
Comparative Evaluation of Two Glass Polyalkenoate Cements: An In Vivo Pilot Study Using a Sheep Model

Abstract
:1. Introduction
2. Materials and Methods
2.1. Glass and Cement Preparation
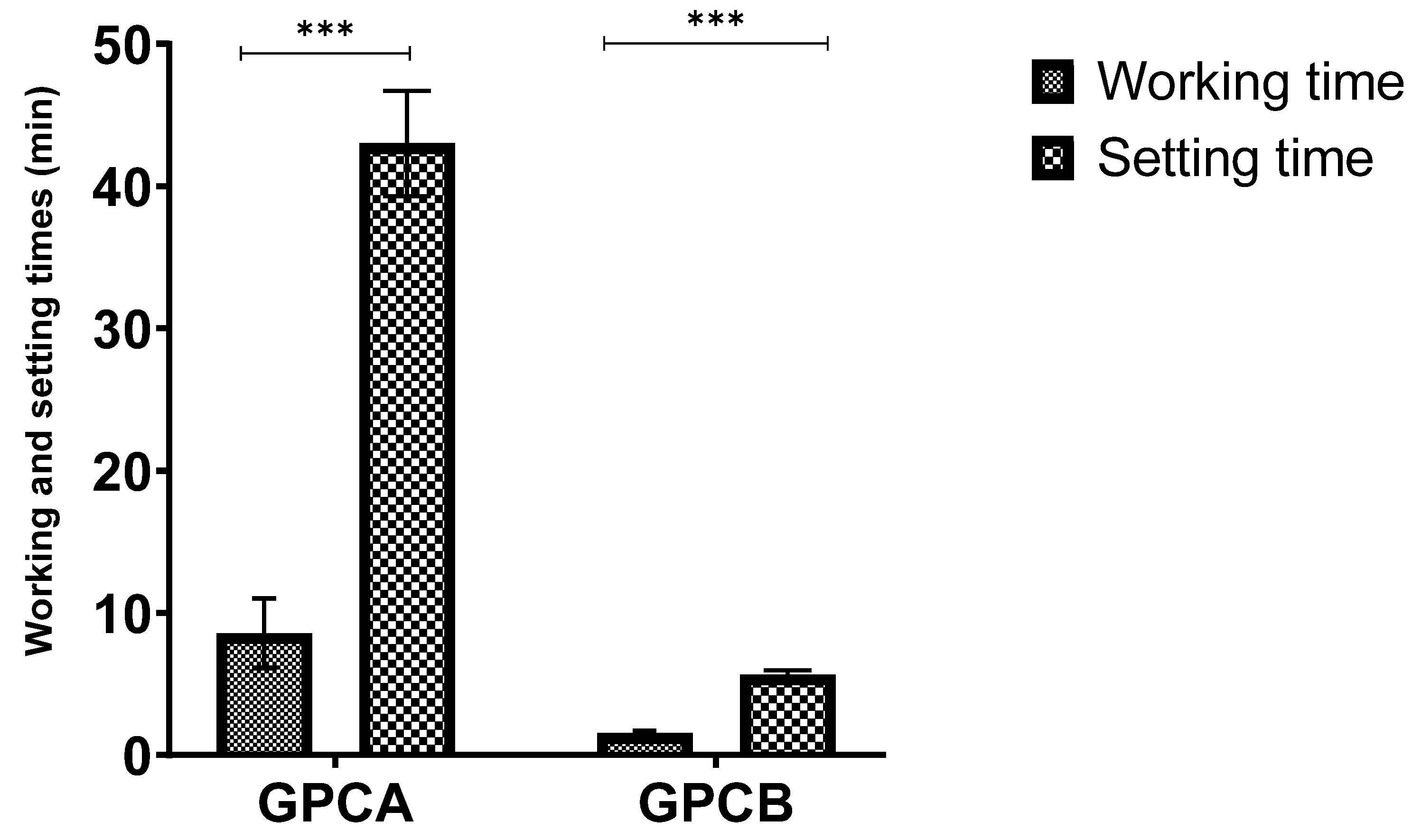
2.2. Working and Setting Times
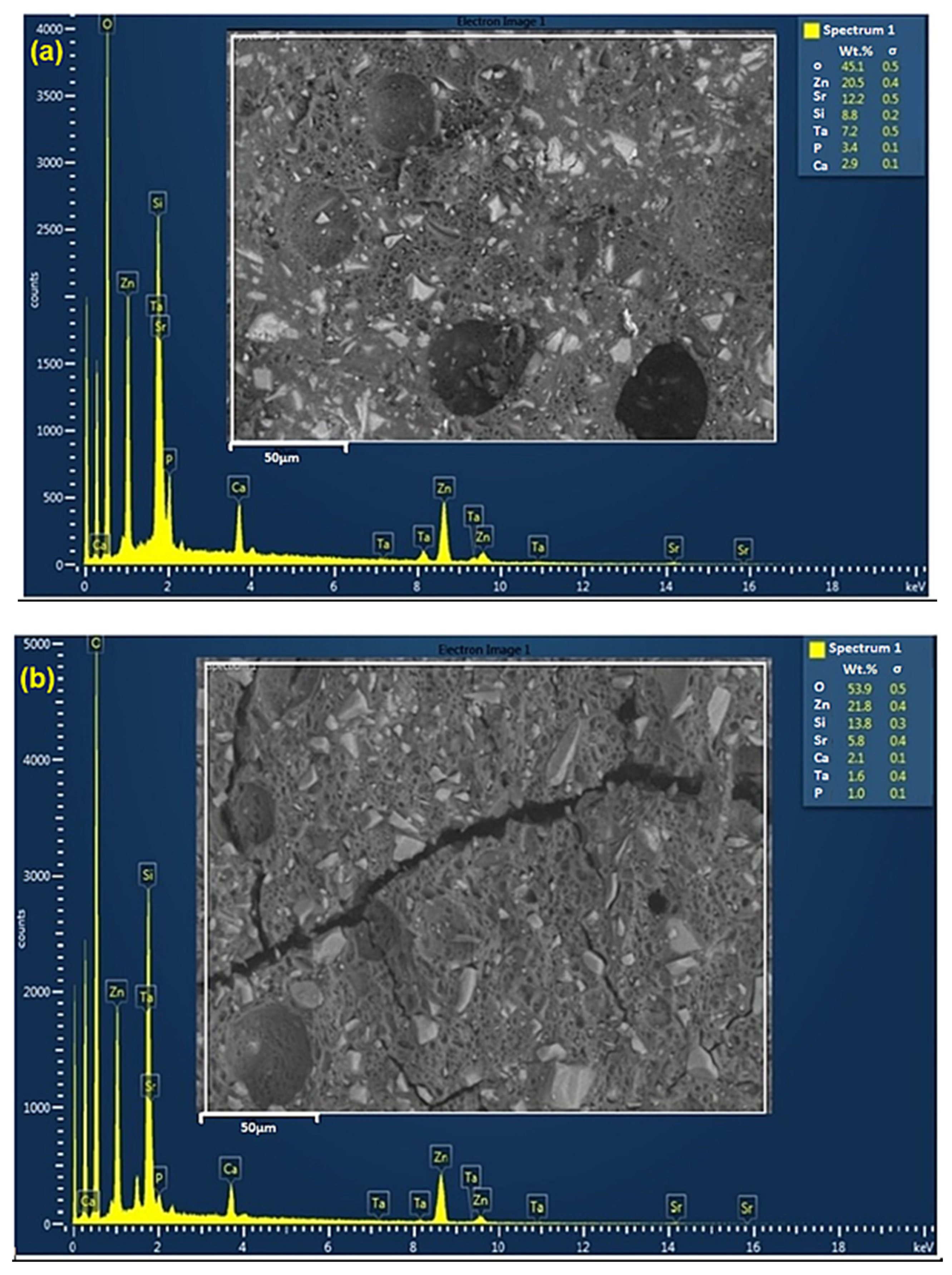
2.3. SEM-EDS Analysis
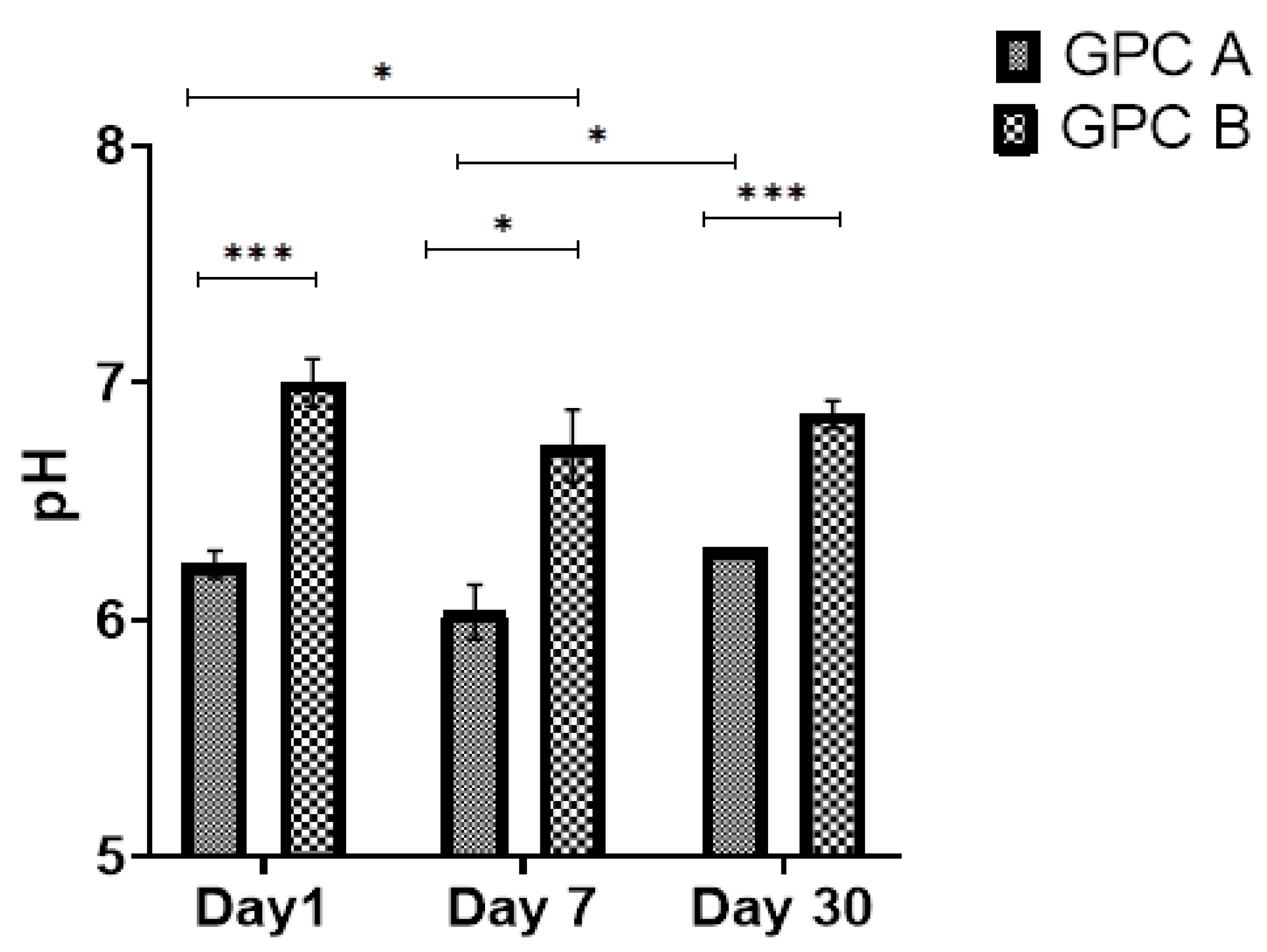
2.4. Ion Release and PH
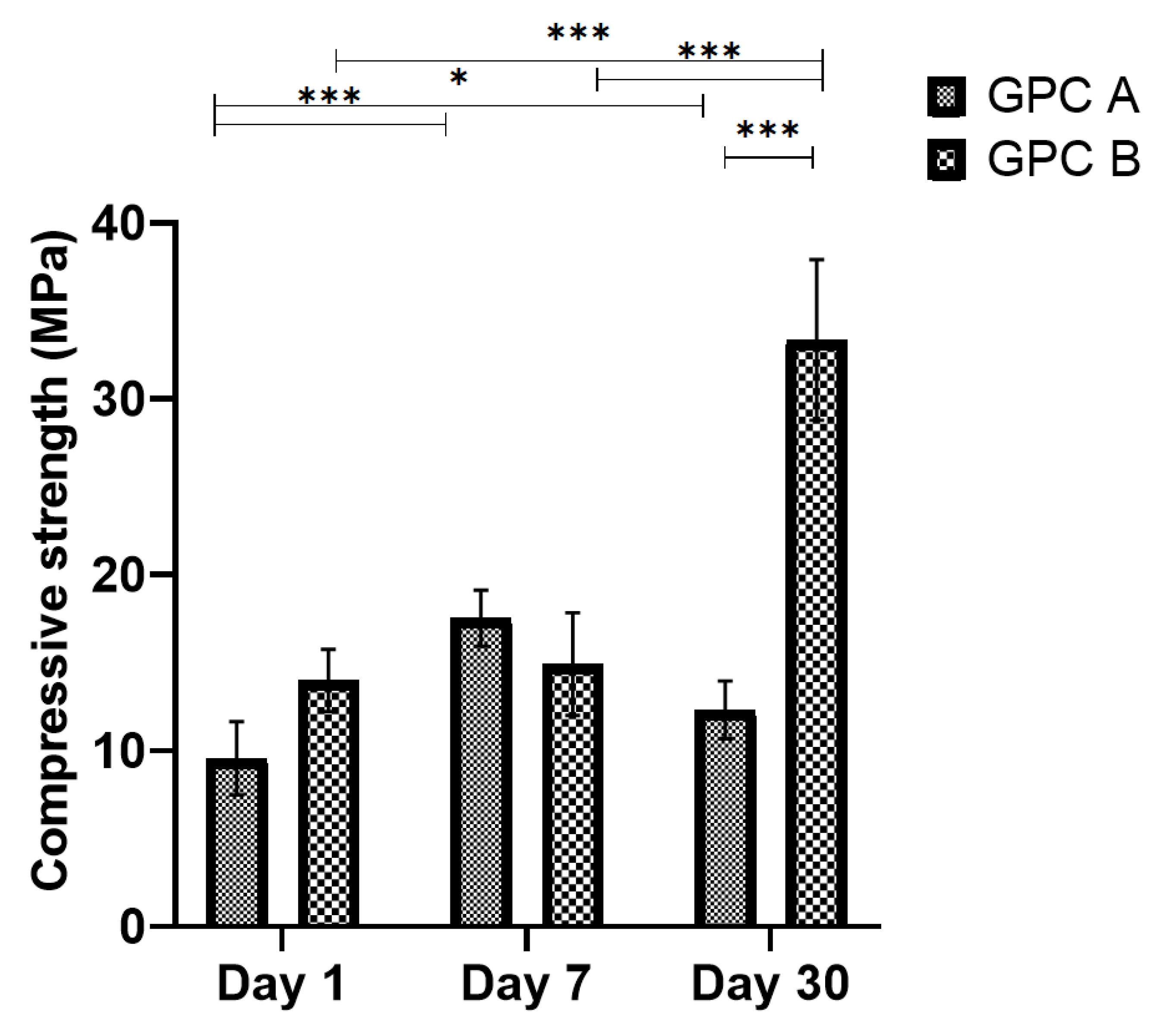
2.5. Compressive Strength
2.6. Cytotoxicity Analysis
2.7. Sheep Preparation and Material Implantation
2.8. CT/micro CT Image Acquisition
2.9. Statistical Analysis
3. Results
3.1. Working and Setting Times
3.2. SEM-EDS Results
3.3. PH Values
3.4. Ion Release Profiles
3.5. Compressive Strength
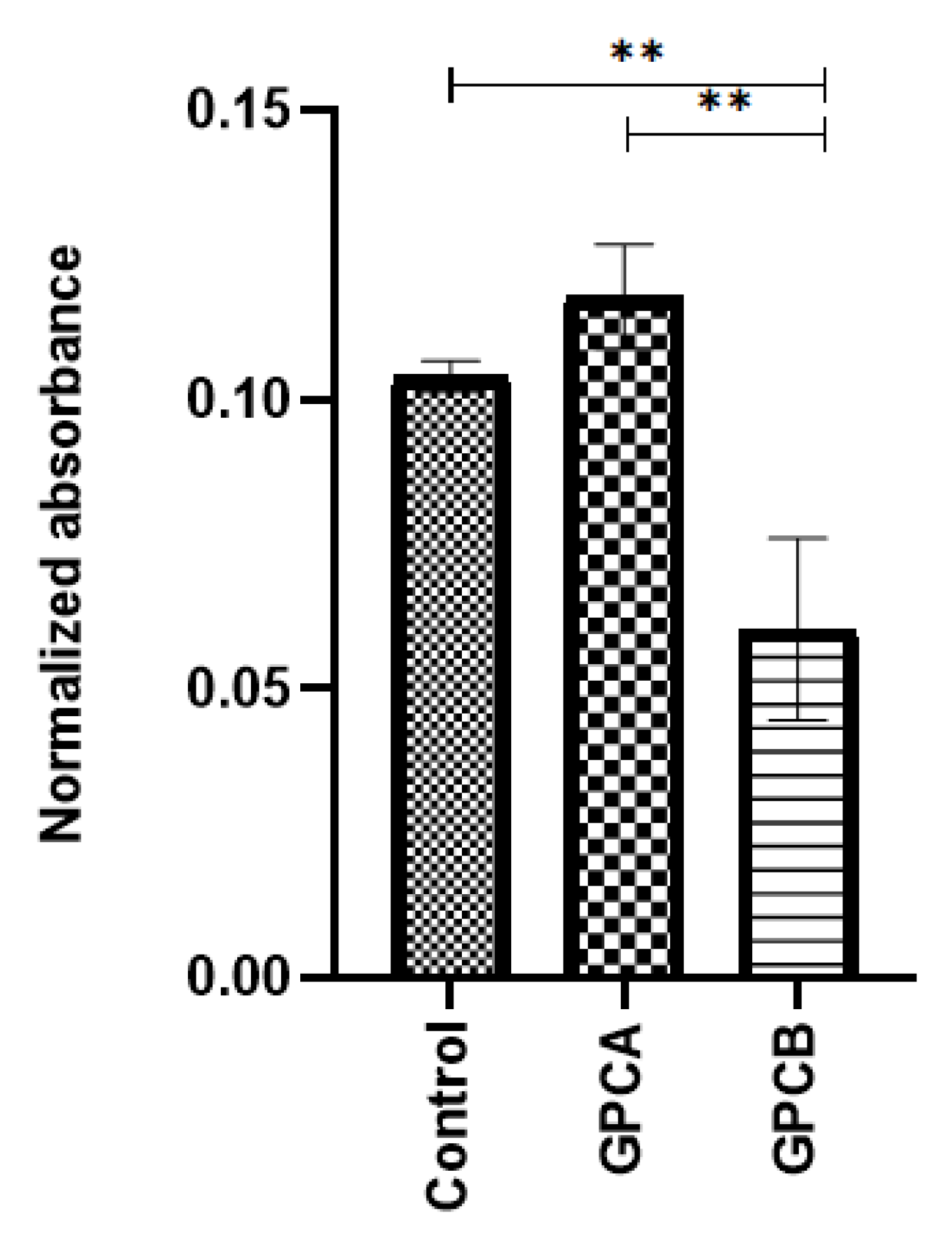
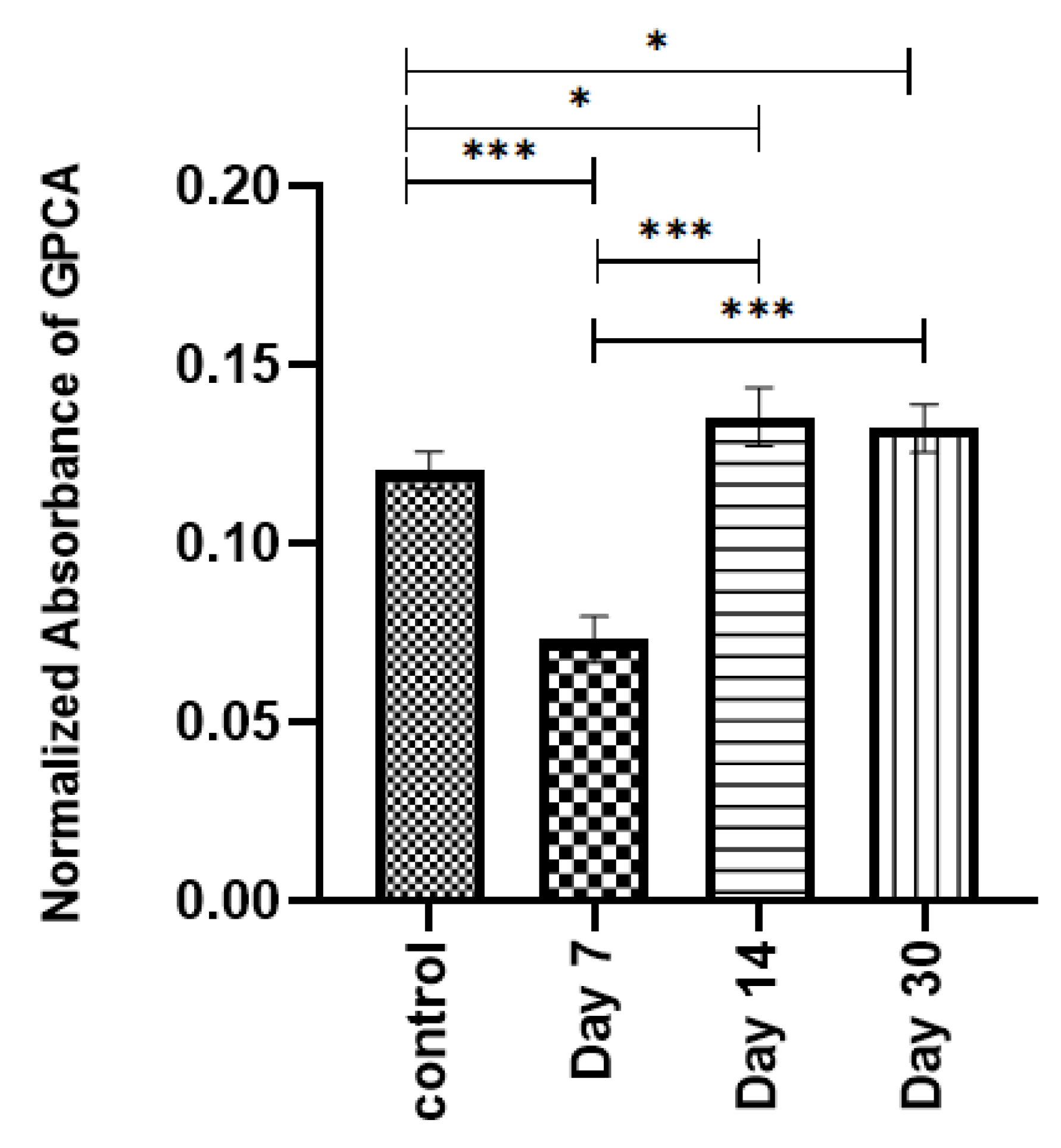
3.6. Cytotoxicity
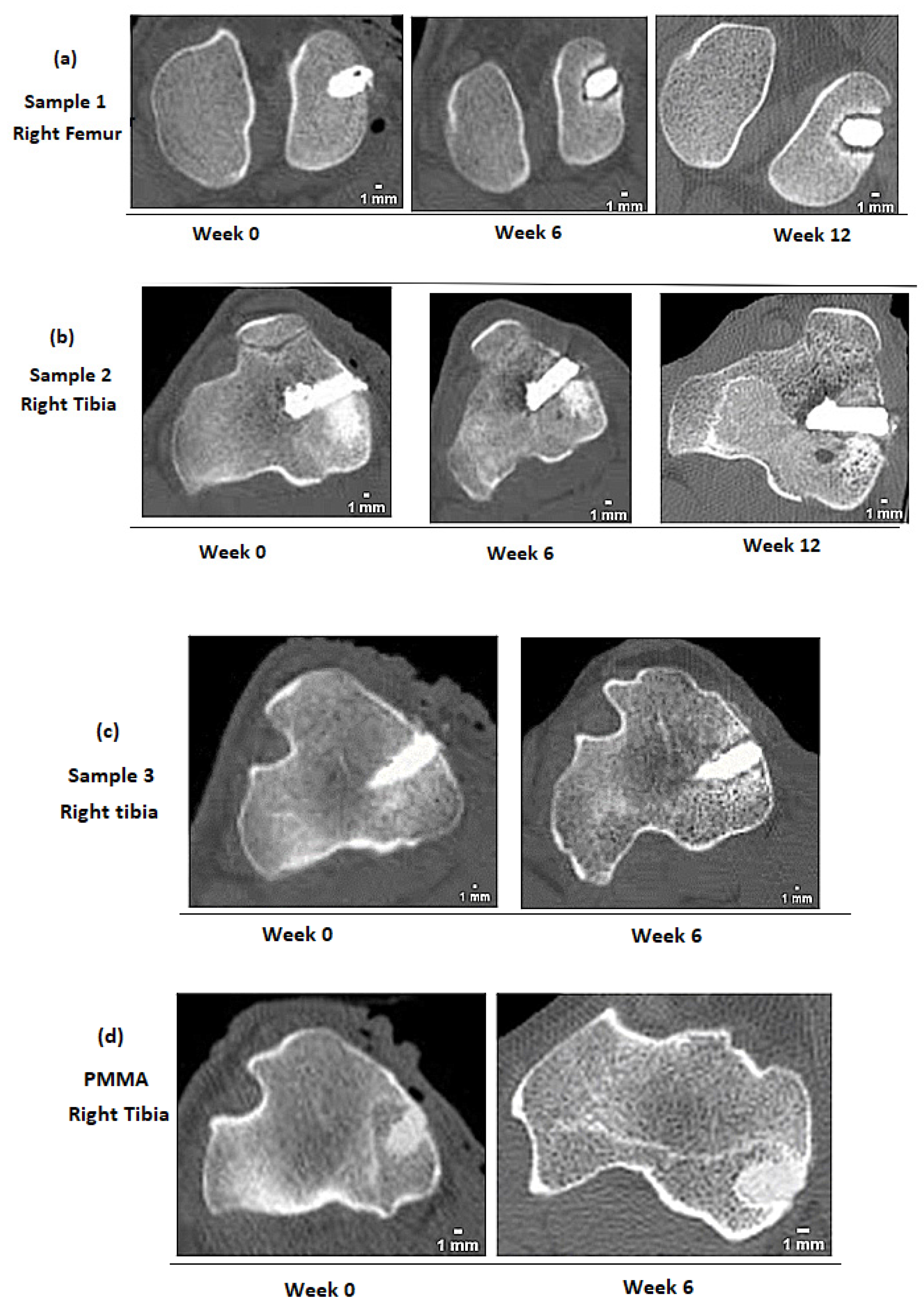
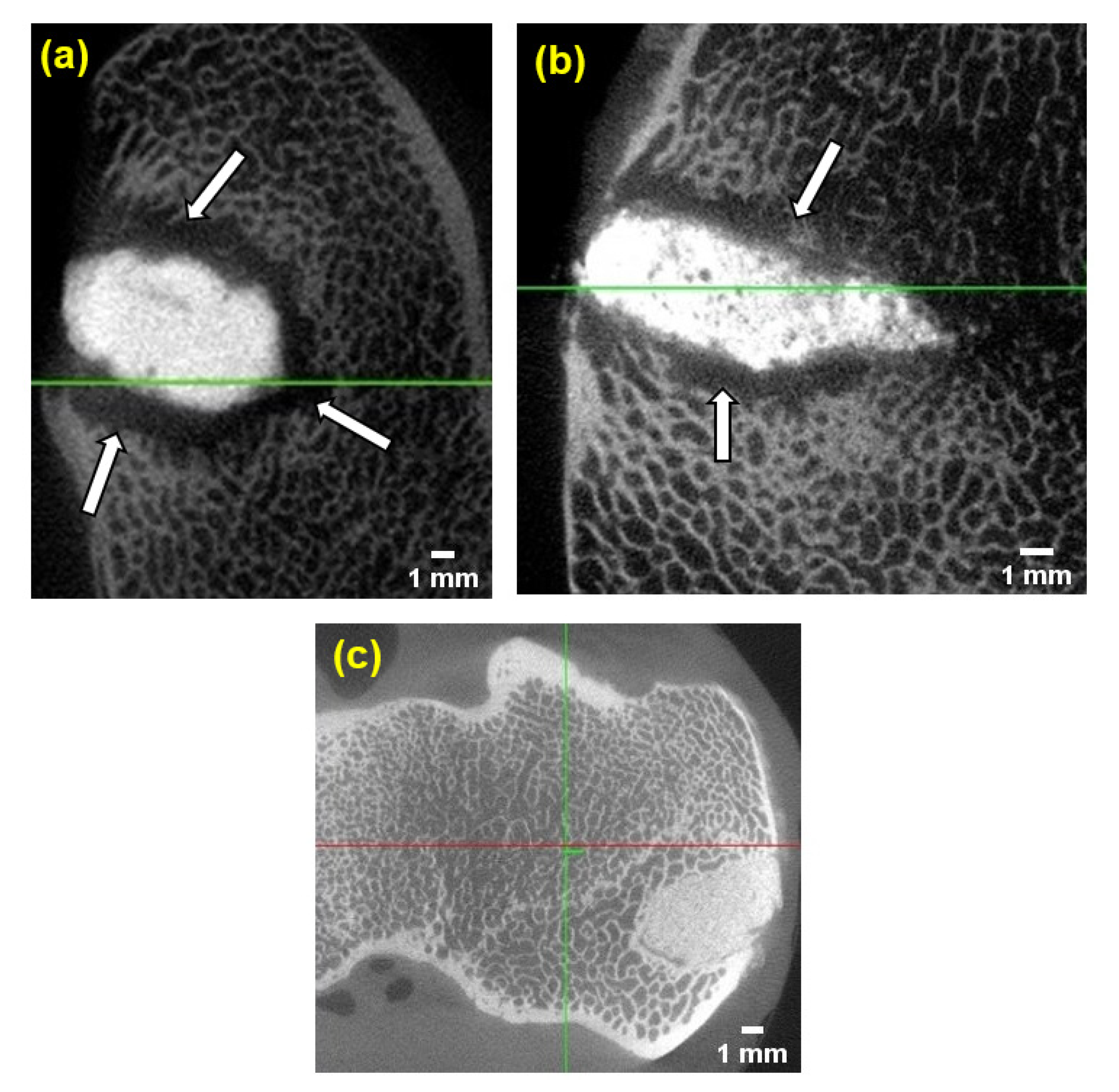
3.7. Bone Response to Implanted GPCs Using CT and Micro-CT Scan Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schwartz, A.M.; Farley, K.X.; Guild, G.N.; Bradbury, T.L. Projections and Epidemiology of Revision Hip and Knee Arthroplasty in the United States to 2030. J. Arthroplast. 2020, 35, S79–S85. [Google Scholar] [CrossRef]
