1. Introduction
In Australia, the aged-care industry faces scrutiny following the publication of the Royal Commission into Aged Care Quality and Safety 2021. Further to the public release of the Royal Commission findings, the sector had to engage in the turmoil of a global pandemic and implement responses to the outbreak of COVID-19 and the threat of outbreaks across its facilities. The immense pressures faced across the sector, combined with the ongoing need for aged-care professionals to keep on top of primary-research studies, serve to underline the value of a literature review in establishing a readily accessible, robust evidence base for policy and practice developments. Synthesized reviews of research are a valuable resource for time-poor aged-care managers and supervisors.
Responding to aspects of the Royal Commission, which locate spiritual care within the holistic welfare of the individual in aged care, the authors hypothesized that it was unrealistic to assume that the spiritual care of people living with dementia could be left solely to aged-care workers. We used as our definition of Spirituality that of Puchalski et al. where Spirituality is defined as ‘a dynamic and intrinsic aspect of humanity through which persons seek ultimate meaning, purpose and transcendence’ (
Puchalski et al. 2014). Spirituality is related to the sacred aspects of people’s experiences and is relational. People experience and connect with their spirituality through their “beliefs, values, traditions and practices” (
Puchalski et al. 2014). Spiritual care provided by health-based practitioners, chaplains or volunteers (including family members) works to connect people to their sources of meaning, particularly in situations of ill health. Moreover, the authors believe that an under-utilized and often ill-equipped source of spiritual care can be found in the networks of friends and relatives of the person living with dementia. This is not unproblematic. Encouraging or deploying relatives and friends to offer spiritual care requires an evidence base for more effectively understanding the emotional, psychological, and spiritual responses of the intended carers when asked to offer spiritual care. Secondly, there is only limited use of evidence-based approaches that consider how such responses might inform the design and delivery of training and preparation materials for the intended carer. Thirdly, an evidence-based approach is needed to better understand the complexities of the spiritual care of people living with dementia, where previous or current religious commitments are involved.
We approach this meta-synthesis with the following research question: how do existing training programs, if at all, identify and address causes of reluctance, or identify and nurture existing personal resources, in preparing relatives and friends to offer spiritual care to people living with dementia?
The objective of this paper is to provide a wide-ranging descriptive analysis of the existing literature on the qualitative research on the spiritual care training available for relatives and friends of people living with dementia. We apply meta-synthesis techniques to undertake this. Our qualitative meta-synthesis enables us to synthesise, combine, and interpret qualitative empirical evidence related to the spiritual care of individuals living with dementia. It offers a clear and robust comparison of the results of different studies in the field of spiritual care and ageing.
Meta-synthesis is a relatively new technique for examining qualitative research (
Jensen and Allen 1996). It provides a qualitative alternative to the systematic review; the latter typically offering a comparative analysis of quantitative research with an emphasis on a statistical analysis of the results of relevant studies. In contrast, meta-synthesis is often used for theory building, theory explication and the descriptive analysis of a phenomenon (
Finfgeld 2003;
Newton 2011). It is also used to amalgamate similar qualitative studies (
Stern and Harris 1985). Our meta-synthesis sets the foundation for our ongoing research towards the description and analysis of the role and response of relatives and friends who are offering spiritual care to people living with dementia.
There are relatively few meta-synthesis reviews to date in the field of spiritual care and dementia. The exceptions include
Ødbehr et al. (
2017), who reviewed the literature on the perception of residents’ and caregivers’ views of spiritual care and how they understand the spiritual needs of people with dementia. Additionally, Eriksen and colleagues’ (
Eriksen et al. 2020) meta-synthesis attempts to locate, interpret, and synthesize the experience of lived time for people with dementia. However, none of the studies to date has explored what personal resources and responses are involved in, or must be developed for, the spiritual care offered by friends and relatives to people living with dementia.
This meta-synthesis reviews the current field of research relating to the spiritual care of people living with dementia, particularly those instances where spiritual care is offered by friends and relatives. Moreover, it highlights the relative lack of evidence-based approaches to the design and delivery of training and preparation for relatives and friends asked to, or expecting to, provide spiritual care to people living with dementia.
The authors will integrate the findings of this meta-synthesis with responses from a two-stage Delphi (to be reported elsewhere), to design and implement an action research process that evaluates a pilot training resource intended to more effectively prepare relatives and friends to offer spiritual care to people living with dementia.
2. Methodology
The meta-synthesis is increasingly appreciated for its systematic and thorough evaluation of the evidence base informing developments in public policy and practice (
Grant and Booth 2009;
Noble-Carr et al. 2019;
Horton 2020). The contribution of the meta-synthesis to the generation of new theories and interpretations of previous research is distinct to the quantifying assumptions underlying a meta-analysis.
In this section, we describe our search strategy, detail our criteria for inclusion and exclusion of literature, and introduce the processes supporting our synthesizing approach to the literature reviewed.
