Carriage of Carbapenem-Resistant Enterobacterales in Adult Patients Admitted to a University Hospital in Italy

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Antimicrobial Resistance
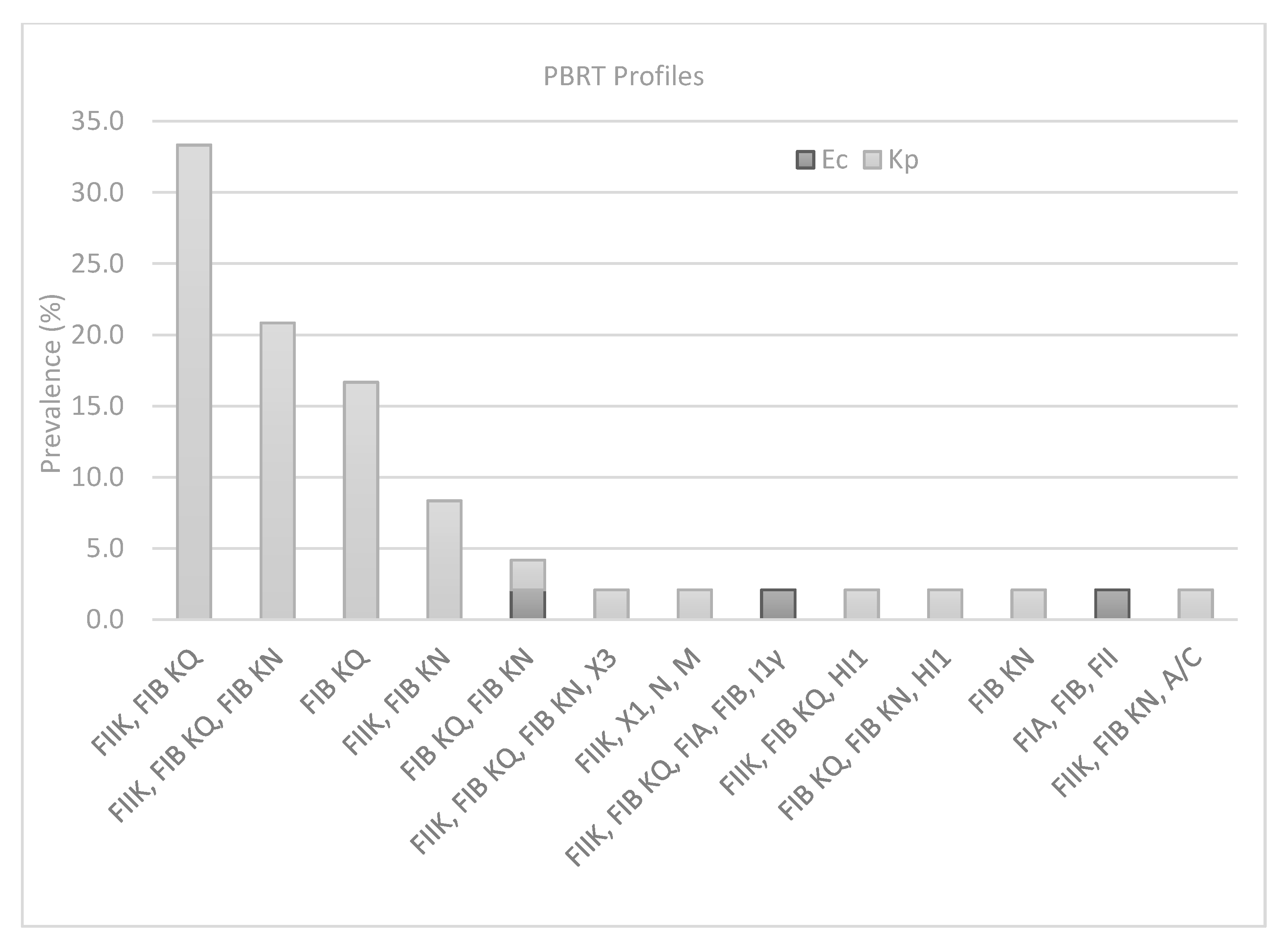
2.2. Plasmid Typing and Classification
2.3. Multilocus Sequence Typing Analysis
2.4. Epidemiological Data
3. Discussion
4. Materials and Methods
4.1. Bacterial Isolates
4.2. Antimicrobial Susceptibility Testing
4.3. Molecular Detection of Resistance Determinants
4.4. PCR-Based Replicon Typing
4.5. Multilocus Sequence Typing (MLST)
4.6. Epidemiological Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bonomo, R.A.; Burd, E.M.; Conly, J.; Limbago, B.M.; Poirel, L.; Segre, J.A.; Westblade, L.F. Carbapenemase-Producing Organisms: A Global Scourge. Clin. Infect. Dis. 2018, 66, 1290–1297. [Google Scholar] [CrossRef] [PubMed]
- Queenan, A.M.; Bush, K. Carbapenemases: The versatile β-lactamases. Clin. Microbiol. Rev. 2007, 20, 440–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambretti, S.; Bassetti, M.; Clerici, P.; Petrosillo, N.; Tumietto, F.; Viale, P.; Rossolini, G.M. Screening for carriage of carbapenem-resistant Enterobacteriaceae in settings of high endemicity: A position paper from an Italian working group on CRE infections. Antimicrob. Resist. Infect. Control 2019, 8, 1–11. [Google Scholar] [CrossRef]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ECDC. SURVEILLANCE REPORT. Surveillance of Antimicrobial Resistance in Europe 2018; European Centre for Disease Prevention and Control (ECDC): Solna, Sweden, 2018. [Google Scholar]
- Giannella, M.; Trecarichi, E.M.; De Rosa, F.G.; Del Bono, V.; Bassetti, M.; Lewis, R.E.; Losito, A.R.; Corcione, S.; Saffioti, C.; Bartoletti, M.; et al. Risk factors for carbapenem-resistant Klebsiella pneumoniae bloodstream infection among rectal carriers: A prospective observational multicentre study. Clin. Microbiol. Infect. 2014, 20, 1357–1362. [Google Scholar] [CrossRef] [Green Version]
- Barbadoro, P.; Dichiara, A.; Arsego, D.; Ponzio, E.; Savini, S.; Manso, E.; D’errico, M.M. Spread of carbapenem-resistant Klebsiella pneumoniae in hub and spoke connected health-care networks: A case study from Italy. Microorganisms 2020, 8, 37. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Ridolfo, A.L.; Rimoldi, S.G.; Pagani, C.; Marino, A.F.; Piol, A.; Rimoldi, M.; Olivieri, P.; Galli, M.; Dolcetti, L.; Gismondo, M.R. Diffusion and transmission of carbapenem-resistant Klebsiella pneumoniae in the medical and surgical wards of a university hospital in Milan, Italy. J. Infect. Public Health 2016, 9, 24–33. [Google Scholar] [CrossRef] [Green Version]