- Canadian Joint Replacement Registry (CJRR) | CIHI. Available online: https://www.cihi.ca/en/canadian-joint-replacement-registry-cjrr (accessed on 11 September 2018).
- Whittaker, J.P.; Dharmarajan, R.; Toms, A.D. The Management of Bone Loss in Revision Total Knee Replacement. J. Bone Jt. Surg. Br. 2008, 90, 981–987. [Google Scholar] [CrossRef] [Green Version]
- Engh, G.A.; Ammeen, D.J. Bone Loss with Revision Total Knee Arthroplasty: Defect Classification and Alternatives for Reconstruction. Instr. Course Lect. 1999, 48, 167–175. [Google Scholar] [PubMed]
- Compston, J. Bone Quality: What Is It and How Is It Measured? Arq. Bras. Endocrinol. Metabol. 2006, 50, 579–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasandoost, L.; Rodriguez, O.; Alhalawani, A.; Zalzal, P.; Schemitsch, E.H.; Waldman, S.D.; Papini, M.; Towler, M.R. The Role of Poly(Methyl Methacrylate) in Management of Bone Loss and Infection in Revision Total Knee Arthroplasty: A Review. J. Funct. Biomater. 2020, 11, 25. [Google Scholar] [CrossRef]
- Fosco, M.; Ayad, R.B.; Amendola, L.; Tigani, D.D. Management of Bone Loss in Primary and Revision Knee Replacement Surgery. Recent Adv. Arthroplast. 2012, 1, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Qiu, Y.Y.; Yan, C.H.; Chiu, K.Y.; Ng, F.Y. Review Article: Treatments for Bone Loss in Revision Total Knee Arthroplasty. J. Orthop. Surg. 2012, 20, 78–86. [Google Scholar] [CrossRef] [Green Version]
