Efficiency of Diagnostic Testing for Helicobacter pylori Infections—A Systematic Review

 ,
,  ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Types of Studies
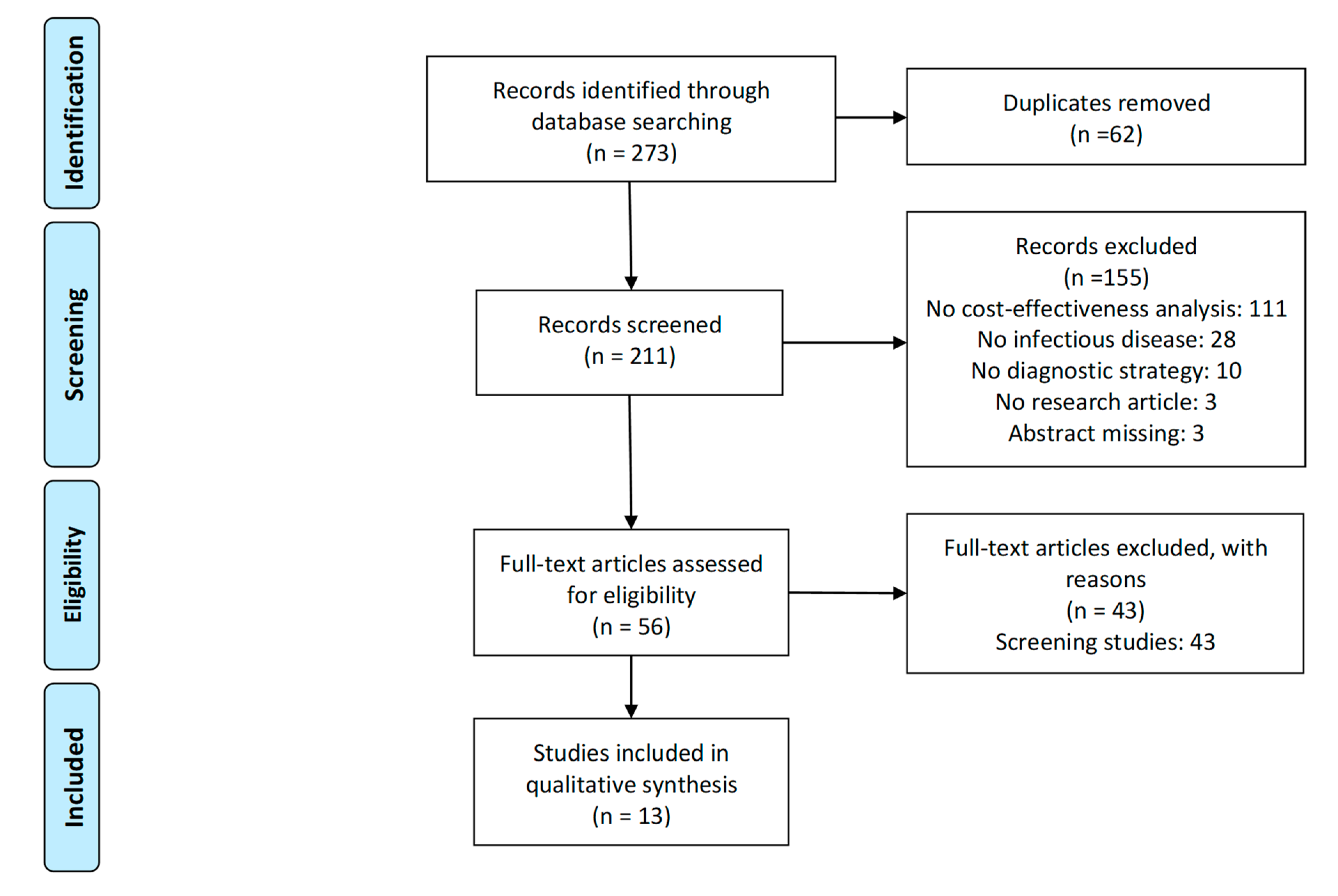
2.2. Search Strategy and Selection Criteria
2.3. Data Extraction and Analysis
3. Results
3.1. Diagnostics of H. pylori Infection Associated with Dyspepsia
3.2. Diagnostics of H. pylori Infection Associated with Duodenal Ulcers
3.3. Diagnostics of. H. pylori Infection
4. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| SCOPUS |
| (TITLE-ABS-KEY(pharmacoeconomic *) |
| OR TITLE-ABS-KEY(cost-effectiveness) |
| OR TITLE-ABS-KEY(“economic evaluation”) |
| OR TITLE-ABS-KEY(“health technology assessment”)) |
| AND (TITLE-ABS-KEY(antibiotic*) |
| OR TITLE-ABS-KEY(infectious) |
| OR TITLE-ABS-KEY(“bacterial infection”) |
| OR TITLE-ABS-KEY(“viral infection”)) |
| AND (TITLE-ABS-KEY(“diagnostic”) |
| OR TITLE-ABS-KEY(“diagnostics”) |
| OR TITLE-ABS-KEY(“test”) |
| OR TITLE-ABS-KEY(“tests”) |
| OR TITLE-ABS-KEY(“testing”)) |
| AND (TITLE-ABS-KEY(“pylori”)) |
| AND PUBYEAR > 1999 |
| AND PUBYEAR < 2020 |
| PUBMED |
| (infectious |
| OR “bacterial infection” |
| OR “viral infection” |
| OR antibiotic * |
| OR antimicrobial) |
| AND (“diagnostic” |
| OR “diagnostics” |
| OR “test” |
| OR “tests” |
| OR “testing”) |
| AND (“1 Januray 2000”[Date—Publication]: “31 December 2020”[Date—Publication]) |
| AND (pharmacoeconomic * |
| OR “cost-effectiveness” |
| OR “economic evaluation” |
| OR “health technology assessment”) |
| AND (“pylori”) |
| WEB OF SCIENCE |
| TS = (((“bacterial infection” |
| OR “viral infection” |
| OR antibiotic * |
| OR antimicrobial |
| OR infectious) |
| AND (“diagnostics” |
| OR “diagnostic” |
| OR “test” |
| OR “tests” |
| OR “testing”) |
| AND |
| (pharmacoeconomic* |
| OR cost-effectiveness |
| OR “economic evaluation” |
| OR “health technology assessment”) |
| AND (“pylori”))) |
| Period of time: 2000–2020 |
References
- Guevara, B.; Cogdill, A.G. Helicobacter pylori: A Review of Current Diagnostic and Management Strategies. Dig. Dis Sci. 2020, 65, 1917–1931. [Google Scholar] [CrossRef]
- Warren, J.R.; Marshall, B. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1983, 1, 1273–1275. [Google Scholar]
- Hu, Y.; Wan, J.-H.; Li, X.-Y.; Zhu, Y.; Graham, D.Y.; Lu, N.-H. Systematic review with meta-analysis: The global recurrence rate of Helicobacter pylori. Aliment. Pharmacol Ther. 2017, 46, 773–779. [Google Scholar] [CrossRef] [Green Version]
- Plummer, M.; Franceschi, S.; Vignat, J.; Forman, D.; de Martel, C. Global burden of gastric cancer attributable to Helicobacter pylori. Int. J. Cancer 2015, 136, 487–490. [Google Scholar] [CrossRef]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef]
- Kasahun, G.G.; Demoz, G.T.; Desta, D.M. Primary Resistance Pattern of Helicobacter pylori to Antibiotics in Adult Population: A Systematic Review. Infect. Drug Resist. 2020, 13, 1567–1573. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Boyanova, L.; Gergova, G.; Evstatiev, I.; Spassova, Z.; Kandilarov, N.; Yaneva, P.; Markovska, R.; Mitov, I. Helicobacter pylori resistance to six antibiotics by two breakpoint systems and resistance evolution in Bulgaria. Infect. Dis. 2016, 48, 56–62. [Google Scholar] [CrossRef]