2.1. Meta-Synthesis Review Process
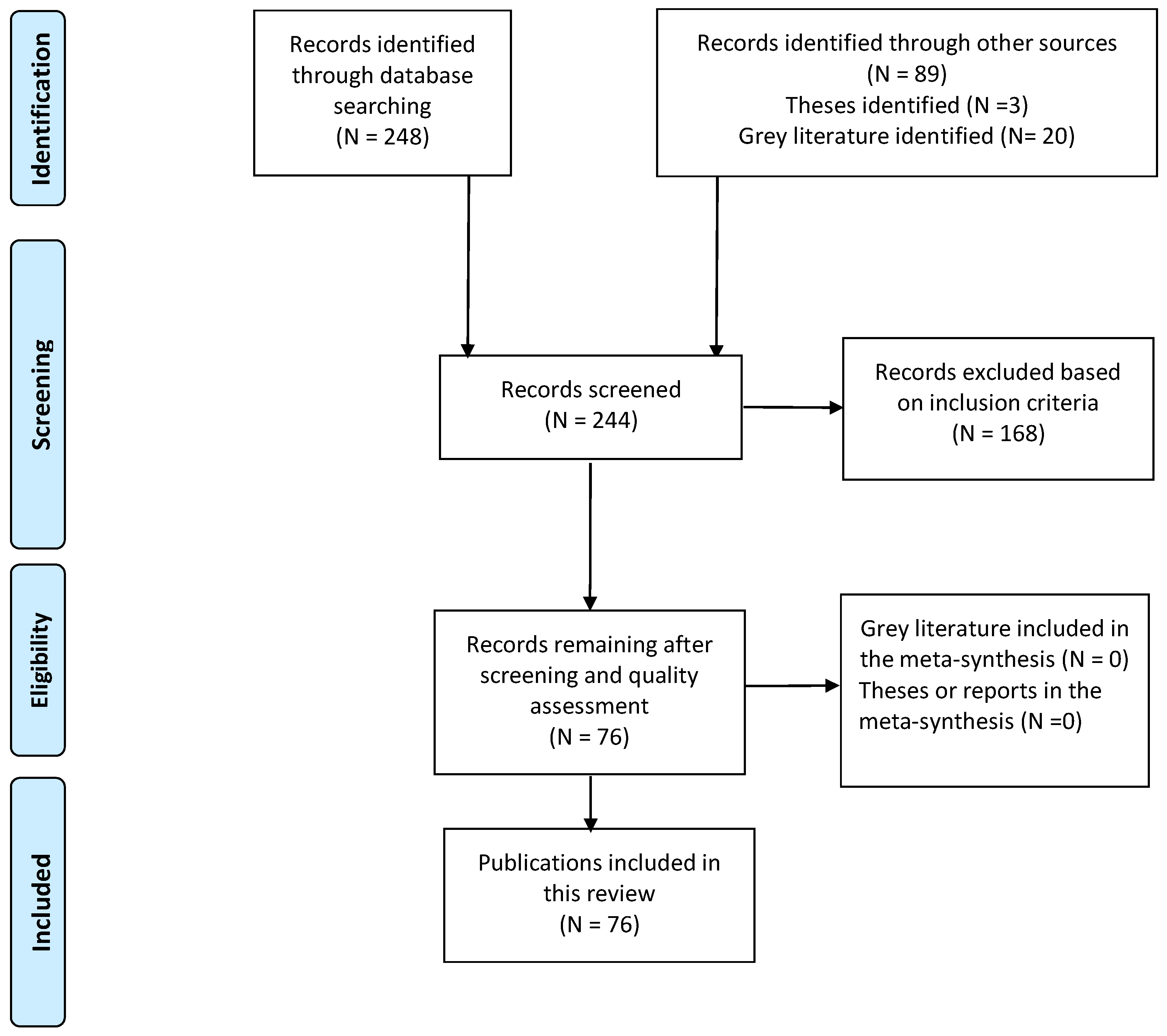
Our meta-synthesis was carried out in seven stages. Successively, these were: i. undertaking an initial literature review and drafting a research question for our research grant application; ii. with the grant awarded, our team commenced a comprehensive literature search and selection of 248 articles referencing spiritual care, spirituality, and dementia; iii. this initial selection was screened using the eligibility criteria and the resulting sample led to a selection of 244 articles that were ultimately considered for screening; iv. after applying our exclusion criteria, a total of 76 articles was assessed by the four authors to meet the quality standards of our inclusion criterion; v. synthesis of the available qualitative research findings from the 76 selected studies; vi. the presentation of our meta-synthesis around six domains; and, finally, viii. the presentation of our analysis, discussion and conclusions based on the studies synthesised. The process of the meta-synthesis is detailed in
Figure 1.
2.2. Search Strategy
Our search criteria were used to synthesise the qualitative evidence base for further investigation of the spiritual care of people living with dementia and, in particular, our research interest in the extent to which the preparation and training of relatives and friends takes account of any personal resources and/or limitations relating to the offering of spiritual care to people living with dementia.
Our search strategy required the four authors to identify and agree on the keyword combinations used to select journal and other articles. The final combinations used were: dementia and spiritual care, spirituality and ageing, families caring for people with dementia, education of families caring for people with dementia, family support and dementia, dementia care and families, spirituality and dementia caregiving, spiritual-care training, and spiritual-care education. Our search was further expanded by a careful inspection of bibliographies listed in each of the studies selected in our initial search.