- Carloni, E.; Andreoni, F.; Omiccioli, E.; Villa, L.; Magnani, M.; Carattoli, A. Comparative analysis of the standard PCR-Based Replicon Typing (PBRT) with the commercial PBRT-KIT. Plasmid 2017, 90, 10–14. [Google Scholar] [CrossRef]
- Singh, K.; Mangold, K.A.; Wyant, K.; Schora, D.M.; Voss, B.; Kaul, K.L.; Hayden, M.K.; Chundi, V.; Peterson, L.R. Rectal screening for Klebsiella pneumoniae carbapenemases: Comparison of real-time PCR and culture using two selective screening agar plates. J. Clin. Microbiol. 2012, 50, 2596–2600. [Google Scholar] [CrossRef] [Green Version]
- Grundmann, H.; Glasner, C.; Albiger, B.; Aanensen, D.M.; Tomlinson, C.T.; Andrasević, A.T.; Cantón, R.; Carmeli, Y.; Friedrich, A.W.; Giske, C.G.; et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE): A prospective, multinational study. Lancet Infect. Dis. 2017, 17, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Sotgiu, G.; Are, B.M.; Pesapane, L.; Palmieri, A.; Muresu, N.; Cossu, A.; Dettori, M.; Azara, A.; Mura, I.I.; Cocuzza, C.; et al. Nosocomial transmission of carbapenem-resistant Klebsiella pneumoniae in an Italian university hospital: A molecular epidemiological study. J. Hosp. Infect. 2018, 99, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wang, X.; Wang, J.; Ouyang, P.; Jin, C.; Wang, R.; Zhang, Y.; Jin, L.; Chen, H.; Wang, Z.; et al. Phenotypic and Genotypic Characterization of Carbapenem-resistant Enterobacteriaceae: Data from a Longitudinal Large-scale CRE Study in China (2012–2016). Clin. Infect. Dis. 2018, 67, S196–S205. [Google Scholar] [CrossRef] [PubMed]
- Patel, G.; Bonomo, R.A. “Stormy waters ahead”: Global emergence of carbapenemases. Front. Microbiol. 2013, 4, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.; Zhang, K.; Chen, W.; Chen, J.; Zheng, J.; Liu, C.; Cheng, L.; Zhou, W.; Shen, H.; Cao, X. Epidemiological characteristics of carbapenem-resistant Enterobacteriaceae collected from 17 hospitals in Nanjing district of China. Antimicrob. Resist. Infect. Control 2020, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadimitriou-Olivgeris, M.; Bartzavali, C.; Lambropoulou, A.; Solomou, A.; Tsiata, E.; Anastassiou, E.D.; Fligou, F.; Marangos, M.; Spiliopoulou, I.; Christofidou, M. Reversal of carbapenemase-producing Klebsiella pneumoniae epidemiology from blaKPC-to blaVIM-harbouring isolates in a Greek ICU after introduction of ceftazidime/avibactam. J. Antimicrob. Chemother. 2019, 74, 2051–2054. [Google Scholar] [CrossRef]
- Zagorianou, A.; Sianou, E.; Iosifidis, E.; Dimou, V.; Protonotariou, E.; Miyakis, S.; Roilides, E.; Sofianou, D. Microbiological and molecular characteristics of carbapenemase-producing klebsiella pneumonia endemic in a tertiary Greek hospital during 2004–2010. Eurosurveillance 2012, 17, 1–7. [Google Scholar] [CrossRef]
