
The Utility of Bedside Assessment Tools and Associated Factors to Avoid Antibiotic Overuse in an Urban PICU of a Diarrheal Disease Hospital in Bangladesh

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Participants
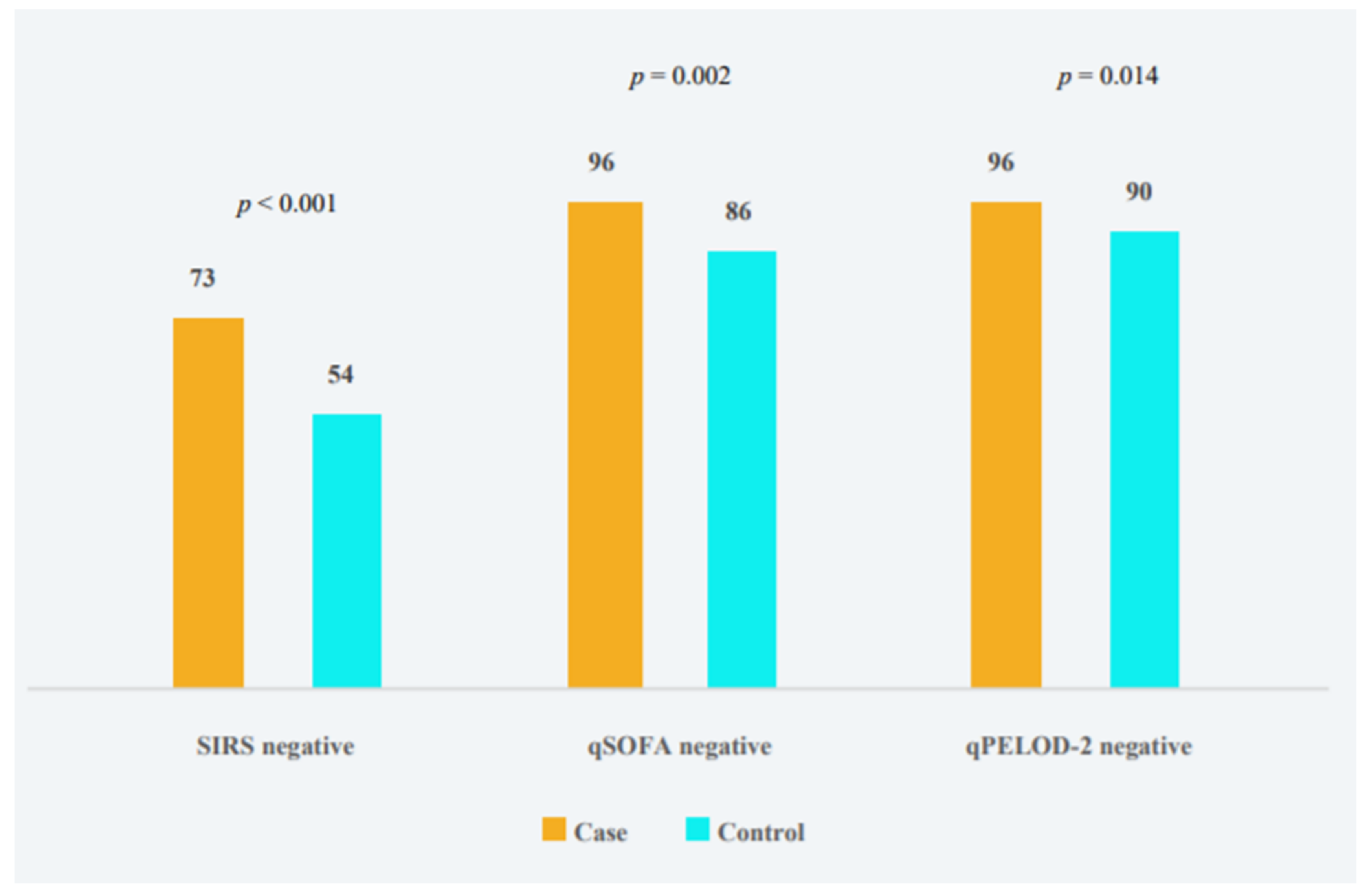
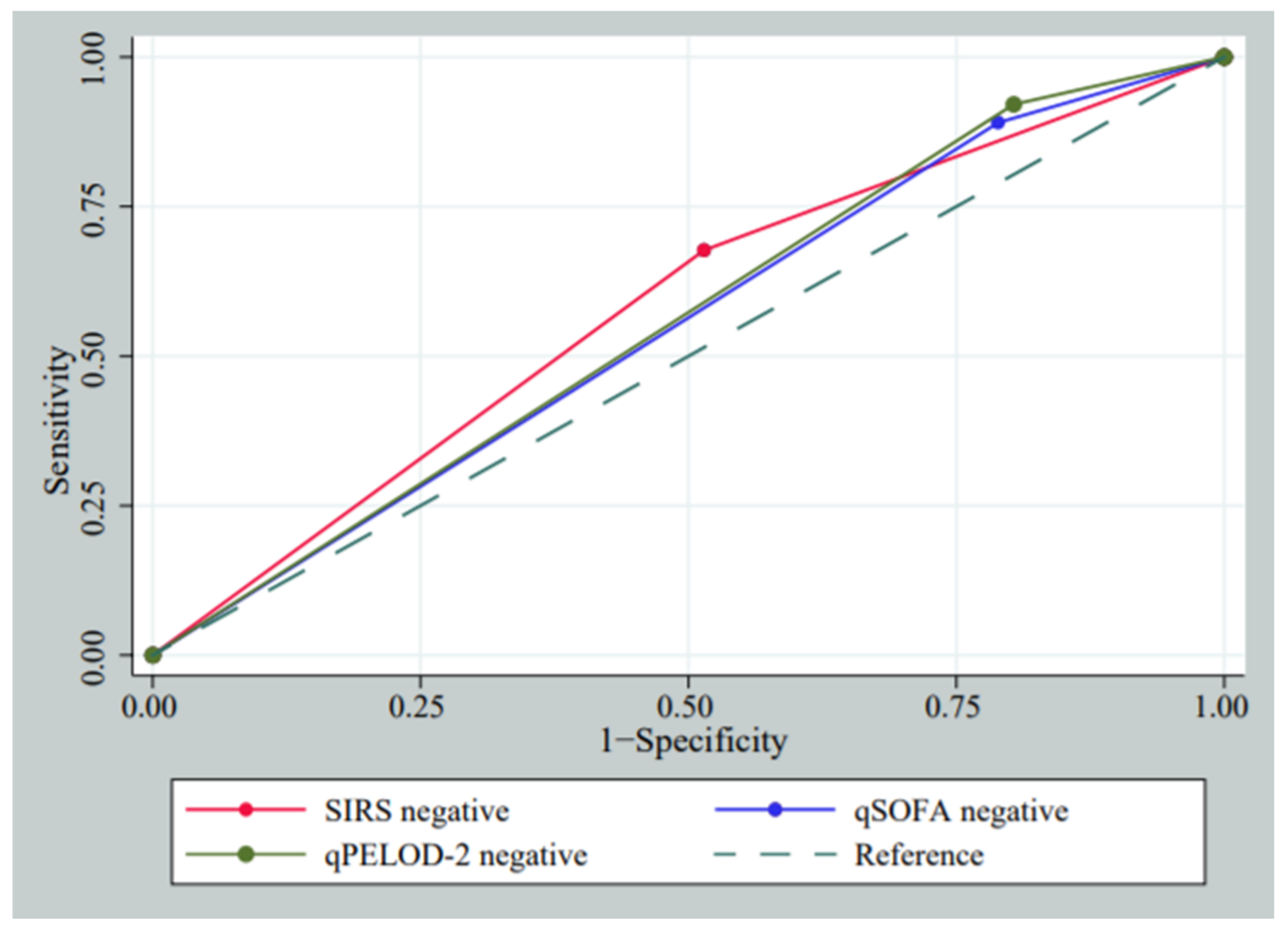
2.2. Utility of Bedside Assessment Tools to Prevent Antibiotic Overuse
2.3. Factors Associated with No Antibiotic Approach in PICU
3. Discussion
Limitation
4. Materials and Methods
4.1. Study Site
4.2. Study Population and Design
4.3. Measurement
4.4. Scoring Systems
4.5. Management
4.6. Definition
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Bus, L.; Gadeyne, B.; Steen, J.; Boelens, J.; Claeys, G.; Benoit, D.; De Waele, J.; Decruyenaere, J.; Depuydt, P. A complete and multifaceted overview of antibiotic use and infection diagnosis in the intensive care unit: Results from a prospective four-year registration. Crit. Care 2018, 22, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Blinova, E.; Lau, E.; Bitnun, A.; Cox, P.; Schwartz, S.; Atenafu, E.; Yau, Y.; Streitenberger, L.; Parshuram, C.S.; Marshall, J.; et al. Point prevalence survey of antimicrobial utilization in the cardiac and pediatric critical care unit. Pediatr. Crit. Care Med. 2013, 14, e280–e288. [Google Scholar] [CrossRef]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The surviving sepsis campaign bundle: 2018 update. Intensive Care Med. 2018, 44, 925–928. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Ceyhan, M.; Yildirim, I.; Ecevit, C.; Aydogan, A.; Ornek, A.; Salman, N.; Somer, A.; Hatipoğlu, N.; Camcioglu, Y.; Alhan, E. Inappropriate antimicrobial use in Turkish pediatric hospitals: A multicenter point prevalence survey. Int. J. Infect. Dis. 2010, 14, e55–e61. [Google Scholar] [CrossRef] [Green Version]
- Fontela, P.S.; Quach, C.; Karim, M.E.; Willson, D.F.; Gilfoyle, E.; McNally, J.D.; Gonzales, M.; Papenburg, J.; Reynolds, S.; Lacroix, J. Determinants of antibiotic tailoring in pediatric intensive care: A national survey. Pediatr. Crit. Care Med. 2017, 18, e395–e405. [Google Scholar] [CrossRef]
- Thu, T.A.; Rahman, M.; Coffin, S.; Harun-Or-Rashid, M.; Sakamoto, J.; Hung, N.V. Antibiotic use in Vietnamese hospitals: A multicenter point-prevalence study. Am. J. Infect. Control 2012, 40, 840–844. [Google Scholar] [CrossRef]
