
Impact of High-Dose Anti-Infective Agents on the Osteogenic Response of Mesenchymal Stem Cells


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. DAPI Cell Count
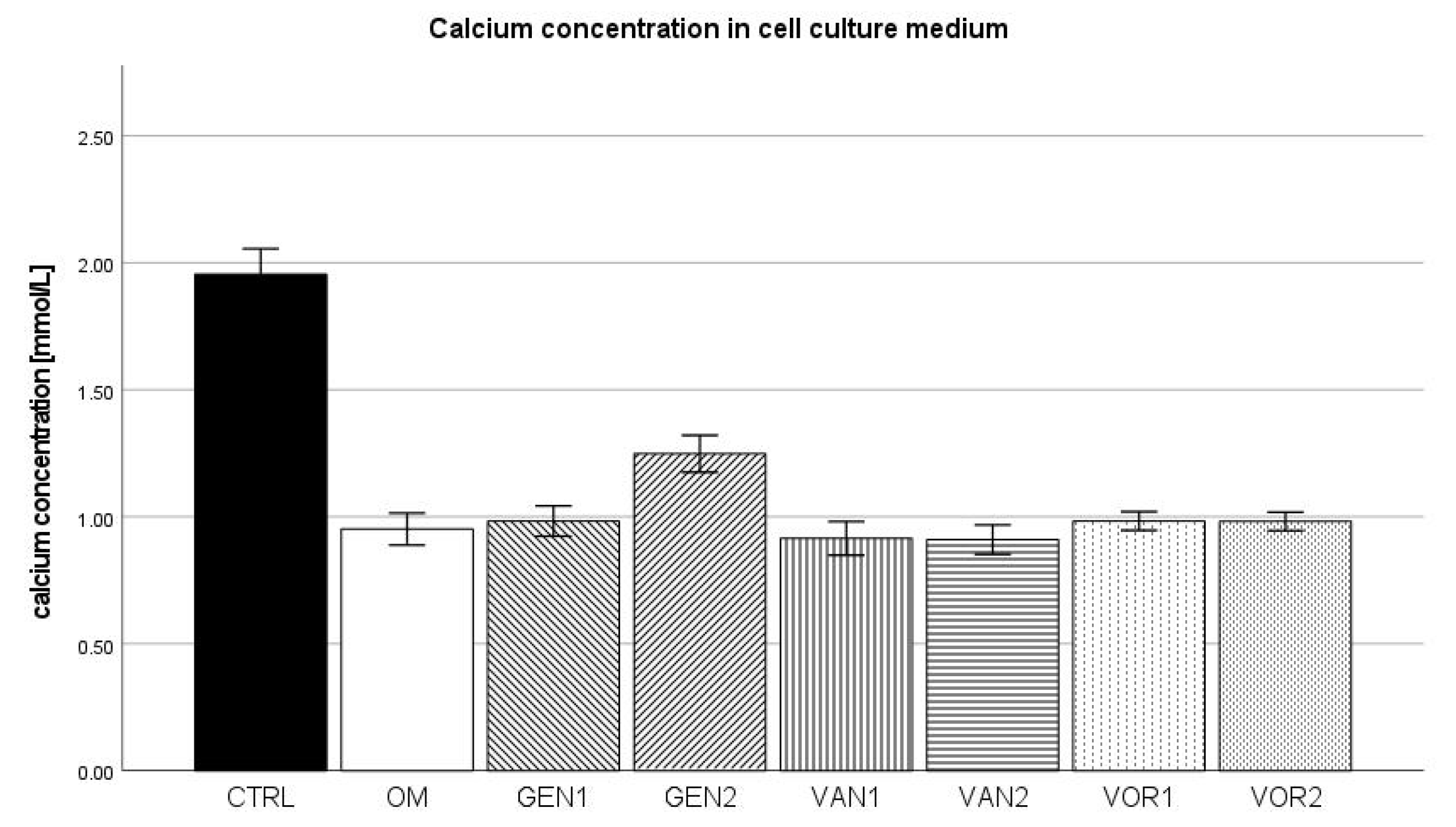
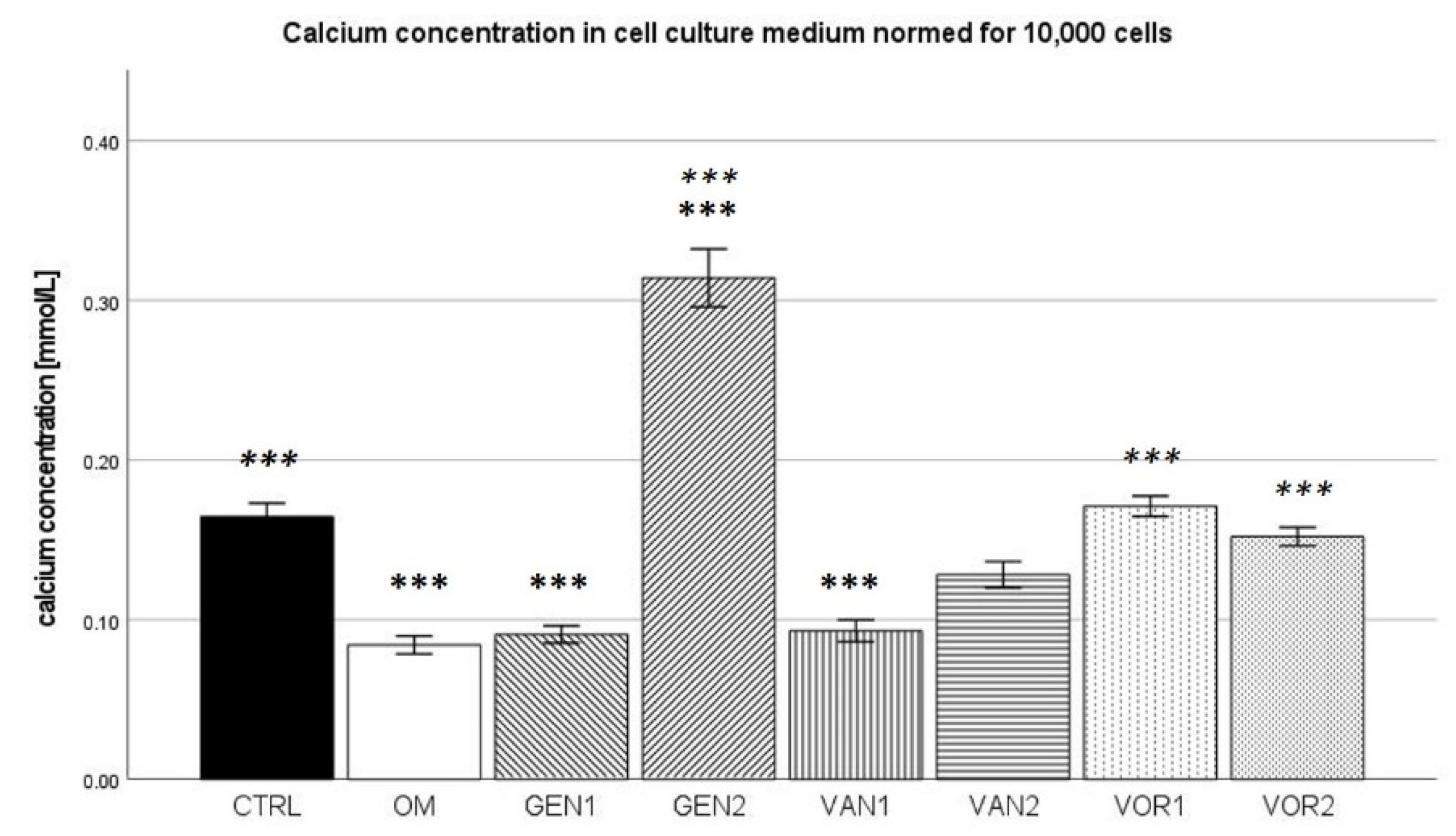
2.2. Calcium Concentration in Cell Culture Medium
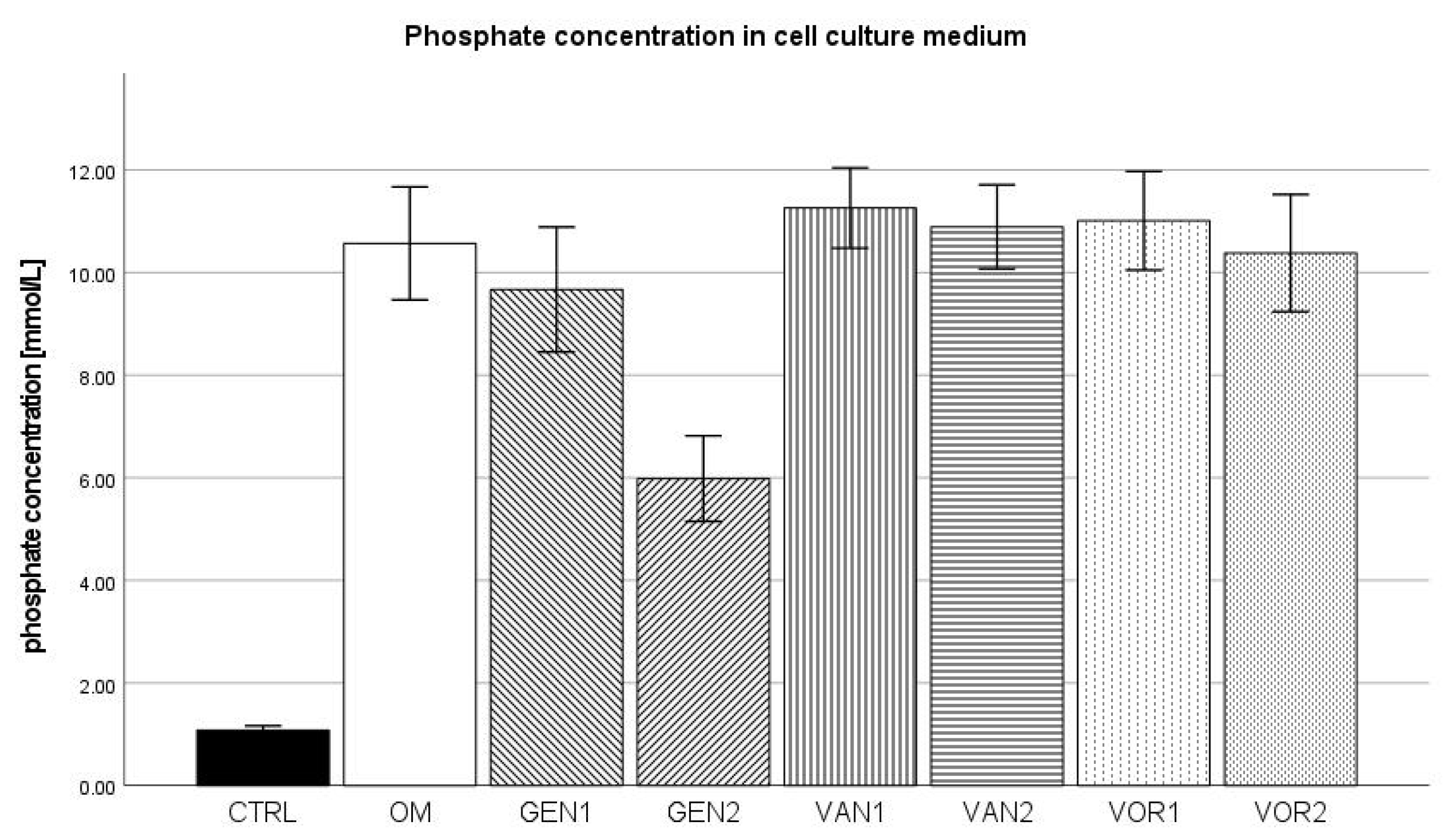
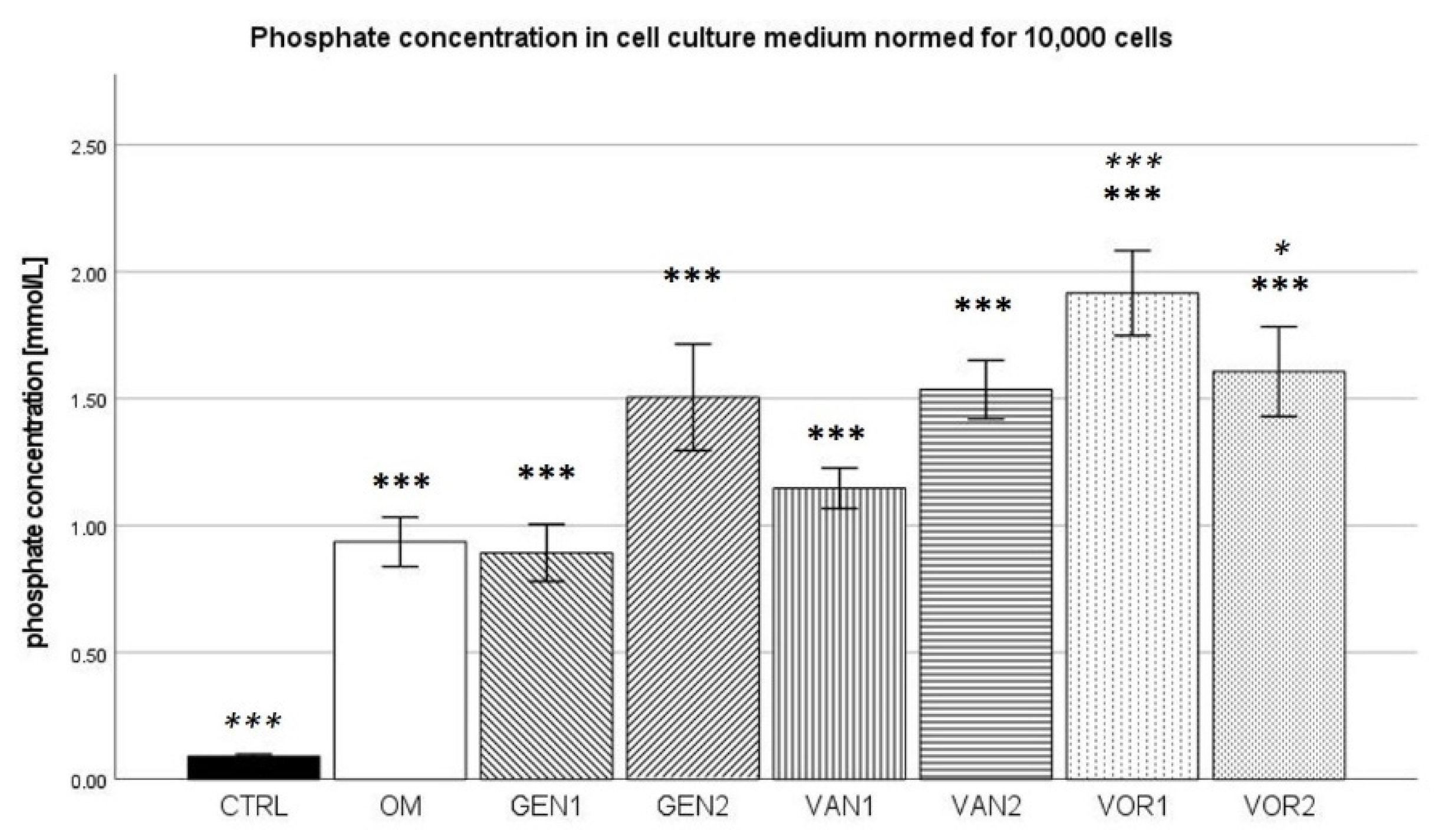
2.3. Phosphate Concentration in Cell Culture Medium
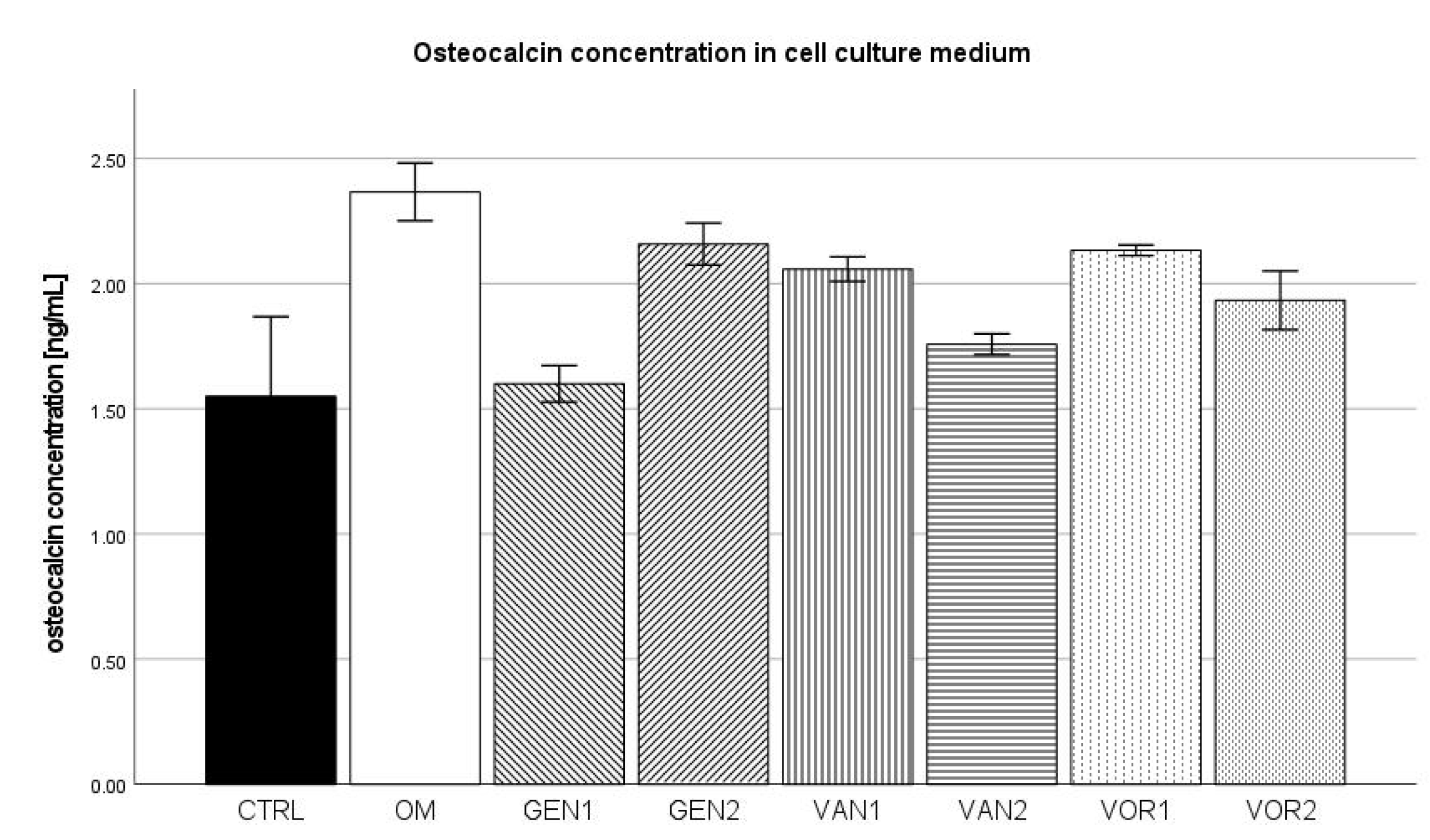
2.4. Osteocalcin Concentration in Cell Culture Medium
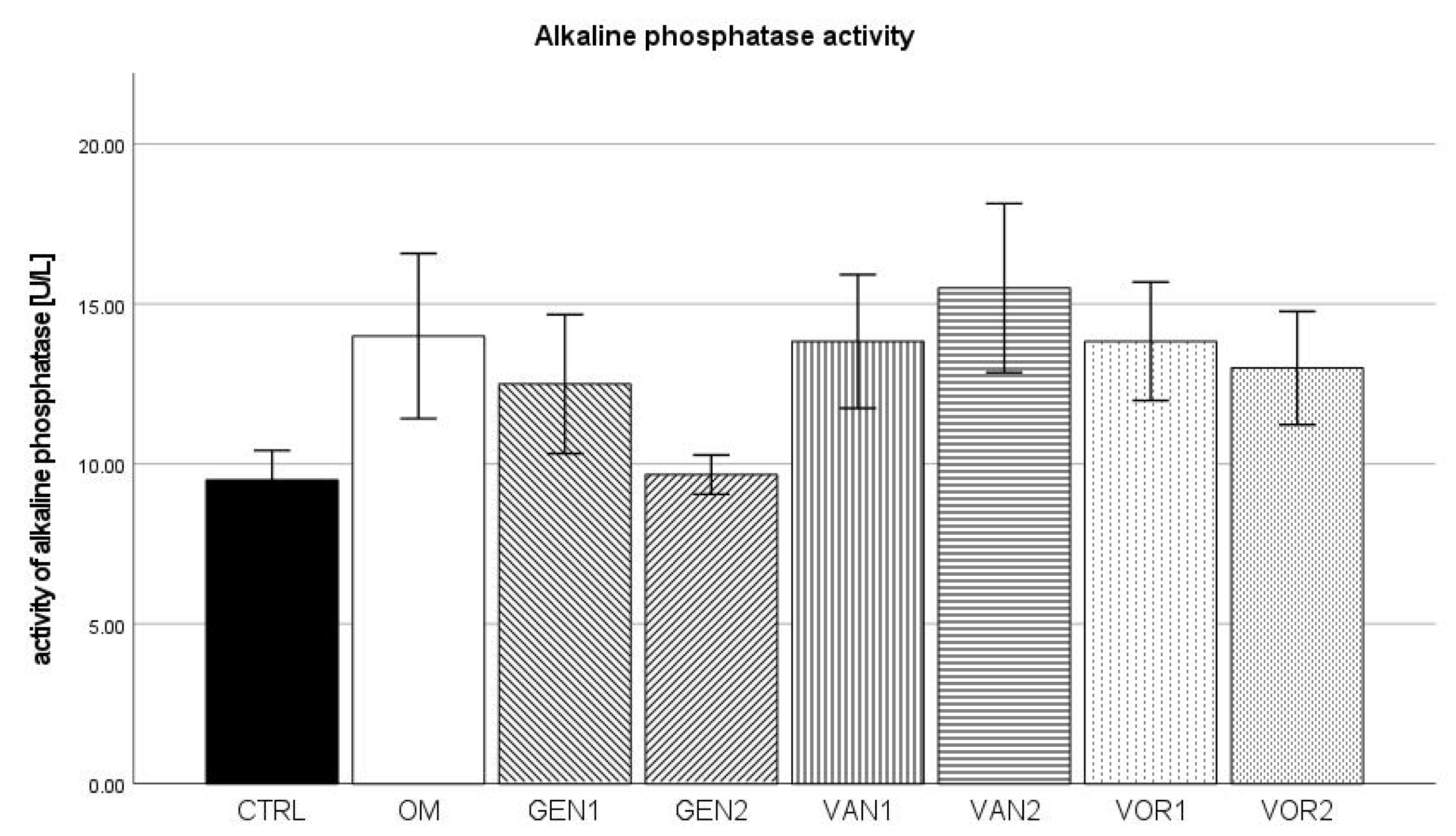
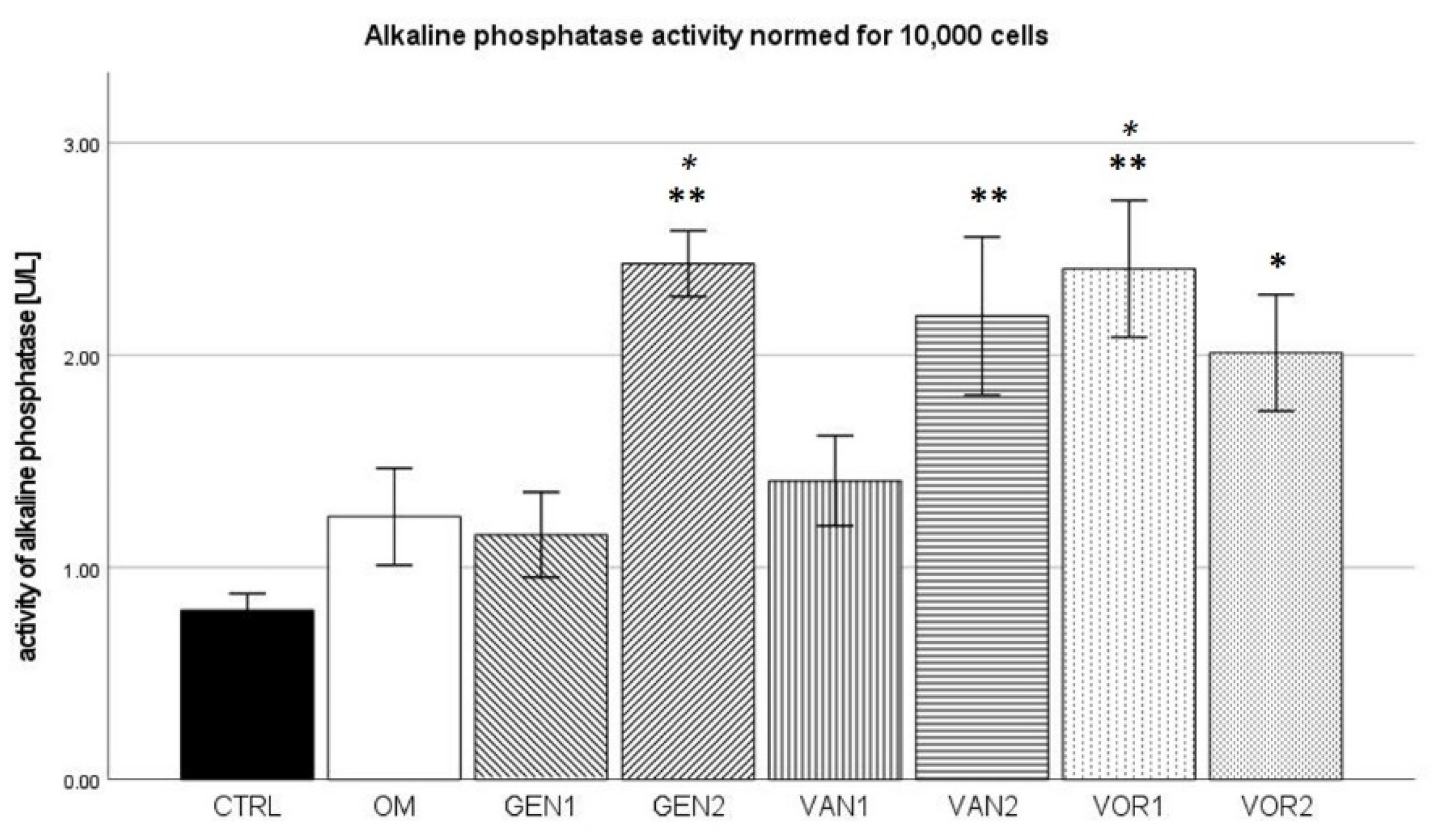
2.5. Alkaline Phosphatase Activity in Cell Culture Medium
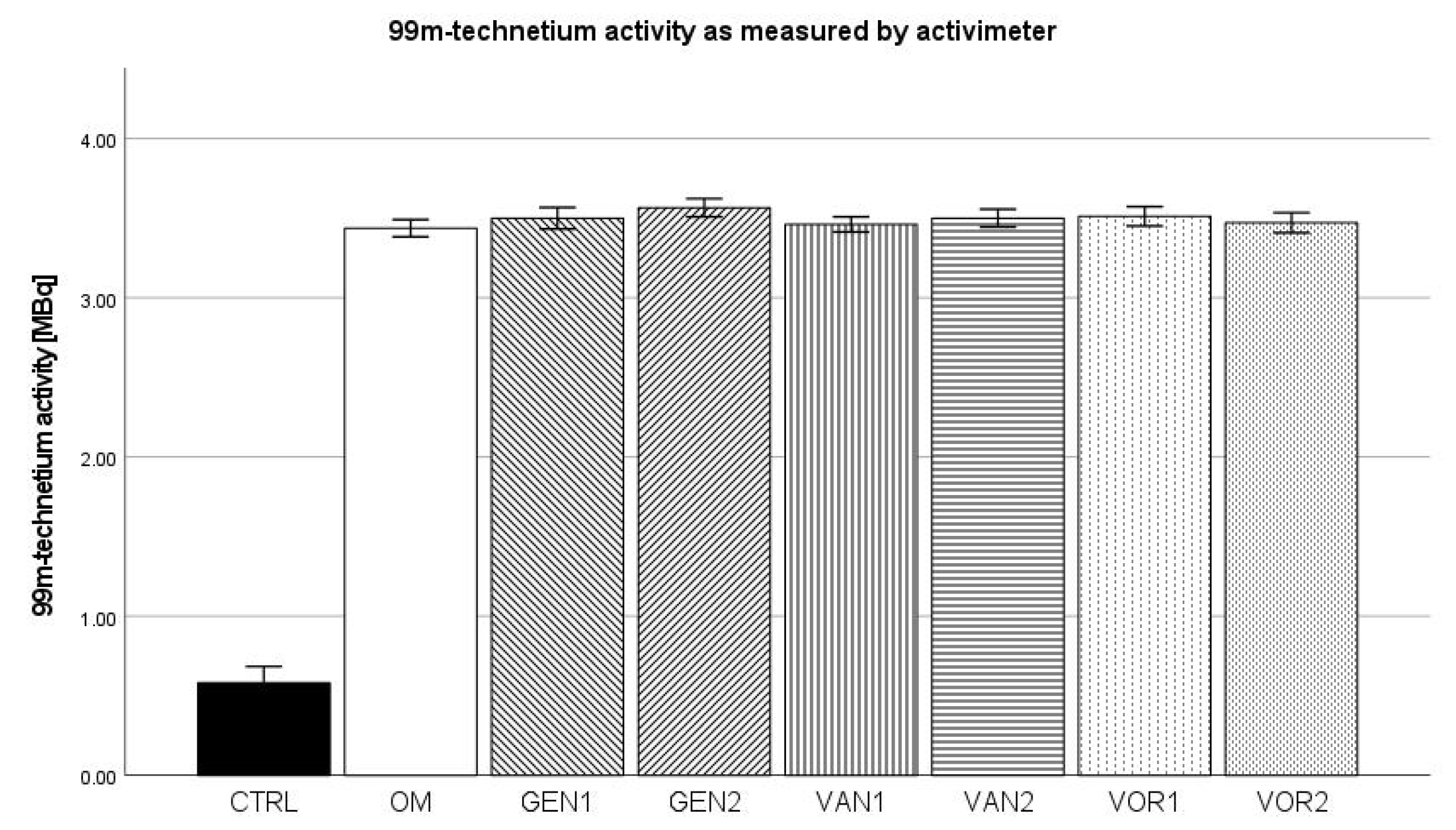
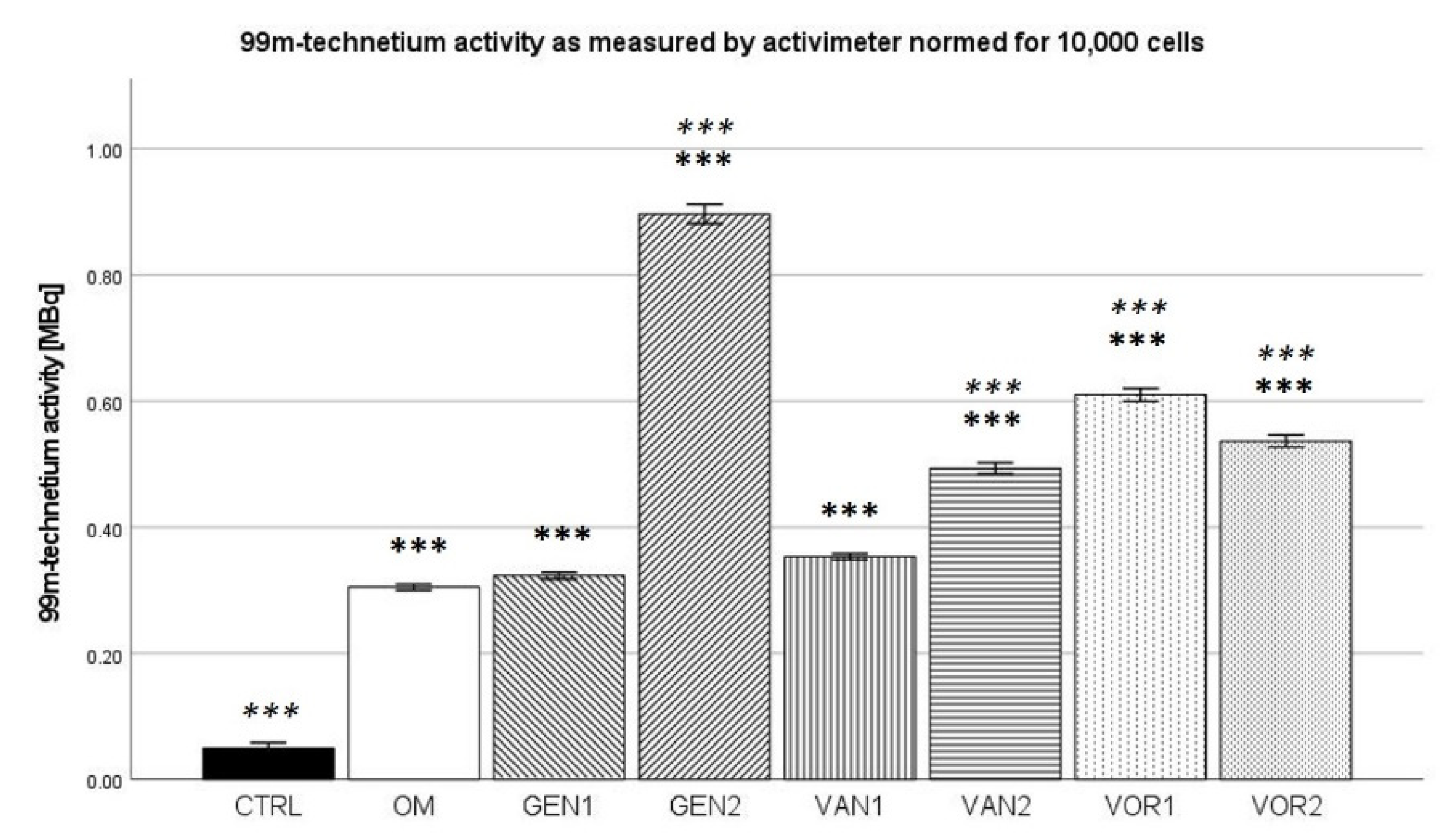
2.6. 99mTechnetium Labeling (Activimeter)
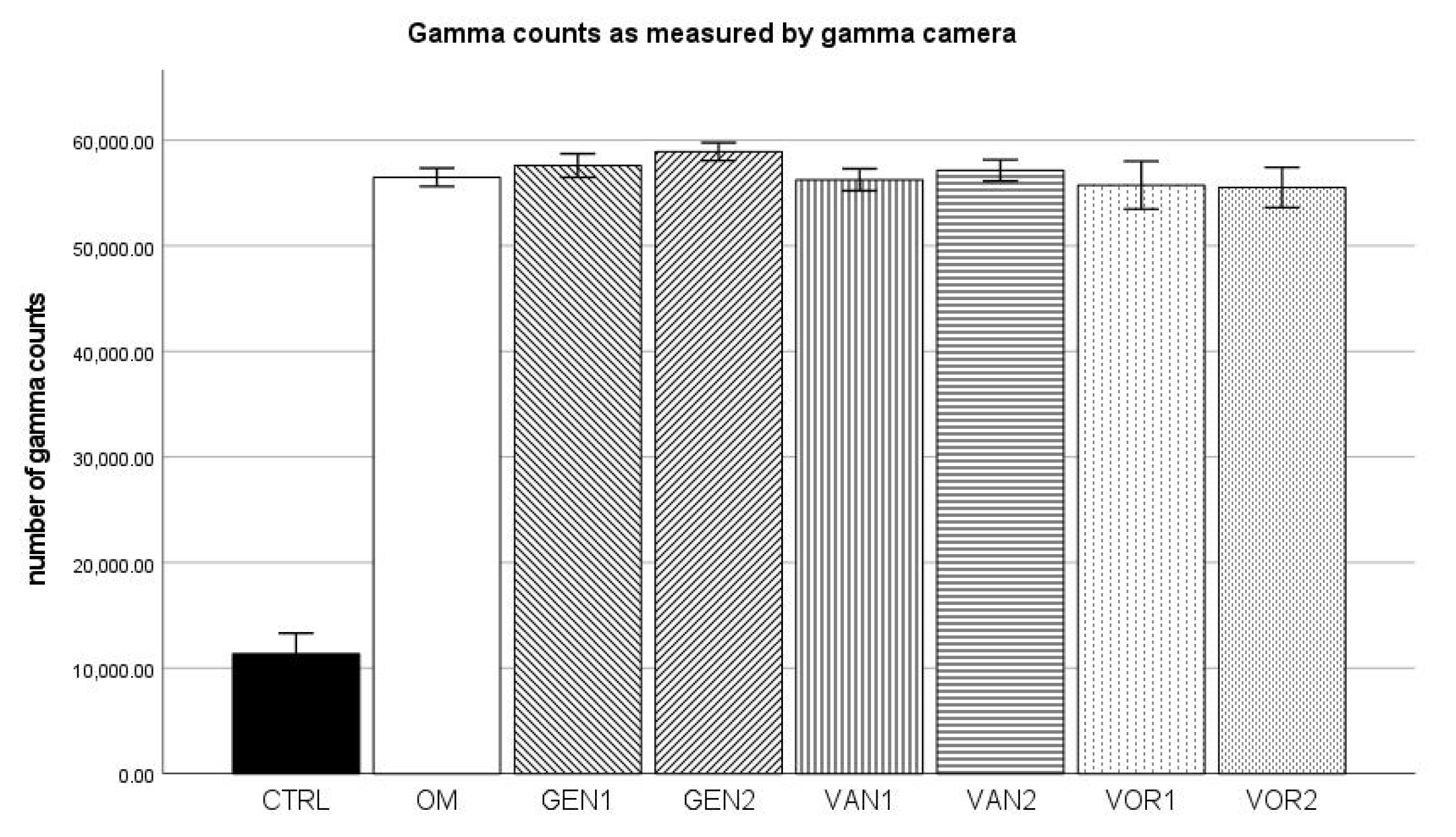
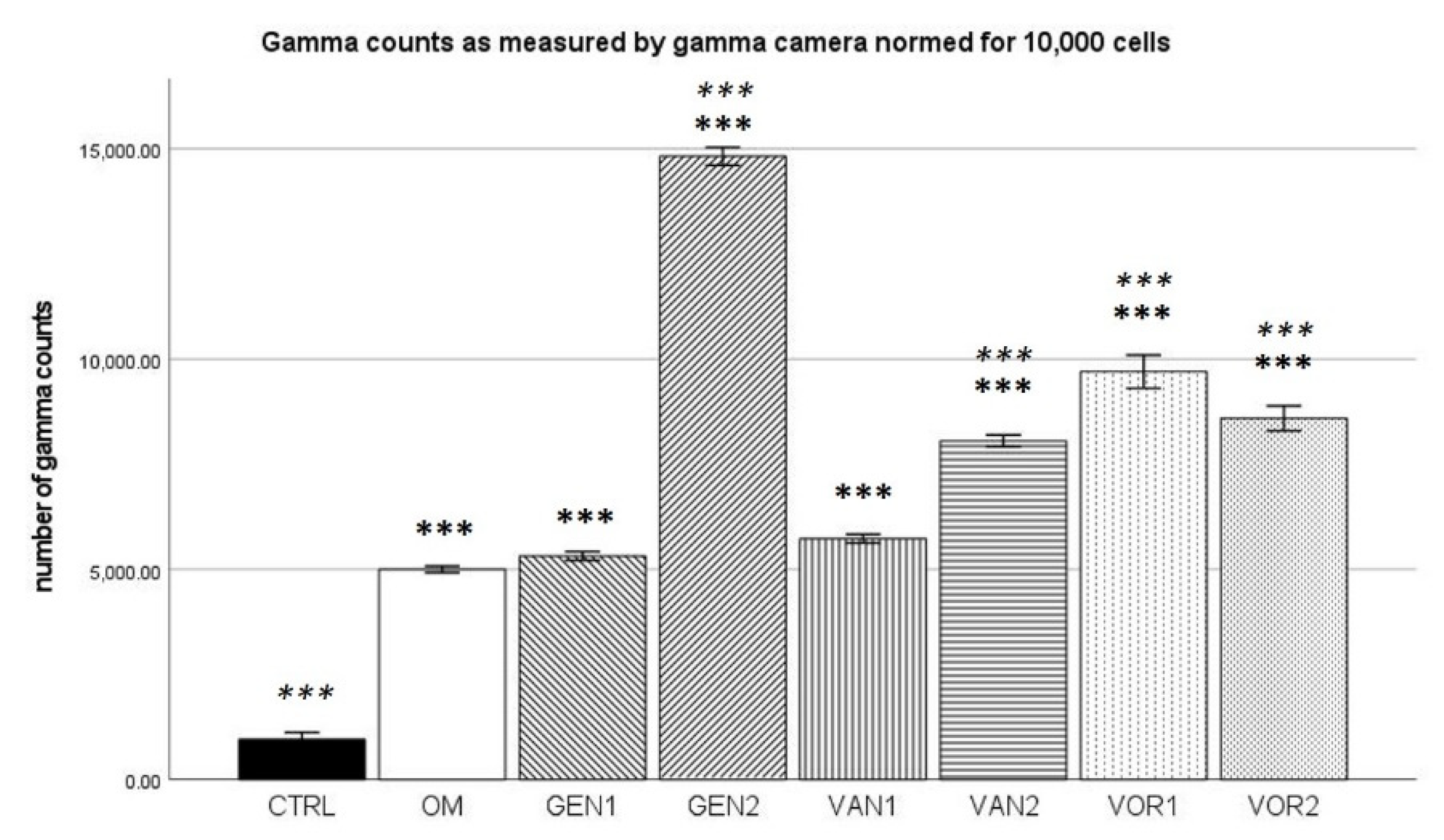
2.7. 99mTechnetium Labeling (Gamma Camera)
3. Discussion
4. Materials and Methods
4.1. Experimental Design at a Glance
4.2. Harvest of HMSC
4.3. HMSC Expansion
4.4. HMSC Differentiation
4.5. DAPI Cell Count
4.6. 99mTc-HDP Labeling and Analysis
4.7. Analyzation of Cell Culture Media
4.8. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Helbig, L.; Guehring, T.; Titze, N.; Nurjadi, D.; Sonntag, R.; Armbruster, J.; Wildemann, B.; Schmidmaier, G.; Gruetzner, A.P.; Freischmidt, H. A new sequential animal model for infection-related non-unions with segmental bone defect. BMC Musculoskelet. Disord. 2020, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Moghaddam, A.; Zimmermann, G.; Hammer, K.; Bruckner, T.; Grützner, P.A.; von Recum, J. Cigarette smoking influences the clinical and occupational outcome of patients with tibial shaft fractures. Injury 2011, 42, 1435–1442. [Google Scholar] [CrossRef]
