
Religious Views of Suffering Profile Groups during COVID-19


School of Psychology & Marriage and Family Therapy, Fuller Theological Seminary, Pasadena, CA 91182, USA
*
Author to whom correspondence should be addressed.
Religions 2022, 13(5), 453; https://0-doi-org.brum.beds.ac.uk/10.3390/rel13050453
Submission received: 28 March 2022
/
Revised: 12 May 2022
/
Accepted: 13 May 2022
/
Published: 17 May 2022
(This article belongs to the Special Issue COVID-19, Mental Health, and Religious Treatment Research)
Abstract
:Religion plays an important role in making sense of adversity, and individuals hold varying beliefs about God’s role in suffering (theodicy). This study examined the association between individuals’ theodicies at the beginning of the COVID-19 pandemic and outcomes of their religiousness and psychological well-being. The first aim was to classify participants into profile groups based on theodicy. The second aim was to compare the groups on religious commitment, COVID-19 stress, anxiety, and psychological well-being. Theodicy was measured with the Views of Suffering Scale among 233 participants. Three distinct groups emerged, viewing God as active, God as passive, and suffering as random. Individuals who held an active view of God’s role were most religiously committed and had the lowest levels of general anxiety and stress regarding COVID-19. In contrast, those who viewed God as passive reported the highest general anxiety level. Those who viewed suffering as random reported the highest level of COVID-19 stress and the lowest level of religious commitment. This study demonstrates the benefits of considering a person-centered approach to understanding theodicy. Even within a predominantly religious sample, the three clusters of active, passive, and random views demonstrated meaningful differences in outcomes between the groups of participants.
Keywords:
COVID-19; views of suffering; Christian; theodicy; religious commitment; anxiety; well-being; cluster analysis1. Introduction
Within a month of its detection in December 2019, in Wuhan, China, the highly contagious acute respiratory syndrome coronavirus-2 (COVID-19) was declared a Public Health Emergency of International Concern by the World Health Organization (WHO 2020). By mid-February 2020, the virus had spread to 20 countries, and by March 2020, COVID-19 was declared a global pandemic (WHO 2020). Clinical features ranged from asymptomatic states to multi-organ dysfunction resulting in death (Singhal 2020; Wang et al. 2020). At the time of this study, two months after the virus was declared a pandemic, case numbers had reached 6 million cases worldwide, and 367,000 deaths (WHO 2020). In the United States, over 1.7 million had been infected, with over 100,000 deaths reported (WHO 2020). The unprecedented disruptions of the COVID-19 pandemic led to stress and anxiety for most people. This study examined how views of God’s role in the midst of suffering is associated with one’s religious commitment, stress, anxiety, and well-being.
In the United States, COVID-19 created mass disruptions across every aspect of life (APA 2020), including job loss, virtual schooling for children, food and supply shortages, home isolation, social distancing, and required personal protective equipment for all interactions outside the home (Harapan et al. 2020). Compounding these disruptions, the ever-present threat of contracting the disease fueled a pervasive and persisting feeling of global suffering. At the time of this study, two months after the implementation of home isolation and school closures, the majority of offices, sit-down restaurants, bars, movie theaters, gyms, and churches remained closed. Weddings and funerals were canceled (NFDA 2020). Visitations were prohibited in high-risk facilities (i.e., hospitals, senior living facilities), preventing people from physically supporting their sick and dying loved ones (CDC 2020a).
1.1. COVID-19 Stress and Anxiety
It has been well established that disruptions to daily routines, threats to physical health, and economic uncertainty generally result in increased stress and anxiety, which often lead to maladaptive coping behaviors (Park et al. 2020). In the early months of the pandemic, researchers sought to understand and predict the psychological impact of COVID-19 on stress and anxiety by reviewing existing literature on previous pandemics, such as the Spanish flu and the 2009 H1N1 pandemic (Rubin et al. 2009; Wheaton et al. 2012). Taylor et al. (2020) identified the unique nature of COVID-19 stressors, including fear of becoming infected, coming into contact with contaminated surfaces, foreigners carrying the infection, socio-economic impacts, behaviors such as compulsive checking and reassurance-seeking around pandemic-related threats, and other post-traumatic symptoms. Horesh and Brown (2020) captured these fears by predicting that COVID-19 would leave deep psychological scars.
During the months of April and May 2020, the yearly APA Stress in America Poll recorded the first statistically significant increase in overall reported stress levels in U.S. adults since its inception in 2007 (APA 2020). Groups with the most significant stress level increases included parents of children under the age of 18 and people of color (APA 2020). A survey by the National Center for Health Statistics and the Census Bureau estimated anxiety and depression would increase three-fold and suicide rates two-fold compared to the previous year (CDC 2020b). Another concern raised by Czeisler et al. (2020) was that almost half of U.S. adults were delaying or avoiding medical care during the pandemic, increasing morbidity and mortality risks associated with treatable and preventable health conditions.
1.2. Religious Commitment and Well-Being
While much of the COVID-19-related research has heretofore focused on public outreach, raising awareness about mental and behavioral health services (Boals and Banks 2020; Horesh and Brown 2020), fostering resilience (PeConga et al. 2020), treating loss and grief (Ishikawa 2020; Vázquez Bandín 2020), or expanding telehealth access and services (Watts et al. 2020), relatively less attention has been given to investigating the attitudes and characteristics of how people have coped religiously with the challenges of the pandemic. A Pew Research study conducted in March 2020 found that the pandemic forced many to re-evaluate their views of life, death, and suffering, revealing that over 55% of individuals had “prayed for an end to the coronavirus” (Pew Research Center 2020). According to a 2019 Gallup poll, 49% of U.S. individuals already considered religion to be “very important” and 64% said they were either satisfied with the influence of religion on their lives or wanted it to have more of an influence (Gallup Inc. 2021).
In the face of acute COVID-19 suffering, it is unsurprising that many turned to religion for answers (Seryczyńska et al. 2021). Previous research established that religious commitment has been helpful for coping with solitude, exclusion, mental illness, physical diseases, immunodeficiencies, and many psychological and social problems (Hart and Koenig 2020). Several researchers have positively associated religious commitment with greater life satisfaction and overall well-being (Lim and Putnam 2010; Roberto et al. 2020; Yonker et al. 2012). Furthermore, some have associated religious commitment to physical and psychological well-being in the context of coping with adversity in particular (Oman and Thoresen 2005; Pargament et al. 2001).
1.3. Meaning-Making
Religion plays an important role in making sense of adversity. In their research on well-being, Haver et al. (2015) suggested that one of well-being’s essential components is a sense of “dealing with problems well”. Park (2005) suggested that a mechanism by which religion helps make life’s hardships more bearable is that it provides a meaning-making system to help explain or provide a context for difficult circumstances. Park’s (2010) theoretical model suggests that one of the goals of the meaning-making process is to seek comprehensibility and significance, and that distress arises when there is a discrepancy between global meaning (core beliefs, goals, and self-representations) and situational meaning (the meaning appraised for a particular stressful event). Thus, meaning-making is the active search for meaning in response to a stressor, and it is a coping mechanism provided by religion. The associations among meaning-making, religion, and adaptive coping are supported by other studies linking meaning-making with physical and emotional well-being in the face of suffering. Büssing et al. (2005), for example, found that cancer patients experienced greater psychological adjustment when they derived meaning from their medical experiences. Edmondson et al. (2008) found that religious beliefs buffered the fear of dying and decreased the likelihood of major depression in individuals with terminal illnesses. Park and Folkman (1997) also associated the activation of religious beliefs and experiences as one of the mechanisms in meaning-making coping.
