
Effectiveness of Pharmacist-Led Brief Educational Intervention for Adherence to the Antibiotics for Lower Respiratory Tract Infections (EATSA) in Post-Conflict Rural Areas of Pakistan: Study Protocol for a Randomized Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives and Hypothesis
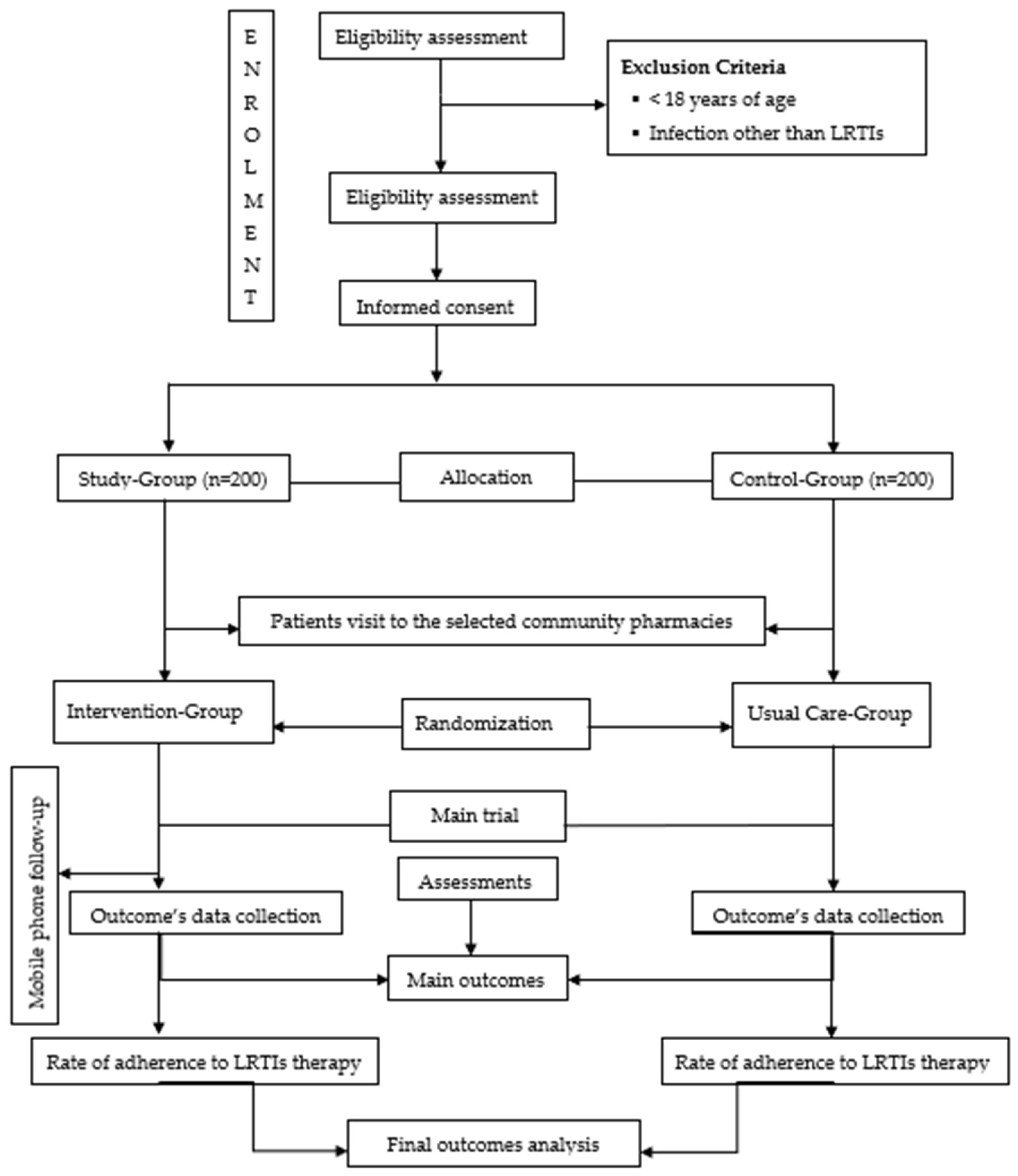
2.2. Study Design
2.3. Study Setting and Population
2.4. Data Collector’s Eligibility Criteria and Training
2.5. Intervention Group
2.5.1. Pharmacists Lead Educational Interventions at Community Pharmacies
2.5.2. Telephone-Based Follow-Up
2.6. Boost Usual Care (BUC)
2.7. Sample Size
2.8. Recruitment of the Participants
Inclusion Criteria
2.9. Randomization
2.10. Concealment of Allocation
2.11. Data Collection
2.12. Blinding
2.13. Participant Timeline
2.14. Outcome Measures
2.14.1. Primary Outcomes
2.14.2. Secondary Outcomes
2.15. Qualitative Evaluation
2.16. Trial Data Management
2.17. Statistical Analysis Methods
2.18. Data Dissemination
2.19. Adverse Event Monitoring
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Trial Status and Registration
Abbreviations
References
- Woodhead, M.; Blasi, F.; Ewig, S.; Garau, J.; Huchon, G.; Ieven, M.; Ortqvist, A.; Schaberg, T.; Torres, A.; van der Heijden, G.; et al. Guidelines for the management of adult lower respiratory tract infections—Full version. Clin. Microbiol. Infect. 2011, 17, E1–E59. [Google Scholar] [CrossRef] [Green Version]
- Troeger, C.; Forouzanfar, M.; Rao, P.C.; Khalil, I.; Brown, A.; Swartz, S.; Fullman, N.; Mosser, J.; Thompson, R.L.; Reiner, R.C.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 1133–1161. [Google Scholar] [CrossRef] [Green Version]
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the Global, Regional, and National Morbidity, Mortality, and Aetiologies of Lower Respiratory Infections in 195 Countries, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Greene, G.; Hood, K.; Little, P.; Verheij, T.; Goossens, H.; Coenen, S.; Butler, C.C. Towards clinical definitions of lower respiratory tract infection (LRTI) for research and primary care practice in Europe: An international consensus study. Prim. Care Respir. J. 2011, 20, 299–306. [Google Scholar] [CrossRef] [PubMed]
- File, T.M., Jr.; Marrie, T.J. Burden of community-acquired pneumonia in North American adults. Postgrad. Med. 2010, 122, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Isturiz, R.E.; Luna, C.M.; Ramirez, J. Clinical and economic burden of pneumonia among adults in Latin America. Int. J. Infect. Dis. 2010, 14, e852–e856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welte, T.; Torres, A.; Nathwani, D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax 2010, 67, 71–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, J.-H.; Thamlikitkul, V.; Hsueh, P.-R. Clinical and economic burden of community-acquired pneumonia amongst adults in the Asia-Pacific region. Int. J. Antimicrob. Agents 2011, 38, 108–117. [Google Scholar] [CrossRef]