- Patzakis, M.J.; Wilkins, J. Factors influencing infection rate in open fracture wounds. Clin. Orthop. Relat. Res. 1989, 243, 36–40. [Google Scholar] [CrossRef]
- Boxma, H.; Broekhuizen, T.; Patka, P.; Oosting, H. Randomised controlled trial of single-dose antibiotic prophylaxis in surgical treatment of closed fractures: The Dutch Trauma Trial. Lancet 1996, 347, 1133–1137. [Google Scholar] [CrossRef]
- Heppert, V.; Wentzensen, A. [Treatment of soft tissue damage--definitive management]. Langenbecks Arch. fur Chir. Suppl. Kongressband. Dtsch. Ges. fur Chir. Kongr. 1998, 115, 964–967. [Google Scholar]
- Schmidt, H.G.; Wittek, F.; Fink, B.; Buck-Gramcko, U. [Treatment of chronic osteitis of the tibia]. Der Unfallchirurg 1992, 95, 566–573. [Google Scholar] [PubMed]
- Oezel, L.; Büren, C.; Scholz, A.O.; Windolf, J.; Windolf, C.D. Effect of antibiotic infused calcium sulfate/hydroxyapatite (CAS/HA) insets on implant-associated osteitis in a femur fracture model in mice. PLoS ONE 2019, 14, e0213590. [Google Scholar] [CrossRef]
- Moussa, F.W.; O Anglen, J.; Gehrke, J.C.; Christensen, G.; A Simpson, W. The significance of positive cultures from orthopedic fixation devices in the absence of clinical infection. Am. J. Orthop. (Belle Mead N. J.) 1997, 26, 617–620. [Google Scholar]
- Metsemakers, W.; Kuehl, R.; Moriarty, F.; Richards, R.; Verhofstad, M.; Borens, O.; Kates, S.; Morgenstern, M. Infection after fracture fixation: Current surgical and microbiological concepts. Injury 2018, 49, 511–522. [Google Scholar] [CrossRef] [Green Version]
- Siopack, J.S.; Jergesen, H.E. Total hip arthroplasty. West J. Med. 1995, 162, 243–249. [Google Scholar]