Our literature search was conducted using the journal databases of the University of Divinity, Deakin University, Victoria University, Monash University, and the State Library of Victoria. Individual collections searched include: ATLA Historical Monographs Collection, BMJ Journals Collection, Academic Search Elite, PubMed Central, BioMed Central, ProQuest Academic, Public Health Database, Scopus, Google Scholar, Web of Science, and the Lancet.
2.3. Inclusion and Exclusion Criteria
From our selection of 364 articles for final consideration, 288 were excluded from the meta-synthesis because they were one or more of the following types of article:
Research focusing on clinical or medical care for dementia patients.
Academic theses or non-research reports.
Studies that did not include aspects of spiritual care for persons living with dementia or resources to equip professional care givers to dementia patients.
Studies that involved a single research subject, such as a case study.
Our inclusion criteria were the primary means of ensuring the quality of each research study under review by our research team. The criteria are common across our discipline and determined that 76 articles (see
Figure 1) were of sufficient research quality and rigour to form a part of our meta-synthesis. Our inclusion criteria are listed here:
Peer-reviewed studies published between 2000 and 2022.
Peer-reviewed studies published in English language.
Peer-reviewed studies available in Australia and internationally.
Diverse qualitative research studies on dementia care from a pastoral and spiritual care perspective.
Peer-reviewed studies focused on family and friends offering spiritual caring for dementia patients.
Peer-reviewed studies focusing on professional care givers offering spiritual caring for dementia patients.
Peer-reviewed studies exploring the inter-relationship of religiosity and spiritual care giving.
All four authors participated in the literature search and screening. Two authors carried out the first round of screening independently while two authors completed the second round by cross-checking to ensure accuracy and to eliminate the potential for bias. All studies retrieved were filtered by one, often two, members of our research team to ensure compliance with the inclusion criteria. Initially, abstract filtering was conducted, then full-text filtering, to ensure that studies related to an aspect of dementia care and the support of family and friends who are caring for persons living with dementia.
We chose articles from 2000 onwards because this period has seen significant growth in research in the issues of importance to people living with dementia and their carers, as well as in spiritual care in all health settings, including aged care.
2.4. Quality Appraisal and Analysis
The research team determined that all reviewed studies satisfy commonly accepted criteria for meta-synthesis, including those listed in
Section 2.3 above (
Atkins et al. 2008;
Thomas and Harden 2008). Quality assessment required all studies to be qualitative, have a clearly stated research methodology, sample a population of relevance to the research question, demonstrate that data-collection methods are robust and relevant to the research questions, clearly describe analytical methods, support analysis with sufficient evidence, and relate to an aspect of spiritual care offered by family and friends of people living with dementia. All four authors participated in the quality appraisal of the selected studies.
The analysis derived from our meta-synthesis falls into six domains. Arriving at the six domains was an iterative process. The initial literature review undertaken for the grant application was the basis for identifying a knowledge gap relating to the preparation and training of friends and relatives offering spiritual care to people living with dementia. A thematic analysis of our initial literature review was published in an edited, ‘Ageing and Spirituality’ thematic edition of a non-academic, quarterly publication, allowing a measure of aged-care industry review (
Jackson and Olorunnisola 2021). Our initial reflection on the relevant literature reviewed suggested the development of the six domains that we believe inform and illustrate the knowledge gap in the research literature.
Our thematic analysis, and the domains that emerge out of our analysis, were identified from our literature review and developed inductively, then synthesised using a combination of thematic and textual narrative synthesis (
Barnett-Page and Thomas 2009). This drew upon similarities and differences and allowed the grouping of descriptive themes into loose or ‘free’ codes (
Thomas and Harden 2008) to allow for progressively more focused synthesis and the eventual emergence of the six domains.
The studies selected and reviewed were subsequently grouped around one of the six domains that we believe are of most significance for the wider research project in which we are engaged, and its central research question, focused on the preparation and training of friends and relatives offering spiritual care to people living with dementia.
The six domains are centred in the following ways: the spirituality of people living with dementia; the spiritual care of people living with dementia; relatives and friends as a resource for spiritual care; spiritual-care resources; religious communities and spiritual care; and spiritual-care training for relatives and friends.
3. Results
3.1. Studies and Their Participants
Our meta-synthesis included 76 articles which reported 72 studies altogether, with five articles replicating reports on the same four studies. The included studies were conducted in Asia, Australia, Canada, Europe, Norway, the UK, and the USA. The results of our meta-synthesis are discussed below, in
Section 3.2,
Section 3.3,
Section 3.4,
Section 3.5,
Section 3.6 and
Section 3.7.
The studies under review adopted a relatively wide range of qualitative methodologies, most notably phenomenological approaches, ethnographic, and grounded theory methodologies. The data-collection methods reflected this diversity, and studies relied upon semi-structured interviews, participant observation, focus groups, and mixed-method studies.