- Morens, D.M.; Taubenberger, J.K.; Fauci, A.S. Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness. J. Infect. Dis. 2008, 198, 962–970. [Google Scholar] [CrossRef]
- Control, C.F.D. Chronic obstructive pulmonary disease among adults--United States, 2011. MMWR Morb. Mortal. Wkly. Rep. 2012, 61, 938. [Google Scholar]
- Feldman, C.; Shaddock, E. Epidemiology of lower respiratory tract infections in adults. Expert Rev. Respir. Med. 2019, 13, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Downie, L.; Armiento, R.; Subhi, R.; Kelly, J.; Clifford, V.; Duke, T. Community-acquired neonatal and infant sepsis in developing countries: Efficacy of WHO’s currently recommended antibiotics—Systematic review and meta-analysis. Arch. Dis. Child. 2013, 98, 146–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaacs, D.; Andresen, D. Combating antibiotic resistance: The war on error. Arch. Dis. Child. 2012, 98, 90–91. [Google Scholar] [CrossRef] [PubMed]
- Marston, H.D.; Dixon, D.M.; Knisely, J.M.; Palmore, T.N.; Fauci, A.S. Antimicrobial resistance. JAMA 2016, 316, 1193–1204. [Google Scholar] [CrossRef] [Green Version]
- Guitor, A.K.; Wright, G.D. Antimicrobial Resistance and Respiratory Infections. Chest 2018, 154, 1202–1212. [Google Scholar] [CrossRef]
- Gajdács, M.; Urbán, E.; Stájer, A.; Baráth, Z. Antimicrobial Resistance in the Context of the Sustainable Development Goals: A Brief Review. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 71–82. [Google Scholar] [CrossRef]
- He, X.; Xie, M.; Li, S.; Ye, J.; Peng, Q.; Ma, Q.; Lu, X.; Zhong, B. Antimicrobial resistance in bacterial pathogens among hospitalized children with community acquired lower respiratory tract infections in Dongguan, China (2011–2016). BMC Infect. Dis. 2017, 17, 614. [Google Scholar] [CrossRef] [Green Version]
- Ramdhani, D.; Azizah, S.N.; Kusuma, S.A.F.; Sediana, D. Antibiotic resistance: Evaluation of levofloxacin treatment in acute res-piratory tract infections cases at the Tasikmalaya City Health Center, Indonesia. J. Adv. Pharm. Technol. Res. 2020, 11, 113–116. [Google Scholar] [CrossRef]
- Jehan, F.; Nisar, I.; Kerai, S.; Balouch, B.; Brown, N.; Rohman, N.; Rizvi, R.; Shafiq, Y.; Zaidi, A.K.M. Randomized Trial of Amoxicillin for Pneumonia in Pakistan. N. Engl. J. Med. 2020, 383, 24–34. [Google Scholar] [CrossRef]