1.4. Theodicy
While it has been established that religion is positively linked to better health outcomes, and that meaning making is one of the mechanisms of adaptive coping, much less is known about the specific dimensions of religion influencing this process. Theodicy, or a person’s religious beliefs regarding the presence of suffering and evil in the world, has become a growing area of interest for psychologists studying religion and religious effects on mental health (Lee and Newberg 2005). Theodicy raises questions about the existence of evil and its presence in connection with an omnipotent and benevolent God (Beck and Taylor 2008; Daugherty et al. 2009; Sharp 2014). Historically speaking, in dealing with the dissonance between a benevolent God and suffering, many Christians often pointed to the “devil” or “sin” as the cause of suffering (Furnham and Brown 1992). Some research has suggested that individuals who more strongly believe in the existence of the devil have a proportionately more satisfying relationship with God and view God as less responsible for the existence of suffering (Beck and Taylor 2008). On the other hand, individuals who did not believe in the devil struggled to accept how a benevolent God could allow suffering in the world (Furnham and Brown 1992).
More recent research on theodicy suggested that individuals who viewed God as having a more active role in suffering (e.g., God is using suffering to build character) tended to report more satisfying engagement with their faith, while those who viewed God as having a more passive role (e.g., God is unable to prevent suffering) had less satisfying engagement with their faith (Wilt et al. 2017). Park et al. (2017) write, “… when a survivor confronts a personal tragedy or trauma, theodicies can provide a needed sense of cohesion and stability in the fabric of one’s meaning system” (p. 28). It follows that a person’s theodicy may have a significant impact on one’s engagement and experience of satisfaction in one’s faith, which then has implications for one’s meaning making in the face of suffering. A person’s theodicy may therefore have implications for one’s adaptive response to COVID-19.
1.5. The Views of Suffering Scale (VOSS)
The Views of Suffering Scale (VOSS) was developed by Hale-Smith et al. (2012) to provide a means of measuring individuals’ beliefs about God’s role in suffering. The VOSS measures participants’ beliefs in theodicies ranging from God using suffering to build character, to God being unable to stop suffering. To develop the measure, Hale-Smith et al. (2012) interviewed community/religious leaders from a range of traditions, read each tradition’s religious texts and teachings, and studied related psychological constructs. Items reflected nuanced Christian beliefs about God’s role in suffering, such as Free Will, Open Theism, Word-Faith, Encounter, Suffering God, and Soul-Building, as well as included differing beliefs about divine providence, unorthodox theistic beliefs (e.g., God does not care or is unloving), and nontheistic beliefs (e.g., suffering is random or the result of karma). The final version of the VOSS includes ten subscales, each representing a different view on suffering.
Six subscales reflect traditional Christian doctrine related to theistic involvement in suffering and one’s relationship with the divine. The subscale Divine Responsibility emphasizes God’s omnipotence and ability to end suffering within the boundaries God has chosen (free will), while the Suffering God subscale focuses on God’s goodness and relational presence amidst human suffering. The Overcoming subscale reflects the belief that humans can overcome suffering through prayer and/or faith in God, while the Encounter subscale includes items representing beliefs that suffering is mysterious and humans encounter God in the questions about suffering. Finally, the Soul-Building subscale emphasizes the belief that suffering is divinely intended as an opportunity for personal growth, while the Providence subscale has items representing the belief that God knows and plans all the details of suffering and is in final control over all aspects of human life.
The remaining four subscales incorporate beliefs that are less traditional or non-theistic in language. Specifically, the subscale Limited Knowledge includes items that are theistic but reflect the less traditional view that God does not protect humans from suffering because God does not know when or how suffering will happen (not omniscient). The Unorthodox subscale, which also includes theistic beliefs, represents views of God as not all good or all loving. Even though the final two subscales do not use theistic language, they contain potentially religious constructs, such as punishment. Thus, Hale-Smith et al. (2012) emphasized the importance of using these subscales even with religious populations. These subscales are Retribution, which features suffering as the result of past wrongdoing (karma), while Random attributes suffering to random acts with no purpose.
1.6. Theodicy and Well-Being
While it has been established that religiousness may be a protective factor in mental health outcomes during COVID-19, little is known about the specific role of theodicy in that protective mechanism. Theodicy, however, has important implications for the mental health field. Wilt et al. (2016) found that those who endorsed a theodicy in which God was viewed as more passive (e.g., God cannot control suffering) were more likely to have higher levels of depression, anxiety, and stress, whereas those whose theodicies incorporated a more active God (e.g., God suffers with people) had higher mental health satisfaction and lower levels of depression, anxiety, and stress (Wilt et al. 2017). Research studies conducted with veterans produced similar results. Beliefs in a retribution theodicy (suffering is God’s punishment for sin) led to increased anxiety and spiritual distress. In contrast, a theodicy in which God suffers with people led to lower levels of anxiety and spiritual distress (Harris et al. 2018).
A study examining the relationship between theodicies and PTSD found that survivors of a traumatic natural disaster who had benevolent theodicies of God (God has control over suffering, is suffering with us, or utilizes human suffering to build character) were less likely to experience the PTSD symptoms which often develop when core beliefs about the world are challenged (McElroy-Heltzel et al. 2018). Characteristics which tended to be attributed to a more active God included loving, kind, and benevolent, whereas the characteristics associated with a more passive God included punishing, angry, and authoritarian (Van Tongeren et al. 2019). The VOSS is useful for measuring individuals’ beliefs about whether God’s role in suffering is active or passive, or whether suffering is random. Given the relationship between these beliefs and individuals’ distress in the face of suffering, the VOSS may help to predict distress.
Previous studies on theodicy that utilized VOSS have taken a variable-centered approach in examining how different theodicy views are associated with psychological well-being. Less is known about whether there are types of people who hold certain VOSS profiles (set of combination scores) and how these clusters differ on psychological well-being from a person-centered approach. Based on our knowledge, there has yet to be a study which classified individuals into profile groups based on their VOSS scores on the ten subscales. The subscales which present God as more active include Soul-Building, Suffering God, Encounter, Divine Responsibility, Providence and Overcoming, whereas those which present God as more passive include Limited Knowledge and Unorthodox. Non-theistic representations of God included Random and Retribution.
Given that COVID-19 has had a global impact on people’s anxiety and stress levels, understanding how a person’s theodicy may positively or negatively contribute to an individual’s well-being in the face of hardships would be important for clinicians, physicians, religious leaders, and community leaders. In addition, it would be important for religious communities to understand the relationship between religious commitment and theodicies.
1.7. The Current Study
This study sought to examine the association between individuals’ theodicies at the beginning of the COVID-19 pandemic and their religiousness and well-being. The targeted sample of participants were those who identified as religious/spiritual. The first aim was to classify participants into profile groups based on how they responded on the ten VOSS subscales. We anticipated having two to four distinct profile groups based on cluster analysis results. The second aim was to compare the participants’ religious commitment, COVID-19 stress, anxiety, and psychological well-being levels across the profile groups. Due to the exploratory nature of this study, we did not have a priori hypotheses.
