Evaluation of Continuous Lactate Monitoring Systems within a Heparinized In Vivo Porcine Model Intravenously and Subcutaneously

 , and
, and
Abstract
:1. Background
2. Materials and Methods
2.1. Sample Fabrication, Preparation, NO Measurements
2.2. Sensor Fabrication and Assembly within Conduit
2.3. Sensor System and Animal Preparation
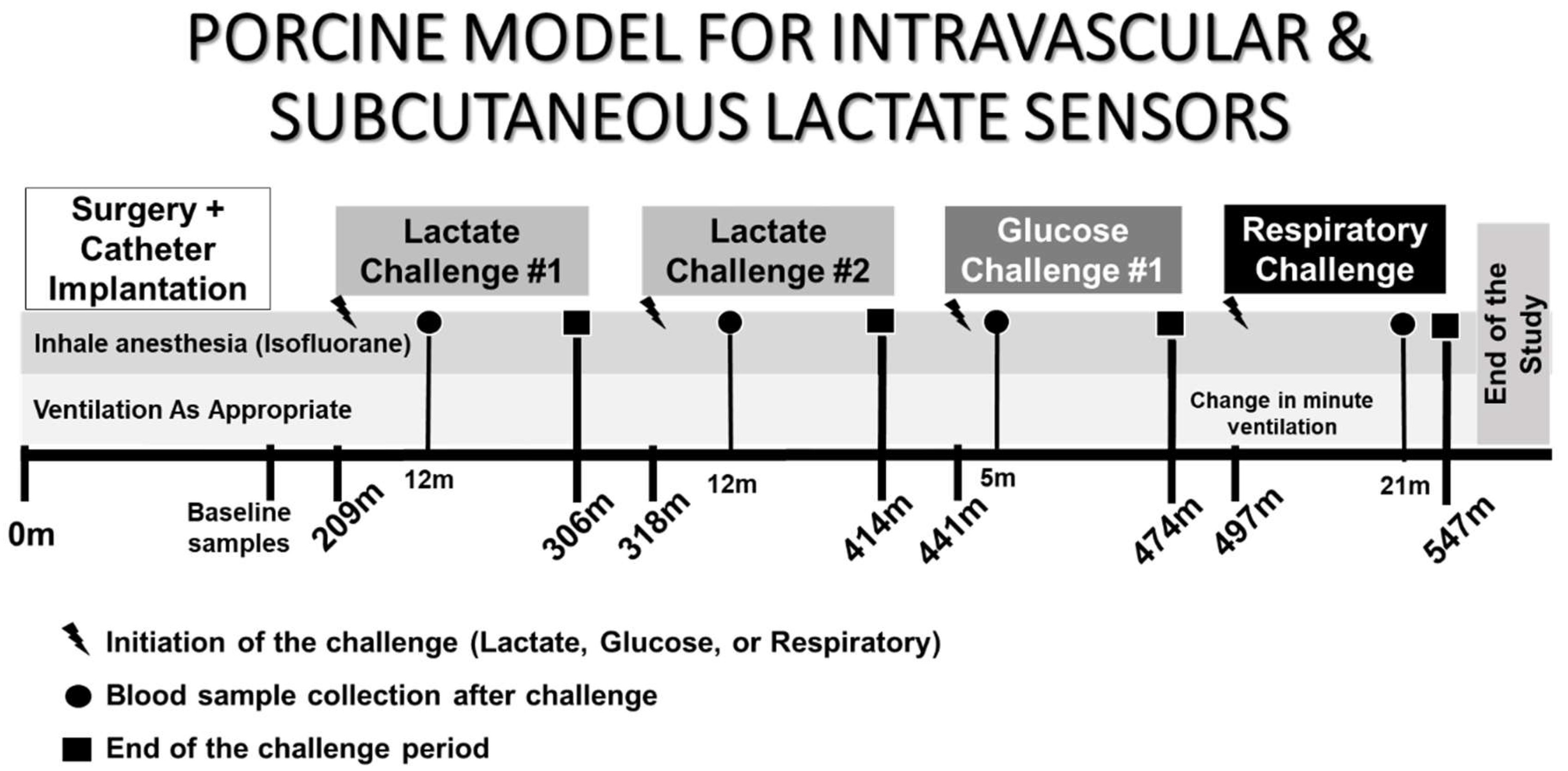
2.4. In Vivo Experimental Interventions for Testing and Assessing Sensor Performance
- Intravenous Lactate Challenge: Sodium L-lactate solution was infused intravenously. Sodium L-lactate (0.18 ± 0.02 moles) was dissolved in 20 mL sterile phosphate buffered saline (PBS), mixed thoroughly, and subsequently placed into an IV infusion bag with accompanying pump for administration a rate of 1500 mL/h over a 15-min infusion time.
- Intravenous Glucose Challenge: 36 g, 18.0 mL bolus of 50% dextrose solution was given IV to the animal over 3 min.
- Respiratory Challenge: Physiological lactic acidosis secondary to hypoxia and hypercapnia was induced by decreasing minute ventilation [44]. Hypercapnia/hypoxia was induced by first drawing blood from the animal and then infusing the blood back to the animal while decreasing 70–75% minute ventilation from baseline. Lower regions and tissues of the animal are distal from the heart and are responsible for circulation of blood and all corresponding analytes leading to lower perfusion efficiency compared to tissues proximal to the heart, accentuated during times of stress such as an induced respiratory challenge. It’s expected to see a signal response of greater magnitude and faster response time from the intravenous and subcutaneous sensors placed in the neck (proximal) than those sensor systems placed in the groin (distal).