- Megraud, F.; Coenen, S.; Versporten, A.; Kist, M.; Lopez-Brea, M.; Hirschl, A.M.; Andersen, L.P.; Goossens, H.; Glupczynski, Y. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut 2013, 62, 34–42. [Google Scholar] [CrossRef]
- Saracino, I.M.; Zullo, A.; Holton, J.; Castelli, V.; Fiorini, G.; Zaccaro, C.; Ridola, L.; Ricci, C.; Gatta, L.; Vaira, D. High prevalence of primary antibiotic resistance in Helicobacter pylori isolates in Italy. J. Gastrointestin. Liver Dis. 2012, 21, 363–365. [Google Scholar]
- Kobayashi, I.; Murakami, K.; Kato, M.; Kato, S.; Azuma, T.; Takahashi, S.I.; Uemura, N.; Katsuyama, T.; Fukuda, Y.; Haruma, K.; et al. Changing antimicrobial susceptibility epidemiology of Helicobacter pylori strains in Japan between 2002 and 2005. J. Clin. Microbiol. 2007, 45, 4006–4010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toros, A.B.; Ince, A.T.; Kesici, B.; Saglam, M.; Polat, Z.; Uygun, A. A new modified concomitant therapy for Helicobacter pylori eradication in Turkey. Helicobacter 2011, 16, 225–228. [Google Scholar] [CrossRef]
- Lu, H.; Zhang, W.; Graham, D.Y. Bismuth-containing quadruple therapy for Helicobacter pylori: Lessons from China. Eur. J. Gastroenterol. Hepatol. 2013, 25, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Yonezawa, H.; Osaki, T.; Kamiya, S. Biofilm Formation by Helicobacter pylori and Its Involvement for Antibiotic Resistance; Manfredi, M., Ed.; BioMed Research International Hindawi Publishing Corporation: London, UK, 2015. [Google Scholar]
- O’Morain, N.R.; Dore, M.P.; O’Connor, A.J.P.; Gisbert, J.P.; O’Morain, C.A. Treatment of Helicobacter pylori infection in 2018. Helicobacter 2018, 23 (Suppl. S1), e12519. [Google Scholar]
- Delgado, J.S.; García-Iglesias, P.; Titó, L.; Puig, I.; Planella, M.; Gené, E.; Saló, J.; Martínez-Cerezo, F.; Molina-Infante, J.; Gisbert, J.P.; et al. Update on the management of Helicobacter pylori infection. Position paper from the Catalan Society of Digestology. Gastroenterol. Hepatol. 2018, 41, 272–280. [Google Scholar]
- González-Carbajal Pascual, M.; Martínez Leyva, L. MAASTRICHT III and dyspepsia. Reasons for a discrepancy. Rev. Cubana Med. 2008, 47, 4. [Google Scholar]
- Saleem, N.; Howden, C.W. Update on the Management of Helicobacter pylori Infection. Curr. Treat. Options Gastroenterol. 2020, 18, 476–487. [Google Scholar] [CrossRef]
- Pichon, M.; Pichard, B.; Barrioz, T.; Plouzeau, C.; Croquet, V.; Fotsing, G.; Chéron, A.; Vuillemin, É.; Wangermez, M.; Haineaux, P.A.; et al. Diagnostic Accuracy of a Noninvasive Test for Detection of Helicobacter pylori and Resistance to Clarithromycin in Stool by the Amplidiag H. pylori+ClariR Real-Time PCR Assay. J. Clin. Microbiol. 2020, 58, e01787-19. [Google Scholar] [CrossRef]