- Abu-Amer, Y.; Darwech, I.; Clohisy, J.C. Aseptic Loosening of Total Joint Replacements: Mechanisms Underlying Osteolysis and Potential Therapies. Arthritis Res. Ther. 2007, 9, S6. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Jia, T.; Gong, W.; Wooley, P.H.; Yang, S.-Y. Effects of Ti, PMMA, UHMWPE, and Co-Cr Wear Particles on Differentiation and Functions of Bone Marrow Stromal Cells. J. Biomed. Mater. Res. A 2013, 101, 2817–2825. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, S.M.; Gautsch, T.L.; Frondoza, C.G.; Riley, L. Macrophage Exposure to Polymethyl Methacrylate Leads to Mediator Release and Injury. J. Orthop. Res. 1991, 9, 406–413. [Google Scholar] [CrossRef]
- Haas, S.S.; Brauer, G.M.; Dickson, G. A Characterization of Polymethylmethacrylate Bone Cement. J. Bone Jt. Surg. Am. 1975, 57, 380–391. [Google Scholar] [CrossRef]
- Wilson, A.D.; Nicholson, J.W. Acid-Base Cements: Their Biomedical and Industrial Applications; Cambridge University Press: Cambridge, UK, 2005; ISBN 978-0-521-67549-9. [Google Scholar]
- Boyd, D.; Clarkin, O.M.; Wren, A.W.; Towler, M.R. Zinc-Based Glass Polyalkenoate Cements with Improved Setting Times and Mechanical Properties. Acta Biomater. 2008, 4, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Crisp, S.; Pringuer, M.A.; Wardleworth, D.; Wilson, A.D. Reactions in Glass Ionomer Cements: II. An Infrared Spectroscopic Study. J. Dent. Res. 1974, 53, 1414–1419. [Google Scholar] [CrossRef] [PubMed]