- Carattoli, A. Plasmids and the spread of resistance. Int. J. Med. Microbiol. 2013, 303, 298–304. [Google Scholar] [CrossRef]
- Villa, L.; García-Fernández, A.; Fortini, D.; Carattoli, A. Replicon sequence typing of IncF plasmids carrying virulence and resistance determinants. J. Antimicrob. Chemother. 2010, 65, 2518–2529. [Google Scholar] [CrossRef] [Green Version]
- Mathers, A.J.; Peirano, G.; Pitout, J.D.D. The role of epidemic resistance plasmids and international high- risk clones in the spread of multidrug-resistant Enterobacteriaceae. Clin. Microbiol. Rev. 2015, 28, 565–591. [Google Scholar] [CrossRef] [Green Version]
- Netikul, T.; Kiratisin, P. Genetic characterization of carbapenem-resistant enterobacteriaceae and the spread of carbapenem-resistant klebsiella pneumonia ST340 at a university hospital in Thailand. PLoS ONE 2015, 10, e0139116. [Google Scholar] [CrossRef] [PubMed]
- Del Franco, M.; Paone, L.; Novati, R.; Giacomazzi, C.G.; Bagattini, M.; Galotto, C.; Montanera, P.G.; Triassi, M.; Zarrilli, R. Molecular epidemiology of carbapenem resistant Enterobacteriaceae in Valle d’Aosta region, Italy, shows the emergence of KPC-2 producing Klebsiella pneumoniae clonal complex 101 (ST101 and ST1789). BMC Microbiol. 2015, 15, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roe, C.C.; Vazquez, A.J.; Esposito, E.P.; Zarrilli, R.; Sahl, J.W. Diversity, virulence, and antimicrobial resistance in isolates from the newly emerging klebsiella pneumoniaeST101 Lineage. Front. Microbiol. 2019, 10, 542. [Google Scholar] [CrossRef] [PubMed]
- Loconsole, D.; Accogli, M.; De Robertis, A.L.; Capozzi, L.; Bianco, A.; Morea, A.; Mallamaci, R.; Quarto, M.; Parisi, A.; Chironna, M. Emerging high-risk ST101 and ST307 carbapenem-resistant Klebsiella pneumoniae clones from bloodstream infections in Southern Italy. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 1–10. [Google Scholar] [CrossRef]
- Villa, L.; Feudi, C.; Fortini, D.; Brisse, S.; Passet, V.; Bonura, C.; Endimiani, A.; Mammina, C.; Ocampo, A.M.; Jimenez, J.N.; et al. Diversity, virulence, and antimicrobial resistance of the KPCproducing klebsiella pneumoniae ST307 clone. Microb. Genom. 2017, 3, e000110. [Google Scholar] [CrossRef]
- Coque, T.M.; Novais, A.; Carattoli, A.; Poirel, L.; Pitout, J.; Peixe, L.; Baquero, F.; Canton, R.; Nordmann, P. Dissemination of clonally related E.coli strains expressing ESBL CTX-M-15. Emerg. Infect. Dis. 2008, 14, 195–200. [Google Scholar] [CrossRef]
- Chowdhury, P.R.; McKinnon, J.; Liu, M.; Djordjevic, S.P. Multidrug resistant uropathogenic Escherichia coli ST405 with a novel, composite IS26 transposon in a unique chromosomal location. Front. Microbiol. 2019, 9, 3212. [Google Scholar] [CrossRef] [Green Version]