3. Results
3.1. In Vivo Monitoring with Blood Lactate Modulation
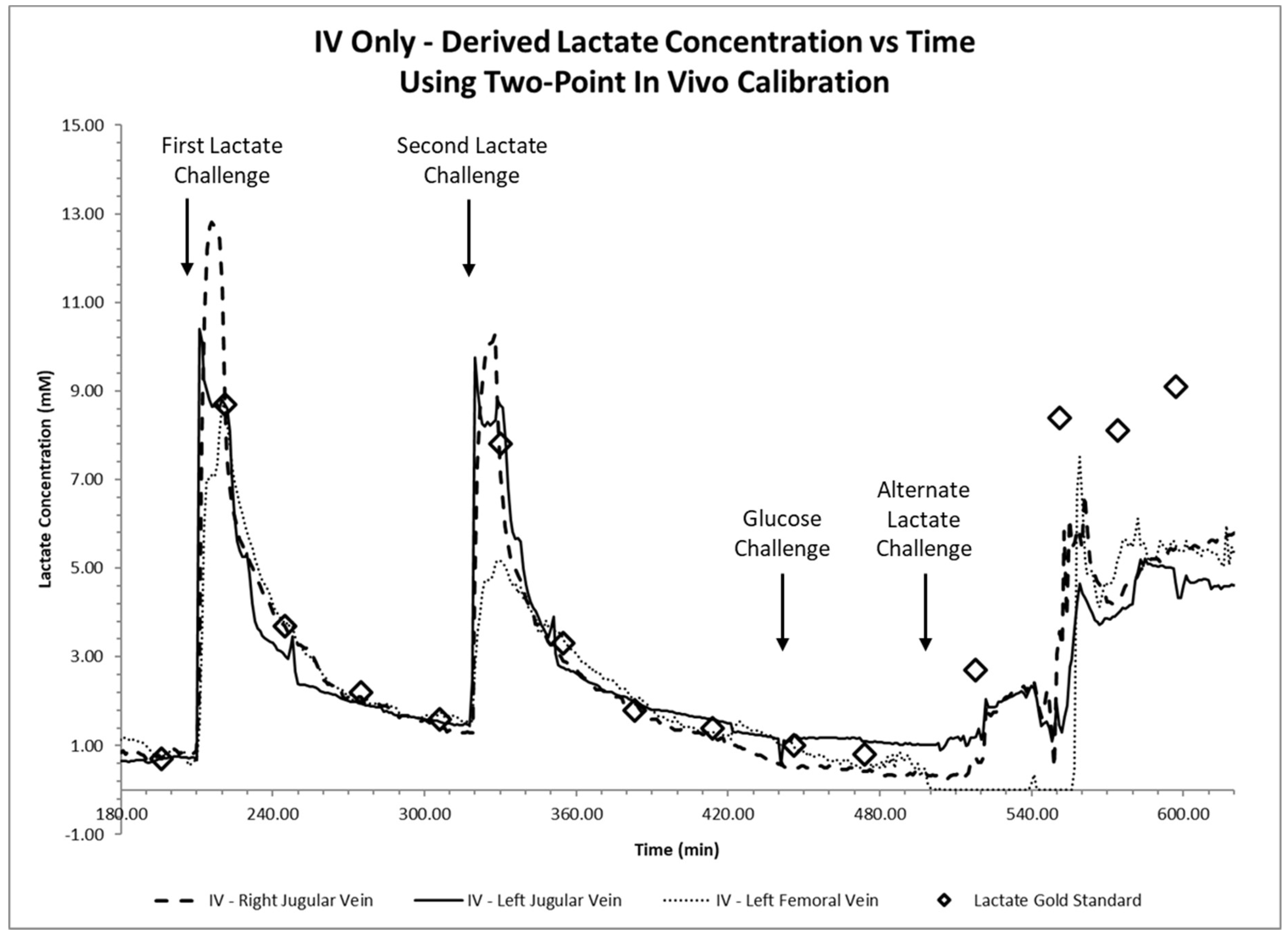
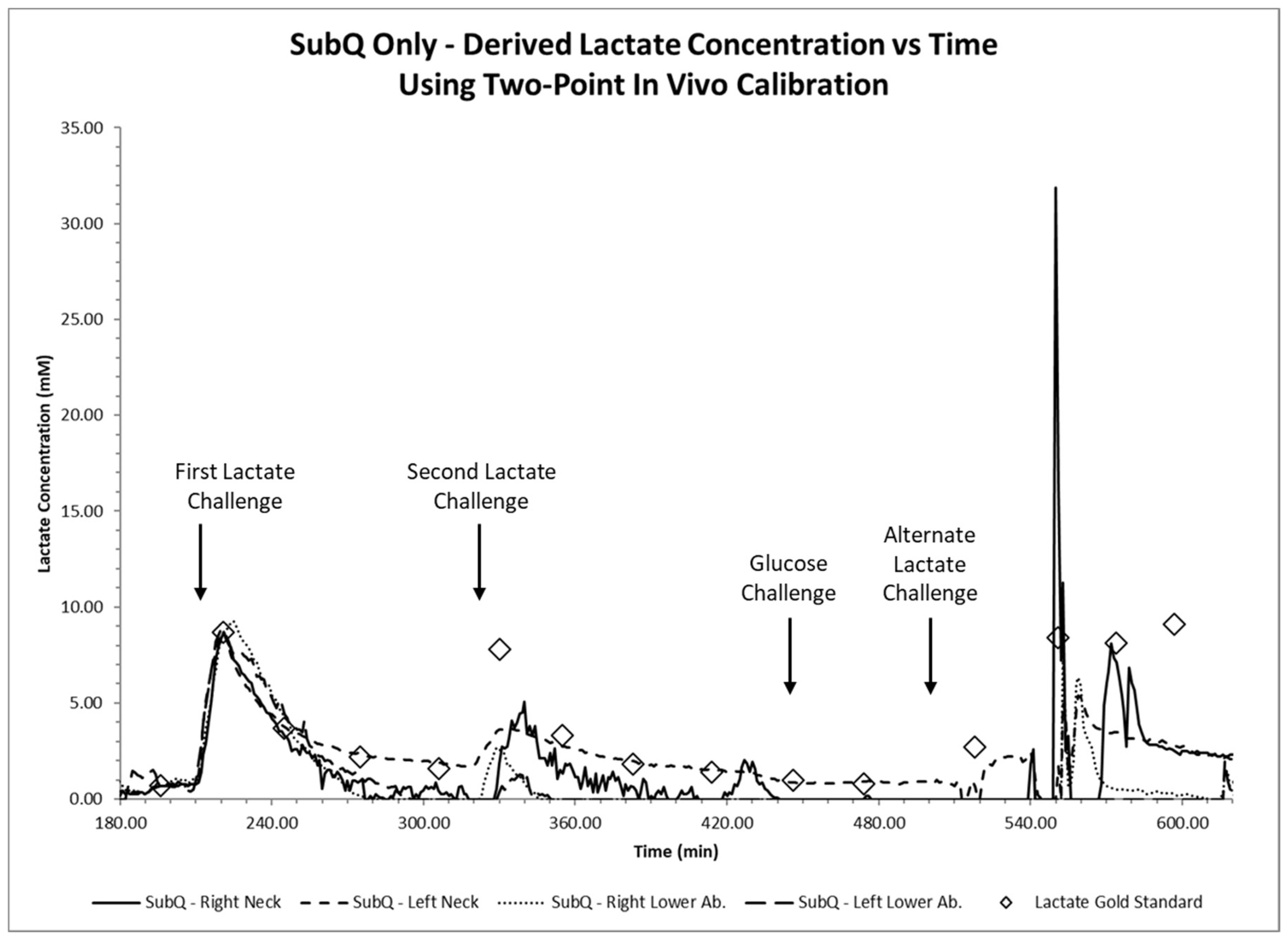
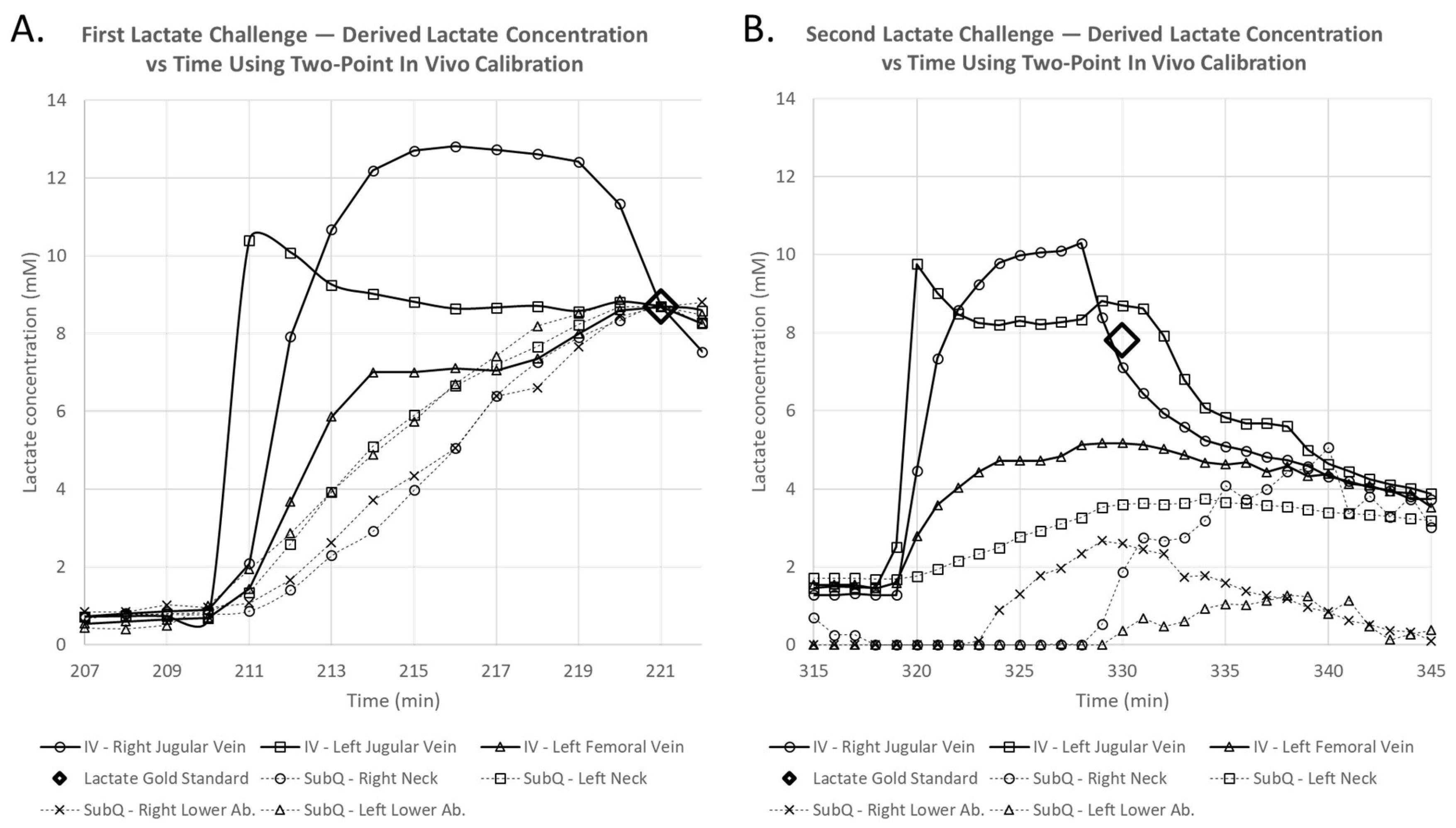
3.2. Intravenous and Subcutaneous Sensing Results
4. Discussion
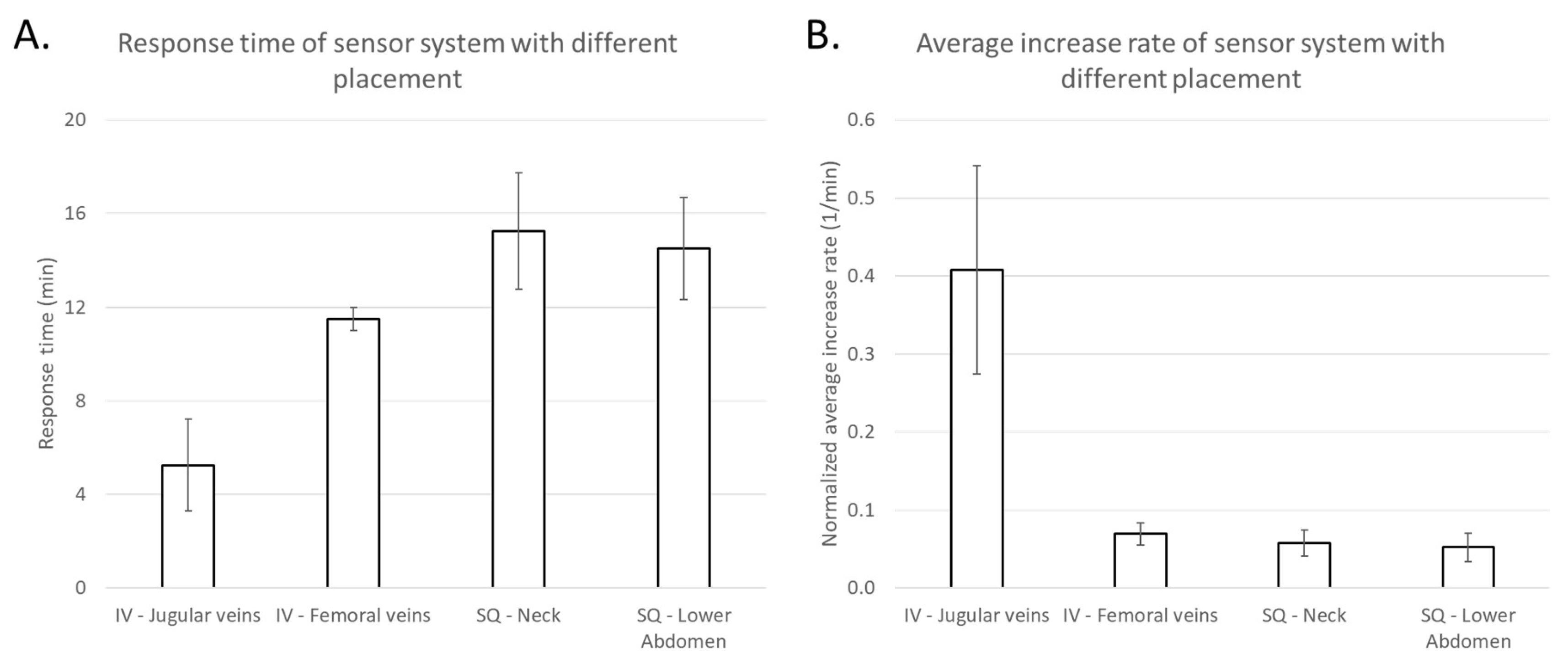
4.1. Intravenous and Subcutaneous Sensors: Response Times and Increase-Rates
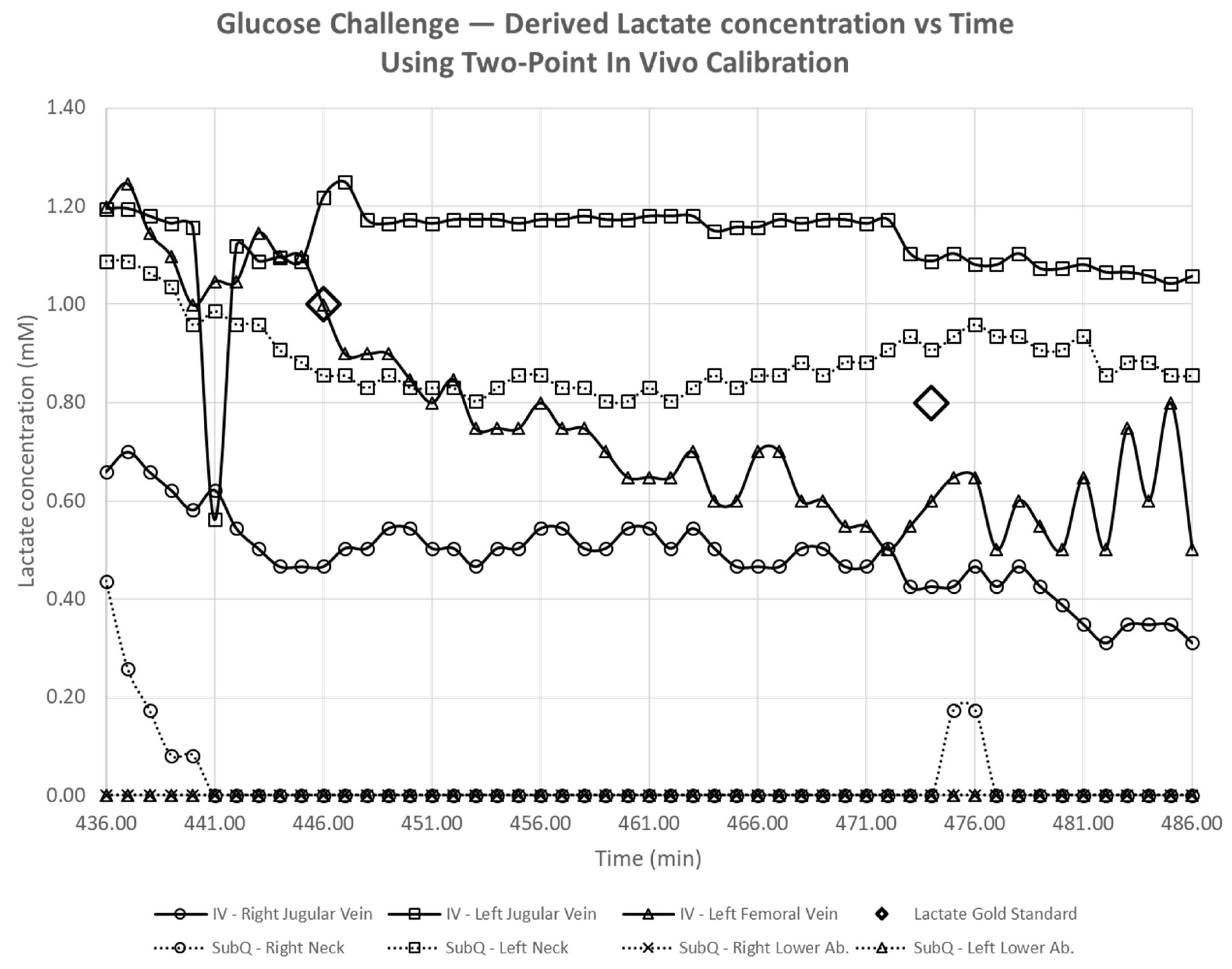
4.2. Intravenous and Subcutaneous Lactate Sensors: No Interference to Variations in Glucose
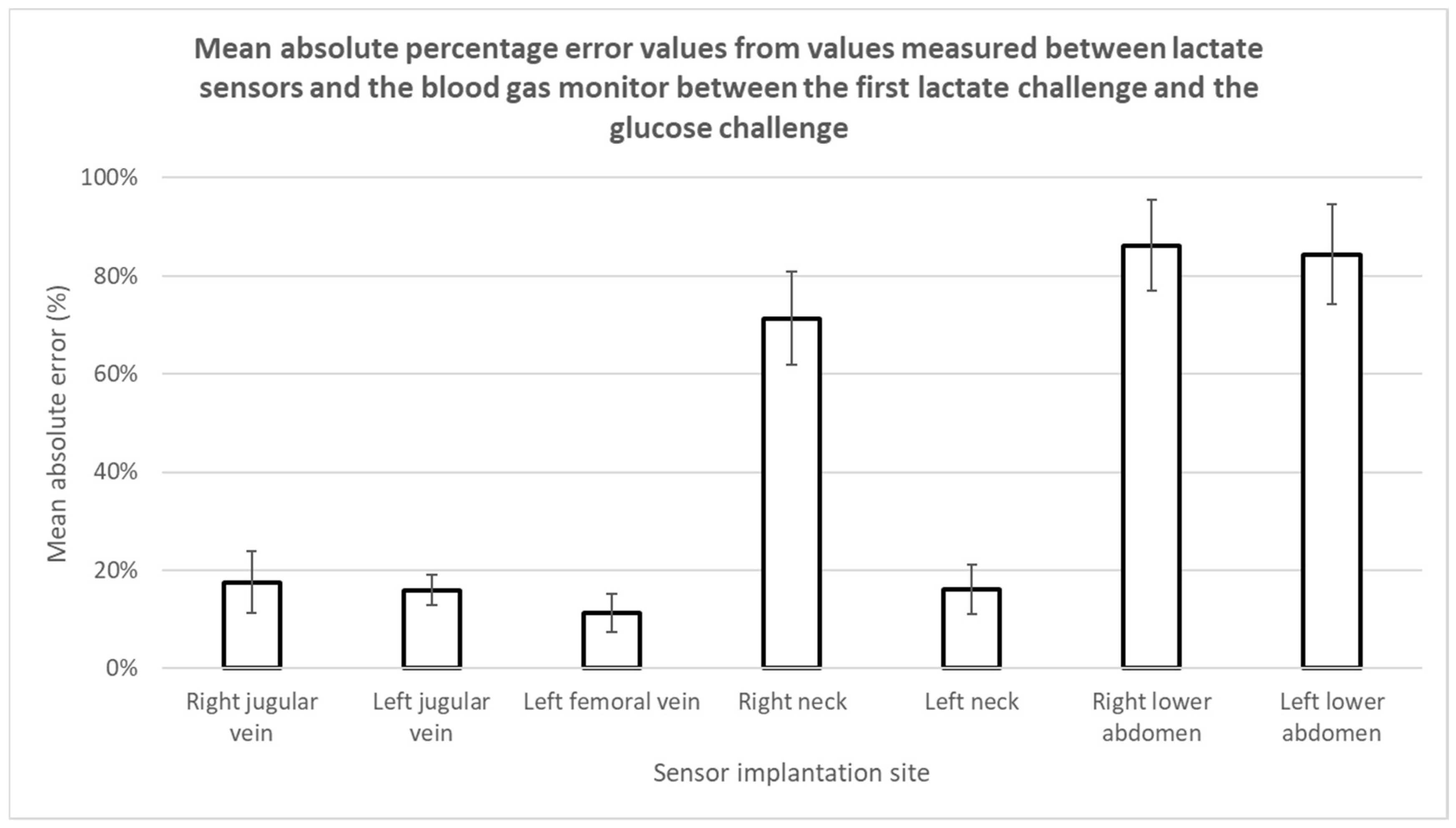
4.3. Intravenous and Subcutaneous Lactate Sensors: Accuracy and Performance
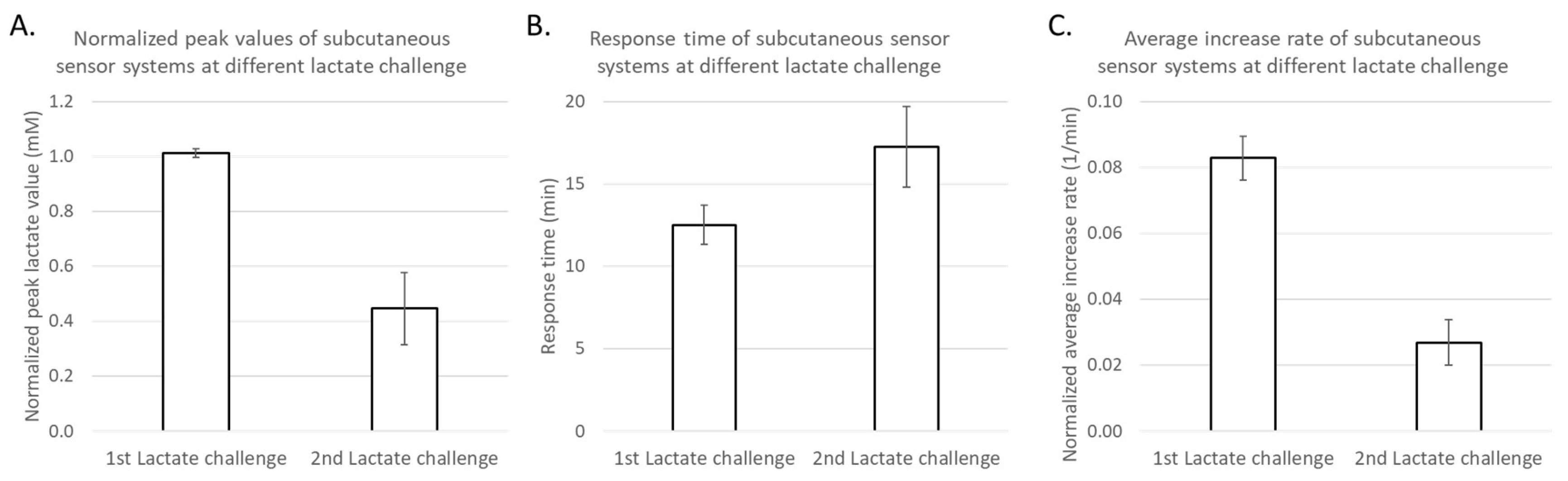
4.4. Subcutaneous Lactate Sensing Results Compared to Blood Lactate via Blood Gas
4.5. Sensor Biocompatibility
4.6. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schumacher, K.R.; Reichel, R.A.; Vlasic, J.R.; Yu, S.; Donohue, J.; Gajarski, R.J.; Charpie, J.R. Rate of increase in serum lactate level risk-stratifies infants after surgery for congenital heart disease. J. Thorac. Cardiovasc. Surg. 2014, 148, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Charpie, J.R.; Dekeon, M.K.; Goldberg, C.S.; Mosca, R.S.; Bove, E.L.; Kulik, T.J. Serial blood lactate measurements predict early outcome after neonatal repair or palliation for complex congenital heart disease. J. Thorac. Cardiovasc. Surg. 2000, 120, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J. The global burden of congenital heart disease. Cardiovasc. J. Afr. 2013, 24, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Jansen, T.C.; van Bommel, J.; Schoonderbeek, F.J.; Sleeswijk Visser, S.J.; van der Klooster, J.M.; Lima, A.P.; Willemsen, S.P.; Bakker, J. Early lactate-guided therapy in intensive