Effects of a Paediatric Antimicrobial Stewardship Program on Antimicrobial Use and Quality of Prescriptions in Patients with Appendix-Related Intraabdominal Infections

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Days of Therapy (DOTs), Length of Therapy (LOT), and Length of Stay (LOS)
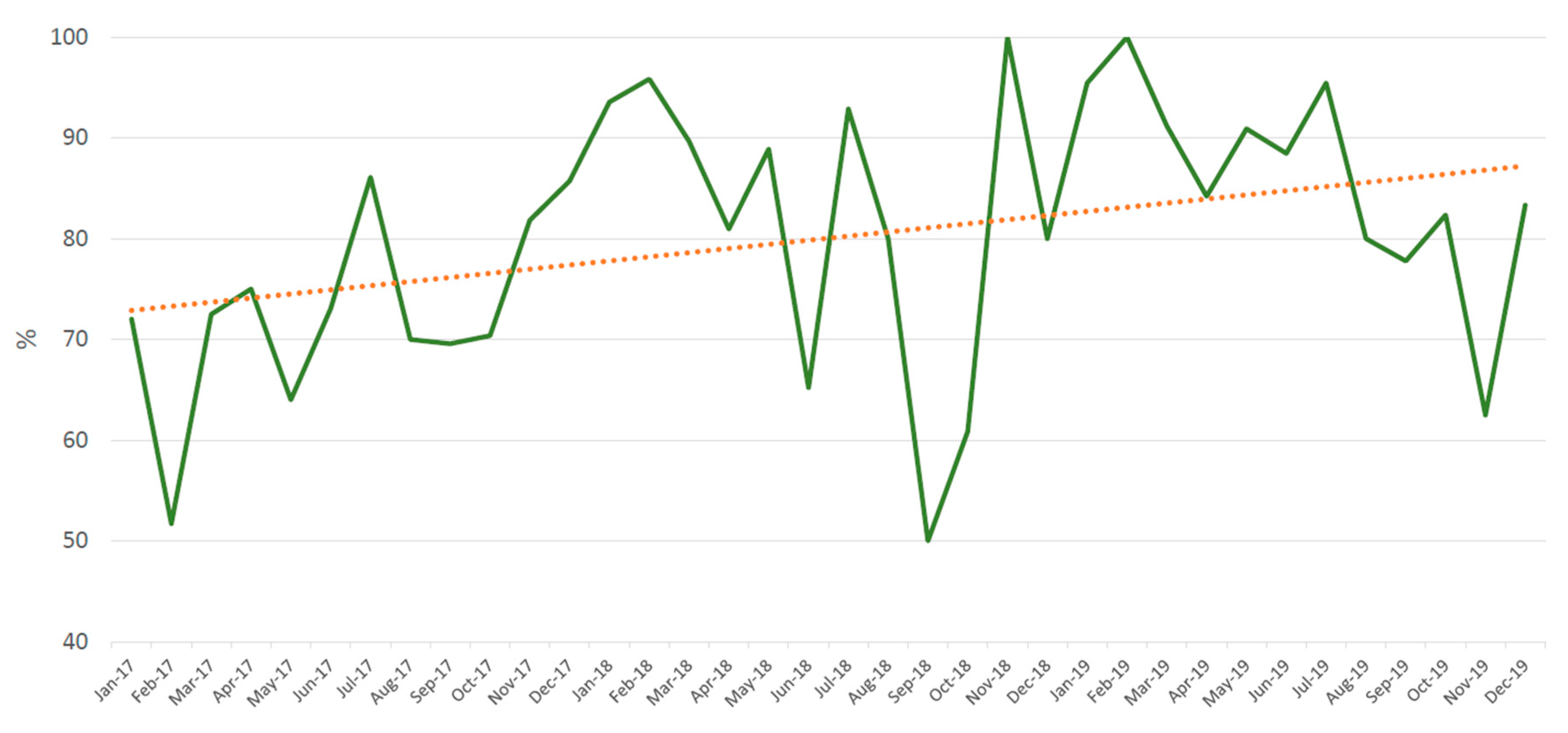
2.2. Quality of Prescriptions
2.3. Other Outcomes
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Setting and Patients
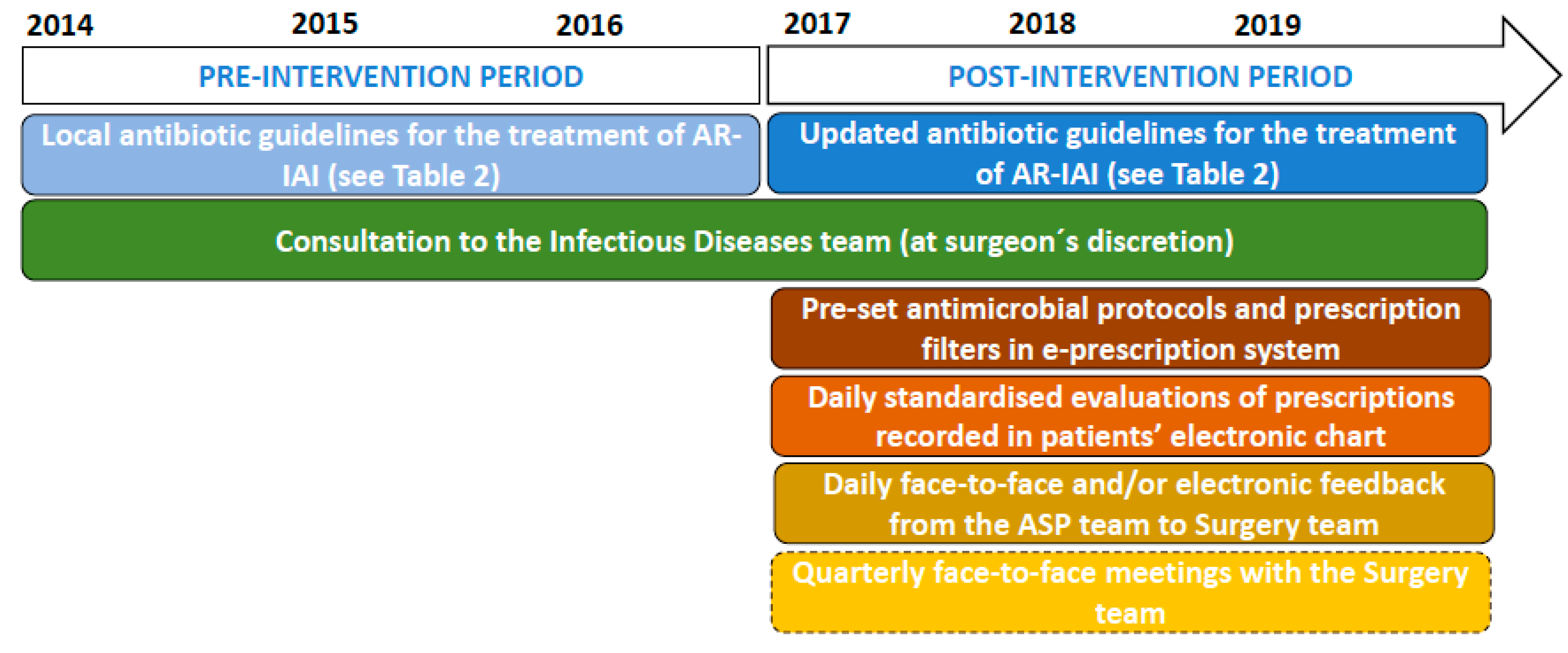
4.3. Intervention: PROA-SJD
4.4. Definitions
4.4.1. Days of Therapy (DOTs), Length of Therapy (LOT), and Length of Stay (LOS)
4.4.2. Quality of Prescriptions
4.4.3. Other Outcomes
4.5. Statistical Methods
4.6. Ethics Statements
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith, M.J.; Gerber, J.S.; Hersh, A.L. Inpatient antimicrobial stewardship in pediatrics: A systematic review. J. Pediatric Infect. Dis. Soc. 2015, 4, e127–e135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hersh, A.L.; De Lurgio, S.A.; Thurm, C.; Lee, B.R.; Weissman, S.J. Antimicrobial stewardship programs in freestanding children’s hospitals. Pediatrics 2015, 135, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; Macdougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Dociety of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, 51–77. [Google Scholar] [CrossRef] [PubMed]
- Di Pentima, M.C.; Chan, S.; Hossain, J. Benefits of a pediatric antimicrobial stewardship program at a children’s hospital. Pediatrics 2011, 128, 1062–1070. [Google Scholar] [CrossRef] [PubMed]
- Newland, J.G.; Hersh, A.L. Purpose and design of antimicrobial stewardship programs in pediatrics. Pediatric Infect. Dis. J. 2010, 29, 862–863. [Google Scholar] [CrossRef] [Green Version]
- Kronman, M.P.; Banerjee, R.; Duchon, J.; Gerber, J.S.; Green, M.D.; Hersh, A.L.; Hyun, D.; Maples, H.; Nash, C.B.; Parker, S.; et al. Expanding existing antimicrobial stewardship programs in pediatrics: What comes next. J. Pediatric Infect. Dis. Soc. 2017, 7, 241–248. [Google Scholar] [CrossRef]