- Lentino, J.R. Prosthetic Joint Infections: Bane of Orthopedists, Challenge for Infectious Disease Specialists. Clin. Infect. Dis. 2003, 36, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Tande, A.J.; Patel, R. Prosthetic Joint Infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parvizi, J.; Aggarwal, V.; Rasouli, M.R. Periprosthetic joint infection: Current concept. Indian J. Orthop. 2013, 47, 10–17. [Google Scholar] [CrossRef]
- Trampuz, A.; Zimmerli, W. Diagnosis and treatment of infections associated with fracture-fixation devices. Injury 2006, 37 (Suppl. S2), S59–S66. [Google Scholar] [CrossRef]
- Gustilo, R.B.; Gruninger, R.P.; Davis, T. Classification of type III (severe) open fractures relative to treatment and results. Orthopedics 1987, 10, 1781–1788. [Google Scholar]
- Song, Z.; Borgwardt, L.; Høiby, N.; Wu, H.; Sørensen, T.S.; Borgwardt, A. Prosthesis infections after orthopedic joint replacement: The possible role of bacterial biofilms. Orthop. Rev. 2013, 5, 14–71. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Moreno, J.; Merino, V.; Nacher, A.; Rodrigo, J.L.; Climente, M.; Merino-Sanjuán, M. Antibiotic-loaded Bone Cement as Prophylaxis in Total Joint Replacement. Orthop. Surg. 2017, 9, 331–341. [Google Scholar] [CrossRef]
- Buchholz, H.; Elson, R.; Engelbrecht, E.; Lodenkamper, H.; Rottger, J.; Siegel, A. Management of deep infection of total hip replacement. J. Bone Jt. Surgery. Br. Vol. 1981, 63, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Anagnostakos, K.; Meyer, C. Antibiotic Elution from Hip and Knee Acrylic Bone Cement Spacers: A Systematic Review. BioMed. Res. Int. 2017, 2017, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Walenkamp, G. Gentamicin PMMA Beads and Other Local Antibiotic Carriers in Two-Stage Revision of Total Knee Infection: A Review. J. Chemother. 2001, 13, 66–72. [Google Scholar] [CrossRef]