care unit patients: A multicenter, open-label, randomized controlled trial. Am. J. Respir. Crit. Care Med. 2010, 182, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Khosravani, H.; Shahpori, R.; Stelfox, H.T.; Kirkpatrick, A.W.; Laupland, K.B. Occurrence and adverse effect on outcome of hyperlactatemia in the critically ill. Crit. Care 2009, 13, R90. [Google Scholar] [CrossRef] [PubMed]
- Vorwerk, C.; Loryman, B.; Coats, T.J.; Stephenson, J.A.; Gray, L.D.; Reddy, G.; Florence, L.; Butler, N. Prediction of mortality in adult emergency department patients with sepsis. Emerg. Med. J. 2009, 26, 254–258. [Google Scholar] [CrossRef]
- van Beest, P.; Kuiper, M.; Spronk, P.E. Lactate: An unusually sensitive parameter of ensuing organ failure? Crit. Care Med. 2010, 38, 337. [Google Scholar] [CrossRef]
- Manikis, P.; Jankowski, S.; Zhang, H.; Kahn, R.J.; Vincent, J.L. Correlation of serial blood lactate levels to organ failure and mortality after trauma. Am. J. Emerg. Med. 1995, 13, 619–622. [Google Scholar] [CrossRef]
- Roumen, R.M.; Redl, H.; Schlag, G.; Sandtner, W.; Koller, W.; AGoris, R.J. Scoring systems and blood lactate concentrations in relation to the development of adult respiratory distress syndrome and multiple organ failure in severely traumatized patients. J. Traumatol. Acute Care Surg. 1993, 35, 349–355. [Google Scholar] [CrossRef]
- Rishu, A.H.; Khan, R.; Al-Dorzi, H.M.; Tamim, H.M.; Al-Qahtani, S.; Al-Ghamdi, G.; Arabi Yaseen, M. Even mild hyperlactatemia is associated with increased mortality in critically ill patients. Crit. Care. 2013, 17, R197. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013, 39, 165–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivers, E.; Nguyen, B.; Havstad, S.; Ressler, J.; Muzzin, A.; Knoblich, B.; Peterson, E.; Tomlanovich, M. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N. Engl. J. Med. 2001, 345, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Rusconi, A.M.; Bossi, I.; Lampard, J.G.; Szava-Kovats, M.; Bellone, A.; Lang, E. Early goal-directed therapy vs usual care in the treatment of severe sepsis and septic shock: A systematic review and meta-analysis. Int. Emerg. Med. 2015, 10, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.E.; Shapiro, N.I.; Trzeciak, S.; Arnold, R.C.; Claremont, H.A.; Kline, J.A.; Emergency Medicine Shock Research Network (EMShockNet) Investigators. Lactate clearance vs. central venous oxygen saturation as goals of early sepsis therapy: A randomized clinical trial. JAMA 2010, 303, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Frost MCW, M.C.; Wolf, A.K.; Meyerhoff, M.E. In Vivo Sensors for Continuous Monitoring of Blood Gases, Glucose and Lactate: Biocompatibility Challenges and Potential Solutions. In Detection Challenges in Clinical Diagnosis; Vadgama, P., Peteu, S., Eds.; RSC Publishing: Cambridge, UK, 2013. [Google Scholar]
- Gifford, R. Continuous glucose monitoring: 40 years, what we’ve learned and what’s next. Chemphyschem 2013, 14, 2032–2044. [Google Scholar] [CrossRef] [PubMed]
- Frost, M.C.; Meyerhoff, M.E. Indwelling Chemical Sensors for Real-Time Clinical Monitoring: Progress and Challenges. Curr. Opin. Chem. Biol. 2002, 6, 633–641. [Google Scholar] [CrossRef]
- Frost, M.; Meyerhoff, M.E. In vivo chemical sensors: Tackling biocompatibility. Anal. Chem. 2006, 78, 7370–7377. [Google Scholar] [CrossRef]
- Ganter, M.; Zollinger, A. Continuous intravascular blood gas monitoring: Development, current techniques, and clinical use of a commercial device. Br. J. Anaesth. 2003, 91, 397–407. [Google Scholar] [CrossRef]