- Kociolek, L.; Patel, S.; Shulman, S.; Zheng, X.; Todd, K.; Gerding, D.N. Clinical and microbiologic assessment of cases of pediatric community-associated Clostridium difficile infection reveals opportunities for improved testing decisions. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- El-Nawawy, A.; Ashraf, G.A.; Antonios, M.A.; Meheissen, M.A.; El-Alfy, M.M. Incidence of multidrug-resistant organism among children admitted to pediatric intensive care unit in a developing country. Microb. Drug Resist. 2018, 24, 1198–1206. [Google Scholar] [CrossRef]
- Dubourg, G.; Raoult, D. Emerging methodologies for pathogen identification in positive blood culture testing. Expert Rev. Mol. Diagn. 2016, 16, 97–111. [Google Scholar] [CrossRef]
- Patel, R. New developments in clinical bacteriology laboratories. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2016; pp. 1448–1459. [Google Scholar]
- Giebel, R.; Worden, C.; Rust, S.; Kleinheinz, G.; Robbins, M.; Sandrin, T. Microbial fingerprinting using matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS): Applications and challenges. Adv. Appl. Microbiol. 2010, 71, 149–184. [Google Scholar]
- Rogers, B.B. The Evolution of the Polymerase Chain Reaction to Diagnose Childhood Infections. Pediatr. Dev. Pathol. 2015, 18, 495–503. [Google Scholar] [CrossRef]
- Goldstein, B.; Giroir, B.; Randolph, A.; International Consensus Conference on Pediatric Sepsis. International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr. Crit. Care Med. 2005, 6, 2–8. [Google Scholar] [CrossRef] [Green Version]
- Chisti, M.J.; Saha, S.; Roy, C.N.; Salam, M.A. Predictors of bacteremia in infants with diarrhea and systemic inflammatory response syndrome attending an urban diarrheal treatment center in a developing country. Pediatr. Crit. Care Med. 2010, 11, 92–97. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock. JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock. JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Leteurtre, S.; Duhamel, A.; Salleron, J.; Grandbastien, B.; Lacroix, J.; Leclerc, F.; Groupe Francophone de Reanimation et d’Urgences Pédiatriques (GFRUP). PELOD-2: An update of the PEdiatric logistic organ dysfunction score. Crit. Care Med. 2013, 41, 1761–1773. [Google Scholar] [CrossRef]