2. Results
2.1. Participants
The sample of this study includes 233 self-identified religious/spiritual individuals. The majority identified as Christian/Protestant (81%), followed by Catholic (17%), Latter-Day Saint (0.4%) and others (3%; e.g., spiritual, agnostic). The majority of participants resided in California (64%) with the remaining scattered across 30 states, and a few outside of the US. The race/ethnicity of the sample includes 63% White, 18% Asian/Indian subcontinent, 8% Hispanic, 2% Black, 3% multiracial, and 6% other. The majority of the sample (71%) were female. The participants’ ages ranged from 18 to 83, with a mean age of 37.
2.2. Data Analysis Plan
To investigate the research questions of this study, we will first calculate a series of descriptive statistics, such as the mean, standard deviation, and Cronbach alpha for each study variable. We will next use cluster analyses to classify participants into profile groups based on their VOSS scores. Finally, we will conduct a series of ANOVA to compare the profile groups on study variables.
2.3. Descriptive Statistics
The means, standard deviations, and Cronbach alpha coefficients of the VOSS subscales, COVID-19 Inventory, DUREL, Short Warwick Edinburgh Mental Well-Being Scale, and DASS-Anxiety are presented in Table 1. The internal consistency coefficient alphas for these scales were generally in accordance with the previous published norms, with the exception of two VOSS subscales—Divine Responsibility and Unorthodox, which demonstrated lower alphas. The intercorrelations between the study variables are also presented in Table 1. COVID-19 stress was negatively correlated with three VOSS subscales—Overcoming, Providence, and Soul-Building and positively correlated with Random. DUREL was positively correlated with six VOSS subscales (i.e., Divine Responsibility, Encounter, Overcoming, Providence, Soul-building, and Suffering God), and negatively correlated with four VOSS subscales (i.e., Limited Knowledge, Random, Retribution, and Unorthodox). Well-being was positively correlated with Divine Responsibility and Overcoming, and negatively correlated with Random. Anxiety was positively correlated with Limited Knowledge and Random.
2.4. Cluster Analysis
Cluster analysis was used to empirically identify profile groups of participants based on their 10 VOSS subscale scores. A two-step procedure with both hierarchical and non-hierarchical analyses was conducted. The number of clusters was determined by following decision-making guidelines from Hair and Black (2000).
The first step of the cluster analyses was conducted with hierarchical cluster analysis using Ward’s linkage method with the squared Euclidian distance measure. The 10 VOSS subscale scores were standardized and used as variables in the analysis. The increases in the agglomeration coefficients were overall small, with an 11% increase viewed as an initial jump when the solution decreased from three to two clusters. Relatively larger increases in agglomeration coefficients indicated that the step combining two clusters resulted in a joint cluster that was markedly heterogeneous (Hair and Black 2000). We therefore chose a three-cluster solution for this study.
The second step was to follow-up with a non-hierarchical k-means cluster analysis for a three-cluster solution. The 10 standardized VOSS subscale means of the clusters from the hierarchical cluster analysis were used as starting points in the k-means analysis. A three-cluster k-means solution converged after six iterations. The three-cluster k-means analysis placed 149 participants in the first cluster (64%; 110 women, 37 men, 1 transgender individual, 1 other gender), 41 participants in the second cluster (18%; 25 women, 16 men), and 43 participants in the third cluster (18%; 30 women, 12 men, 1 other gender). There were no statistically significant differences based on gender distribution across the three groups, χ2 (6, N = 233) = 5.13, p = 0.53. There were also no significant differences in age across the three groups based on ANOVA with Tukey post hoc tests.
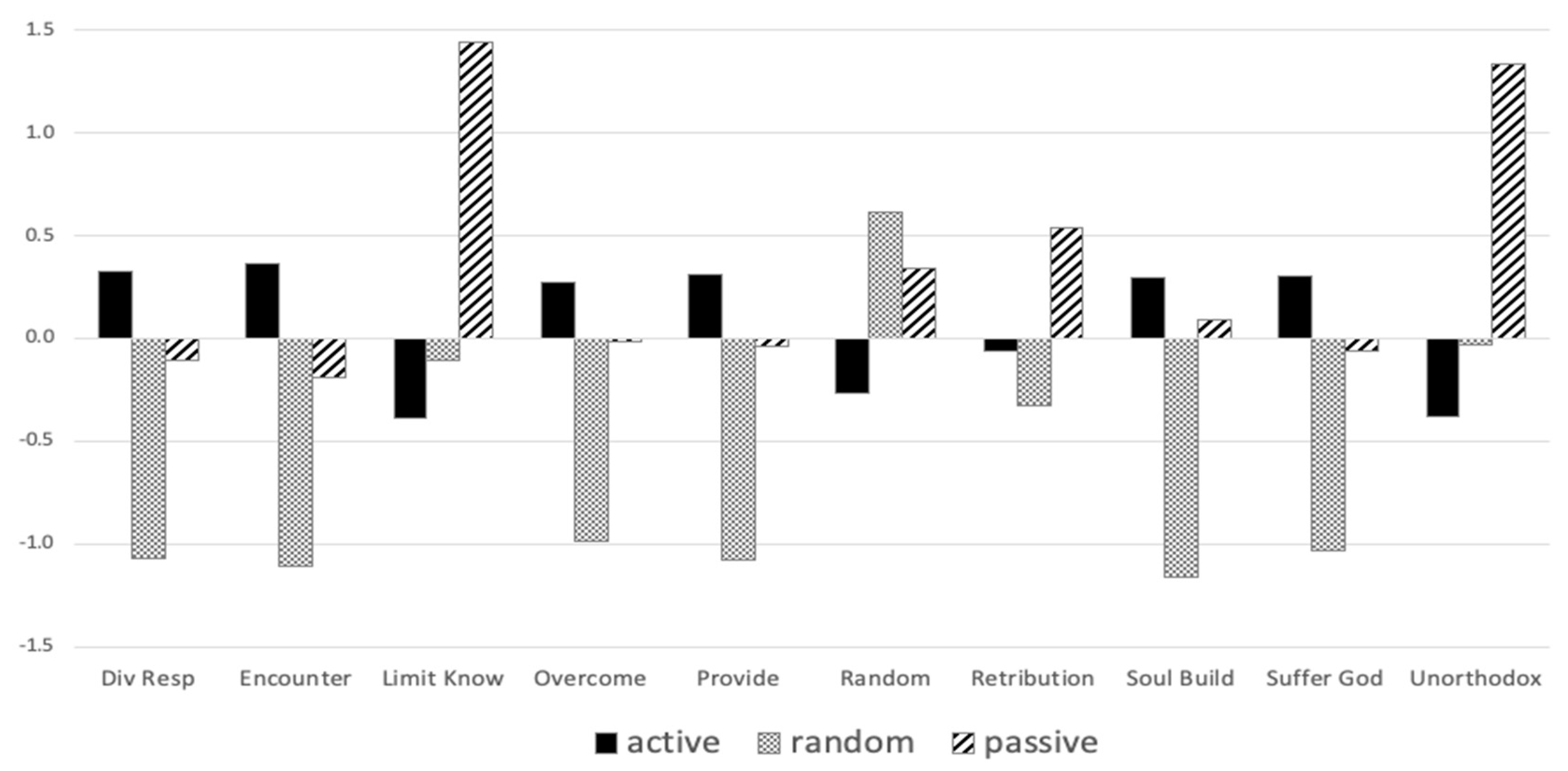
Standardized scores of all 10 VOSS subscales for each cluster group are presented in Figure 1. The first cluster scored the highest on six VOSS subscales—Divine Responsibility, Encounter, Overcoming, Providence, Soul-building, and Suffering God. These subscales all contained beliefs about suffering that reflected an active involvement of God with suffering, and they tended to have a more positive valence regarding God’s involvement (e.g., God suffers as people suffer, God will stop suffering if a person has enough faith, suffering is a way God catalyzes personal growth, God can and does intervene with suffering, etc.). As such, this cluster was labeled Active View. The second cluster had a profile with all negative VOSS z-scores, with the exception of Random. This cluster also had the highest Random subscale z-score among all three groups, indicating a belief that suffering is a random occurrence rather than related to God’s intervention or lack thereof. Thus, this cluster was labeled Random View. The third cluster scored the highest on three VOSS subscales—Limited Knowledge, Retribution, Unorthodox. These three subscales all reflect either God’s inability or lack of desire to intervene with suffering (reflecting a more negatively valenced view of God’s role), or suffering being a natural retributive consequence to wrongdoing (i.e., karma). Thus, this group was labeled Passive View.