- Zou, Y.; Qian, X.; Liu, X.; Song, Y.; Song, C.; Wu, S.; An, Y.; Yuan, R.; Wang, Y.; Xie, Y. The effect of antibiotic resistance on Helicobacter pylori eradication efficacy: A systematic review and meta-analysis. Helicobacter 2020, 25, e12714. [Google Scholar] [CrossRef]
- Kim, S.Y.; Chung, J.-W. Best Helicobacter pylori Eradication Strategy in the Era of Antibiotic Resistance. Antibiotics 2020, 9, 436. [Google Scholar] [CrossRef]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382.e17. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulia, M.S.; O’Brien, T.P.; Hou, P.C.; Schuman, A.; Sambursky, R. Multi-Tiered Screening and Diagnosis Strategy for COVID-19: A Model. for Sustainable Testing Capacity in Response to Pandemic. Ann. Med. 2020, 52, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Bhise, V.; Rajan, S.S.; Sittig, D.F.; Morgan, R.O.; Chaudhary, P.; Singh, H. Defining and Measuring Diagnostic Uncertainty in Medicine: A Systematic Review. J. Gen. Intern. Med. 2018, 33, 103–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husereau, D. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. BMJ 2013, 346, 1049. [Google Scholar] [CrossRef] [Green Version]
- Chey, W.D.; Fendrick, A.M. Noninvasive Helicobacter pylori testing for the “test-and-treat” strategy: A decision analysis to assess the effect of past infection on test choice. Arch. Intern. Med. 2001, 161, 2129–2132. [Google Scholar] [CrossRef] [Green Version]
- Makris, N.; Barkun, A.; Crott, R.; Fallone, C.A. Cost-effectiveness of alternative approaches in the management of dyspepsia. Int. J. Technol. Assess. Health Care 2003, 19, 446–464. [Google Scholar] [CrossRef]
- García-Altés, A.; Rota, R.; Barenys, M.; Abad, Á.; Moreno, V.; Pons, J.M.; Piqué, J. Cost-effectiveness of a “score and scope” strategy for the management of dyspepsia. Eur. J. Gastroenterol. Hepatol. 2005, 17, 709–719. [Google Scholar]
- You, J.H.S.; Wong, P.-L.; Wu, J.C.Y. Cost-effectiveness of Helicobacter pylori “test and treat” for patients with typical reflux symptoms in a population with a high prevalence of H. pylori infection: A Markov model analysis. Scand. J. Gastroenterol. 2006, 41, 21–29. [Google Scholar] [CrossRef]
- Holmes, K.P.; Fang, J.C.; Jackson, B.R. Cost-effectiveness of six strategies for Helicobacter pyloridiagnosis and management in uninvestigated dyspepsia assuming a high resource intensity practice pattern. BMC Health Serv. Res. 2010, 10, 344. [Google Scholar] [CrossRef] [Green Version]
- Papaefthymiou, A.; Liatsos, C.; Georgopoulos, S.D.; Apostolopoulos, P.; Doulberis, M.; Kyriakos, N.; Giakoumis, M.; Papadomichelakis, M.; Galanopoulos, M.; Katsinelos, P.; et al. Helicobacter pylori eradication regimens in an antibiotic high-resistance European area: A cost-effectiveness analysis. Helicobacter 2020, 25, e12666. [Google Scholar] [CrossRef] [PubMed]
- Rich, M.; Scheiman, J.M.; Tierney, W.; Fendrick, A.M. Is upper gastrointestinal radiography a cost-effective alternative to a Helicobacter pylori “test and treat” strategy for patients with suspected peptic ulcer disease? Am. J. Gastroenterol. 2000, 95, 651–658. [Google Scholar] [PubMed]