- Crisp, S.; Ferner, A.J.; Lewis, B.G.; Wilson, A.D. Properties of Improved Glass-Ionomer Cement Formulations. J. Dent. 1975, 3, 125–130. [Google Scholar] [CrossRef]
- Sidhu, S.K.; Nicholson, J.W. A Review of Glass-Ionomer Cements for Clinical Dentistry. J. Funct. Biomater. 2016, 7, 16. [Google Scholar] [CrossRef]
- Alhalawani, A.M.F.; Curran, D.J.; Boyd, D.; Towler, M.R. The Role of Poly(Acrylic Acid) in Conventional Glass Polyalkenoate Cements: A Review. J. Polym. Eng. 2016, 36, 221–237. [Google Scholar] [CrossRef] [Green Version]
- Kovarik, R.E.; Haubenreich, J.E.; Gore, D. Glass Ionomer Cements: A Review of Composition, Chemistry, and Biocompatibility as a Dental and Medical Implant Material. J. Autom. Inf. Sci. 2005, 15. [Google Scholar] [CrossRef]
- de Camargo, F.L.L.; Lancellotti, A.C.; de Lima, A.F.; Geraldo Martins, V.R.; de Souza Gonçalves, L. Effects of a Bleaching Agent on Properties of Commercial Glass-Ionomer Cements. Restor. Dent. Endod. 2018, 43. [Google Scholar] [CrossRef] [PubMed]