- Velasco, E.; Simó, S.; Ríos-Barnés, M.; López, M.G.; Monsonís, M.; Urrea, M.; Jordan, I.; Mas, A.; Casadevall, R.; Ormazábal, D.; et al. Benefits of a pediatric antimicrobial stewardship program in antimicrobial use and quality of prescriptions in a referral children’s hospital. J. Pediatr. 2020, 225, 222–230. [Google Scholar] [CrossRef]
- Brett, A.; Bielicki, J.; Newland, J.G.; Rodrigues, F.; Schaad, U.B.; Sharland, M. Neonatal and pediatric antimicrobial stewardship programs in Europe-defining the research agenda. Pediatr. Infect. Dis. J. 2013, 32, e456–e465. [Google Scholar] [CrossRef]
- Donà, D.; Barbieri, E.; Daverio, M.; Lundin, R.; Giaquinto, C.; Zaoutis, T.; Sharland, M. Implementation and impact of pediatric antimicrobial stewardship programs: A systematic scoping review. Antimicrob. Resist. Infect. Control. 2020, 9, 3. [Google Scholar] [CrossRef]
- Willis, Z.I.; Duggan, E.M.; Gillon, J.; Blakely, M.L.; Di Pentima, M.C. Improvements in antimicrobial prescribing and outcomes in pediatric complicated appendicitis. Pediatr. Infect. Dis. J. 2018, 37, 429–435. [Google Scholar] [CrossRef]
- Sartelli, M.; Duane, T.M.; Catena, F.; Tessier, J.M.; Coccolini, F.; Kao, L.S.; De Simone, B.; Labricciosa, F.M.; May, A.K.; Ansaloni, L.; et al. Antimicrobial stewardship: A call to action for surgeons. Surg. Infect. 2016, 17, 625–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Della Polla, G.; Bianco, A.; Mazzea, S.; Napolitano, F.; Angelillo, I.F. Preoperative antibiotic prophylaxis in elective minor surgical procedures among adults in southern Italy. Antibiotics 2020, 9, 713. [Google Scholar] [CrossRef] [PubMed]
- Güerri-Fernández, R.; Villar-García, J.; Herrera-Fernández, S.; Trenchs-Rodríguez, M.; Fernández-Morato, J.; Moro, L.; Sancho, J.; Grande, L.; Clará, A.; Grau, S.; et al. An antimicrobial stewardship program reduces antimicrobial therapy duration and hospital stay in surgical wards. Rev. Esp. Quimioter. 2016, 29, 119–121. [Google Scholar] [PubMed]