- Leclerc, F.; Duhamel, A.; Deken, V.; Grandbastien, B.; Leteurtre, S. Can the pediatric logistic organ dysfunction-2 score on day 1 be used in clinical criteria for sepsis in children? Pediatr. Crit. Care Med. 2017, 18, 758–763. [Google Scholar] [CrossRef] [Green Version]
- Paño-Pardo, J.R.; Schüffelmann-Gutiérrez, C.; Escosa-Garcia, L.; Laplaza-González, M.; Moreno-Ramos, F.; Gómez-Gil, R.; López, J.; Jordán, I.; Téllez, C.; de la Oliva, P. Opportunities to improve antimicrobial use in paediatric intensive care units: A nationwide survey in Spain. Clin. Microbiol. Infect. 2016, 22, 171–177. [Google Scholar] [CrossRef]
- Van Nassau, S.C.; van Beek, R.H.; Driessen, G.J.; Hazelzet, J.A.; van Wering, H.M.; Boeddha, N.P. Translating Sepsis-3 Criteria in Children: Prognostic Accuracy of Age-Adjusted Quick SOFA Score in Children Visiting the Emergency Department With Suspected Bacterial Infection. Front. Pediatr. 2018, 6, 266. [Google Scholar] [CrossRef]
- Goulden, R.; Hoyle, M.-C.; Monis, J.; Railton, D.; Riley, V.; Martin, P.; Martina, R.; Nsutebu, E. qSOFA, SIRS and NEWS for predicting inhospital mortality and ICU admission in emergency admissions treated as sepsis. Emerg. Med. J. 2018, 35, 345–349. [Google Scholar] [CrossRef]
- Rogawski, E.T.; Platts-Mills, J.A.; Seidman, J.C.; John, S.; Mahfuz, M.; Ulak, M.; Shrestha, S.K.; Soofi, S.B.; Yori, P.P.; Mduma, E. Use of antibiotics in children younger than two years in eight countries: A prospective cohort study. Bull. World Health Organ. 2017, 95, 49. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, P.; Borte, M.; Zimmer, K.P.; Huppertz, H.I. Complications in hospitalized children with acute gastroenteritis caused by rotavirus: A retrospective analysis. Eur. J. Pediatr. 2012, 171, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Forman, S.; Crofton, P.; Huang, H.; Marshall, T.; Fares, K.; McIntosh, N. The epidemiology of hypernatraemia in hospitalised children in Lothian: A 10-year study showing differences between dehydration, osmoregulatory dysfunction and salt poisoning. Arch. Dis. Child. 2012, 97, 502–507. [Google Scholar] [CrossRef]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Platts-Mills, J.A.; Babji, S.; Bodhidatta, L.; Gratz, J.; Haque, R.; Havt, A.; McCormick, B.J.; McGrath, M.; Olortegui, M.P.; Samie, A.; et al. Pathogen-specific burdens of community diarrhoea in developing countries: A multisite birth cohort study (MAL-ED). Lancet Glob. Health 2015, 3, e564–e575. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.C.M.; Berkley, J.A. Guidelines for the treatment of dysentery (shigellosis): A systematic review of the evidence. Paediatr. Int. Child Health 2018, 38, S50–S65. [Google Scholar] [CrossRef] [Green Version]
- Afroze, F.; Ahmed, T.; Sarmin, M.; Shahid, A.S.M.S.B.; Shahunja, K.; Shahrin, L.; Chisti, M.J. Risk factors and outcome of Shigella encephalopathy in Bangladeshi children. PLoS Negl. Trop. Dis. 2017, 11, e0005561. [Google Scholar] [CrossRef] [Green Version]
- WHO. Guideline: Updates on the Management of Severe Acute Malnutrition in Infants and Children; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Chisti, M.J.; Salam, M.A.; Ashraf, H.; Faruque, A.S.; Bardhan, P.K.; Hossain, M.I.; Shahid, A.S.; Shahunja, K.M.; Das, S.K.; Imran, G.; et al. Clinical risk factors of death from pneumonia in children with severe acute malnutrition in an urban critical care ward of Bangladesh. PLoS ONE 2013, 8, e73728. [Google Scholar] [CrossRef]
- Hooli, S.; Colbourn, T.; Lufesi, N.; Costello, A.; Nambiar, B.; Thammasitboon, S.; Makwenda, C.; Mwansambo, C.; McCollum, E.D.; King, C. Correction: Predicting Hospitalised Paediatric Pneumonia Mortality Risk: An External Validation of RISC and mRISC, and Local Tool Development (RISC-Malawi) from Malawi. PLoS ONE 2018, 13, e0193557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, C.M.; Olofin, I.; Flaxman, S.; Fawzi, W.W.; Spiegelman, D.; Caulfield, L.E.; Black, R.E.; Ezzati, M.; Danaei, G.; Nutrition Impact Model Study. The effect of multiple anthropometric deficits on child mortality: Meta-analysis of individual data in 10 prospective studies from developing countries. Am. J. Clin. Nutr. 2013, 97, 896–901. [Google Scholar] [CrossRef] [Green Version]
- WHO. Revised WHO Classification and Treatment of Pneumonia in Children at Health Facilities: Evidence Summaries; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Chisti, M.J.; Ahmed, T.; Ashraf, H.; Faruque, A.S.; Bardhan, P.K.; Dey, S.K.; Huq, S.; Das, S.K.; Salam, M.A. Clinical predictors and outcome of metabolic acidosis in under-five children admitted to an urban hospital in Bangladesh with diarrhea and pneumonia. PLoS