- Blades, M.C.; Moore, D.P.; Revell, P.A.; Hill, R. In Vivo Skeletal Response and Biomechanical Assessment of Two Novel Polyalkenoate Cements Following Femoral Implantation in the Female New Zealand White Rabbit. J. Mater. Sci. Mater. Med. 1998, 9, 701–706. [Google Scholar] [CrossRef]
- Roberts, H.W.; Berzins, D.W. Early Reaction Kinetics of Contemporary Glass-Ionomer Restorative Materials. J. Adhes Dent. 2015, 17, 67–75. [Google Scholar] [CrossRef]
- Griffin, S.G.; Hill, R.G. Influence of Glass Composition on the Properties of Glass Polyalkenoate Cements. Part I: Influence of Aluminium to Silicon Ratio. Biomaterials 1999, 20, 1579–1586. [Google Scholar] [CrossRef]
- Taïr, K.; Kharoubi, O.; Taïr, O.A.; Hellal, N.; Benyettou, I.; Aoues, A. Aluminium-Induced Acute Neurotoxicity in Rats: Treatment with Aqueous Extract of Arthrophytum (Hammada Scoparia). J. Acute Dis. 2016, 5, 470–482. [Google Scholar] [CrossRef] [Green Version]
- Alhalawani, A.M.F.; Curran, D.J.; Pingguan-Murphy, B.; Boyd, D.; Towler, M.R. A Novel Glass Polyalkenoate Cement for Fixation and Stabilisation of the Ribcage, Post Sternotomy Surgery: An Ex-Vivo Study. J. Funct. Biomater. 2013, 4, 329–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Towler, M.R.; Boyd, D.; Clarkin, O. A Bone Cement. Google Patents WO2008090533A2, 31 July 2008. Available online: https://patents.google.com/patent/WO2008090533A2/en (accessed on 2 August 2020).