- Coule, L.W.; Truemper, E.J.; Steinhart, C.M.; Lutin, W.A. Accuracy and utility of a continuous intra-arterial blood gas monitoring system in pediatric patients. Crit. Care Med. 2001, 29, 420–426. [Google Scholar] [CrossRef]
- Shapiro, B.A. In-Vivo Monitoring of Arterial Blood Gases and pH. Respir. Care 1992, 37, 165–169. [Google Scholar]
- Wahr, J.A.; Tremper, K.K. Continuous intravascular blood gas monitoring. J. Cardiothoracic. Vasc. Anesth. 1994, 8, 342–353. [Google Scholar] [CrossRef]
- Meyerhoff, M.E. In Vivo Blood-Gas and Electrolyte Sensors: Progress and Challenges. Anal. Chem. 1993, 12, 257–266. [Google Scholar] [CrossRef]
- Mahutte, C.K.; Sassoon, C.S.; Muro, J.R.; Hansmann, D.R.; Maxwell, T.P.; Miller, W.W.; Yafuso, M. Progress in the development of a fluorescent intravascular blood gas system in man. J. Clin. Monit. 1990, 6, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Rathee, K.; Dhull, V.; Dhull, R.; Singh, S. Biosensors based on electrochemical lactate detection: A comprehensive review. Biochem. Biophys. Rep. 2016, 5, 35–54. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Major, T.C.; Bartlett, R.H.; Meyerhoff, M.E. Intravascular glucose/lactate sensors prepared with nitric oxide releasing poly(lactide-co-glycolide)-based coatings for enhanced biocompatibility. Biosens. Bioelectron. 2011, 26, 4276–4282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, K.W.; Qin, Y.; Major, T.C.; Meyerhoff, M.E. Improved thromboresistance and analytical performance of intravascular amperometric glucose sensors using optimized nitric oxide release coatings. Chin. Chem. Lett. 2015, 26, 464–468. [Google Scholar]