- Nicolas-Chanoine, M.H.; Bertrand, X.; Madec, J.Y. Escherichia coli st131, an intriguing clonal group. Clin. Microbiol. Rev. 2014, 27, 543–574. [Google Scholar] [CrossRef] [Green Version]
- Salomão, M.C.; Freire, M.P.; Boszczowski, I.; Raymundo, S.F.; Guedes, A.R.; Levin, A.S. Increased risk for carbapenem-resistant enterobacteriaceae colonization in intensive care units after hospitalization in emergency department. Emerg. Infect. Dis. 2020, 26, 1156–1163. [Google Scholar] [CrossRef]
- Salomão, M.C.; Guimarães, T.; Duailibi, D.F.; Perondi, M.B.M.; Letaif, L.S.H.; Montal, A.C.; Rossi, F.; Cury, A.P.; Duarte, A.J.S.; Levin, A.S.; et al. Carbapenem-resistant Enterobacteriaceae in patients admitted to the emergency department: Prevalence, risk factors, and acquisition rate. J. Hosp. Infect. 2017, 97, 241–246. [Google Scholar] [CrossRef]
- Giufrè, M.; Ricchizzi, E.; Accogli, M.; Barbanti, F.; Monaco, M.; de Araujo, F.P.; Farina, C.; Fazii, P.; Mattei, R.; Sarti, M.; et al. Colonization by multidrug-resistant organisms in long-term care facilities in Italy: A point-prevalence study. Clin. Microbiol. Infect. 2017, 23, 961–967. [Google Scholar] [CrossRef] [Green Version]
- Richter, S.S.; Marchaim, D. Screening for carbapenem-resistant Enterobacteriaceae: Who, When, and How? Virulence 2017, 8, 417–426. [Google Scholar] [CrossRef]
- Giske, C.G.; Gezelius, L.; Samuelsen, Ø.; Warner, M.; Sundsfjord, A.; Woodford, N. A sensitive and specific phenotypic assay for detection of metallo-β-lactamases and KPC in Klebsiella pneumoniae with the use of meropenem disks supplemented with aminophenylboronic acid, dipicolinic acid and cloxacillin. Clin. Microbiol. Infect. 2011, 17, 552–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn. Microbiol. Infect. Dis. 2011, 70, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Wirth, T.; Falush, D.; Lan, R.; Colles, F.; Mensa, P.; Wieler, L.H.; Karch, H.; Reeves, P.R.; Maiden, M.C.J.; Ochman, H.; et al. Sex and virulence in Escherichia coli: An evolutionary perspective. Mol. Microbiol. 2006, 60, 1136–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| a Isolate | b PBRT Profile | c CR Genes | d Antibiotic Resistance | e ST | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CN | AK | TOB | TZP | FOS | AMS | CIP | LEV | CXM | SXT | ||||
| Kp_6 | FIIK, FIB KQ | blaKPC | R | R | R | S | S | S | R | S | R | S | 512 |
| Kp_14 | blaKPC | S | S | S | S | S | S | S | S | R | S | ||
| Kp_48 | blaKPC | S | S | S | S | S | S | S | R | R | S | ||
| Kp_56 | blaKPC | S | S | S | S | S | S | S | R | R | S | ||
| Kp_58 | blaKPC | S | S | S | S | R | S | R | R | R | S | ||