2.5. Analyses of Variances
Analyses of variance (ANOVA) were conducted to determine if there were significant differences among the cluster groups of participants classified into Active View, Random View, and Passive View. These groups were compared on their scores for COVID-19 stress, DUREL, well-being, and anxiety. Univariate ANOVAs revealed statistically significant differences between clusters for COVID-19 stress, DUREL, and anxiety. Effect sizes (η2) for the statistically significant mean differences ranged from 0.03 to 0.28. Those in the Active View cluster reported lower COVID-19 stress than those in the Random View cluster. Those in the Active View cluster reported lower anxiety than those in the Passive View cluster. As for DUREL, those with an Active View reported significantly higher religiousness than those with a Passive View; those in the Random View cluster reported significantly lower DUREL scores than in the other two groups. These results, along with the Tukey post hoc comparisons, are presented in Table 2.
3. Discussion
This is the first study to examine different profile groups on how religious/spiritual individuals perceive God’s role in the midst of their suffering. Three distinct groups emerged, viewing God as active, God as passive, and suffering as random. Individuals who held an active view of God’s role were the most religiously committed and had the lowest level of general anxiety and stress regarding COVID-19. In contrast, those who viewed God as passive reported the highest general anxiety level. Those who viewed suffering as random reported the highest level of COVID-19 stress and the lowest level of religious commitment. However, there were no significant differences among these groups in their overall mental well-being. Taken together, these findings not only identified distinct patterns of how people tend to view God in the midst of suffering, but also provided empirical support that individuals’ views of God are associated with their religiousness and psychological status.
3.1. Cluster Profiles
The three clusters identified in the study parallel early findings in the development of the VOSS scale. The Active View cluster incorporates participants reporting higher scores on the subscales describing more traditional (orthodox) views of God’s involvement in suffering, characterizing God as an all-knowing, all-loving, and all-powerful deity. Hale-Smith et al. (2012) noted that the items in these subscales were closely related to each other in preliminary factor analyses during scale development, and the six subscales were all significantly correlated with a measure of Christian Orthodoxy. The Random View cluster also reflected the way in which the VOSS Random subscale items were initially developed to assess atheistic or agnostic views (Hale-Smith et al. 2012). Participants in the Random View cluster reported higher beliefs in the randomness of suffering, but also lower levels of beliefs associated with the divine as involved or interested in suffering.
Participants in the Passive View cluster reported views of suffering which incorporated theistic beliefs; however, this view characterized the divine being as having limited capacities to know, predict or impact suffering, as well as limited care or love for humans amidst suffering. These views are unorthodox to Christian traditions, and they were seen as separate from the traditional beliefs reflected in six of the VOSS subscales (Hale-Smith et al. 2012). However, it is interesting to note that those in the Passive View cluster also scored highest on the Retribution subscale. While these items are not written with a theistic framework, it raises the possibility that participants read items such as, “Individuals experience suffering as a result of their past wrongdoing”, with a perspective that God might be causing this retributive suffering.
3.2. Views of Suffering and Adjustment
Membership in the Active View, Passive View, and Random View clusters demonstrated unique relationships with the outcome variables in the study, suggesting that beliefs about suffering played a role in one’s adjustment to an unprecedented traumatic event such as the COVID-19 pandemic. The participants who reported a set of beliefs construing suffering as an experience where God was actively involved, intended growth, planned the details, and suffered along with participants had the most positive outcomes. These participants reported the lowest levels of Anxiety and COVID-19 distress. These findings suggest that having a global meaning structure (Park 2010), which includes theodicies where the divine cares about and is actively involved with human suffering, provides a framework to cope more effectively and develop a positive approach to the situational stressors of COVID-19.
These findings mirror other research associating positive mental health outcomes or reduced mental distress with theodicies that attributed positive characteristics to God’s involvement in suffering (Harris et al. 2018; McElroy-Heltzel et al. 2018; Wilt et al. 2017). This suggests that having a global meaning system that includes specific beliefs about God’s presence, intention, and support during suffering provides an important resource when appraising the meaning of a crisis such as the COVID-19 pandemic. Hall et al. (2021) have explored this phenomenon more deeply within Christian traditions using the construct of “sanctification of suffering” (p. 798). They write:
Generally, this sanctification has taken the form of seeing suffering as being permitted by God or in God’s will (e.g., Job 1:12, 2:6), as being used for God’s purposes (e.g., to increase perseverance; Romans 5:3–5; James 1:2–4), or as directing one toward God or connecting one with God (e.g., Philippians 3:10–11).(p. 798)
Furthermore, Hall et al. (2021) developed a Christian Sanctification of Suffering measure, which indicated that the construct is positively associated with flourishing and satisfaction, while not significantly related to negative outcomes of depression and anxiety (Hall et al. 2021). The results of this study suggest that believing the divine is active in suffering (unrelated to a specific situation) can potentially buffer possible distress in a community-wide crisis event.
The Random View cluster represents a set of participants who reported limited belief in divine involvement in suffering, as well as the strongest beliefs that suffering is a random occurrence. The random and uninvolved nature of this set of beliefs precludes the possibility of developing a sense of comprehensibility and significance (Park 2010) with regard to the pandemic. Interestingly, the random cluster reported the highest levels of COVID-19-related distress. The cluster also indicated the lowest levels of religious involvement, which may also limit access to other resources (social support, practical support, religious identity) which have been shown to contribute to resilience in the midst of a crisis (Eriksson and Yeh 2012).
Finally, the Passive View cluster members reported the highest level of anxiety. The combined beliefs reported in this cluster characterized God as the opposite of all-knowing and all-loving, and included beliefs of retribution. This suggests that those whose global meaning structure includes God, but views God as having limited involvement or knowledge, and/or lack of love and care, may be at greater risk of experiencing increased distress in situational suffering. Within this passive global meaning system, a person in crisis navigates the negative emotions related to both the stressor, as well as the lack of care from God or access to God. As noted earlier, beliefs that God is punishing have been associated with higher levels of mental distress (Harris et al. 2018; Park et al. 2017).
One theoretical construct which could help explain these findings is Terror Management Theory (TMT), a psychological orientation that attempts to explain how humans develop certain cultural worldviews and the functions these serve (Greenberg et al. 1997). Central to this theory is the belief that the awareness of death is a fundamental existential terror common to all people. In response to this terror, humans develop cultural worldviews which serve to “ameliorate anxiety by imbuing the universe with order and meaning, by providing standards of value that are derived from that meaningful conception of reality, and by promising protection and death transcendence to those who meet those standards of value” (Greenberg et al. 1997, p. 65). Multiple studies have linked aspects of religiousness (e.g., intrinsically held religious beliefs, death transcendence) to reduced anxiety and increased feelings of meaning in the face of mortality salience (Jonas and Fischer 2006; Van Tongeren et al. 2021). This suggests that religion can serve as an adaptive coping mechanism for dealing with death anxiety.