- Isefuku, S.; Joyner, C.J.; Simpson, A.H.R.W. Gentamicin May Have an Adverse Effect on Osteogenesis. J. Orthop. Trauma 2003, 17, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Siljander, M.; Sobh, A.H.; Baker, K.; Baker, E.A.; Kaplan, L.M. Multidrug-Resistant Organisms in the Setting of Periprosthetic Joint Infection—Diagnosis, Prevention, and Treatment. J. Arthroplast. 2018, 33, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Pulido, L.; Ghanem, E.; Joshi, A.; Purtill, J.J.; Parvizi, J. Periprosthetic Joint Infection: The Incidence, Timing, and Predisposing Factors. Clin. Orthop. Relat. Res. 2008, 466, 1710–1715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirby, A.; Graham, R.; Williams, N.; Wootton, M.; Broughton, C.M.; Alanazi, M.; Anson, J.; Neal, T.J.; Parry, C.M. Staphylococcus aureus with reduced glycopeptide susceptibility in Liverpool, UK. J. Antimicrob. Chemother. 2010, 65, 721–724. [Google Scholar] [CrossRef] [Green Version]
- Aljutayli, A.; Marsot, A.; Nekka, F. An Update on Population Pharmacokinetic Analyses of Vancomycin, Part I: In Adults. Clin. Pharmacokinet. 2020, 59, 671–698. [Google Scholar] [CrossRef] [PubMed]
- Widmer, A.F.; Frei, R.; Rajacic, Z.; Zimmerli, W. Correlation between In Vivo and In Vitro Efficacy of Antimicrobial Agents against Foreign Body Infections. J. Infect. Dis. 1990, 162, 96–102. [Google Scholar] [CrossRef] [Green Version]
- Lotfipour, F.; Abdollahi, S.; Jelvehgari, M.; Valizadeh, H.; Hassan, M.; Milani, M. Study of Antimicrobial Effects of Vancomycin Loaded PLGA Nanoparticles Against Enterococcus Clinical Isolates. Drug Res. 2013, 64, 348–352. [Google Scholar] [CrossRef]
