeuw. 2020. "Transcending the Suffering in Cancer: Impact of a Spiritual Life Review Intervention on Spiritual Re-Evaluation, Spiritual Growth and Psycho-Spiritual Wellbeing" Religions 11, no. 3: 142. https://0-doi-org.brum.beds.ac.uk/10.3390/rel11030142