
Co-Developing an Antibiotic Stewardship Tool for Dentistry: Shared Decision-Making for Adults with Toothache or Infection



Abstract
:1. Introduction
2. Results
2.1. Stage 1—Understanding the Behaviour/Prioritising Factors
- (1)
- Engaging patient in (rather than just giving them a leaflet or telling them the treatment decision) during urgent dental appointments; and
- (2)
- The use of diagrams on a leaflet (as per the Royal College of General Practitioner’s Urinary Tract Infection self-management leaflet of the Treat Antibiotics Responsibly: Guidance, Education Tools (TARGET) toolkit) to nudge and assist the dentist to explain the diagnosis to the patient [14].
2.2. Stage 2—Identification of Behaviour Change Techniques
2.3. Stage 3—Planning to Deliver the Tool and Acceptability Testing
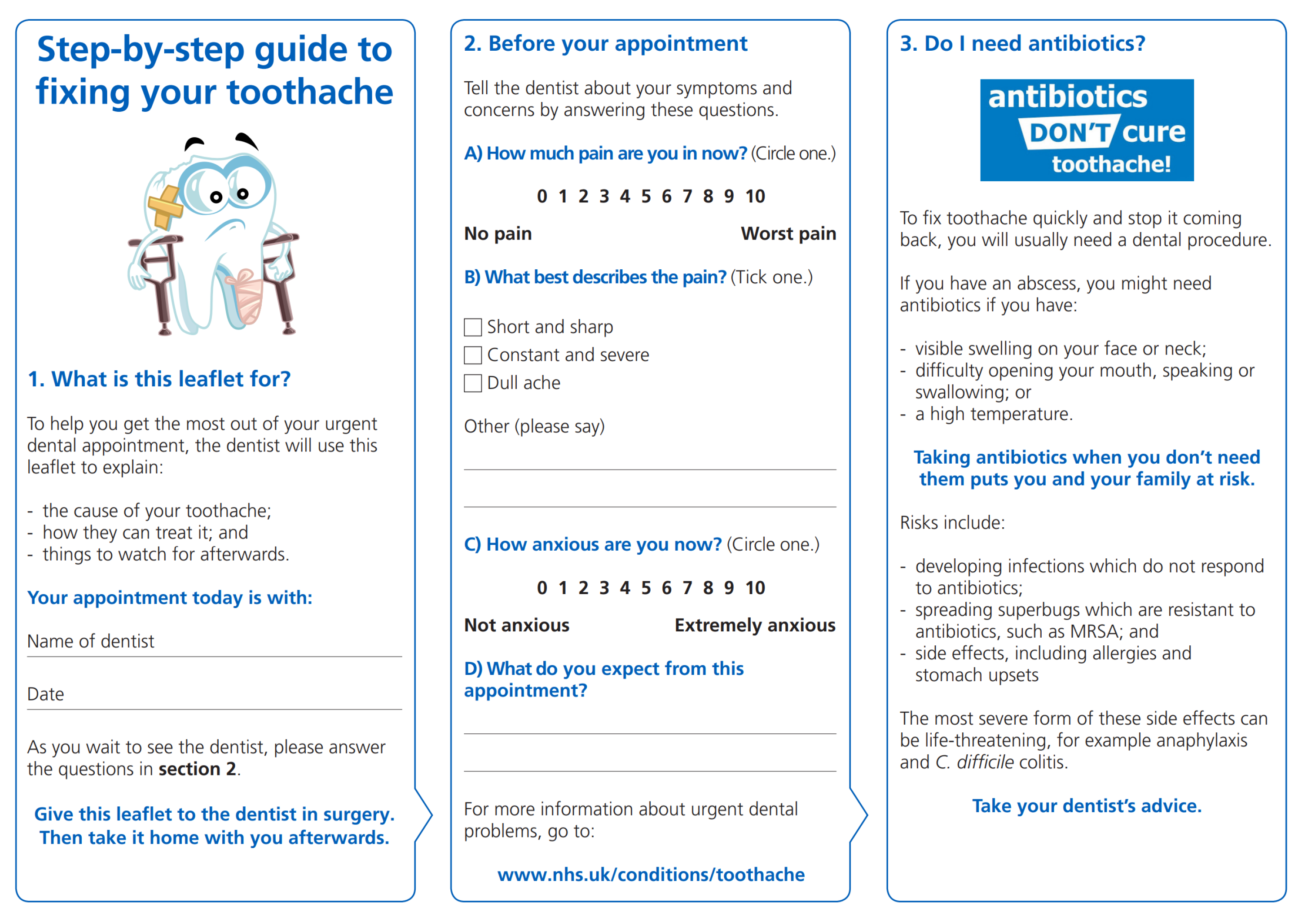
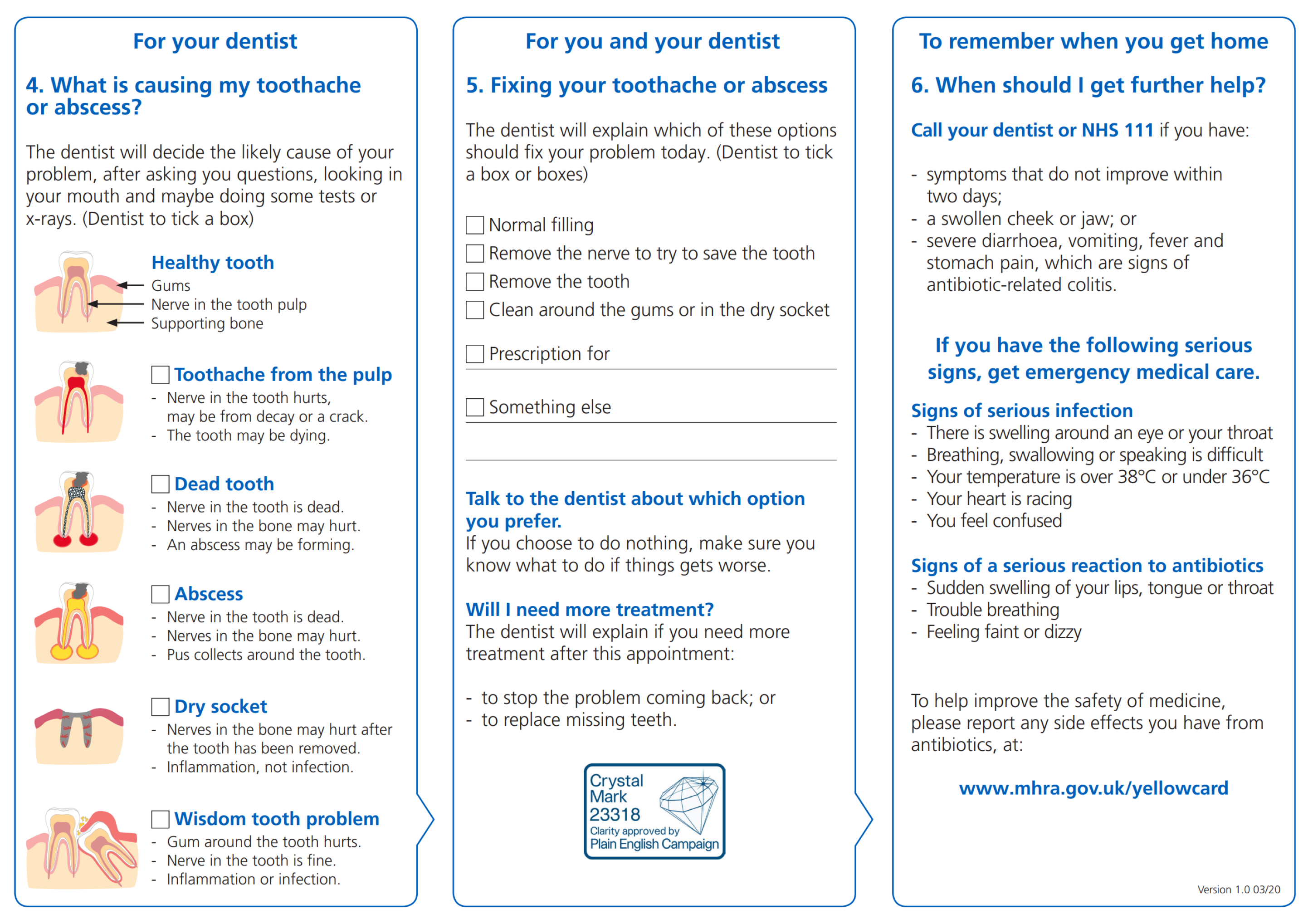
2.3.1. Description of the Worksheet
2.3.2. Planning to Deliver the Worksheet Tool as Part of a Wider Intervention
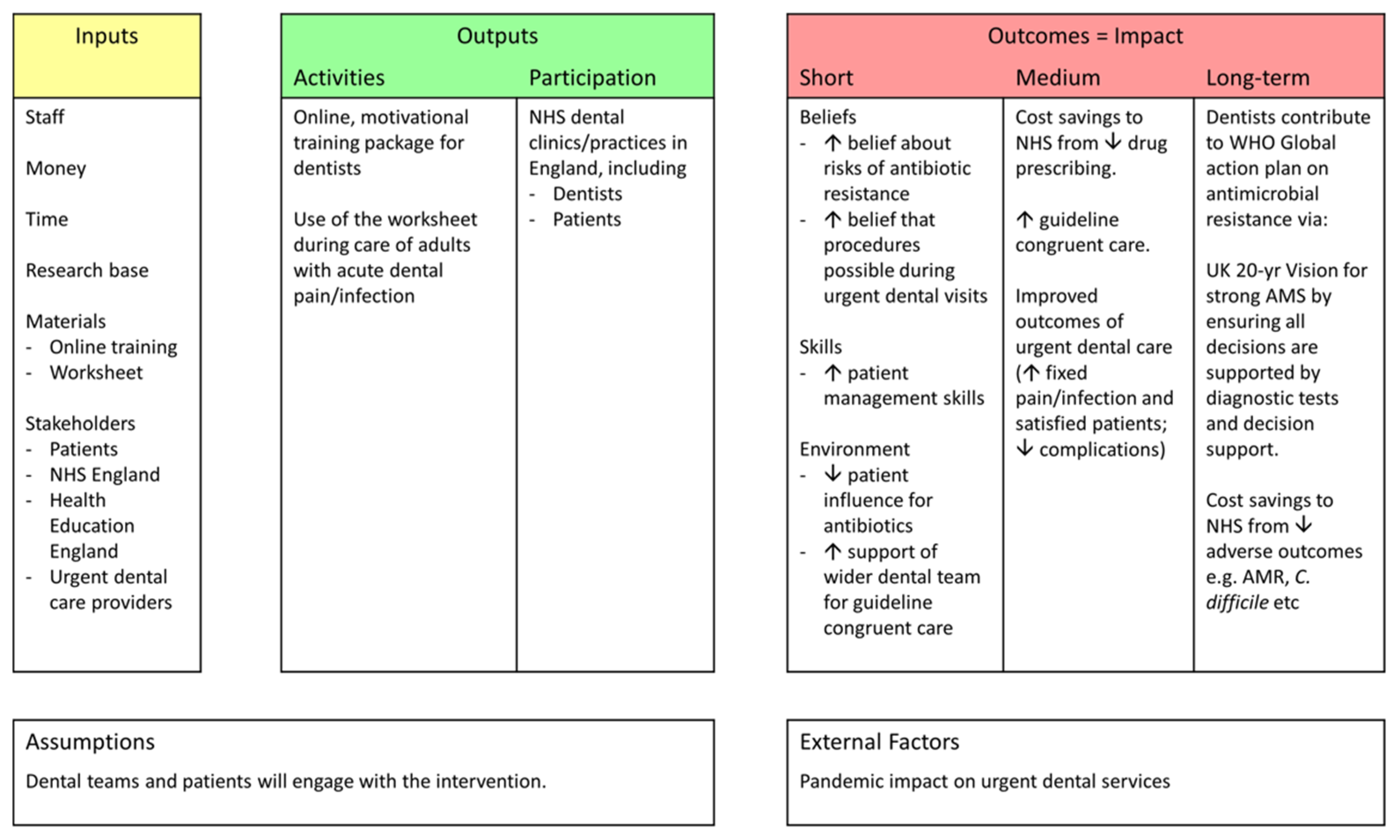
2.4. Logic Model for the Shared Decision-Making, Dental Antibiotic Stewardship Intervention
3. Discussion
4. Materials and Methods