- Schmidt, K.; McLaren, A.; Pauken, C.; McLemore, R. Voriconazole Is Cytotoxic at Locally Delivered Concentrations: A Pilot Study. Clin. Orthop. Relat. Res. 2013, 471, 3165–3170. [Google Scholar] [CrossRef] [Green Version]
- Chandra, J.; Kuhn, D.M.; Mukherjee, P.K.; Hoyer, L.; McCormick, T.; Ghannoum, M.A. Biofilm Formation by the Fungal Pathogen Candida albicans: Development, Architecture, and Drug Resistance. J. Bacteriol. 2001, 183, 5385–5394. [Google Scholar] [CrossRef] [Green Version]
- Bink, A. Anti-Biofilm Strategies: How to Eradicate Candida Biofilms? Open Mycol. J. 2011, 5, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Marra, F.; Robbins, G.M.; Masri, B.; Duncan, C.; Wasan, K.M.; Kwong, E.H.; Jewesson, P.J. Amphotericin B-loaded bone cement to treat osteomyelitis caused by Candida albicans. Can. J. Surg. 2001, 44, 383–386. [Google Scholar] [PubMed]
- Allen, K.C.; Sanchez, C.J., Jr.; Niece, K.L.; Wenke, J.C.; Akers, K.S. Voriconazole Enhances the Osteogenic Activity of Human OsteoblastsIn Vitrothrough a Fluoride-Independent Mechanism. Antimicrob. Agents Chemother. 2015, 59, 7205–7213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossner, T.; Helbig, L.; Schmidmaier, G.; Haberkorn, U.; Gotterbarm, T. 99mTc-polyphosphonate labelling—Enhancement of a novel method for the quantification of osteogenic differentiation of MSCs in vitro. Injury 2020. [Google Scholar] [CrossRef]
- Rathbone, C.R.; Cross, J.D.; Brown, K.V.; Murray, C.K.; Wenke, J.C. Effect of various concentrations of antibiotics on osteogenic cell viability and activity. J. Orthop. Res. 2011, 29, 1070–1074. [Google Scholar] [CrossRef]