- Foolad, F.; Nagel, J.L.; Eschenauer, G.; Patel, T.S.; Nguyen, C.T. Disease-based antimicrobial stewardship: A review of active and passive approaches to patient management. J. Antimicrob. Chemother. 2017, 72, 3232–3244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saar, S.; Mihnovitš, V.; Lustenberger, T.; Rauk, M.; Noor, E.-H.; Lipping, E.; Isand, K.-G.; Lepp, J.; Lomp, A.; Lepner, U.; et al. Twenty-four hour versus extended antibiotic administration after surgery in complicated appendicitis: A randomized controlled trial. J. Trauma Acute Care Surg. 2019, 86, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Solomkin, J.S.; Mazuski, J.E.; Bradley, J.S.; Rodvold, K.A.; Goldstein, E.J.C.; Baron, E.J.; O’Neill, P.J.; Chow, A.W.; Dellinger, E.P.; Eachempati, S.R.; et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 133–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawyer, R.G.; Claridge, J.A.; Nathens, A.B.; Rotstein, O.D.; Duane, T.M.; Evans, H.L.; Cook, C.H.; O’Neill, P.J.; Mazuski, J.E.; Askari, R.; et al. Trial of short-course antimicrobial therapy for intraabdominal infection. N. Engl. J. Med. 2015, 372, 1996–2005. [Google Scholar] [CrossRef] [Green Version]
- Rattan, R.; Allen, C.J.; Sawyer, R.G.; Askari, R.; Banton, K.L.; Claridge, J.A.; Cocanour, C.S.; Coimbra, R.; Cook, C.H.; Cuschieri, J.; et al. Patients with complicated intra-abdominal infection presenting with sepsis do not require longer duration of antimicrobial therapy. J. Am. Coll. Surg. 2016, 222, 440–446. [Google Scholar] [CrossRef]
- Basoli, A.; Chirletti, P.; Cirino, E.; D’Ovidio, N.G.; Doglietto, G.B.; Giglio, D.; Giulini, S.M.; Malizia, A.; Taffurelli, M.; Petrovic, J.; et al. A prospective, double-blind, multicenter, randomized trial comparing ertapenem 3 vs >or=5 days in community-acquired intraabdominal infection. J. Gastrointest. Surg. 2008, 12, 592–600. [Google Scholar] [CrossRef]
- Cole, K.; Phlamon, M.; Petite, S.E. Comparison of short-course and prolonged antimicrobial therapy in the management of intra-abdominal infections. Surg. Infect. 2019, 20, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, C.; Zak, M.; Avery, L.; Brown, J. Treatment modalities and antimicrobial stewardship initiatives in the management of intra-abdominal infections. Antibiotics 2016, 5, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, B.R.; Kallehave, F.L.; Andersen, H.K. Antibiotics versus placebo for prevention of postoperative infection after appendicectomy. Cochrane Database Syst. Rev. 2005, CD001439. [Google Scholar] [CrossRef]