COVID-19 has increased people’s awareness of death worldwide, given the growing case numbers and death counts globally. In the face of such suffering, our findings indicated that those who had higher levels of religiousness experienced higher levels of well-being and lower levels of stress from COVID-19. Furthermore, those who had more random or passive views of God’s involvement in suffering experienced increased anxiety. These results could be representative of TMT theory, indicating that participants with higher religiousness, particularly those who had more active views of God’s involvement in suffering, possessed religious worldviews that allowed them to cope more adaptively with the suffering experienced due to COVID-19.
3.3. Limitations and Future Directions
While our findings from a predominantly Christian sample add to the existing literature on Christian views of suffering during COVID-19, there are several study limitations worth noting. First, our study uses a cross-sectional design, which does not determine causal effects. For example, it is uncertain whether participants’ theodicy profiles lead to specific psychological stress outcomes and religiousness, or vice versa. To better understand potential causal relationships, future research using longitudinal or experimental designs is needed. Second, participants were queried on their general beliefs about suffering in the midst of COVID-19, rather than specifically on how they viewed God’s involvement in, or relationship to, the COVID-19 pandemic. This distinction is noteworthy, warranting further study to examine individuals’ theodicies concerning COVID-19-specific or other collective suffering (as opposed to individual suffering). Third, exposure to COVID-19-related stressors differs among individuals, and is based on many factors. In this study, we were unable to account for all types of COVID-19-related challenges, losses, and threats. The varying impact of COVID-19 on individual participants is unaccounted for in our study, and it may represent other important factors related to the findings of this study. Future studies may examine the differing types and levels of individual suffering as potential moderators between collective suffering (e.g., natural disaster, pandemic) and psychological outcomes. Fourth, further investigation is needed to examine other constructs, such as mortality salience, against the VOSS groupings, to better clarify how our findings fit with the TMT framework. Fifth, most participants in this study were Christians from a convenience sample recruited through a snowball approach. Thus, generalizability is limited. Future studies may also want to explore the views of suffering in other religious and non-religious traditions, across different regions and countries, or more closely examine worldviews of Christian sub-groups (Hall and Hill 2019).
3.4. Practical Implications
Our research showed that there are distinct patterns of theodicies regarding suffering. Additionally, we have empirical evidence supporting the association between theodicies, religious functioning, and psychological health. Given these findings, the VOSS provides a tool for relating theodicies directly to health outcomes and informing clinical assessment and treatment planning for individuals in distress (Hale-Smith et al. 2012). For example, the VOSS can be used, either as a full assessment scale or verbal discussion of sample items, to identify risk factors for experiencing distress in how they view suffering. Situating our findings within the context of the early days of the COVID-19 pandemic is crucial. During this time period, significant upheaval was felt throughout communities and societies while limited information was available on the impact of COVID-19, specifics of how the disease was spread, and predicted outcomes for those infected. Many turned to unhealthy and maladaptive coping mechanisms (e.g., substance abuse) in the face of COVID-19 risks (Park et al. 2020). Studying theodicy is one way to help individuals and communities connect with meaning making as a way of coping.
An additional implication of our study findings is the importance of considering religious beliefs about suffering in the context of clinical interventions. Clinicians who integrate religious and theological components into their clinical work may find that clients bring more of their faith into clinical sessions after a crisis. Clinicians who are familiar with theodicies of suffering may be more likely to identify strengths and risk factors facing their clients related to their theodicies. For example, our findings suggest that theodicies in which the divine cares about and is actively involved with human suffering provide a framework leading to adaptive coping. Alternatively, individuals with theistic beliefs according to which the divine is uninvolved, lacking power, or unloving, may be at greater risk for distress and maladaptive coping in the context of a community-wide traumatic event, such as COVID-19. Incorporating conversation in therapy about religious beliefs, and not simply religious affiliation, allows for early assessment of risk factors, and clarification about the clients’ meaning-making process during a crisis (Park et al. 2017).
Another practical implication concerns raising clinicians’ and researchers’ awareness about the impact that religious and community leaders have on people’s theodicies. During times of crisis, it may be wise to examine the theodicies being communicated by religious and community groups, especially given the impact that these beliefs have on the ways that people cope. It is worth reflecting on the fact that in times of crisis, leaders are responding in real-time, the same way as others. Implicit and explicit messages they communicate about understanding suffering does impact how people will cope.
In the same way, it is also important for clinicians to examine their own theodicies in times of crisis. During the COVID-19 global pandemic, clinicians and clients are living through a shared distressing experience. Clients understand the pandemic through their theodicies, and so do clinicians. It is important for clinicians to examine and be aware of their own theodicies in order to consider potential countertransference with clients who share or do not share their views.
4. Materials and Methods
4.1. Procedure
The study was approved by the IRB of the researchers’ institution and was conducted through an online survey. Participants were recruited via a snowball approach through the researchers’ social networks, which included three of the co-authors along with a small group of research collaborators. Invitations to participate were sent by email and posted on social media with a link to access the Qualtrics online survey. Participants were first informed through the title that the study was to investigate Navigating COVID—Christian Views and Experiences and needing to be at least 18 years of age to be eligible. They were asked to give consent to participate, and then directed to a set of demographic questions, followed by several measures. The data was collected during the period April–May 2020. Despite the information that the study was to investigate Christian views and experiences, 22 participants indicated “none” on the question item asking about their religious orientation, and they were excluded from the dataset for all analyses.
4.2. Measures
4.2.1. Views of Suffering
The Views of Suffering Scale (VOSS; Hale-Smith et al. 2012) was used to measure individuals’ views on God’s role in suffering. The 30-item measure was rated on a Likert Scale ranging from 1 = strongly disagree to 6 = strongly agree. The VOSS consisted of 10 subscales—Divine Responsibility, Encounter, Limited Knowledge, Overcoming, Providence, Random, Retribution, Soul-building, Suffering God, and Unorthodox. Sample questions included “God is all-powerful and can change situations to alleviate suffering” (Divine Responsibility) and “Karma is the best explanation for individuals’ suffering” (Retribution). The scale has demonstrated adequate reliability with Cronbach alphas for subscales ranging between 0.70 to 0.89, and construct validity with various VOSS subscales correlated with related constructs such as Christian Orthodoxy, God images of Challenge, Providence, and Benevolence (Hale-Smith et al. 2012).
4.2.2. Religious Commitment
The Duke University Religion Index (DUREL; Koenig and Büssing 2010) was used to measure religious commitment. The five items were rated on a Likert Scale ranging from 1 = definitely not true or more than once a week/day to 6 = definitely true of me or rarely/never, dependent upon whether the item was phrased to be rated in a true/false or frequency manner. Sample questions included “How often do you attend church, synagogue, mosque, or other religious meetings” (organizational religious activity) and “I try hard to carry my religion over into all other dealings in life” (intrinsic religiosity). The scale has demonstrated adequate reliability with Cronbach alphas ranging from 0.78 to 0.91 and construct validity by its associations with other measures of religiousness (Koenig and Büssing 2010).