Collectively, across all studies reviewed, the responses of at least 2698 individual participants are represented. The largest study (
Heo and Koeske 2013) was an observation study that explored the relationship between religious coping, burden appraisal, depression, and race, among 211 African-American, 220 White, and 211 Hispanic caregivers, (a total of 642 participants) using structural equation modelling (SEM). Of the two smallest studies, a semi-structured interview study in the USA explored spiritual meaning in care giving by relatives of people living with dementia (
Acton and Miller 2003). An Australian study used interpretive phenomenological analysis to examine the caregiving experiences of Italian-Australian caregivers residing in Perth (
Benedetti et al. 2013). Each of these studies had nine participants.
All the studies we reviewed included a broad range of participants depending on their research questions and focus. Several studies included the gender breakdown of participants while other did not. Ten studies were conducted with family caregivers, three studies had professional caregivers as participants, whilst several studies had a mixture of participants from different professional backgrounds, families and persons living with dementia.
3.2. Studies Related to the Spirituality of People Living with Dementia
Ambivalence regarding the benefit or necessity of spiritual care of people living with dementia: Three of the reviewed articles discuss the provision of spiritual care for people living with dementia by professionals or the spiritual beliefs of the family carers. The authors of a scoping review of papers discussing a good death for people living with dementia reviewed 11 papers from an initial set of 2729 (
Takahashi et al. 2021). Only one paper mentioned that the spiritual needs of the person living with dementia should be addressed.
Kevern and colleagues’ review of 17 papers from an initial list of 89 questioned whether spiritual or religious resources assisted those caring for people living with dementia to make meaning of their caring roles (
Kevern and Stifoss-Hanssen 2020). Only three of the studies had spirituality or religion as the focus of the research. Their research subsequently reviewed spontaneous and unmoderated posts on a spiritual-care forum on the Alzheimer’s website and analysed these using interpretive phenomenological analysis. The writers were divided between those who saw a positive spiritual benefit in caring for someone with dementia and those who struggled to see anything spiritual in it.
Ge and colleagues (
Ge et al. 2021) interviewed sixteen African-American people living with dementia, their carers, and church leaders, about the effect of COVID-19 on their Christian religious activities. They reported an increase in people living with dementia attending shorter online services, an increase in telephone and email communication, and increased home deliveries of items such as consecrated communion for some congregations. Carers described the benefit of online services and the reception of communion, shared by relatives of the person living with dementia. However, there was no discussion about the provision of spiritual care by family members.
In the paper by Chen and colleagues from Taiwan, people living with early-stage dementia were interviewed about their spirituality (
Chen et al. 2019). They discussed the importance of family members in assisting them in their spiritual needs.
The personal spirituality of the carer can be a resource for care-giving: Two interview projects with small groups focused on the caring roles and spiritual well-being of carers of people living with dementia. These demonstrate that most assessed their personal spiritual or religious practices as a resource for spiritual care giving (
Acton and Miller 2003;
Baumgardner and Mayo 2021). The participants of a video-based group support program for carers of people living with dementia also reported that their spiritual beliefs assisted them in their caring roles (
Damianakis et al. 2018).
Two reports from Jocelyn McGee and colleagues’, focusing on spirituality and caring for people with early-stage dementia, duplicated the same study, initially as a brief conference report from a conference (
McGee et al. 2020) and later an article (
McGee et al. 2021). The findings suggest that those who experienced a sense of grace in their spiritual lives were able to bring that to caring for their relatives.
The impact of diverse ethnic identity on spirituality: Four papers reported on particular ethnic or cultural groups and their spiritual care for people living with dementia and their carers. One paper interviewed twelve family members about the spiritual care of their relatives, provided by the staff in a dementia care facility in Slovenia (
Reljić et al. 2021). Their responses centre on the friendliness or dignity shown by the staff to their family members, with a brief mention of the importance of the staff knowing their relatives’ religious beliefs. Twenty-one Native-Alaskan caregivers’ responses to open-ended questions about caring for relatives living with dementia showed that not only were spiritual practices beneficial for the carers but also for the sufferers when they shared in the practices (
Fife et al. 2021). Two papers reporting on the provision of care for Italian Australians (
Benedetti et al. 2013) and Vietnamese Americans (
Meyer et al. 2015) show that a majority in both studies felt that their spiritual or religious practices helped them to cope with dementia.
Our synthesis of studies in this first domain demonstrated that understanding what is meant by the spirituality of people living with dementia is important. For some studies, the conclusion seems to be filed in the ‘too hard’ basket. Other studies showed that some carers are undecided about whether people living with dementia possess or express spirituality at all and consequently express uncertainty about the effectiveness of spiritual care. Yet other studies show that where understandings of spiritual care are aligned with specifically religious practices, it is more likely that respondents will underline the value of spiritual care. Of the studies we reviewed, most tended to locate the practice of spiritual care within a broader practice that is attentive to the holistic care of the person living with dementia. We believe there remains a need for further qualitative research that furnishes better theories and understandings of spirituality and dementia: whether it is in fact possible, whether there are particular forms it takes among people living with dementia, and whether it is more, or less, helpful to conceive of it in conjunction with religious practices and convictions. Arriving at an understanding of the spirituality of people living with dementia is important, for it is precisely this quality, or aspect of the human person, that spiritual care is intended to sustain and nurture.
3.3. Studies of the Spiritual Care of People Living with Dementia
Based on the criteria presented in
Section 2.2 and
Section 2.3, the research literature reviewed suggests a six-fold synthesis of the literature within this domain.