- Litz, C.N.; Asuncion, J.B.; Danielson, P.D.; Chandler, N.M. Timing of antimicrobial prophylaxis and infectious complications in pediatric patients undergoing appendectomy. J. Pediatr. Surg. 2018, 53, 449–451. [Google Scholar] [CrossRef] [PubMed]
- Lob, S.H.; Badal, R.E.; Bouchillon, S.K.; Hawser, S.P.; Hackel, M.A.; Hoban, D.J. Epidemiology and susceptibility of gram-negative appendicitis pathogens: SMART 2008–2010. Surg. Infect. 2013, 14, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Viel-Thériault, I.; Bettolli, M.; Toye, B.; Harrison, M.-A.; Le Saux, N. Contemporary microbiology and antimicrobial treatment of complicated appendicitis: The value of a short-term study. Pediatr. Infect. Dis. J. 2019, 38, e290–e294. [Google Scholar] [CrossRef] [PubMed]
- Popovski, Z.; Mercuri, M.; Main, C.; Sne, N.; Walsh, K.; Sung, M.; Rice, T.; Mertz, D. Multifaceted intervention to optimize antibiotic use for intra-abdominal infections. J. Antimicrob. Chemother. 2015, 70, 1226–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubrovskaya, Y.; Papadopoulos, J.; Scipione, M.R.; Altshuler, J.; Phillips, M.; Mehta, S.A. Antibiotic stewardship for intra-abdominal infections: Early impact on antimicrobial use and patient outcomes. Infect. Control Hosp. Epidemiol. 2012, 33, 427–429. [Google Scholar] [CrossRef]
- Skarda, D.E.; Schall, K.; Rollins, M.; Andrews, S.; Olson, J.; Greene, T.; McFadden, M.; Thorell, E.A.; Barnhart, D.; Meyers, R.; et al. A dynamic postoperative protocol provides efficient care for pediatric patients with non-ruptured appendicitis. J. Pediatr. Surg. 2015, 50, 149–152. [Google Scholar] [CrossRef]
- Tamma, P.D.; Avdic, E.; Keenan, J.F.; Zhao, Y.; Anand, G.; Cooper, J.; Dezube, R.; Hsu, S.; Cosgrove, S.E. What is the more effective antibiotic stewardship intervention: Preprescription authorization or postprescription review with feedback? Clin. Infect. Dis. 2017, 64, 537–543. [Google Scholar]
- Hurst, A.L.; Child, J.; Pearce, K.; Palmer, C.; Todd, J.K.; Parker, S.K. Handshake stewardship: A highly effective rounding-based antimicrobial optimization service. Pediatr. Infect. Dis. J. 2016, 35, 1104–1110. [Google Scholar] [CrossRef] [Green Version]