- Ghoshal, U.C.; Das, A. Management strategies for duodenal ulcer in India in the Helicobacter pylori era: An economic analysis. Natl. Med J. India 2002, 15, 140–144. [Google Scholar] [PubMed]
- Ghoshal, U.C.; Aggarwal, R.; Sreenivasa Baba, C. Recurrent duodenal ulcer haemorrhage: A pharmacoeconomic comparison of various management strategies. Expert Opin. Pharmacother. 2003, 4, 1593–1603. [Google Scholar] [CrossRef]
- Cho, J.-H.; Jeon, S.R.; Kim, H.G.; Jin, S.-Y.; Park, S. Cost-effectiveness of a tailored Helicobacter pylori eradication strategy based on the presence of a 23S ribosomal RNA point mutation that causes clarithromycin resistance in Korean patients. J. Gastroenterol. Hepatol. 2019, 34, 700–706. [Google Scholar] [CrossRef]
- Vakil, N.; Rhew, D.; Soll, A.; Ofman, J.J. The cost-effectiveness of diagnostic testing strategies for Helicobacter pylori. Am. J. Gastroenterol. 2000, 95, 1691–1698. [Google Scholar] [CrossRef]
- Omata, F.; Shimbo, T.; Ohde, S.; Deshpande, G.A. Cost-Effectiveness Analysis of Helicobacter Pylori Diagnostic Methods in the Patients with Atrophic Gastritis. Gastroenterology 2017, 152, S448. [Google Scholar] [CrossRef] [Green Version]
- Beresniak, A.; Malfertheiner, P.; Franceschi, F.; Liebaert, F.; Salhi, H.; Gisbert, J.P. Helicobacter pylori “Test-and-Treat” strategy with urea breath test: A cost-effective strategy for the management of dyspepsia and the prevention of ulcer and gastric cancer in Spain—Results of the Hp-Breath initiative. Helicobacter 2020, 25, e12693. [Google Scholar] [CrossRef] [Green Version]
- Shirin, H.; Kenet, G.; Shevah, O.; Wardi, Y.; Birkenfeld, S.; Shahmurov, M.; Bruck, R.; Niv, Y.; Moss, S.F.; Avni, Y. Evaluation of a novel continuous real time 13C urea breath analyser for Helicobacter pylori. Aliment. Pharmacol. Ther. 2001, 15, 389–394. [Google Scholar] [CrossRef]
- Hirayama, Y.; Kawai, T.; Otaki, J.; Kawakami, K.; Harada, Y. Prevalence of Helicobacter pylori infection with healthy subjects in Japan. J. Gastroenterol. Hepatol. 2014, 29, 16–19. [Google Scholar] [CrossRef]
- Castañeda Guillot, C. Sobrecrecimiento bacteriano intestinal. Rev. Médica Chile 2006, 8, 4–7. [Google Scholar]
- Xuan, S.; Zangwill, K.M.; Ni, W.; Ma, J.; Hay, J.W. Cost-Effectiveness Analysis of Four Common Diagnostic Methods for Clostridioides difficile Infection. J. Gen. Intern. Med. 2020, 35, 1102–1110. [Google Scholar] [CrossRef] [PubMed]
- Kastenberg, Z.J.; Hurley, M.P.; Luan, A.; Vasu-Devan, V.; Spain, D.A.; Owens, D.K.; Goldhaber-Fiebert, J.D. Cost-effectiveness of preoperative imaging for appendicitis after indeterminate ultrasonography in the second or third trimester of pregnancy. Obstet. Gynecol. 2013, 122, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Shen, B. Diagnosis and treatment of patients with pouchitis. Drugs 2003, 63, 453–461. [Google Scholar] [CrossRef]
- Pilotto, A.; Franceschi, M. Helicobacter pylori infection in older people. World J. Gastroenterol. 2014, 20, 6364–6373. [Google Scholar] [CrossRef]