Studies focused on the interconnections between general person-centred care and spiritual care: These consider the crucial relationships between spirituality, spiritual care and patient-centred care and try to use this for shaping spiritual care in general (
Vincensi 2019). While, from a more medical and general healthcare perspective, others have elaborated on this approach with a high level of integration of spirituality and healthcare as a primary goal (
Puchalski et al. 2014).
Research studies oriented towards spiritual care as a dimension of palliative care: While not at the forefront of our aims in this project, the research group found a substantial body of literature focusing on spiritual care as a dimension of palliative care. Taking its starting point from a merely medical approach to care, there is strong evidence that paying attention to the nature of end-of-life care (e.g., holding off on unnecessary treatment, etc.), opens opportunities for a focus on specific elements of spiritual care (
van der Steen et al. 2014). Based on the changing needs of persons living with dementia in their final stages of life, a different and sensitive approach to spiritual care comes into view (
van der Steen et al. 2017).
Research focused on the norms, principles, and predictors of spiritual care: Studies suggest a lack of definitional and operational clarity regarding guidelines for spiritual care published in the
National Guidelines for Spiritual Care in Aged Care (
Pringle et al. 2016). While focused on the Australian context, the document gives a strong impetus to the quality of spiritual care.
Studies that investigate spiritual care for people living with dementia in specific contexts and locations: Research acknowledges the potential differences in spiritual care, depending on the context or the specific location in which spiritual care is offered. A Norwegian study looked at the possibilities for spiritual care given by nurses in nursing homes (
Ødbehr et al. 2014). New insights helped to reframe a broader view of spiritual care, enabling carers to attend to resident’s spiritual needs. Participating nurses became more aware and skilled in integrating spiritual care into general care.
Research studies developing or investigating theoretical perspectives relating to the spiritual care of people living with dementia: Several studies focused on the views of residents and caregivers about spiritual care needs (e.g.,
Ødbehr et al. 2017). Findings indicate a need for the performance of comforting religious ritual associated with a relational approach to persons living with dementia. Holistic and integrated approaches are most valuable when professional carers and providers, aware of research into spiritual care and aged care, collaborate to provide spiritual care (
Bursell and Mayers 2010). This research connects spiritual tasks in later life to the role spiritual care can play in the construction of meaning and comfort (
MacKinlay and Trevitt 2007). Research shows that theological reflection on spiritual care for people living with dementia involves an appropriate theology of care and the way the lived experience of dementia connects with this (
Goodall 2014).
Our synthesis of studies in this second domain suggested that spiritual care, where reflexively integrated with the holistic care of the person living with dementia, is of demonstrable value for end-of-life care. However, we continue to note a relative lack of evidence-based guidelines for such care. In some contexts, this appears to operate to greater effect, and this is frequently seen where a characteristically broad understanding and practice of spiritual care is associated with comforting rituals that make space, where appropriate, for familiar religious rituals.
3.4. Relatives and Friends as a Resource for Spiritual Care
Caregiving by professional carers as well as family caregivers is an onerous task that involves different levels of stress and emotional wellbeing (
Damianakis et al. 2018;
Fisher 2012;
Clissett et al. 2013). Family caregivers often carry the weight of long-term health and psychological outcomes from their caregiving to relatives living with dementia, more so than professional caregivers (
Duggleby et al. 2013).
Hope and connection: One major resource that the family provides in the process of caregiving is hope. Hope is a psychosocial resource that catalyses the social, spiritual, emotional and physical dimensions of family caregivers and the well-being of persons living with dementia. Family caregivers lean on hope to meet their own needs and to continue to stay motivated to support persons living with dementia (
Duggleby et al. 2009). Duggleby offers varying definitions of hope, illustrating how hope can strengthen connectedness (
Duggleby et al. 2013). Hopefulness informs the anticipation of a better outcome for the future or as a guarantor of a certain quality of life. Hope was seen to foster a strong connection between people living with dementia and their family, nurturing hopes, for example, that the person living with dementia might remain a functional part of the family. Even where family members had accepted the irreversible nature of dementia, there remained the hope that this continuing connectedness would increase the likelihood of a peaceful death (
Duggleby et al. 2013).
Culture and familial obligations for the spiritual care of people living with dementia: The trends in person-centred care plans among most cultural groups are influenced by filial obligation. There are certain expectations that some cultures have about how to look after their older people, especially the moral obligation of paying one’s dues to the older generation. This can determine whether to put them in a residential aged-care facility or to care for them while they live with the rest of the family at home (
Benedetti et al. 2013;
Meyer et al. 2015;
Sikes and Hall 2017;
Reljić et al. 2021).
Family and relatives can contribute to the care plans of people living with dementia by providing information about cultural symbols, objects, and family histories, to care planners. These provide points of connection to the personhood of the individual living with dementia. Such information will also prove helpful in equipping care givers intending to use reminiscence therapies that address cultural, religious, and family history. These studies imply that it is sub-optimal to plan and deliver an effective person-centred care program without at least considering the involvement of family and friends of people living with dementia.