- Steinman, M.A.; Ranji, S.R.; Shojania, K.G.; Gonzales, R. Improving antibiotic selection: A systematic review and quantitative analysis of quality improvement strategies. Med. Care 2006, 44, 617–628. [Google Scholar] [CrossRef]
- Bryant, J.; McDonald, V.M.; Boyes, A.; Sanson-Fisher, R.; Paul, C.; Melville, J. Improving medication adherence in chronic obstruc-tive pulmonary disease: A systematic review. Respir. Res. 2013, 14, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, L.M.; Cordina, M. Educational intervention to enhance adherence to short-term use of antibiotics. Res. Soc. Adm. Pharm. 2019, 15, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Kandeel, A.; Palms, D.L.; Afifi, S.; Kandeel, Y.; Etman, A.; Hicks, L.A.; Talaat, M. An educational intervention to promote appropriate antibiotic use for acute respiratory infections in a district in Egypt- pilot study. BMC Public Health 2019, 19, 498. [Google Scholar] [CrossRef]
- Khan, F.U.; Khan, F.U.; Hayat, K.; Chang, J.; Saeed, A.; Khan, Z.; Fang, Y. Knowledge, attitude and practices among consumers toward antibiotics use and antibiotic resistance in Swat, Khyber-Pakhtunkhwa, Pakistan. Expert Rev. Anti-Infect. Ther. 2020, 18, 937–946. [Google Scholar] [CrossRef]
- Rahman, A.; Khan, M.N.; Hamdani, S.U.; Chiumento, A.; Akhtar, P.; Nazir, H.; Nisar, A.; Masood, A.; Din, I.U.; Khan, N.A.; et al. Effectiveness of a brief group psychological intervention for women in a post-conflict setting in Pakistan: A single-blind, cluster, randomised controlled trial. Lancet 2019, 393, 1733–1744. [Google Scholar] [CrossRef]
- Rome, S. Crisis and reconciliation in Swat. Pak. A J. Pak. Stud. 2010, 3, 53–79. [Google Scholar]
- Khan, M.; Hamdani, S.; Chiumento, A.; Dawson, K.; Bryant, R.A.; Sijbrandij, M.; Nazir, H.; Akhtar, P.; Masood, A.; Wang, D.; et al. Evaluating feasibility and acceptability of a group WHO trans-diagnostic inter-vention for women with common mental disorders in rural Pakistan: A cluster randomised controlled feasibility trial. Epidemiol. Psychiatr. Sci. 2019, 28, 77–87. [Google Scholar] [CrossRef]
- Chotani, R.A. Crisis in the Swat Valley of Pakistan: Need for international action. Lancet 2009, 374, 23–24. [Google Scholar] [CrossRef]
- Atif, M.; Razzaq, W.; Mushtaq, I.; Malik, I.; Razzaq, M.; Scahill, S.; Babar, Z.U.D. Pharmacy Services beyond the Basics: A Qualitative Study to Explore Perspectives of Pharmacists towards Basic and Enhanced Pharmacy Services in Pakistan. Int. J. Environ. Res. Public Health 2020, 17, 2379. [Google Scholar] [CrossRef] [Green Version]
- Smart, G. Know When Antibiotics Work; US Centers for Disease Control and Prevention: Atlanta, GA, USA, 2013.