{kind=link}
| CHEERS Items | H. pylori Infection Associated with Dyspepsia (n = 6) | H. pylori Infection Associated with Duodenal Ulcer (n = 4) | H. pylori Infection Alone (n = 3) |
|---|---|---|---|
| Title | 100% | 100% | 100% |
| Abstract | 100% | 100% | 100% |
| Background and objective | 100% | 100% | 100% |
| Target population | 100% | 100% | 100% |
| Setting | 16% | 25% | 100% |
| Study perspective | 100% | 100% | 100% |
| Interventions compared | 100% | 100% | 100% |
| Treatment | 100% | 100% | 33% |
| Time horizon | 16% | 100% | 33% |
| Discount rate for health outcomes | 0% | 0% | 0% |
| Discount rate for economic outcomes | 0% | 25% | 0% |
| Reported clinical outcomes | 100% | 100% | 100% |
| Measurement of effectiveness | 100% | 100% | 100% |
| Resource and cost estimations | 100% | 100% | 100% |
| Currency year used | 50% | 25% | 33% |
| Type of model | 100% | 100% | 100% |
| Assumptions | 100% | 100% | 100% |
| Analytical methods | 100% | 100% | 100% |
| Study parameters | 100% | 100% | 100% |
| Characterizing uncertainty | 100% | 100% | 100% |
| Study findings, limitations, generalizability and current knowledge | 83% | 100% | 100% |
| Source of funding | 83% | 0% | 33% |
| Conflicts of interest | 50% | 0% | 33% |
| First Author (year) | Country | Setting | Perspective and Time Horizon | Type of Model | Strategies Compared 1 | Treatment | AMR Included | Uncertainty Reported |
|---|---|---|---|---|---|---|---|---|
| Chey (2001) [27] | USA | PC | Healthcare center’s— NA | Decision tree | (1) Antibody test, if positive treat; (2) Active H. pylori infection test, if positive treat | Lansoprazole, clarithromycin and amoxicillin | No | SAG |
| Makris (2003) [28] | Canada | PC | Healthcare payer’s— 1 year | Decision tree | (1) Empirical eradication therapy; (2) Endoscopy; (3) Barium examination; (4) Eradication therapy; (5) Antisecretory regimen; (6) UBT; (7) Laboratory testing, if positive therapy; (8) H. pylori test and urea breath test | Eradication therapy | No | DSA, tornado diagram, two-way SAG |
| García- Altés (2005)[29] | Spain | PC | Healthcare payer’s— 1 year | Decision tree | (1) Endoscopy; (2) Score and scope; (3) Test and scope; (4) Test and treat; (5) Empirical antisecretory treatment | Clarithromycin, amoxicillin and omeprazole | No | DSA, two-way SAG |
| You (2006) [30] | China | PC | Healthcare center’s— 1 year | Markov model | (1) Treat none; (2) Empirical PPI therapy; (3) Test and treat; (4) Endoscopy | Eradication therapy or PPI | Yes | DSA |
| Holmes (2010) [31] | USA | PC | Societal-lifetime | Markov model | (1) H. pylori tests; (2) H. pylori IgG test; (3) Stool antigen test; (4) IgG test; (5) UBT; (6) PPI trial | Eradication therapy or PPI | No | PSA |
| Papaefthymiou (2020) [32] | Greece | Hospital | Healthcare payer’s— 1 year | Decision tree | (1) Esophagogastroduodenoscopy; (2) Specific UBT test for H. pylori; (3) Giemsa stain | Non-bismuth quadruple eradication | Yes | DSA |