- Ito, A.; Kawamura, H.; Otsuka, M.; Ikeuchi, M.; Ohgushi, H.; Ishikawa, K.; Onuma, K.; Kanzaki, N.; Sogo, Y.; Ichinose, N. Zinc-Releasing Calcium Phosphate for Stimulating Bone Formation. Mater. Sci. Eng. C 2002, 22, 21–25. [Google Scholar] [CrossRef]
- Marie, P.J.; Ammann, P.; Boivin, G.; Rey, C. Mechanisms of Action and TherapeuticPotential of Strontium in Bone. Calcif. Tissue Int. 2001, 69, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Alhalawani, A.M.F.; Towler, M.R. The Effect of ZnO↔Ta2O5 Substitution on the Structural and Thermal Properties of SiO2-ZnO-SrO-CaO-P2O5 Glasses. Mater. Charact. 2016, 114, 218–224. [Google Scholar] [CrossRef]
- Towler, M.R.; Alhalawani, A.M.F.A.R. Glasses, Cements and Uses Thereof. U.S. Patent 10815144, 25 January 2018. [Google Scholar]
- Alhalawani, A.M.; Towler, M.R. A Novel Tantalum-Containing Bioglass. Part I. Structure and Solubility. Mater. Sci. Eng. C 2017, 72, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Martini, L.; Fini, M.; Giavaresi, G.; Giardino, R. Sheep Model in Orthopedic Research: A Literature Review. Comp. Med. 2001, 51, 292–299. [Google Scholar]
- An, Y.H.; Freidman, R.J. Animal Models in Orthopaedic Research; CRC Press: Boca Raton, FL, USA, 1998; ISBN 978-0-8493-2115-3. [Google Scholar]
- Pearce, A.I.; Richards, R.G.; Milz, S.; Schneider, E.; Pearce, S.G. Animal Models for Implant Biomaterial Research in Bone: A Review. Eur. Cells Mater. 2007, 13, 1–10. [Google Scholar] [CrossRef]
- Sommer, N.G.; Hahn, D.; Okutan, B.; Marek, R.; Weinberg, A.-M. Animal Models in Orthopedic Research: The Proper Animal Model to Answer Fundamental Questions on Bone Healing Depending on Pathology and Implant Material. Anim. Models Med. Biol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Newman, E.; Turner, A.S.; Wark, J.D. The Potential of Sheep for the Study of Osteopenia: Current Status and Comparison with Other Animal Models. Bone 1995, 16, 277S–284S. [Google Scholar] [CrossRef]
- Li, B.; Webster, T. Orthopedic Biomaterials: Progress in Biology, Manufacturing, and Industry Perspectives; Springer: Berlin/Heidelberg, Germany, 2018; ISBN 978-3-319-89542-0. [Google Scholar]
- Oheim, R.; Amling, M.; Ignatius, A.; Pogoda, P. Large Animal Model for Osteoporosis in Humans: The Ewe. Eur. Cell Mater. 2012, 24, 372–385. [Google Scholar] [CrossRef] [PubMed]
- Madry, H.; Ochi, M.; Cucchiarini, M.; Pape, D.; Seil, R. Large Animal Models in Experimental Knee Sports Surgery: Focus on Clinical Translation. J. Exp. Orthop. 2015, 2, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, M.; Townsend, K.; Bauer, T.; Gabriel, S.; O’Connell, M.; Clifford, A. Evaluation of the Safety of a Novel Knee Load-Bypassing Device in a Sheep Model. J. Bone Jt. Surg. Am. Vol. 2012, 94, 77–84. [Google Scholar] [CrossRef]
- Zarrinkalam, M.R.; Beard, H.; Schultz, C.G.; Moore, R.J. Validation of the Sheep as a Large Animal Model for the Study of Vertebral Osteoporosis. Eur. Spine J. 2009, 18, 244–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wancket, L.M. Animal Models for Evaluation of Bone Implants and Devices: Comparative Bone Structure and Common Model Uses. Vet. Pathol. 2015, 52, 842–850. [Google Scholar] [CrossRef] [Green Version]
- Mehrvar, C.; Deignan, E.; Hurtig, M.; Cohen, G.; Zalzal, P.; Safir, O.; Alhalawani, A.; Papini, M.; Towler, M.R. In Vivo Analysis of a Proprietary Glass-Based Adhesive for Sternal Fixation and Stabilization Using Rabbit and Sheep Models. J. Mater. Sci. Mater. Med. 2021, 32, 53. [Google Scholar] [CrossRef] [PubMed]
- Alhalawani, A.M.; Mehrvar, C.; Stone, W.; Waldman, S.D.; Towler, M.R. A Novel Tantalum-Containing Bioglass. Part II. Development of a Bioadhesive for Sternal Fixation and Repair. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 71, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Gee, E.C.A.; Eleotério, R.; Bowker, L.M.; Saithna, A.; Hunt, J.A. The Influence of Tantalum on Human Cell Lineages Important for Healing in Soft-Tissue Reattachment Surgery: An in-Vitro Analysis. J. Exp. Orthop. 2019, 6, 40. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Xie, K.; Jiang, W.; Wang, L.; Li, G.; Zhao, S.; Wu, W.; Hao, Y. In Vitro and in Vivo Study of 3D-Printed Porous Tantalum Scaffolds for Repairing Bone Defects. ACS Biomater. Sci. Eng. 2019, 5, 1123–1133. [Google Scholar] [CrossRef] [Green Version]
- Balla, V.K.; Bose, S.; Davies, N.M.; Bandyopadhyay, A. Tantalum—A Bioactive Metal for Implants. JOM 2010, 62, 61–64. [Google Scholar] [CrossRef]
- Hasandoost, L.; Alhalawani, A.; Rodriguez, O.; Yazdi, A.R.; Zalzal, P.; Schemitsch, E.H.; Waldman, S.D.; Papini, M.; Towler, M.R. Calcium Sulfate-Containing Glass Polyalkenoate Cement for Revision Total Knee Arthroplasty Fixation. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 108, 3356–3369. [Google Scholar] [CrossRef] [PubMed]
- 14:00–17:00 ISO 9917-1:2007. Available online: http://www.iso.org/cms/render/live/en/sites/isoorg/contents/data/standard/04/58/45818.html (accessed on 3 April 2019).