- Antoci, V., Jr.; Adams, C.S.; Hickok, N.J.; Shapiro, I.M.; Parvizi, J. Antibiotics for Local Delivery Systems Cause Skeletal Cell Toxicity In Vitro. Clin. Orthop. Relat. Res. 2007, 462, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.T.; Chandrasekar, P.H. Adverse effects of voriconazole: Over a decade of use. Clin. Transplant. 2016, 30, 1377–1386. [Google Scholar] [CrossRef]
- Jiang, N.; Guo, F.; Sun, B.; Zhang, X.; Xu, H. Different Effects of Fluoride Exposure on the Three Major Bone Cell Types. Biol. Trace Element Res. 2019, 193, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Luong, M.-L.; Al-Dabbagh, M.; Groll, A.H.; Racil, Z.; Nannya, Y.; Mitsani, D.; Husain, S. Utility of voriconazole therapeutic drug monitoring: A meta-analysis. J. Antimicrob. Chemother. 2016, 71, 1786–1799. [Google Scholar] [CrossRef]
- Deelstra, J.J.; Neut, D.; Jutte, P.C. Successful Treatment of Candida Albicans–Infected Total Hip Prosthesis With Staged Procedure Using an Antifungal-Loaded Cement Spacer. J. Arthroplast. 2013, 28, 374.e5–374.e8. [Google Scholar] [CrossRef] [Green Version]
- Tanikake, Y.; Akahane, M.; Furukawa, A.; Tohma, Y.; Inagaki, Y.; Kira, T.; Tanaka, Y. Calcium Concentration in Culture Medium as a Nondestructive and Rapid Marker of Osteogenesis. Cell Transplant. 2017, 26, 1067–1076. [Google Scholar] [CrossRef] [Green Version]
- Akahane, M.; Dohi, Y.; Imamura, T.; Ueha, T.; Shimizu, T.; Tohma, Y.; Kido, A.; Tanaka, Y.; Kawate, K. Secretory osteocalcin as a nondestructive osteogenic marker of tissue-engineered bone. J. Orthop. Sci. 2011, 16, 622–628. [Google Scholar] [CrossRef]
- Tobiume, H.; Kanzaki, S.; Hida, S.; Ono, T.; Moriwake, T.; Yamauchi, S.; Tanaka, H.; Seino, Y. Serum Bone Alkaline Phosphatase Isoenzyme Levels in Normal Children and Children with Growth Hormone (GH) Deficiency: A Potential Marker for Bone Formation and Response to GH Therapy 1. J. Clin. Endocrinol. Metab. 1997, 82, 2056–2061. [Google Scholar] [CrossRef] [Green Version]