In this third domain, our synthesis highlighted the resilience of relatives and friends that is nurtured by the psychosocial resource of hope and hopefulness at end of life. For others, the provision of spiritual care is an unavoidable familial and cultural obligation. In several studies, hope and obligation were strongly correlated with family history and religious commitment, including the use of symbolic ritual and artefacts. However, in such instances, the impact of caring for a person living with dementia upon the carer’s religious commitment is frequently ambiguous and unpredictable. In all instances, the research studies demonstrate that training for relatives and friends increases confidence and sustains hopefulness.
3.5. Spiritual Care Resources
A total of 25 studies was reviewed. Thirteen articles described or introduced the use of a variety of tools and resources intended for use in providing spiritual care for people living with dementia. Spiritual reminiscence therapy (SRT), the Dementia-Community Adaptation Model (D-CAM), procedural memory and emotional attachment (PERAT), music therapy, religious readings, or prayer were evaluated in the six qualitative studies that were reviewed for this section of our meta-synthesis.
Spiritual reminiscence therapy can tap religious life stories: SRT is a review of life stories that involve people trying to find meaning, with spirituality as a resource, in their life and their future hopes (
Elias 2018). In 2018, a meta-synthesis by Elias noted that there had been only one previous SRT study, conducted in 2002. Her meta-synthesis reviewed two studies of 39 participants in Australia and Latvia. She concluded that SRT can be an effective intervention for people living with dementia, including the likely raising awareness of transcendence, though noting the need for further research to broaden the evidence base (
Elias 2018).
Elias explored the association of identity theory with SRT in an observational study in Malaysia that made effective use of focus groups to demonstrate that SRT’s contribution to promoting connectedness and meaning, as a function of shared identity (
Elias 2018). Naediwati and Rekawati similarly emphasise the value of the collective and shared experience of SRT in their discussion of spiritual reminiscence group therapy (
Naediwati and Rekawati 2019) and note demonstrable benefits for elderly patients with mental-health incapacities, noting a reduction in loneliness, anxiety and depression.
Religious practices, connection through attentive presence, and spiritual care: Our literature search revealed numerous articles describing a wide range of religious practices and attendance at religious services. However, very few met our criteria for inclusion in this meta-synthesis. Smeaton and Maher’s literature review of 56 such articles describes practices that emphasise sensory, non-cognitive spiritual practices. These include the use of art, music therapy, religious symbols, SRT, and PERAT (
Smeaton and Maher 2016). Whilst the articles reviewed by Smeaton and Maher undoubtedly represent expert opinion on the use of these various practices, relatively few systematic research studies have been conducted in relationship to them.
Attending multisensory religious services as connection and identity: Attendance at multisensory, or ‘dementia-friendly’, religious services has been argued to promote social support and connectedness. Attendance at religious services is discussed separately, although it can be considered a subset of ‘religious practices’. However, the social and communal benefits are worth noting separately. In an ethnographic study of twelve participants in Arkansas, Beuscher and Grando highlight the use of prayer, readings from the Christian Bible, and continuing involvement in appropriate ministry roles (
Beuscher and Grando 2009). They showed that these practices sustained faith and reliance on God, sustained social connection, and nurtured a sense of hopefulness.
Epps and colleagues’ observational research on 60 African-American participants involved in church attendance suggests that the social support of the attentive presence of other churchgoers helped attune the individual living with dementia to transcendence, and deepen their connection to others (
Epps et al. 2019). They also identified care-giver stressors and noted the use of a Dementia-Community Adaptation Model (D-CAM) to address stressors and related factors.
Synthesis of findings in this fourth domain demonstrated that the capacity of therapeutic approaches to spiritual care can raise awareness of transcendence, promote connectedness and meaning, and reduce anxiety and depression. In contrast, there is a more limited evidence base for the extent to which attendance at religious services confers similar benefits, though smaller-scale studies suggest this is a potentially fruitful area for further research. Such studies note social and communal benefits, and point to the likelihood of increased connectedness and hopefulness.
3.6. Religious Communities and Spiritual Care
Religious Communities and spiritual care: Religious communities have a role to play in the spiritual care of people living with dementia. Our meta-synthesis highlights the emergence of the ‘Dementia Friendly Communities’ movement in the UK, which has resulted in advancing a dementia-friendly church (
Kevern and Primrose 2020), and ‘Dementia-friendly faith village worship services that are of great support for African American families’ (
Epps et al. 2019,
2020).
Religious communities encourage inclusion and belonging: They can provide a structured environment for families and friends of people living with dementia as well as assisting the dementia sufferer to cope better. Religiosity can be organizational (formal communal meetings including worship services), non-organizational (individual prayer or liturgical activities), and subjective (the significance an individual’s attributes to religious belief or practice) (
Despoina et al. 2018). Creating a familiar religious environment for people living with dementia can support a reconnection to lost memories, particularly where this includes religious texts or symbols with which the person living with dementia is familiar (
Despoina et al. 2018;
Epps et al. 2020). Religious communities have improved the quality of life for people living with dementia by organising needs-based religious programs, services of worship, or musical activities that are sympathetic to the prior, or current, spirituality of persons living with dementia (
Heo and Koeske 2013).