- Grau, S.; Bou, G.; Fondevilla, E.; Nicolás, J.; Rodríguez-Maresca, M.; Martínez-Martínez, L. How to measure and monitor antimicrobial consumption and resistance. Enferm. Infecc. Microbiol. Clin. 2013, 31, 16–24. [Google Scholar] [CrossRef]
- Baditoiu, L.; Axente, C.; Lungeanu, D.; Muntean, D.; Horhat, F.; Moldovan, R.; Hogea, E.; Bedreag, O.; Sandesc, D.; Licker, M. Intensive care antibiotic consumption and resistance patterns: A cross-correlation analysis. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- Christensen, E.W.; Spaulding, A.B.; Pomputius, W.F.; Grapentine, S.P. Effects of hospital practice patterns for antibiotic administration for pneumonia on hospital lengths of stay and costs. J. Pediatric. Infect. Dis. Soc. 2019, 8, 115–121. [Google Scholar] [CrossRef]
- CODA Collaborative; Flum, D.R.; Davidson, G.H.; Monsell, S.E.; Shapiro, N.I.; Odom, S.R.; Sanchez, S.E.; Drake, F.T.; Fischkoff, K.; Johnson, J.; et al. A Randomized Trial Comparing Antibiotics with Appendectomy for Appendicitis. N. Engl. J. Med. 2020, 383, 1907–1919. [Google Scholar]
- Huang, L.; Yin, Y.; Yang, L.; Wang, C.; Li, Y.; Zhou, Z. Comparison of Antibiotic Therapy and Appendectomy for Acute Uncomplicated Appendicitis in Children: A Meta-analysis. JAMA Pediatr. 2017, 171, 426–434. [Google Scholar] [CrossRef]
- Ashiru-Oredope, D.; Budd, E.L.; Bhattacharya, A.; Din, N.; McNulty, C.A.M.; Micallef, C.; Ladenheim, D.; Beech, E.; Murdan, S.; Hopkins, S. Implementation of antimicrobial stewardship interventions recommended by national toolkits in primary and secondary healthcare sectors in England: TARGET and Start Smart Then Focus. J. Antimicrob. Chemother. 2016, 71, 1408–1414. [Google Scholar] [CrossRef]
- Donà, D.; Luise, D.; La Pergola, E.; Montemezzo, G.; Frigo, A.; Lundin, R.; Zaoutis, T.; Gamba, P.; Giaquinto, C. Effects of an antimicrobial stewardship intervention on perioperative antibiotic prophylaxis in pediatrics. Antimicrob. Resist. Infect. Control. 2019, 8, 13. [Google Scholar] [CrossRef] [Green Version]