- Weller, R.; Sinclair, C. Chapter 25—Equine diagnostic imaging. In Equine Medicine, Surgery and Reproduction, 2nd ed.; Mair, T.S., Love, S., Schumacher, J., Smith, R.K., Frazer, G., Eds.; W.B. Saunders: Oxford, UK, 2012; pp. 499–559. ISBN 978-0-7020-2801-4. [Google Scholar]
- Barry, T.I.; Clinton, D.J.; Wilson, A.D. The Structure of a Glass-Io Nomer Cement and Its Relationship to the Setting Process. J. Dent. Res. 1979, 58, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Crowe, S.B.; Bennett, J.; Lathouras, M.; Lancaster, C.M.; Sylvander, S.R.; Chua, B.; Bettington, C.S.; Lin, C.Y.; Kairn, T. Impact of Radiopacified Bone Cement on Radiotherapy Dose Calculation. Phys. Imaging Radiat. Oncol. 2020, 14, 12–16. [Google Scholar] [CrossRef]
- Khader, B.A.; Curran, D.J.; Peel, S.; Towler, M.R. Glass Polyalkenoate Cements Designed for Cranioplasty Applications: An Evaluation of Their Physical and Mechanical Properties. J. Funct. Biomater. 2016, 7, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, A.C.; Thorpe, M.F. Eighty Years of Random Networks. Phys. Status Solidi b 2013, 250, 931–936. [Google Scholar] [CrossRef]
- Brauman, J.I. Glasses and Amorphous Materials. Science 1995, 267, 1887. [Google Scholar] [CrossRef] [Green Version]
- Shelby, J.E. Introduction to Glass Science and Technology, 3rd ed.; Royal Society of Chemistry: London, UK, 2020; ISBN 978-1-83916-141-4. [Google Scholar]
- Boyd, D.; Towler, M.R.; Watts, S.; Hill, R.G.; Wren, A.W.; Clarkin, O.M. The Role of Sr2+ on the Structure and Reactivity of SrO-CaO-ZnO-SiO2 Ionomer Glasses. J. Mater. Sci. Mater. Med. 2008, 19, 953–957. [Google Scholar] [CrossRef]
- Massera, J.; Hupa, L. Influence of SrO Substitution for CaO on the Properties of Bioactive Glass S53P4. J. Mater. Sci. Mater. Med. 2014, 25, 657–668. [Google Scholar] [CrossRef]
- Garza-García, M.; López-Cuevas, J.; Gutiérrez-Chavarría, C.A.; Piedad-Sánchez, N.; Camporredondo-Saucedo, E.; Hernández-Ibarra, O. Effect of Gradual Substitution of CaO by SrO in Glass-Ceramic Materials of the System SiO2-Al2O3-CaF2-RO (R = Ca, Mg, Sr). MRS Online Proc. Libr. OPL 2012, 1373. [Google Scholar] [CrossRef]
- Cordeiro, L.; Silva, R.M.; de Pietro, G.M.; Pereira, C.; Ferreira, E.A.; Ribeiro, S.J.L.; Messaddeq, Y.; Cassanjes, F.C.; Poirier, G. Thermal and Structural Properties of Tantalum Alkali-Phosphate Glasses. J. Non-Cryst. Solids 2014, 402, 44–48. [Google Scholar] [CrossRef] [Green Version]
- Jaidka, S.; Somani, R.; Singh, D.J.; Shafat, S. Comparative Evaluation of Compressive Strength, Diametral Tensile Strength and Shear Bond Strength of GIC Type IX, Chlorhexidine-Incorporated GIC and Triclosan-Incorporated GIC: An in Vitro Study. J. Int. Soc. Prev. Community Dent. 2016, 6, S64–S69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuya, S.; Maeda, T.; Ohta, M. IR and NMR Analyses of Hardening and Maturation of Glass-Ionomer Cement. J. Dent. Res. 1996, 75, 1920–1927. [Google Scholar] [CrossRef] [PubMed]
- Niranjan, P.; Alhalawani, A.; Phull, S.; Beniluz, I.; Krishnan, B.; Zalzal, P.; Towler, M. Injectable Glass Polyalkenoate Cements: Evaluation of Their Rheological and Mechanical Properties with and without the Incorporation of Lidocaine Hydrochloride. Biomed. Phys. Eng. Express 2018, 4, 027002. [Google Scholar] [CrossRef]
- Andersen, L.K.; Contera, S.A.; Justesen, J.; Duch, M.; Hansen, O.; Chevallier, J.; Foss, M.; Pedersen, F.S.; Besenbacher, F. Cell Volume Increase in Murine MC3T3-E1 Pre-Osteoblasts Attaching onto Biocompatible Tantalum Observed by Magnetic AC Mode Atomic Force Microscopy. Eur. Cell Mater. 2005, 10, 61–68; discussion 68–69. [Google Scholar] [CrossRef] [PubMed]
- Sagomonyants, K.B.; Hakim-Zargar, M.; Jhaveri, A.; Aronow, M.S.; Gronowicz, G. Porous Tantalum Stimulates the Proliferation and Osteogenesis of Osteoblasts from Elderly Female Patients. J. Orthop. Res. 2011, 29, 609–616. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, S.; Guo, L.; Dong, M.; Liu, B.; Mamdouh, W. Collagen Coated Tantalum Substrate for Cell Proliferation. Colloids Surf. B Biointerfaces 2012, 95, 10–15. [Google Scholar] [CrossRef]
- Balla, V.K.; Bodhak, S.; Bose, S.; Bandyopadhyay, A. Porous Tantalum Structures for Bone Implants: Fabrication, Mechanical and in Vitro Biological Properties. Acta Biomater. 2010, 6, 3349–3359. [Google Scholar] [CrossRef] [Green Version]
- Winkler, T.; Sass, F.A.; Duda, G.N.; Schmidt-Bleek, K. A Review of Biomaterials in Bone Defect Healing, Remaining Shortcomings and Future Opportunities for Bone Tissue Engineering: The Unsolved Challenge. Bone Jt. Res. 2018, 7, 232–243. [Google Scholar] [CrossRef]
- Lansdown, A.B.G. Calcium: A Potential Central Regulator in Wound Healing in the Skin. Wound Repair Regen. 2002, 10, 271–285. [Google Scholar] [CrossRef]
- Bruyne, M.A.A.D.; Moor, R.J.G.D. The Use of Glass Ionomer Cements in Both Conventional and Surgical Endodontics. Int. Endod. J. 2004, 37, 91–104. [Google Scholar] [CrossRef]
- Offermanns, V.; Andersen, O.Z.; Sillassen, M.; Almtoft, K.P.; Andersen, I.H.; Kloss, F.; Foss, M. A Comparative in Vivo Study of Strontium-Functionalized and SLActiveTM Implant Surfaces in Early Bone Healing. Int. J. Nanomed. 2018, 13, 2189–2197. [Google Scholar] [CrossRef] [Green Version]
- Morohashi, T.; Sano, T.; Yamada, S. Effects of Strontium on Calcium Metabolism in Rats. I. A Distinction between the Pharmacological and Toxic Doses. Jpn. J. Pharmacol. 1994, 64, 155–162. [Google Scholar] [CrossRef]