ONE 2012, 7, e39164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modi, P.; Munyaneza, R.B.M.; Goldberg, E.; Choy, G.; Shailam, R.; Sagar, P.; Westra, S.J.; Nyakubyara, S.; Gakwerere, M.; Wolfman, V. Oxygen saturation can predict pediatric pneumonia in a resource-limited setting. J. Emerg. Med. 2013, 45, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Chisti, M.J.; Salam, M.A.; Bardhan, P.K.; Faruque, A.S.; Shahid, A.S.; Shahunja, K.; Das, S.K.; Hossain, M.I.; Ahmed, T. Severe sepsis in severely malnourished young Bangladeshi children with pneumonia: A retrospective case control study. PLoS ONE 2015, 10, e0139966. [Google Scholar] [CrossRef]
- Haghbin, S.; Serati, Z.; Sheibani, N.; Haghbin, H.; Karamifar, H. Correlation of hypocalcemia with serum parathyroid hormone and calcitonin levels in pediatric intensive care unit. Indian J. Pediatr. 2015, 82, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Shin, S.M.; Jeong, M.; Cho, D.H.; Lee, K.H.; Eisenhut, M.; Kronbichler, A.; Moritz, M.; Il Shin, J. Hyponatremia in children with respiratory infections: A cross-sectional analysis of a cohort of 3938 patients. Sci. Rep. 2018, 8, 16494. [Google Scholar] [CrossRef] [PubMed]
- Naveed-ur-Rehman Siddiqui, Z.A.; Jurair, H.; Haque, A. Mortality patterns among critically ill children in a Pediatric Intensive Care Unit of a developing country. Indian J. Crit. Care Med. Peer-Rev. Off. Publ. Indian Soc. Crit. Care Med. 2015, 19, 147. [Google Scholar]
- Punchak, M.; Hall, K.; Seni, A.; Buck, W.C.; DeUgarte, D.A.; Hartford, E.; Kelly, R.B.; Muando, V.I. Epidemiology of Disease and Mortality From a PICU in Mozambique. Pediatr. Crit. Care Med. 2018, 19, e603–e610. [Google Scholar] [CrossRef] [PubMed]
- Chisti, M.J.; Pietroni, M.A.; Smith, J.H.; Bardhan, P.K.; Salam, M.A. Predictors of death in under-five children with diarrhoea admitted to a critical care ward in an urban hospital in Bangladesh. Acta Paediatr. 2011, 100, e275–e279. [Google Scholar] [CrossRef] [PubMed]
- Chisti, M.J.; Salam, M.A.; Smith, J.H.; Ahmed, T.; Pietroni, M.A.; Shahunja, K.M.; Shahid, A.S.; Faruque, A.S.; Ashraf, H.; Bardhan, P.K.; et al. Bubble continuous positive airway pressure for children with severe pneumonia and hypoxaemia in Bangladesh: An open, randomised controlled trial. Lancet 2015, 386, 1057–1065. [Google Scholar] [CrossRef]