- Rao, M.; Pang, X.; Yang, J. Tobramycin promotes fracture healing by accelerating osteogenesis differentiation of MSCs through activating Wnt/β-catenin pathway. Minerva Medica. 2020, 111, 189–192. [Google Scholar] [CrossRef]
- Booysen, E.; Gijsen, H.S.-V.; Deane, S.M.; Ferris, W.; Dicks, L.M.T. The Effect of Vancomycin on the Viability and Osteogenic Potential of Bone-Derived Mesenchymal Stem Cells. Probiotics Antimicrob. Proteins 2018, 11, 1009–1014. [Google Scholar] [CrossRef]
- Eder, C.; Schenk, S.; Trifinopoulos, J.; Külekci, B.; Kienzl, M.; Schildböck, S.; Ogon, M. Does intrawound application of vancomycin influence bone healing in spinal surgery? Eur. Spine J. 2015, 25, 1021–1028. [Google Scholar] [CrossRef]
- Lee, G.-H.; Hwang, J.-D.; Choi, J.-Y.; Park, H.-J.; Cho, J.-Y.; Kim, K.-W.; Chae, H.-J.; Kim, H.-R. An acidic pH environment increases cell death and pro-inflammatory cytokine release in osteoblasts: The involvement of BAX Inhibitor-1. Int. J. Biochem. Cell Biol. 2011, 43, 1305–1317. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.H.; Bae, Y.C.; Jung, J.S. Role of Toll-Like Receptors on Human Adipose-Derived Stromal Cells. STEM CELLS 2006, 24, 2744–2752. [Google Scholar] [CrossRef]
- Fiedler, T.; Salamon, A.; Adam, S.; Herzmann, N.; Taubenheim, J.; Peters, K. Impact of bacteria and bacterial components on osteogenic and adipogenic differentiation of adipose-derived mesenchymal stem cells. Exp. Cell Res. 2013, 319, 2883–2892. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, S.; James, A.W.; Blough, J.; Donneys, A.; Wang, S.C.; Cederna, P.S.; Buchman, S.R.; Levi, B. Reconciling the effects of inflammatory cytokines on mesenchymal cell osteogenic differentiation. J. Surg. Res. 2013, 185, 278–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barza, M.; Lauermann, M.; Barza, M. Why Monitor Serum Levels of Gentamicin? Clin. Pharmacokinet. 1978, 3, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Álvarez, R.; Cortés, L.E.L.; Molina, J.; Cisneros, J.M.; Pachón, J. Optimizing the Clinical Use of Vancomycin. Antimicrob. Agents Chemother. 2016, 60, 2601–2609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colding-Rasmussen, T.; Horstmann, P.; Petersen, M.M.; Hettwer, W. Antibiotic Elution Characteristics and Pharmacokinetics of Gentamicin and Vancomycin from a Mineral Antibiotic Carrier: An in vivo Evaluation of 32 Clinical Cases. J. Bone Jt. Infect. 2018, 3, 234–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]














Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofmann, J.; Klingele, S.; Haberkorn, U.; Schmidmaier, G.; Grossner, T. Impact of High-Dose Anti-Infective Agents on the Osteogenic Response of Mesenchymal Stem Cells. Antibiotics 2021, 10, 1257. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101257
Hofmann J, Klingele S, Haberkorn U, Schmidmaier G, Grossner T. Impact of High-Dose Anti-Infective Agents on the Osteogenic Response of Mesenchymal Stem Cells. Antibiotics. 2021; 10(10):1257. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101257
Chicago/Turabian StyleHofmann, Jakob, Sabrina Klingele, Uwe Haberkorn, Gerhard Schmidmaier, and Tobias Grossner. 2021. "Impact of High-Dose Anti-Infective Agents on the Osteogenic Response of Mesenchymal Stem Cells" Antibiotics 10, no. 10: 1257. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101257