| Kp_194 | blaKPC | S | S | S | S | R | S | S | S | R | S | ||
| Kp_282 | blaKPC | S | S | S | S | R | S | S | S | S | S | ||
| Kp_484 | blaKPC | R | R | R | S | S | S | R | R | R | R | ||
| Kp_485 | blaKPC | S | S | S | S | S | S | S | S | S | S | ||
| Kp_593 | blaKPC | S | S | R | R | R | R | S | S | R | S | ||
| Kp_605 | blaKPC | S | S | S | S | R | S | R | R | S | S | ||
| Kp_612 | blaKPC | R | R | R | S | S | S | R | R | R | R | ||
| Kp_613 | blaKPC | S | S | S | S | R | R | R | R | R | S | ||
| Kp_654 | blaKPC, blaVIM | S | R | R | S | R | R | R | R | R | R | ||
| Kp_660 | blaKPC | S | S | S | S | S | S | S | S | S | S | ||
| Kp_672 | blaKPC | R | R | R | S | S | S | R | S | R | S | ||
| Kp_506 | FIB KQ | blaKPC | S | S | S | S | S | S | S | S | S | S | 512 |
| Kp_604 | blaKPC | S | R | R | S | S | S | R | R | R | S | ||
| Kp_689 | blaKPC | S | S | S | R | R | R | R | R | S | S | ||
| Kp_690 | blaKPC | S | S | S | R | R | S | S | S | S | S | ||
| Kp_691 | blaKPC | S | S | S | S | S | S | R | R | S | S | ||
| Kp_696 | blaKPC | S | S | S | R | S | S | S | S | S | S | ||
| Kp_712 | blaKPC | S | S | S | S | R | R | R | S | S | S | ||
| Kp_714 | blaKPC | R | R | R | S | S | S | S | S | S | S | ||
| Kp_176 | FIIK, FIB KQ, FIB KN | blaKPC | S | S | S | S | S | S | S | S | S | S | 512 |
| Kp_13 | blaKPC | R | S | S | R | R | R | R | R | R | S | ||
| Kp_59 | blaKPC | S | S | S | R | R | R | S | S | S | S | ||
| Kp_60 | blaKPC | S | S | S | S | R | R | S | S | R | S | ||
| Kp_186 | blaKPC | S | S | S | S | S | S | S | S | S | S | ||
| Kp_187 | blaKPC | S | S | S | S | S | R | S | S | R | S | ||
| Kp_283 | blaKPC | S | S | S | R | S | R | S | S | S | S | ||
| Kp_285 | blaKPC | S | S | S | R | S | R | S | S | S | S | ||
| Kp_673 | blaKPC | S | S | S | S | S | S | S | S | R | S | ||
| Kp_679 | blaKPC | S | S | S | S | S | S | S | S | S | S | ||
| Kp_15 | FIIK, FIB KQ, HI1 | blaKPC | R | S | S | S | S | S | R | S | R | S | 512 |
| Kp_245 | FIIK, FIB KQ, FIB KN, X3 | blaKPC | S | S | S | S | S | R | S | S | S | S | 512 |
| Kp_709 | FIB KN | blaKPC | S | S | S | R | S | R | S | S | S | S | 101 |
| Kp_9 | FIIK, FIB KN | blaKPC | S | S | S | R | S | R | S | R | S | S | 101 |
| Kp_16 | blaKPC | R | S | S | S | S | R | R | S | R | S | ||
| Kp_17 | blaKPC | S | R | R | S | R | S | R | R | R | S | ||
| Kp_284 | blaKPC | S | S | S | S | S | S | S | S | S | S | ||
| Kp_19 | FIIK, FIB KN, A/C | blaKPC | S | R | S | S | R | S | R | R | R | S | 101 |
| Kp_49 | FIB KQ, FIB KN | blaKPC | S | S | S | R | S | R | S | S | S | S | 101 |
| Kp_640 | FIIK, X1,N, M | blaKPC | S | R | R | S | S | S | R | R | R | S | 307 |
| Kp_707 | FIB KQ, FIB KN, HI1 | blaKPC | S | S | S | R | R | R | S | R | R | S | 307 |