4.2.3. COVID-19 Stress
We adapted the 10-item H1N1 Swine Flu Scale (Wheaton et al. 2012) to create a COVID-19 version measuring a pandemic’s impact on anxiety and stress. Items were rated on a Likert scale ranging from 0 = not at all to 4 = very much. Sample items included “To what extent are you concerned about COVID-19?” and “How quickly do you believe contamination from COVID-19 is spreading in the U.S.?”.
4.2.4. General Anxiety
The Depression, Anxiety, Stress Scale (DASS; Lovibond and Lovibond 1995) was used to measure anxiety. In this study, we only included the 7-item Anxiety subscale. Items were rated on a Likert Scale ranging from 0 = did not apply to me to 3 = applied to me very much, or most of the time. Sample items included “I felt I was close to panic” and “I felt scared without any good reason”. The DASS Anxiety subscale scores have demonstrated adequate internal consistency reliability with a Cronbach alpha of 0.84 in a sample of Christians (Wang et al. 2021).
4.2.5. Mental Well-Being
The Short Warwick Edinburgh Mental Well-being Scale (SWEMWBS; Haver et al. 2015) was used to measure mental wellbeing. The SWEMWBS consists of seven items from the original Warwick Edinburgh Mental Well-being Scale (Tennant et al. 2007). Items were rated on a Likert scale ranging from 1 = none of the time to 5 = all the time. Sample items included “I’ve been feeling relaxed” and “I’ve been dealing with problems well”. The SWEMWBS has demonstrated strong reliability with a Cronbach alpha of 0.90 (Haver et al. 2015) and adequate construct validity through its associations with mindfulness, positive affect, and emotional regulation (Haver et al. 2015).
4.3. Statistical Software
IBM SPSS Statistics version 27 was used for the data analyses in this study.
5. Conclusions
This study demonstrates the benefits of considering a person-centered approach to understanding theodicy, and in particular when using the VOSS scale. Even within a predominantly religious sample, the three clusters of Active View, Passive View, and Random View demonstrated meaningful differences in outcomes between the groups of participants.
Author Contributions
K.T.W. lead the team in project design and data analyses. K.J.C., M.J. and M.R.C. contributed in the data collection. C.B.E. contributed in interpreting the key findings. All authors participated in the writing and editing of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Fuller Theological Seminary (#1754729-1 on 26 April 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We appreciate the contributions from Eleanor Baylon, Justine Duyst, Rachel Green, Joanna Huang, Hannah Lankheet, and Brede Parker in the data collection process. We also appreciate Eleanor Baylon’s involvement in writing parts of the earlier draft of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- APA (American Psychological Association). 2020. Stress in America 2020: Stress in the Time of COVID-19, Volume One. Available online: https://www.apa.org (accessed on 2 January 2022).
- Beck, Richard, and Sara Taylor. 2008. The emotional burden of monotheism: Satan, theodicy, and relationship with God. Journal of Psychology and Theology 36: 151–60. [Google Scholar] [CrossRef]
- Boals, Adriel, and Jonathan B. Banks. 2020. Stress and cognitive functioning during a pandemic: Thoughts from stress researchers. Psychological Trauma: Theory, Research, Practice, and Policy 12: S255–S257. [Google Scholar] [CrossRef]
- Büssing, Arndt, Thomas Ostermann, and Peter F. Matthiessen. 2005. The Role of Religion and Spirituality in Medical Patients in Germany. Journal of Religion and Health 44: 321–40. [Google Scholar] [CrossRef]
- CDC (Centers for Disease Control and Prevention). 2020a. Guidelines: Opening Up America Again. White House. Available online: https://www.whitehouse.gov/openingamerica/ (accessed on 2 January 2022).
- CDC (Centers for Disease Control and Prevention). 2020b. Mental Health: Household Pulse Survey. National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/covid19/pulse/mental-health.htm (accessed on 2 January 2022).
- Czeisler, Mark É., Kristy Marynak, Kristie E. Clarke, Zainab Salah, Iju Shakya, Joann M. Thierry, Nida Ali, Hannah McMillan, Joshua F. Wiley, Matthew D. Weaver, and et al. 2020. Delay or avoidance of medical care because of COVID-19–related concerns—United States, June 2020. Morbidity and Mortality Weekly Report 69: 1250–57. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, Timothy K., Aimee M. West, Melissa E. Williams, and Jakob M Brockman. 2009. Measuring theodicy: Individual differences in the perception of divine intervention. Pastoral Psychology 58: 43–47. [Google Scholar] [CrossRef]
- Edmondson, Donald, Crystal L. Park, Stephenie R. Chaudoir, and Jennifer H. Wortmann. 2008. Death Without God: Religious Struggle, Death Concerns, and Depression in the Terminally III. Psychological Science 19: 754–58. [Google Scholar] [CrossRef]
- Eriksson, Cynthia B., and Dow-Ann Yeh. 2012. Grounded transcendence: Resilience to trauma through spirituality and religion. In Individual Ttrauma: Recovering from Deep Wounds and Exploring the Potential for Renewal. Edited by Kathryn Gow and Marek J. Celinski. New York: Nova Science Publishers, pp. 53–71. [Google Scholar]
- Furnham, Adrian, and Laurence B. Brown. 1992. Theodicy: A neglected aspect of the psychology of religion. The International Journal for the Psychology of Religion 2: 37–45. [Google Scholar] [CrossRef]
- Gallup Inc. 2021. Religion. Available online: https://news.gallup.com/poll/1690/Religion.aspx (accessed on 2 January 2022).