- Nathan, C.F.; Hibbs, J.B., Jr. Role of nitric oxide synthesis in macrophage antimicrobial activity. Curr. Opin. Immunol. 1991, 3, 65–70. [Google Scholar] [CrossRef]
- Mannick, J.B. Immunoregulatory and antimicrobial effects of nitrogen oxides. Proc. Am. Thorac. Soc. 2006, 3, 161–165. [Google Scholar] [CrossRef]
- Frost, M.C.; Rudich, S.M.; Zhang, H.; Maraschio, M.A.; Meyerhoff, M.E. In vivo biocompatibility and analytical performance of intravascular amperometric oxygen sensors prepared with improved nitric oxide-releasing silicone rubber coating. Anal. Chem. 2002, 74, 5942–5947. [Google Scholar] [CrossRef]
- Frost, M.C.; Reynolds, M.M.; Meyerhoff, M.E. Polymers incorporating nitric oxide releasing/generating substances for improved biocompatibility of blood-contacting medical devices. Biomaterials 2005, 26, 1685–1693. [Google Scholar] [CrossRef]
- Reynolds, M.M.; Frost, M.C.; Meyerhoff, M.E. Nitric oxide-releasing hydrophobic polymers: Preparation, characterization, and potential biomedical applications. Free Radic. Biol. Med. 2004, 37, 926–936. [Google Scholar] [CrossRef] [PubMed]
- Annich, G.M.; Meinhardt, J.P.; Mowery, K.A.; Ashton, B.A.; Merz, S.I.; Hirschl, R.B.; Meyerhoff Mark, E.; Bartlett Robert, H. Reduced platelet activation and thrombosis in extracorporeal circuits coated with nitric oxide release polymers. Crit. Care Med. 2000, 28, 915–920. [Google Scholar] [CrossRef]
- Fleser, P.S.; Nuthakki, V.K.; Malinzak, L.E.; Callahan, R.E.; Seymour, M.L.; Reynolds, M.M.; Meyerhoff Mark, E.; Bartlett Robert, H. Nitric oxide-releasing biopolymers inhibit thrombus formation in a sheep model of arteriovenous bridge grafts. J. Vasc. Surg. 2004, 40, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Radomski, M.W.; Palmer, R.M.; Moncada, S. Endogenous nitric oxide inhibits human platelet adhesion to vascular endothelium. Lancet 1987, 2, 1057–1058. [Google Scholar] [CrossRef]