4.1. Stage 1—Understanding the Behaviour/Prioritising Factors
4.2. Stage 2—Identification of Behaviour Change Techniques
4.3. Stage 3—Planning to Deliver the Tool and Acceptability Testing
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Action Plan on Antimicrobial Resistance. Available online: https://apps.who.int/iris/handle/10665/193736 (accessed on 1 November 2021).
- HM Government. Contained and Controlled. The UK’s 20-Year Vision for Antimicrobial Resistance. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/773065/uk-20-year-vision-for-antimicrobial-resistance.pdf (accessed on 1 November 2021).
- Thompson, W.; Williams, D.; Pulcini, C.; Sanderson, S.; Calfon, P.; Verma, M. The Essential Role of the Dental Team in Reducing Antibiotic Resistance; FDI World Dental Federation: Geneva, Switzerland, 2020. [Google Scholar]
- NHS Digital. NHS Dental Statistics for England—2017–18, Annual Report. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-dental-statistics/2017-18-annual-report (accessed on 1 November 2021).
- NHSBSA. eDEN. Available online: https://www.nhsbsa.nhs.uk/access-our-data-products/eden (accessed on 1 November 2021).
- NICE. Managing Common Infections: Guidance for Primary Care; NICE: London, UK, 2021. [Google Scholar]