- Greenberg, Jeff, Sheldon Solomon, and Tom Pyszczynski. 1997. Terror management theory of self-esteem and cultural worldviews: Empirical assessments and conceptual refinements. Advances in Experimental Social Psychology 29: 61–139. [Google Scholar] [CrossRef]
- Hair, Joseph, and William C. Black. 2000. Cluster analysis. In Reading and Understanding More Multivariate Statistics. Edited by Laurence G. Grimm and Paul R. Yarnold. Washington: American Psychological Association, pp. 147–205. [Google Scholar]
- Hale-Smith, Amy, Crystal L. Park, and Donal Edmondson. 2012. Measuring beliefs about suffering: Development of the Views of Suffering Scale. Psychological Assessment 24: 855–66. [Google Scholar] [CrossRef] [Green Version]
- Hall, M. Elizabeth, and Peter Hill. 2019. Meaning-making, suffering, and religion: A worldview conception. Mental Health, Religion & Culture 22: 467–79. [Google Scholar]
- Hall, M. Elizabeth Lewis, Jason McMartin, David Wang, Laura Shannonhouse, Jamie D. Aten, Eric J. Silverman, and Lauren A. Decker. 2021. The Christian Sanctification of Suffering Scale: Measure development and relationship to well-being. Mental Health, Religion & Culture 24: 796–813. [Google Scholar]
- Harapan, Harapan, Naoya Itoh, Amanda Yufika, Wira Winardi, Synat Keam, Haypheng Te, Dewi Megawati, Zinatul Hayati, Abram L. Wagner, and Mudatsir Mudatsir. 2020. Coronavirus disease 2019 (COVID-19): A literature review. Journal of Infection and Public Health 13: 667–73. [Google Scholar] [CrossRef]
- Harris, J. Irene, Timothy Usset, and Zhen H. Cheng. 2018. Theodicy and spiritual distress among veterans managing posttraumatic stress. Spirituality in Clinical Practice 5: 240–50. [Google Scholar] [CrossRef]
- Hart, Curtis W., and Harold G. Koenig. 2020. Religion and health during the COVID-19 pandemic. Journal of Religion and Health 59: 1141–43. [Google Scholar] [CrossRef]
- Haver, Annie, Kristin Akerjordet, Peter Caputi, Trude Furunes, and Christopher Magee. 2015. Measuring mental well-being: A validation of the Short Warwick–Edinburgh Mental Well-Being Scale in Norwegian and Swedish. Scandinavian Journal of Public Health 43: 721–27. [Google Scholar] [CrossRef]
- Horesh, Danny, and Adam D. Brown. 2020. Traumatic stress in the age of COVID-19: A call to close critical gaps and adapt to new realities. Psychological Trauma: Theory, Research, Practice, and Policy 12: 331–35. [Google Scholar] [CrossRef]
- Ishikawa, Rachel Zack. 2020. I may never see the ocean again: Loss and grief among older adults during the COVID-19 pandemic. Psychological Trauma: Theory, Research, Practice, and Policy 12: S85–86. [Google Scholar] [CrossRef]
- Jonas, Eva, and Peter Fischer. 2006. Terror management and religion: Evidence that intrinsic religiousness mitigates worldview defense following mortality salience. Journal of Personality and Social Psychology 91: 553–67. [Google Scholar] [CrossRef]
- Koenig, Harold G., and Arndt Büssing. 2010. The Duke University Religion Index (DUREL): A five-Item measure for use in epidemiological studies. Religions 1: 78–85. [Google Scholar] [CrossRef] [Green Version]
- Lee, Bruce Y., and Andrew B. Newberg. 2005. Religion and Health: A Review and Critical Analysis. Zygon 40: 443–68. [Google Scholar] [CrossRef]
- Lim, Chaeyoon, and Robert D. Putnam. 2010. Religion, social networks, and life satisfaction. American Sociological Review 75: 914–33. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, Peter F., and Sydney H. Lovibond. 1995. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy 33: 335–43. [Google Scholar] [CrossRef]
- McElroy-Heltzel, Stacey E., Edward B. Davis, Don E. Davis, Jamie D. Aten, Joshua N. Hook, Daryl R. Van Tongeren, and Jenny Hwang. 2018. Benevolent theodicies protect against PTSD following a natural disaster. Journal of Psychology and Christianity 37: 6–16. [Google Scholar]
- NFDA (National Funeral Directors Association). 2020. Situation Update: Novel Coronavirus (COVID-19). Available online: https://www.nfda.org/covid-19 (accessed on 2 January 2022).
- Oman, Doug, and Carl E. Thoresen. 2005. Do religion and spirituality influence health. In Handbook of the Psychology of Religion and Spirituality. Edited by Raymond F. Paloutzian and Crystal L. Park. New York: Guilford Press, pp. 435–59. [Google Scholar]
- Pargament, Kenneth I., Nalini Tarakeshwar, Christopher G. Ellison, and Keith M. Wulff. 2001. Religious coping among the religious: The relationships between religious coping and well-being in a national sample of Presbyterian clergy, elders, and members. Journal for the Scientific Study of Religion 40: 497–513. [Google Scholar] [CrossRef]
- Park, Crystal L. 2005. Religion as a meaning-making framework in coping with life stress. Journal of Social Issues 61: 707–29. [Google Scholar] [CrossRef]
- Park, Crystal L. 2010. Making sense of the meaning literature: An integrative review of meaning making and its effects on adjustment to stressful life events. Psychological Bulletin 136: 257–301. [Google Scholar] [CrossRef]
- Park, Crystal L., and Susan Folkman. 1997. Meaning in the context of stress and coping. Review of General Psychology 1: 115–44. [Google Scholar] [CrossRef]
- Park, Crystal L., Joseph M. Currier, J. Irene Harris, and Jeanne M. Slattery. 2017. Trauma, Meaning, and Spirituality: Translating Research into Clinical Practice. Washington: American Psychological Association. [Google Scholar]
- Park, Crystal L., Beth S. Russell, Michael Fendrich, Lucy Finkelstein-Fox, Morica Hutchison, and Jessica Becker. 2020. Americans’ COVID-19 stress, coping, and adherence to CDC guidelines. Journal of General Internal Medicine 35: 2296–303. [Google Scholar] [CrossRef]
- PeConga, Emma K., Gabrielle M. Gauthier, Ash Holloway, Rosemary S. W. Walker, Peter L. Rosencrans, Lori A. Zoellner, and Michele Bedard-Gilligan. 2020. Resilience is spreading: Mental health within the COVID-19 pandemic. Psychological Trauma: Theory, Research, Practice, and Policy 12: S47–S48. [Google Scholar] [CrossRef]
- Pew Research Center. 2020. Most Americans Say Coronavirus Outbreak Has Impacted Their Lives. Social & Demographic Trends. Available online: https://www.pewsocialtrends.org/2020/03/30/most-americans-say-coronavirus-outbreak-has-impacted-their-lives/ (accessed on 2 January 2022).
- Roberto, Anka, Alicia Sellon, Sabrina T. Cherry, Josalin Hunter-Jones, and Heidi Winslow. 2020. Impact of spirituality on resilience and coping during the COVID-19 crisis: A mixed-method approach investigating the impact on women. Health Care for Women International 41: 1313–34. [Google Scholar] [CrossRef]
- Rubin, G. James, Richard Amlôt, Lisa Page, and Simon Wessely. 2009. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: Cross sectional telephone survey. BMJ 339: b2651. [Google Scholar] [CrossRef] [Green Version]
- Seryczyńska, Berenika, Lluis Oviedo, Piotr Roszak, Suvi-Maria Katariina Saarelainen, Hilla Inkilä, Josefa Torralba Albaladejo, and Francis-Vincent Anthony. 2021. Religious capital as a central factor in coping with the COVID-19: Clues from an international survey. European Journal of Science and Theology 17: 67–81. [Google Scholar]
- Sharp, Shane. 2014. Monotheistic theodicy as imaginary face-work. Sociological Forum 29: 873–92. [Google Scholar] [CrossRef]
- Singhal, Tanu. 2020. A review of coronavirus disease-2019 (COVID-19). The Indian Journal of Pediatrics 87: 281–86. [Google Scholar] [CrossRef] [Green Version]
- Taylor, Steven, Caeleigh A. Landry, Michelle M. Paluszek, Thomas A. Fergus, Dean McKay, and Gordon J. G. Asmundson. 2020. Development and initial validation of the COVID Stress Scales. Journal of Anxiety Disorders 72: 102232. [Google Scholar] [CrossRef]
- Tennant, Ruth, Louise Hiller, Ruth Fishwick, Stephen Platt, Stephen Joseph, Scott Weich, Jane Parkinson, Jenny Secker, and Sarah Stewart-Brown. 2007. The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health and Quality of life Outcomes 5: 1–13. [Google Scholar] [CrossRef] [Green Version]
- Van Tongeren, Daryl R., Mark Sanders, Megan Edwards, Edward B. Davis, Jamie D. Aten, Jennifer M. Ranter, and Angela Tsarouhis. 2019. Religious and spiritual struggles alter god representations. Psychology of Religion and Spirituality 11: 225–32. [Google Scholar] [CrossRef]
- Van Tongeren, Daryl R., Jeffrey D. Green, and Taylor Richmond. 2021. In the valley of the shadow of death: The existential benefits of imbuing life and death with meaning. Psychology of Religion and Spirituality. Advance online publication. [Google Scholar] [CrossRef]
- Vázquez Bandín, Carmen. 2020. Only the living can witness the passing of death: Mourning in times of pandemic. The Humanistic Psychologist 48: 357–62. [Google Scholar] [CrossRef]
- Wang, Lisheng, Yiru Wang, Dawei Ye, and Qingquan Liu. 2020. A review of the 2019 Novel Coronavirus (COVID-19) based on current evidence. International Journal of Antimicrobial Agents 55: 105948. [Google Scholar] [CrossRef]
- Wang, Kenneth T., Miriam S. Kang, Hsiu-Chi Lee, and Irene Sipan. 2021. The Religious Perfectionism Scale: A cross-cultural psychometric evaluation among Christians in the United States. Journal of Psychology and Theology. Advance online publication. [Google Scholar] [CrossRef]
- Watts, Stéphanie, André Marchand, Stéphanie Bouchard, Patrick Gosselin, Frédéric Langlois, Geneviéve Belleville, and Michel J. Dugas. 2020. Telepsychotherapy for generalized anxiety disorder: Impact on the working alliance. Journal of Psychotherapy Integration 30: 208–25. [Google Scholar] [CrossRef]
- Wheaton, Michael G., Jonathan S. Abramowitz, Noah C. Berman, Laura E. Fabricant, and Bumi O Olatunji. 2012. Psychological predictors of anxiety in response to the H1N1 (swine flu) pandemic. Cognitive Therapy and Research 36: 210–18. [Google Scholar] [CrossRef]
- WHO (World Health Organization). 2020. Coronavirus Disease (COVID-19): Situation Report, 162. Available online: https://apps.who.int/iris/handle/10665/332970 (accessed on 2 January 2022).