- Radomski, M.W.; Palmer, R.M.; Moncada, S. The role of nitric oxide and cGMP in platelet adhesion to vascular endothelium. Biochem. Biophys Res. Commun. 1987, 148, 1482–1489. [Google Scholar] [CrossRef]
- Yan, Q.Y.; Peng, B.; Su, G.; Cohan, B.E.; Major, T.C.; Meyerhoff, M.E. Measurement of Tear Glucose Levels with Amperometric Glucose Biosensor/Capillary Tube Configuration. Anal. Chem. 2011, 83, 8341–8346. [Google Scholar] [CrossRef] [PubMed]
- Bindra, D.S.; Zhang, Y.N.; Wilson, G.S.; Sternberg, R.; Thevenot, D.R.; Moatti, D.; Reach, G. Design and Invitro Studies of a Needle-Type Glucose Sensor for Subcutaneous Monitoring. Anal. Chem. 1991, 63, 1692–1696. [Google Scholar] [CrossRef] [Green Version]
- Carelli, I.; Chiarotto, I.; Curulli, A.; Palleschi, G. Electropolymerization of hydroxybenzene and aminobenzene isomers on platinum electrodes to assemble interference-free electrochemical biosensors. Electrochim. Acta 1996, 41, 1793–1800. [Google Scholar] [CrossRef]
- Geise, R.J.; Adams, J.M.; Barone, N.J.; Yacynych, A.M. Electropolymerized Films to Prevent Interferences and Electrode Fouling in Biosensors. Biosen. Bioelectron. 1991, 6, 151–160. [Google Scholar] [CrossRef]
- Brisbois, E.J.; Handa, H.; Major, T.C.; Bartlett, R.H.; Meyerhoff, M.E. Long-term nitric oxide release and elevated temperature stability with S-nitroso-N-acetylpenicillamine (SNAP)-doped Elast-eon E2As polymer. Biomaterials 2013, 34, 6957–6966. [Google Scholar] [CrossRef]
- Guide for the Care and Use of Laboratory Animals, 8th ed.; National Academies Press: Washington, DC, USA, 2011.