| Ec_136 | FIA, FIB, FII | - | S | S | R | S | S | R | R | R | R | S | 405 |
| Ec_705 | FIB KQ, FIB KN | blaKPC | S | S | S | R | R | R | R | R | R | S | 405 |
| Ec_178 | FIIK, FIB KQ, FIA, FIB, I1γ | blaKPC | S | S | S | R | R | R | R | R | R | S | 131 |
| Variables | Control | % | Cases | % | p |
|---|---|---|---|---|---|
| Age | |||||
| <44 | 2 | 4.2% | 4 | 8.3% | NS |
| 45–64 | 17 | 35.4% | 17 | 35.4% | NS |
| >65 | 29 | 60.4% | 27 | 56.3% | NS |
| Sex | |||||
| Male | 30 | 62.5% | 32 | 66.7% | NS |
| Origin of Patients | |||||
| Emergency department | 40 | 83.3% | 25 | 52.1% | <0.001 |
| Home | 3 | 6.3% | 10 | 20.8% | NS |
| 1 LTCF | - | 4 | 8.3% | 0.041 | |
| Other hospital | 5 | 10.4% | 9 | 18.8% | NS |
| Hospital admission during the previous 30 days | 11 | 22.9% | 11 | 22.9% | NS |
| Comorbidities | |||||
| Diabetes | 3 | 6.3% | 8 | 16.7% | NS |
| Renal disease | 13 | 27.1% | 7 | 14.6% | NS |
| Cardiovascular disease | 11 | 22.9% | 6 | 12.5% | NS |
| 2 COPD | 7 | 14.6% | 3 | 6.3% | NS |
| Cancer | 10 | 20.8% | 10 | 20.8% | NS |
| Presence of disability | 1 | 2.1% | 5 | 10.4% | NS |
| Respiratory failure | 14 | 29.2% | 9 | 18.8% | NS |
| Urinary tract infection | 9 | 18.8% | 3 | 6.3% | NS |
| Administration of antibiotics | 14 | 29.17% | 25 | 52.08% | 0.022 |
| Variables | OR | p Value | 95%CI |
|---|---|---|---|
| Previous use of antibiotics | 3.76 | 0.006 | 1.45–9.72 |
| Previous hospital admission 30 days | 3.00 | 0.023 | 1.16–7.71 |
| Emergency department (ED) | 0.27 | 0.010 | 0.10–0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbadoro, P.; Bencardino, D.; Carloni, E.; Omiccioli, E.; Ponzio, E.; Micheletti, R.; Acquaviva, G.; Luciani, A.; Masucci, A.; Pocognoli, A.; et al. Carriage of Carbapenem-Resistant Enterobacterales in Adult Patients Admitted to a University Hospital in Italy. Antibiotics 2021, 10, 61. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010061
Barbadoro P, Bencardino D, Carloni E, Omiccioli E, Ponzio E, Micheletti R, Acquaviva G, Luciani A, Masucci A, Pocognoli A, et al. Carriage of Carbapenem-Resistant Enterobacterales in Adult Patients Admitted to a University Hospital in Italy. Antibiotics. 2021; 10(1):61. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010061
Chicago/Turabian StyleBarbadoro, Pamela, Daniela Bencardino, Elisa Carloni, Enrica Omiccioli, Elisa Ponzio, Rebecca Micheletti, Giorgia Acquaviva, Aurora Luciani, Annamaria Masucci, Antonella Pocognoli, and et al. 2021. "Carriage of Carbapenem-Resistant Enterobacterales in Adult Patients Admitted to a University Hospital in Italy" Antibiotics 10, no. 1: 61. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010061