- Goycochea-Valdivia, W.A.; Moreno-Ramos, F.; Paño-Pardo, J.R.; Aracil-Santos, F.J.; Baquero-Artigao, F.; del Rosal-Rabes, T.; Mellado-Peña, M.J.; Escosa-García, L. Identifying priorities to improve paediatric in-hospital antimicrobial use by cross-sectional evaluation of prevalence and appropriateness of prescription. Enferm. Infecc. Microbiol. Clin. 2017, 35, 556–562. [Google Scholar] [CrossRef]
- Cook, P.P.; Gooch, M. Long-term effects of an antimicrobial stewardship programme at a tertiary-care teaching hospital. Int. J. Antimicrob. Agents. 2015, 45, 262–267. [Google Scholar] [CrossRef]
- Peñalva, G.; Fernández-Urrusuno, R.; Turmo, J.M.; Hernández-Soto, R.; Pajares, I.; Carrión, L.; Vázquez-Cruz, I.; Botello, B.; García-Robredo, B.; Cámara-Mestres, M.; et al. Long-term impact of an educational antimicrobial stewardship programme in primary care on infections caused by extended-spectrum β-lactamase-producing Escherichia coli in the community: An interrupted time-series analysis. Lancet Infect. Dis. 2020, 20, 199–207. [Google Scholar] [CrossRef]
- Bundy, D.G.; Byerley, J.S.; Liles, E.A.; Perrin, E.M.; Katznelson, J.; Rice, H.E. Does this child have appendicitis? JAMA 2007, 298, 438–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, B.; Giroir, B.; Randolph, A. International Consensus Conference on Pediatric Sepsis. International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr. Crit. Care Med. 2005, 6, 2–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, H.; Nathwani, D. Global-PPS: Global Point Prevalence Survey of Antimicrobial Consumption and Resistance 2017 (Protocol-version September 2016). Global-PPS. Available online: http://www.global-pps.com/documents/ (accessed on 30 October 2020).
- European Centre for Disease Prevention and Control. Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals–Protocol Version 5.3. ECDC. Available online: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/PPS-HAI-antimicrobial-use-EU-acute-care-hospitals-V5-3.pdf (accessed on 30 October 2020).
- Point Prevalence Survey of the Spanish Study of the Prevalence of Nosocomial Infections (EPINE-PPS) (Codebook. Version 9.0). SEMPSPH. Available online: http://www.sempsph.com/media/com_jnews/upload/EPINE-EPPS%202016%20Protocolo%20(v9.0).pdf (accessed on 30 October 2020).