- Efunshile, A.M.; Ezeanosike, O.; Nwangwu, C.C.; Konig, B.; Jokelainen, P.; Robertson, L.J. Apparent overuse of antibiotics in the management of watery diarrhoea in children in Abakaliki, Nigeria. BMC Infect. Dis. 2019, 19, 275. [Google Scholar] [CrossRef]
- Schlapbach, L.J.; Straney, L.; Bellomo, R.; MacLaren, G.; Pilcher, D. Prognostic accuracy of age-adapted SOFA, SIRS, PELOD-2, and qSOFA for in-hospital mortality among children with suspected infection admitted to the intensive care unit. Intensive Care Med. 2018, 44, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarmin, M.; Ahmed, T.; Bardhan, P.K.; Chisti, M.J. Specialist hospital study shows that septic shock and drowsiness predict mortality in children under five with diarrhoea. Acta Paediatr. 2014, 103, e306–e311. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Chisti, M.J.; Graham, S.M.; Duke, T.; Ahmed, T.; Ashraf, H.; Faruque, A.S.; La Vincente, S.; Banu, S.; Raqib, R.; Salam, M.A. A prospective study of the prevalence of tuberculosis and bacteraemia in Bangladeshi children with severe malnutrition and pneumonia including an evaluation of Xpert MTB/RIF assay. PLoS ONE 2014, 9, e93776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Children without Antibiotic (n = 164) | Children with Antibiotic (n = 346) | OR | 95% CI | p-Value |
|---|---|---|---|---|---|
| Male | 104 (63) | 211 (61) | 1.11 | (0.75–1.63) | 0.598 |
| Age in months (median, IQR) | 10.1 (7.1, 14.0) | 8.1 (5.4, 12.3) | - | 0.002 | |
| Breast feed | 108 (65) | 218 (63) | 1.13 | (0.77, 1.67) | 0.532 |
| Immunized as per EPI schedule | 127 (77) | 261 (75) | 1.12 | (0.72, 1.74) | 0.620 |
| SAM | 0 | 119 (23) | - | - | - |
| Severe stunting | 7 (4) | 86 (25) | 0.13 | (0.06, 0.30) | <0.001 |
| Severe under weight | 11 (7) * | 132 (38) | 0.12 | (0.06, 0.22) | <0.001 |
| Watery stool | 148 (90) | 287 (83) | 1.90 | (1.06, 3.42) | 0.030 |
| Duration of diarrhea | 152/164, 3.0 (2.0, 5.0) | 313/346, 3.0 (2.0, 5.0) | 0.193 | ||
| History of vomiting | 44 (27) | 66 (19) | 1.56 | (1.00, 2.41) | 0.048 |
| Dehydration | 39 (24) | 123 (36) | 0.56 | (0.37, 0.86) | 0.008 |
| Fever | 36 (22) | 97 (28) | 0.72 | (0.47, 1.12) | 0.149 |
| Age specific fast breathing | 53/157 (34) | 176/340 (52) | 0.47 | (0.32, 0.70) | <0.001 |