Dementia-aware worship: Worship service attendance can provide an opportunity for socialisation, a renewed sense of personhood, and reconnection with others in a familiar environment (
Epps et al. 2020). It can foster a sense of belonging, inclusion, and increased positivity. Worship services must be sensitive to the needs of the dementia patient, emphasising simplicity of format, and the use of familiar imagery, symbols, and sounds (
Epps et al. 2020). Multi-sensory approaches have particular value in residential and specific worship contexts (
Walters 2007;
Schultze 2012). Rituals, music, tangible liturgical rhythms, symbols, and art contribute to the spiritual care of dementia patients.
In the face of these research reports, other studies show that it is often problematic for people living with dementia to participate in religious gatherings, as indicated by their reduced participation in religious gatherings. The level of personal energy required to participate, the burden of care on the family and carers, and the stigma associated with dementia in public settings often constitute hindrances to religious participation (
Katsuno 2003;
Kevern and Primrose 2020). Running a dementia-friendly service requires expertise and resources to enable adequate participation. Most religious communities are only able to run dementia-friendly worship privately (
Plunkett and Chen 2016;
Kevern and Primrose 2020).
While the intellectual and cognitive aspects of religion continue to decline in a person living with dementia, one study suggests a strategy of compensation in which greater attention is paid to other elements of religion, such as appealing to the senses, encouraging touch and bodily engagement, and focussing on the communal and mystical experience of God (
Wrigley-Carr 2021). Ignatian meditation, as a form of spirituality, has proven useful for nurturing the spirituality of people living with dementia by stimulating the senses and the imagination of the person living with dementia (
Wrigley-Carr 2021).
Our synthesis of studies in our fifth domain identified a growing number of dementia-aware religious communities experimenting with multi-sensory religious rituals and collective experiences. Inclusion and belonging associated with familiar religious environments can reconnect the person living with dementia to forgotten memories and identities. Our synthesis suggests that religious communities might usefully develop forms of attentive presence that rely upon spiritual care that values and nurtures forms of spirituality associated with the non-cognitive, the mystical, the meditative and the sensory.
3.7. Spiritual Care Training for Relatives and Friends
Spiritual-care education or training was referenced in 33 studies. Fifteen quantitative and eleven non-qualifying studies were excluded, leaving seven studies that were primarily focused on the training of professional care staff, social workers, end-of-life specialist nurses, or chaplains involved in palliative care. In one study, patients were involved in the co-design of training resources and it suggested that they were happier talking to non-clergy volunteers about spirituality (
Yardley et al. 2009).
Inadequate attention to spiritual self-awareness inhibits delivery of holistic training: Baldacchino’s research demonstrates that a participatory approach to spiritual-care training facilitated spiritual self-awareness of the carers. This becomes a valuable resource that complements ‘theoretical’ knowledge of spiritual-care provision to the recipient (
Baldacchino 2011;
Chahrour et al. 2021;
Viftrup et al. 2021). Chahrour concludes that ‘You cannot talk about death if you have not processed the concept of your own death’ in outlining research which demonstrates that effective spiritual care draws on spiritual self-reflection, self-awareness, introspection and vulnerability (
Chahrour et al. 2021). Viftrup underscores the importance of the carer’s self-awareness of their spiritual needs, beliefs and values (
Viftrup et al. 2021).
Co-designed training and non-coercive spiritual care: Two studies strongly emphasized the co-design of spiritual-care training (
Yardley et al. 2009;
Viftrup et al. 2021), with Yardley’s research including patient perspectives that encouraged carers to learn and practice how to ask non-coercive spiritual-care questions (
Yardley et al. 2009). Their fears were evidenced by expert informants who insisted that while spiritual care
might be initiated by either the carer or the patient (
Yardley et al. 2009), the patient must retain control of any spiritual care offered (
Puchalski et al. 2009).
Viftrup’s research evaluates a co-designed training curriculum that integrates theoretical perspectives, self-reflection, and improvised scenarios with professional actors (
Viftrup et al. 2021). Both
Baldacchino (
2011) and
Viftrup et al. (
2021) offer research-led curriculum evaluation, an important corrective to Chahrour’s observation that their research was unable to identify any studies focusing specifically on developing and evaluating an educational course on delivering spiritual care.
The benefits and impact of spiritual care training: All studies positioned spiritual care as a component of holistic care, mostly in palliative care settings. Several studies highlighted the value of training in helping to develop a shared spiritual language (
Chahrour et al. 2021;
Tornøe et al. 2015;
Viftrup et al. 2021;
Yardley et al. 2009). In the case of people living with dementia who are cognitively impaired, there are several studies that demonstrate how training can better equip carers to offer non-cognitive responses. Among these, one advocates for a more holistic bio-psychosocial spiritual-care model (
Puchalski et al. 2009), a second emphasizes the importance of active presence and silence as a means of consolation (
Tornøe et al. 2015), and several studies outline elements of training curricula that position the carer as an agent of change through vulnerable encounter (
Chahrour et al. 2021;
Viftrup et al. 2021;
Tornøe et al. 2015;
Yardley et al. 2009).