- Brauer, D.S.; Gentleman, E.; Farrar, D.F.; Stevens, M.M.; Hill, R.G. Benefits and Drawbacks of Zinc in Glass Ionomer Bone Cements. Biomed. Mater. 2011, 6, 045007. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-N.; Jiang, S.; Pan, H.; Tang, R. Less Is More: Silicate in the Crystallization of Hydroxyapatite in Simulated Body Fluids. CrystEngComm 2016, 18, 379–383. [Google Scholar] [CrossRef]
- Cohen-Solal, M. Strontium Overload and Toxicity: Impact on Renal Osteodystrophy. Nephrol. Dial. Transplant. 2002, 17, 30–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witek, L.; Shi, Y.; Smay, J. Controlling Calcium and Phosphate Ion Release of 3D Printed Bioactive Ceramic Scaffolds: An in Vitro Study. J. Adv. Ceram. 2017, 6, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.N.; Hwang, H.-S.; Oh, S.-H.; Roshanzadeh, A.; Kim, J.-W.; Song, J.H.; Kim, E.-S.; Koh, J.-T. Elevated Extracellular Calcium Ions Promote Proliferation and Migration of Mesenchymal Stem Cells via Increasing Osteopontin Expression. Exp. Mol. Med. 2018, 50, 1–16. [Google Scholar] [CrossRef]
- Wang, P.; Qiao, P.; Xing, H.; Zhang, R.; Lingling, E.; Liu, H. Cytotoxicity, Oxidative Stress, and Autophagy Effects of Tantalum Nanoparticles on MC3T3-E1 Mouse Osteoblasts. J. Nanosci. Nanotechnol. 2020, 20, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Zhou, M.; Gu, W.; Shen, Z.; Ma, X.; Lu, F.; Yang, X.; Zheng, Y.; Gou, Z. Zinc-/Copper-Substituted Dicalcium Silicate Cement: Advanced Biomaterials with Enhanced Osteogenesis and Long-Term Antibacterial Properties. J. Mater. Chem. B 2020, 8, 1060–1070. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.; Zhang, W.; Tian, P.; Meng, F.; Zhu, H.; Jiang, X.; Liu, X.; Chu, P.K. Stimulation of Bone Growth Following Zinc Incorporation into Biomaterials. Biomaterials 2014, 35, 6882–6897. [Google Scholar] [CrossRef] [PubMed]
- Arnett, T.R. Extracellular pH regulates bone cell function. J. Nutr. 2008, 138, 415S–418S. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | Bone Defect Depth | Treatment Option |
|---|---|---|
| Minor and contained cancellous bony defects | <5 mm depth | Poly(methyl methacrylate) (PMMA) fill, morselized allograft or autograft |
| Defects in one femoral condyle or one tibial plateau | 5–10 mm depth | Morselized allograft or metal augments |
| 10–20 mm depth | Metal augments, metaphyseal sleeves, structural allografts | |
| Both femoral condyles or tibial plateaus are damaged | <20 mm depth | Metal augments, metaphyseal sleeves, structural allografts, custom-made prostheses, cones |
| Deficient metaphyseal segment; a bone loss that comprises a major portion of the condyle or plateau | >20 mm depth | Structural allografts, custom-made component, cones |
| Advantages | Disadvantages |
|---|---|
| Realistic mechanical loads acting on the limbs [36] | Higher maintenance and handling costs compared to certain animal models (e.g., rabbits) [37] |
| Similar body weight, and metabolism to humans [32,36] | Denser trabecular bone and different microstructure compared to humans (BMD values for human bone: ~180 mg/cm3 vs. BMD value for sheep: ~440 mg/cm3) [32,38] Slower bone turnover compared to human bone |
| Easily available, ethically better accepted than dogs [39] | - |
| Tested successfully as load-bearing bone defect models (femur, tibia, ulna) [37,39,40] | - |
| Suitable for evaluation of potential treatments for osteoporosis [41] | - |
| Comparable tibial blood supply (young sheep) [42] | - |
| Glass Formulations | SiO2 | ZnO | CaO | SrO | P2O5 | Ta2O5 | Cement Formulation [Glass (g):PAA (g):DI Water] |
|---|---|---|---|---|---|---|---|
| Glass A (wt.%) | 23.79 | 32.32 | 4.63 | 16.73 | 8.99 | 13.50 | 10 g:7.5 g:7.5 mL PAA molecular weight: 50 k Glass particle size: 30–45 µm |
| Glass B (wt.%) [48] | 38.75 | 38.81 | 4.52 | 11.14 | 3.81 | 2.97 | 10 g:7.5 g:7.5 mL PAA molecular weight: 50 k Glass particle size: 10–20 µm |
| Glass C (wt.%) [43] | 41.79 | 42.45 | 9.75 | 6.00 | - | - | 3 g:0.9 g:0.9 mL PAA molecular weight: 210 k Glass particle size: 45–63 µm |
| Ion | Toxicity Level (Reported in the Literature) | Effect | Maximum Concentration of Ions in the Present Study (GPCA and GPCB) |
|---|---|---|---|
| Zinc (Zn) | ˃26.1 PPM [73] | Cell death [73] | 25.2 PPM |
| Silicate (Si) | ˃224.6 PPM [74] | Inhibits the nucleation of hydroxyapatite [74] | 32.8 PPM |
| Strontium (Sr) | ˃700.9 PPM [75] | Decreases bone mineralization [75] | 25.2 PPM |
| Phosphorous (P) | ˃41 PPM [76] | Cell death [76] | 23.8 PPM |
| Calcium (Ca) | ˃235 PPM [77] | Decreases matrix mineralization [77] | 13.7 PPM |
| Tantalum (Ta) | ˃25 PPM [78] | Decrease in cell viability [78] | 0.4 PPM |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasandoost, L.; Marx, D.; Zalzal, P.; Safir, O.; Hurtig, M.; Mehrvar, C.; Waldman, S.D.; Papini, M.; Towler, M.R. Comparative Evaluation of Two Glass Polyalkenoate Cements: An In Vivo Pilot Study Using a Sheep Model. J. Funct. Biomater. 2021, 12, 44. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb12030044
Hasandoost L, Marx D, Zalzal P, Safir O, Hurtig M, Mehrvar C, Waldman SD, Papini M, Towler MR. Comparative Evaluation of Two Glass Polyalkenoate Cements: An In Vivo Pilot Study Using a Sheep Model. Journal of Functional Biomaterials. 2021; 12(3):44. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb12030044
Chicago/Turabian StyleHasandoost, Leyla, Daniella Marx, Paul Zalzal, Oleg Safir, Mark Hurtig, Cina Mehrvar, Stephen D. Waldman, Marcello Papini, and Mark R. Towler. 2021. "Comparative Evaluation of Two Glass Polyalkenoate Cements: An In Vivo Pilot Study Using a Sheep Model" Journal of Functional Biomaterials 12, no. 3: 44. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb12030044