| Chest in-drawing | 4 (2) | 89 (26) | 0.07 | (0.03, 0.20) | <0.001 |
| Adventitious sound on lung auscultation | 1 (0.6) | 119 (34) | 0.01 | (0.00, 0.08) | |
| Hypoxemia | 2 (1) ** | 59 (17) | 0.06 | (0.01, 0.25) | <0.001 |
| Abdominal distension | 4 (2) | 42 (12) | 0.18 | (0.06, 0.51) | <0.001 |
| Seizure | 84 (51) | 106 (31) | 2.37 | (1.62, 3.48) | <0.001 |
| Altered mentation | 41 (25) | 145 (42) | 0.46 | (0.30, 0.70) | <0.001 |
| Development delay | 5 (3) | 38 (11) | 0.25 | (0.09, 0.66) | 0.003 |
| Congenital heart disease | 3 (2) | 23 (7) | 0.26 | (0.08, 0.88) | 0.021 |
| Death | 0 (0) | 8 (5.3) | 0.044 |
| Characteristics | Case (n = 164) | Control (n = 346) | OR | 95% CI | p-Value |
|---|---|---|---|---|---|
| Hypernatremia | 53 (32) | 66 (19) | 2.03 | (1.33, 3.09) | 0.001 |
| Hyponatremia | 14 (9) | 76 (22) | 0.33 | (0.18, 0.61) | <0.001 |
| Hypokalemia | 46 (28) | 128 (37) | 0.66 | (0.44, 0.99) | 0.047 |
| Hyperkalemia | 7 (4) | 44 (13) | 0.31 | (0.13, 0.69) | 0.003 |
| Acidosis | 92 (56) | 210 (61) | 0.83 | (0.57, 1.21) | 0.324 |
| Hypocalcemia | 36 (22) | 115 (33) | 0.56 | (0.37, 0.87) | 0.009 |
| Anemia | 87 (53) | 184 (53) | 0.99 | (0.68, 1.44) | 0.978 |
| Leukocytosis | 75/140 (54) | 203/318 (64) | 0.65 | (0.44, 0.98) | 0.038 |
| Microscopic evidence of invasive diarrhea | 8 (5) | 45 (13) | 0.34 | (0.16, 0.75) | 0.005 |
| Laboratory evidence of CNS infection | 0 | 9 (3) | - | 0.029 | |
| Bacteremia | 0 | 41 (12) | - | - | <0.001 |
| Bacterial isolates from stool culture | 3/17 (18) | 41/177 (23) | 0.71 | (0.19, 2.59) | 0.767 |
| * Scores | Sensitivity% (95% CI) | Specificity% (95% CI) | NPV% (95% CI) | PPV% (95% CI) | AUROC (95% CI) | Comparison to AUROC | p-Value |
|---|---|---|---|---|---|---|---|
| Negative SIRS | 72.1 −(64.8, 78.7) | 46.0 −(40.6, 51.4) | 76.8 −(70.5, 82.4) | 39.9 −(34.4, 45.5) | 0.59 −(0.55, 0.63) | Negative SIRS vs. qPELOD-2 | 0.023 |
| Negative qSOFA | 95.9 −(91.8, 98.3) | 17.1 −(13.2, 21.4) | 89.4 −(79.4, 95.6) | 36.5 −(32.1, 41.1) | 0.56 −(0.54, 0.59) | Negative SIRS vs. qSOFA | 0.262 |
| Negative qPELOD-2 | 95.9 −(91.8, 98.3) | 13.0 −(9.6, 17.0) | 86.5 −(74.2, 94.4) | 35.4 −(31.1, 39.9) | 0.54 −(0.52, 0.57) | Negative qSOFA vs. qPELOD-2 | 0.071 |
| Characteristics | OR | (95% CI) | p-Value |
|---|---|---|---|
| Male sex | 1.44 | (0.82, 2.54) | 0.202 |
| Age in months | 1.03 | (1.01, 1.07) | 0.024 |