- Wilt, Joshua A., Julie J. Exline, Joshua B. Grubbs, Crystal C. Park, and Kenneth I. Pargament. 2016. God’s role in suffering: Theodicies, divine struggle, and mental health. Psychology of Religion and Spirituality 8: 352–62. [Google Scholar] [CrossRef]
- Wilt, Joshua A., Julie J. Exline, Matthew J. Lindberg, Crystal L. Park, and Kenneth I. Pargament. 2017. Theological beliefs about suffering and interactions with the divine. Psychology of Religion and Spirituality 9: 137–47. [Google Scholar] [CrossRef]
- Yonker, Julie E., Chelsea A. Schnabelrauch, and Laura G. DeHaan. 2012. The relationship between spirituality and religiosity on psychological outcomes in adolescents and emerging adults: A meta-analytic review. Journal of Adolescence 35: 299–314. [Google Scholar] [CrossRef]
Figure 1.
VOSS subscale scores by cluster groups.


{kind=link}
Table 1.
Descriptive statistics and intercorrelations between study variables.
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Div Resp | 0.37 | |||||||||||||
| 2 | Encounter | 0.45 | 0.60 | ||||||||||||
| 3 | Limit Know | −0.10 | −0.01 | 0.82 | |||||||||||
| 4 | Overcome | 0.26 | 0.32 | 0.05 | 0.66 | ||||||||||
| 5 | Provide | 0.39 | 0.37 | −0.02 | 0.33 | 0.78 | |||||||||
| 6 | Random | −0.19 | −0.12 | 0.22 | −0.13 | −0.19 | 0.74 | ||||||||
| 7 | Retribution | 0.11 | 0.00 | 0.20 | 0.26 | −0.04 | −0.06 | 0.65 | |||||||
| 8 | Soul Build. | 0.49 | 0.41 | −0.01 | 0.34 | 0.54 | −0.21 | 0.13 | 0.86 | ||||||
| 9 | Suffer God | 0.41 | 0.52 | 0.08 | 0.36 | 0.32 | −0.11 | 0.02 | 0.30 | 0.85 | |||||
| 10 | Unorthodox | −0.15 | −0.17 | 0.42 | −0.12 | −0.02 | 0.10 | 0.17 | −0.04 | −0.24 | 0.58 | ||||
| 11 | DUREL | 0.51 | 0.46 | −0.28 | 0.24 | 0.28 | −0.25 | −0.16 | 0.27 | 0.47 | −0.42 | 0.85 | |||
| 12 | COVID | −0.10 | −0.06 | 0.01 | −0.20 | −0.22 | 0.14 | −0.05 | −0.17 | 0.02 | 0.05 | −0.17 | 0.88 | ||
| 13 | Anxiety | −0.13 | 0.02 | 0.23 | −0.04 | −0.09 | 0.21 | 0.04 | −0.01 | 0.02 | 0.10 | −0.21 | 0.30 | 0.81 | |
| 14 | Well-being | 0.25 | 0.04 | −0.06 | 0.16 | 0.09 | −0.24 | −0.02 | 0.00 | 0.07 | −0.03 | 0.25 | −0.22 | −0.44 | 0.80 |
| Mean | 12.17 | 12.68 | 4.27 | 8.94 | 9.57 | 8.65 | 5.79 | 11.10 | 13.37 | 3.86 | 4.03 | 26.99 | 3.17 | 23.92 | |
| S.D. | 2.98 | 3.39 | 2.30 | 3.16 | 4.00 | 3.51 | 2.49 | 3.69 | 3.86 | 1.89 | 0.93 | 7.46 | 3.64 | 4.04 |
Note: N = 233. Absolute correlation values greater than or equal to 0.14 are significant at p < 0.05; those greater than or equal to 0.18 are significant at p < 0.01; and those greater than or equal to 0.23 are significant at p < 0.001. Cronbach alphas are presented in bold across the diagonal.
Table 2.
Means and standard deviations by cluster groups.
| Active | Random | Passive | ||||||
|---|---|---|---|---|---|---|---|---|
| n = 149 | n = 41 | n = 43 | ||||||
| Subscale | M | SD | M | SD | M | SD | F | η2 |
| DUREL | 4.38 a | 0.59 | 3.19 b | 1.12 | 3.59 c | 1.04 | 43.91 *** | 0.28 |
| COVID | 26.11 a | 7.83 | 29.66 b | 5.53 | 27.50 ab | 7.23 | 3.86 * | 0.03 |
| Anxiety | 2.64 a | 3.14 | 3.51 ab | 3.93 | 4.67 b | 4.50 | 5.68 ** | 0.05 |
| Well-being | 24.36 | 3.73 | 23.22 | 4.75 | 23.06 | 4.21 | 2.48 | 0.02 |
Note: * p < 0.05, ** p < 0.01, *** p < 0.001. Values with differing superscripts indicate significant within-row mean score differences between the clusters, using Tukey B post hoc comparisons significant at p < 0.05.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wang, K.T.; Cowan, K.J.; Eriksson, C.B.; Januzik, M.; Conant, M.R. Religious Views of Suffering Profile Groups during COVID-19. Religions 2022, 13, 453. https://0-doi-org.brum.beds.ac.uk/10.3390/rel13050453
AMA Style
Wang KT, Cowan KJ, Eriksson CB, Januzik M, Conant MR. Religious Views of Suffering Profile Groups during COVID-19. Religions. 2022; 13(5):453. https://0-doi-org.brum.beds.ac.uk/10.3390/rel13050453
Chicago/Turabian StyleWang, Kenneth T., Krista J. Cowan, Cynthia B. Eriksson, Matthew Januzik, and Moriah R. Conant. 2022. "Religious Views of Suffering Profile Groups during COVID-19" Religions 13, no. 5: 453. https://0-doi-org.brum.beds.ac.uk/10.3390/rel13050453
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.