- Wu, Y.; Rojas, A.P.; Griffith, G.W.; Skrzypchak, A.M.; Lafayette, N.; Bartlett, R.H.; Meyerhoff, M.E. Improving Blood Compatibility of Intravascular Oxygen Sensors Via Catalytic Decomposition of S-Nitrosothiols to Generate Nitric Oxide In Situ. Sens. Actuators B Chem. 2007, 121, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Witer, L.J.; Howard, R.A.; Trahanas, J.M.; Bryner, B.S.; Alghanem, F.; Hoffman, H.R.; Meyerhoff, M.E. Large Animal Model of Pumpless Arteriovenous Extracorporeal CO(2) Removal Using Room Air via Subclavian Vessels. ASAIO J. 2016, 62, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Clarke, W.L.; Cox, D.; Gonder-Frederick, L.A.; Carter, W.; Pohl, S.L. Evaluating Clinical Accuracy of Systems for Self-Monitoring of Blood Glucose. Diabetes Care 1987, 10, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Boyne, M.S.; Silver, D.M.; Kaplan, J.; Saudek, C.D. Timing of Changes in Interstitial and Venous Blood Glucose Measured With a Continuous Subcutaneous Glucose Sensor. Diabetes 2003, 52, 2790–2794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cengiz, E.; Tamborlane, W.V. A Tale of Two Compartments: Interstitial Versus Blood Glucose Monitoring. Diabetes Technol. Ther. 2009, 11 (Suppl. 1), S11-6. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Dube, S.; Slama, M.; Errazuriz, I.; Amezcua, J.C.; Kudva, Y.C.; Peyser, T.; Carter, R.E.; Cobelli, C.; Basu, R. Time Lag of Glucose From Intravascular to Interstitial Compartment in Humans. Diabetes 2013, 62, 4083–4087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, A.; Dube, S.; Veettil, S.; Slama, M.; Kudva, Y.C.; Peyser, T.; Carter, R.E.; Cobelli, C.; Basu, R. Time Lag of Glucose From Intravascular to Interstitial Compartment in Type 1 Diabetes. J. Diabetes Sci. Technol. 2015, 9, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Gelman, S. General anesthesia and hepatic circulation. Can. J. Physiol. Pharmacol. 1987, 65, 1762–1779. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | IV1 | IV2 | IV3 | SQ1 | SQ2 | SQ3 | SQ4 |
|---|---|---|---|---|---|---|---|
| Placement Location | Right Jugular vein | Left Jugular vein | Left Femoral Vein | Right Neck | Left Neck | Right Lower Abdomen | Left Lower Abdomen |
| Tissue Environment | IV | IV | IV | SQ | SQ | SQ | SQ |
| In Vivo Performance | Close to Gold Standard | Close to Gold Standard | Close to Gold Standard, but reduced peak intensity | Significant deviation after 1st lactate challenge | Closest subcutaneous to Gold Standard, reduced peak intensity | Significant deviation after 1st lactate challenge | Significant deviation after 1st lactate challenge |
| Clotting Observed | NEGATIVE | NEGATIVE | NEGATIVE | NEGATIVE | NEGATIVE | NEGATIVE | NEGATIVE |
| Lactate Concentration (mmol/L) | Glucose Concentration (mg/dL) | ||||||
|---|---|---|---|---|---|---|---|
| Lactate Challenge # | Initial | Post-infusion | 25 min Post-infusion | 60 min Post-infusion | Initial | 25 min Post-infusion | 60 min Post-infusion |
| 1 | 0.7 | 8.9 | 3.7 | 2.2 | 102 | 114 | 130 |
| 2 | 1.6 | 7.8 | 3.3 | 1.8 | 136 | 131 | 134 |
| Glucose Concentration (mg/dL) | Lactate Concentration (mmol/L) | ||||||
| Glucose Challenge # | Initial | 5 min Post-infusion | 30 min Post-infusion | Initial | 5 min Post-infusion | 30 min Post-infusion | |
| 1 | 156 | 218 | 175 | 1.4 | 1.0 | 0.8 | |
| PaCO2 (mmHg) | PaO2 (mmHg) | pH | SO2 % | Lactate (mmol/L) | Glucose (g/dL) | |
|---|---|---|---|---|---|---|
| Initial | 40.9 | 252 | 7.509 | 99.9 | 0.8 | 175 |
| 45 min Post-challenge | 70.2 | 29.4 | 7.339 | 37.7 | 2.7 | 176 |
| IV—Right Jugular Vein | IV—Left Jugular Vein | IV—Left Femoral Vein | SQ—Right Neck | SQ—Left Neck | SQ—Right Lower Abdomen | SQ—Left Lower Abdomen | |
|---|---|---|---|---|---|---|---|
| Time from 1st lactate infusion to peak (min) | 7 | 2 | 12 | 12 | 11 | 16 | 11 |
| Normalized average increase rate (1/min) | 0.213 | 0.605 | 0.084 | 0.082 | 0.090 | 0.064 | 0.095 |
| Time from 2nd lactate infusion to peak (min) | 10 | 2 | 11 | 22 | 16 | 11 | 20 |
| Normalized average increase rate (1/min) | 0.145 | 0.669 | 0.055 | 0.037 | 0.021 | 0.039 | 0.010 |
| IV—Right Jugular Vein | IV—Left Jugular Vein | IV—Left Femoral Vein | SQ—Right Neck | SQ—Left Neck | SQ—Right Lower Abdomen | SQ—Left Lower Abdomen | |
|---|---|---|---|---|---|---|---|
| Kendall’s tau | −0.674 | −0.427 | −0.745 | −0.281 | −0.0436 | N/A | N/A |
| Two-sided p-value | 5.60 × 10−11 | 2.50 × 10−5 | 7.60 × 10−14 | 0.0141 | 0.6744 | N/A | N/A |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolf, A.; Renehan, K.; Ho, K.K.Y.; Carr, B.D.; Chen, C.V.; Cornell, M.S.; Ye, M.; Rojas-Peña, A.; Chen, H. Evaluation of Continuous Lactate Monitoring Systems within a Heparinized In Vivo Porcine Model Intravenously and Subcutaneously. Biosensors 2018, 8, 122. https://0-doi-org.brum.beds.ac.uk/10.3390/bios8040122
Wolf A, Renehan K, Ho KKY, Carr BD, Chen CV, Cornell MS, Ye M, Rojas-Peña A, Chen H. Evaluation of Continuous Lactate Monitoring Systems within a Heparinized In Vivo Porcine Model Intravenously and Subcutaneously. Biosensors. 2018; 8(4):122. https://0-doi-org.brum.beds.ac.uk/10.3390/bios8040122
Chicago/Turabian StyleWolf, Alexander, Kevin Renehan, Kenneth K. Y. Ho, Benjamin D. Carr, Chieh V. Chen, Marie S. Cornell, Minyi Ye, Alvaro Rojas-Peña, and Hao Chen. 2018. "Evaluation of Continuous Lactate Monitoring Systems within a Heparinized In Vivo Porcine Model Intravenously and Subcutaneously" Biosensors 8, no. 4: 122. https://0-doi-org.brum.beds.ac.uk/10.3390/bios8040122