- Clifford, S.; Barber, N.; Elliott, R.A.; Hartley, E.; Horne, R. Patient-centred advice is effective in improving adherence to medicines. Pharm. World Sci. 2006, 28, 165–170. [Google Scholar] [CrossRef]
- Noordzij, M.; Tripepi, G.; Dekker, F.; Zoccali, C.; Tanck, M.; Jager, K.J. Sample size calculations: Basic principles and common pitfalls. Nephrol. Dial. Transplant. 2010, 25, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Weinman, J.; Hankins, M. The beliefs about medicines questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychol. Health 1999, 14, 1–24. [Google Scholar] [CrossRef]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Morisky, D.E.; Ang, A.; Krousel-Wood, M.; Ward, H.J. Predictive validity of a medication adherence measure in an outpatient setting. J. Clin. Hypertens. 2008, 10, 348–354. [Google Scholar] [CrossRef] [Green Version]
- Muntner, P.; Joyce, C.; Holt, E.; He, J.; Morisky, D.; Webber, L.S.; Krousel-Wood, M. Defining the Minimal Detectable Change in Scores on the Eight-Item Morisky Medication Adherence Scale. Ann. Pharmacother. 2011, 45, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Vik, S.A.; Maxwell, C.J.; Hogan, D.B. Measurement, Correlates, and Health Outcomes of Medication Adherence Among Seniors. Ann. Pharmacother. 2004, 38, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Atif, M.; Asghar, S.; Mushtaq, I.; Malik, I.; Amin, A.; Babar, Z.-U.-D.; Scahill, S. What drives inappropriate use of antibiotics? A mixed methods study from Bahawalpur, Pakistan. Infect. Drug Resist. 2019, 12, 687–699. [Google Scholar] [CrossRef] [Green Version]
- Chiumento, A.; Hamdani, S.U.; Khan, M.N. Evaluating effectiveness and cost-effectiveness of a group psychological in-tervention using cognitive behavioural strategies for women with common mental disorders in conflict-affected rural Paki-stan: Study protocol for a randomised controlled trial. Trials 2017, 18, 190. [Google Scholar] [CrossRef] [Green Version]
- Green, J.; Thorogood, N. Beginning Data Analysis. Qualitative Methods for Health Research, 3rd ed.; Sage: London, UK, 2014; pp. 209–217. [Google Scholar]
- Campbell, M.K.; Piaggio, G.; Elbourne, D.R.; Altman, D.G.; the CONSORT Group. Consort 2010 statement: Extension to cluster randomised trials. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef] [Green Version]
- Ali, I.; Ahmad, J.; Khan, A.U.; Khan, T.; Khan, J.; Ul-Haq, Z. Self-medication and non-adherence with antibiotics: The current situation in Pakistan. J. Pharm. Pract. Res. 2016, 46, 34–37. [Google Scholar] [CrossRef]
- Malik, U.R.; Chang, J.; Hashmi, F.; Atif, N.; Basir, H.; Hayat, K.; Khan, H.U.; Kabba, J.A.; Lambojon, K.; Fang, Y.; et al. A Simulated Client Exploration of Nonprescription Dispensing of Antibiotics at Drug-stores for Pediatric Acute Diarrhea and Upper Respiratory Infection in Lahore, Pakistan. Infect. Drug Resist. 2021, 14, 1129. [Google Scholar] [CrossRef]
- Khan, F.U.; Khan, F.U.; Hayat, K.; Ahmad, T.; Khan, A.; Chang, J.; Malik, U.R.; Khan, Z.; Lambojon, K.; Fang, Y. Knowledge, Attitude, and Practice on Antibiotics and Its Resistance: A Two-Phase Mixed-Methods Online Study among Pakistani Community Pharmacists to Promote Rational Antibiotic Use. Int. J. Environ. Res. Public Health 2021, 18, 1320. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.U.; Fang, Y.; Khan, Z.; Khan, F.U.; Malik, Z.I.; Ahmed, N.; Khan, A.H.; Rehman, A.U. Occurrence, associated risk factors, and treatment of surgical site infections in Pakistan. Eur. J. Inflamm. 2020, 18, 2058739220960547. [Google Scholar] [CrossRef]
- Khan, F.U.; Khan, Z.; Fang, Y. Need of Guidelines and Antimicrobial Stewardship in Pakistan for Perioperative Surgical Practices to Prevent Surgical Site Infections. J. Coll. Physicians Surg. Pak. JCPSP 2020, 30, 882–883. [Google Scholar] [PubMed]