| First Author (year) | Country | Setting | Perspective and Horizon | Type of Model | Strategies Compared 1 | Treatment | AMR Included | Uncertainty Reported |
|---|---|---|---|---|---|---|---|---|
| Rich (2000) [33] | USA | NA | Healthcare payer’s—1 year | Decision tree | (1) Test and treat; (2) Upper gastrointestinal radiography | Antibiotics and antisecretory agents | No | SAG |
| Ghoshal (2002) [34] | India | PC | Healthcare payer’s—1 year | Decision tree | (1) Anti-secretory therapy; (2) RUT and histological examination for H. pylori; (3) Empirical triple therapy | Antisecretory, amoxycillin and tinidazole or PPI | No | Two-way SAG |
| Ghoshal (2003) [35] | India | Hospital | Healthcare payer’s—2 years | Decision tree | (1) Anti-secretory therapy; (2) RUT and histological examination for H. pylori; (3) Empirical triple therapy | Antisecretory, amoxycillin and tinidazole or PPI | No | DSA, two-way SAG |
| Cho (2019) [36] | Korea | Hospital | Healthcare payer’s—1 year | Decision tree | (1) RUT; (2) DPO-PCR | Triple regimen or quadruple regimen | Yes | SAG, CE acceptability curve |
| First Author (year) | Country | Setting | Perspective and Horizon | Type of Model | Strategies Compared 1 | Treatment | AMR Included | Uncertainty Reported |
|---|---|---|---|---|---|---|---|---|
| Vakil (2000) [37] | USA | PC | Healthcare payer’s—NA | Decision tree | Thirty-six testing strategies, included sequences of: test for H. pylori, serology ELISA, UBT, fingerstick blood test, stool antigen test, RUT and histology | NA | No | SAG |
| Omata (2017) [38] | Japan | PC | Societal—1 year | Decision tree | (1) RUT; (2) Histology; (3) Bacterial culture; (4) Serum H. pylori IgG antibody (SHPAb); (5) UBT; (6) SHPAg; (7) UHPAb | Lansoprazole, amoxicillin and clarithromycin | Yes | SAG, CE acceptability curve |
| Beresniak (2020) [39] | Spain | PC | Healthcare system’s—1 year | Decision tree | (1) Test and treat for H. pylori; (2) UBT; (3) Endoscopy; (4) Symptomatic treatment | Antibiotics (1st and 2nd line) | No | PSA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas García, P.; van der Pol, S.; van Asselt, A.D.I.; Postma, M.; Rodríguez-Ibeas, R.; Juárez-Castelló, C.A.; González, M.; Antoñanzas, F. Efficiency of Diagnostic Testing for Helicobacter pylori Infections—A Systematic Review. Antibiotics 2021, 10, 55. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010055
Rojas García P, van der Pol S, van Asselt ADI, Postma M, Rodríguez-Ibeas R, Juárez-Castelló CA, González M, Antoñanzas F. Efficiency of Diagnostic Testing for Helicobacter pylori Infections—A Systematic Review. Antibiotics. 2021; 10(1):55. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010055
Chicago/Turabian StyleRojas García, Paula, Simon van der Pol, Antoinette D. I. van Asselt, Maarten Postma, Roberto Rodríguez-Ibeas, Carmelo A. Juárez-Castelló, Marino González, and Fernando Antoñanzas. 2021. "Efficiency of Diagnostic Testing for Helicobacter pylori Infections—A Systematic Review" Antibiotics 10, no. 1: 55. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010055