| Hypernatremia | 2.64 | (1.31, 5.31) | 0.006 |
| Hyponatremia | 0.39 | (0.17, 0.86) | 0.021 |
| Hypocalcemia | 0.46 | (0.24, 0.89) | 0.018 |
| Hyperkalemia | 0.44 | (0.15, 1.25) | 0.122 |
| Acute watery diarrhea | 1.08 | (0.45, 2.61) | 0.856 |
| Dehydration | 0.75 | (0.39, 1.46) | 0.401 |
| Severe stunting | 0.62 | (0.19, 1.99) | 0.423 |
| Severe underweight | 0.23 | (0.08, 0.65) | 0.005 |
| Altered mentation | 0.43 | (0.23, 0.80) | 0.008 |
| History of vomiting | 1.86 | (0.96, 3.61) | 0.066 |
| Age specific fast breathing | 0.88 | (0.50, 1.55) | 0.653 |
| Lower chest wall in-drawing | 0.16 | (0.04, 0.61) | 0.008 |
| Adventitious sound on lung auscultation | 0.22 | (0.00, 0.17) | <0.001 |
| Abdominal distension | 0.18 | (0.05, 0.60) | 0.005 |
| Documented seizure | 1.50 | (0.85, 2.65) | 0.156 |
| Development delay | 0.32 | (0.09, 1.10) | 0.072 |
| Congenital heart disease | 0.39 | (0.03, 4.65) | 0.462 |
| Microscopic evidence of invasive diarrhea | 0.19 | (0.07, 0.48) | <0.001 |
| Leukocytosis | 0.94 | (0.53, 1.67) | 0.841 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afroze, F.; Faruk, M.T.; Kamal, M.; Kabir, F.; Sarmin, M.; Sharifuzzaman; Chakraborty, M.; Hossain, M.R.; Shikha, S.S.; Chowdhury, V.P.; et al. The Utility of Bedside Assessment Tools and Associated Factors to Avoid Antibiotic Overuse in an Urban PICU of a Diarrheal Disease Hospital in Bangladesh. Antibiotics 2021, 10, 1255. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101255
Afroze F, Faruk MT, Kamal M, Kabir F, Sarmin M, Sharifuzzaman, Chakraborty M, Hossain MR, Shikha SS, Chowdhury VP, et al. The Utility of Bedside Assessment Tools and Associated Factors to Avoid Antibiotic Overuse in an Urban PICU of a Diarrheal Disease Hospital in Bangladesh. Antibiotics. 2021; 10(10):1255. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101255
Chicago/Turabian StyleAfroze, Farzana, Md. Tanveer Faruk, Mehnaz Kamal, Farhad Kabir, Monira Sarmin, Sharifuzzaman, Mithun Chakraborty, Md. Rezaul Hossain, Shamima Sharmin Shikha, Visnu Pritom Chowdhury, and et al. 2021. "The Utility of Bedside Assessment Tools and Associated Factors to Avoid Antibiotic Overuse in an Urban PICU of a Diarrheal Disease Hospital in Bangladesh" Antibiotics 10, no. 10: 1255. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101255