- Khan, Z.; Ahmed, N.; Rehman, A.; Khan, F.U.; Saqlain, M.; Martins, M.A.P.; Rahman, H. Audit of pre-operative antibiotic prophylaxis usage in elective surgical procedures in two teaching hospitals, Islamabad, Pakistan: An observational cross-sectional study. PLoS ONE 2020, 15, e0231188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, F.U.; Khan, Z.; Ahmed, N.; Rehman, A. A General Overview of Incidence, Associated Risk Factors, and Treatment Outcomes of Surgical Site Infections. Indian J. Surg. 2020, 82, 449–459. [Google Scholar] [CrossRef]


{kind=link}
| Terms | Definition |
|---|---|
| AB (Acute Bronchitis) | A patient with no chronic lung disease, acute sickness, symptoms connected to or clinical evidence that accompanies cough, which may/may not be productive, with LRTI advised and no alternative explanation (i.e., asthma/sinusitis). |
| Suspected community-acquired pneumonia | Cough and fever for more than four days with at least one new symptom chest, or dyspnea, and no other obvious causes. |
| Definite community-acquired pneumonia | Same as the above, according to the outcomes of lung studies of chest radiographs, shadowing in the elderly, followed by acute clinical (unspecified) disease for no apparent reason. |
| Acute exacerbation of COPD | An occurrence in the course of the sickness characterized by the patient’s receding symptoms of cough, dyspnea, and sputum, as well as their day-to-day inconsistency, sufficient to allow for a change in treatment. |
| Acute exacerbation of bronchiectasis | A decline in the patient’s baseline dyspnea, sputum, and regular cough beyond inconsistency, sufficient to necessitate a change in care in a patient with bronchiectasis. |
| Influenza | Acute illness characterized by increased cough, body aches, headache, and sore throat, often accompanied by a fever. |
| STUDY PERIOD | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Enrollment | Allocation | Post Allocation | Close-Out Time | ||||||
| TIME POINT | T1 | W1 | W2 | W3 | W4 | W5 | W6 | W7 | |
| ENROLLMENT: | |||||||||
| Eligibility | |||||||||
| Consent | |||||||||
| Baseline Data | |||||||||
| Allocations | |||||||||
| INTERVENTIONS: | |||||||||
| leaflets |  | ||||||||
| Booklets | |||||||||
| WHO awareness | |||||||||
| Usual Care | |||||||||
| ASSESSMENT: | Outcomes analysis | ||||||||
| Baseline variables | x | x | x | x | x | x | x | x | |
| Therapy success rate | x | x | x | x | x | x | x | x | |
| Primary Outcomes | |||||||||
| Overall Adherence Secondary Outcomes | x | x | x | x | x | x | x | x | |
| Stakeholders | Allocation | Pharmacist-Led Interventions | Community Pharmacists | Outcome Assessment | Data Analysis |
|---|---|---|---|---|---|
| Trial Observer (PI) | a | a | a | a | a |
| Trial Participants | n/a | n/a | n/a | n/a | n/a |
| Duty Pharmacists | n/a | a | a | n/a | n/a |
| Data accumulators | n/a | n/a | n/a | n/a | n/a |
| Data analysts | n/a | n/a | n/a | n/a | a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, F.U.; Fang, Y. Effectiveness of Pharmacist-Led Brief Educational Intervention for Adherence to the Antibiotics for Lower Respiratory Tract Infections (EATSA) in Post-Conflict Rural Areas of Pakistan: Study Protocol for a Randomized Controlled Trial. Antibiotics 2021, 10, 1147. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101147
Khan FU, Fang Y. Effectiveness of Pharmacist-Led Brief Educational Intervention for Adherence to the Antibiotics for Lower Respiratory Tract Infections (EATSA) in Post-Conflict Rural Areas of Pakistan: Study Protocol for a Randomized Controlled Trial. Antibiotics. 2021; 10(10):1147. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101147
Chicago/Turabian StyleKhan, Faiz Ullah, and Yu Fang. 2021. "Effectiveness of Pharmacist-Led Brief Educational Intervention for Adherence to the Antibiotics for Lower Respiratory Tract Infections (EATSA) in Post-Conflict Rural Areas of Pakistan: Study Protocol for a Randomized Controlled Trial" Antibiotics 10, no. 10: 1147. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101147