- Benić, M.S.; Milanič, R.; Monnier, A.A.; Gyssens, I.C.; Adriaenssens, N.; Versporten, A.; Zanichelli, V.; Le Maréchal, M.; Huttner, B.; Tebano, G.; et al. Metrics for quantifying antibiotic use in the hospital setting: Results from a systematic review and international multidisciplinary consensus procedure. J. Antimicrob. Chemother. 2018, 73, vi50–vi58. [Google Scholar] [CrossRef]
- Moehring, R.W.; Dodds Ashley, E.S.; Ren, X.; Lokhnygina, Y.; Baker, A.W.; Jones, T.M.; Lewis, S.S.; Sexton, D.J.; Anderson, D.J. Denominator matters in estimating antimicrobial use: A comparison of days present and patient days. Infect. Control Hosp. Epidemiol. 2018, 39, 612–615. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Preintervention Period | Postintervention Period | ||||||
|---|---|---|---|---|---|---|---|
| Indicator | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | p |
| Days of therapy/100 patient days | 128.1 (118.4–143.6) | 122.6 (109.7–132.8) | 114.0 (110.6–126.8) | 128.8 (122.3–157.2) | 132.8 (117.2–140.6) | 144.0 (133.8–158.9) | 0.113 |
| Length of therapy/AR-IAI (days) | 4.7 (4.5–5.2) | 4.7 (4.4–5.4) | 5.2 (4.8–5.6) | 4.5 (4.0–4.6) | 4.4 (4.0–5.2) | 4.1 (3.9–4.6) | 0.298 |
| Length of stay/AR-IAI (days) | 4.2 (4.0–4.7) | 4.5 (3.9–5.0) | 4.6 (3.8–5.1) | 4.0 (3.7–4.5) | 4.1 (3.7–4.9) | 3.6 (3.3–3.9) | 0.314 |
| Readmission rates | 2.6 (2.0–3.1) | 3.2 (2.7–3.9) | 5.9 (5.5–6.7) | 4.7 (4.1–5.1) | 3.5 (2.9–4.0) | 5.8 (5.3–6.3) | 0.513 |
| Case fatality rates | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.0 |
| AR-IAI (Recommended Duration of Treatment) | Preintervention Period (2014–2016) | Postintervention Period (2017–2019) |
|---|---|---|
| Phlegmonous appendicitis (1 to 3 doses) * | Cefoxitin | Cefoxitin |
| Alternative: | Alternative: | |
| Gentamicin + metronidazole | Gentamicin + metronidazole | |
| Gangrenous appendicitis with or without local peritonitis (3 to 5 days) | Cefoxitin | Cefoxitin |
| Alternative: | Alternative: | |
| Gentamicin + metronidazole | Gentamicin + metronidazole | |
| Appendicular peritonitis (7 to 10 days) | Piperacillin–tazobactam | Ceftriaxone plus metronidazole |
| Alternative: | Alternative: | |
| Gentamicin + metronidazole | Gentamicin + metronidazole or piperacillin–tazobactam | |
| Appendicular abscess or mass (7 to 10 days) & | Amoxicillin–clavulanate | Amoxicillin–clavulanate |
| Alternative: | Alternative: | |
| Piperacillin–tazobactam | Gentamicin + metronidazole | |
| Appendicular-related sepsis [43] | Meropenem 7–10 days | Meropenem 5–7 days |
| Alternative: | Alternative: | |
| Piperacillin–tazobactam +/− aminoglycoside | Piperacillin–tazobactam +/− aminoglycoside |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simó, S.; Velasco-Arnaiz, E.; Ríos-Barnés, M.; López-Ramos, M.G.; Monsonís, M.; Urrea-Ayala, M.; Jordan, I.; Casadevall-Llandrich, R.; Ormazábal-Kirchner, D.; Cuadras-Pallejà, D.; et al. Effects of a Paediatric Antimicrobial Stewardship Program on Antimicrobial Use and Quality of Prescriptions in Patients with Appendix-Related Intraabdominal Infections. Antibiotics 2021, 10, 5. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010005
Simó S, Velasco-Arnaiz E, Ríos-Barnés M, López-Ramos MG, Monsonís M, Urrea-Ayala M, Jordan I, Casadevall-Llandrich R, Ormazábal-Kirchner D, Cuadras-Pallejà D, et al. Effects of a Paediatric Antimicrobial Stewardship Program on Antimicrobial Use and Quality of Prescriptions in Patients with Appendix-Related Intraabdominal Infections. Antibiotics. 2021; 10(1):5. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010005
Chicago/Turabian StyleSimó, Sílvia, Eneritz Velasco-Arnaiz, María Ríos-Barnés, María Goretti López-Ramos, Manuel Monsonís, Mireia Urrea-Ayala, Iolanda Jordan, Ricard Casadevall-Llandrich, Daniel Ormazábal-Kirchner, Daniel Cuadras-Pallejà, and et al. 2021. "Effects of a Paediatric Antimicrobial Stewardship Program on Antimicrobial Use and Quality of Prescriptions in Patients with Appendix-Related Intraabdominal Infections" Antibiotics 10, no. 1: 5. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010005