The Norwegian study we reviewed established several quite concrete training impacts upon the trainee carers, including increased courage and competency to provide spiritual care that deals with fear and uncertainty, providing thoughtful preparation for attentive presence (at the bedside), and identifying spiritual suffering and conveying consolation in such instances (
Tornøe et al. 2015).
Relatives and friends as community spiritual carers: As noted above, in only one study were volunteer carers referenced during the research undertaken (
Yardley et al. 2009). Yardley’s research suggests that, when patients have a chance to co-design training for spiritual care, they see a potentially greater benefit from volunteers offering spiritual care than professional clergy (
Yardley et al. 2009). Puchalski’s report of expert informants helps to identify the use of a ‘community carer’ for the non-professional care of people living with dementia (
Puchalski et al. 2009). We will continue to evaluate the usefulness of this language as we attempt to develop our own training resource for the volunteer relatives and friends offering spiritual care to people living with dementia.
As we do so, we will remain alert to research that we may have inadvertently overlooked that more directly addresses our research question. Until such time, we remain convinced that, whilst our initial literature search included an encouraging number of articles that described, encouraged, or recommended the value of volunteers offering spiritual care, we are not aware of any research-led development or evaluation of training that is being offered to community spiritual carers of people living with dementia.
The synthesis of studies in our final domain suggested that community carers (Puchalski’s term for relatives and friends) are best equipped through training and preparation that prioritises introspection, self-awareness, and self-reflection. Most studies acknowledge the role of vulnerable encounter, and frequently associate this with silent consolation, attentive presence, non-coercion, and bio-psychosocial, or holistic, spiritual-care models. Acknowledging and responding to the community carer’s fears, anxieties, and uncertainty is as important as more theoretical knowledge about the experience of living with dementia.
4. A Summary of Our Meta-Synthesis Review Findings
Our meta-synthesis has been directed towards addressing our research question, ‘How do existing training programs, if at all, identify and address causes of reluctance, or identify and nurture existing personal resources, in preparing relatives and friends to offer spiritual care to people living with dementia?’
Our review of the qualifying literature, based on selection criteria outlined in section two, shows that a wide range of qualitative research studies have engaged in a reasonably extensive investigation of the spiritual care of people in palliative care, with a somewhat smaller number focused on the spiritual care of people living with dementia. Many of these studies focus on professional caregivers, including chaplains, counsellors, and social workers. However, the range of participants in these studies, including those we identify here as ‘community carers’, provides useful and generalizable outcomes.
Our meta-synthesis of these studies demonstrates that spiritual-care good practice locates it as an integral part of the holistic care of the person living with dementia. Whilst we acknowledge that there remains the need for further research to demonstrate or quantify the difference that spiritual care makes in every instance, we are satisfied that this meta-synthesis of existing research leads to the conclusion that there are demonstrable benefits where spiritual care is offered, without coercion, to people living with dementia.
Moreover, our meta-synthesis demonstrates that relatives and friends are an indispensable source of hope and connectedness, a resource for understanding cultural and familial obligations, and a source for the religiously informed personal histories and life stories that can be referenced in various forms of reminiscence therapy. Whilst relatively under-researched, a growing number of qualitative studies find value in the use of religious practices and symbols, including attendance at communal and multi-sensory religious activities. Studies consistently demonstrate that religiosity does not exhaust the category of spirituality, but it nevertheless remains central for many cultural groups in sustaining the hopefulness and connection that sustain resilience and reduce anxiety for the person living with dementia.
Our meta-synthesis demonstrates that spiritual-care training for people living with dementia sits upon a relatively limited evidence-base. Most training is directed towards understanding the phenomenon of dementia. Relatively little of the work reviewed here addresses the way that preparation addresses the spirituality of either the carer or the person living with dementia. Our meta-synthesis excluded quite a number of articles, which lack an evidence base, which nevertheless attempt to define the spirituality of the person living with dementia, outline the spiritual care that ought to be offered, or which propose or promote certain spiritual-care tools and resources. Lacking an adequate research-led evidence base, these accounts run the risk of being either ill-conceived or potentially damaging.
Evidence-based research studies excluded from our review tend to focus on the formal training of professional carers, and the inclusion of spiritual-care training within these programs is not as common as one might expect.
5. Conclusions
In conceiving of relatives and friends as community spiritual carers for people living with dementia, our meta-synthesis points towards the need for training resources that equip them with the capacity and confidence to prioritise attentive presence, acquire increased spiritual and emotional intelligence, and become more confident in the use of primarily sensory, non-cognitive, spiritual practices.
The integration of spiritual care into a holistic model of care that is bio-psychosocial requires forms of preparation and training that better prepare and equip self-reflective community carers with the skills and aptitude for attentive presence, through which they are to be understood as agents of change through vulnerable encounter.
The value of this meta-synthesis for our continuing research is its contribution to identifying a knowledge gap. It has highlighted the lack of an adequate resource to train and prepare community carers to offer spiritual care to people living with dementia. Moreover, it has anticipated the need for an evidence base on which we might conceive and develop a more effective set of formational and educational processes for preparing relatives and friends to offer spiritual care to people living with dementia. The extent to which it is necessary to do this with reference to assumptions of religiosity remain to be demonstrated.



{kind=link}