- House of Commons. Delivering Core NHS and Care Services during the Pandemic and Beyond; Health and Social Care Committee: London, UK, 2020. [Google Scholar]
- CQC. Dental Mythbuster 3: Dental Radiography and X-rays. Available online: https://www.cqc.org.uk/guidance-providers/dentists/dental-mythbuster-3-dental-radiography-x-rays (accessed on 1 November 2021).
- Thompson, W.; Douglas, G.; Pavitt, S.; Sandoe, J.; McEachan, R.; Tonkin-Crine, S. Factors associated with prescribing of systemic antibacterial drugs to adult patients in urgent primary health care, especially dentistry. J. Antimicrob. Chemother. 2019, 74, 2139–2152. [Google Scholar] [CrossRef] [Green Version]
- Coxeter, P.; Del Mar, C.B.; McGregor, L.; Beller, E.M.; Hoffmann, T.C. Interventions to facilitate shared decision making to address antibiotic use for acute respiratory infections in primary care. Cochrane Database Syst. Rev. 2015, 2015, CD010907. [Google Scholar] [CrossRef] [Green Version]
- Thompson, W.; McEachan, R.; Pavitt, S.; Douglas, G.; Bowman, M.; Sandoe, J. Clinician and Patient Factors Influencing Treatment Decisions: Ethnographic Study of Antibiotic Prescribing and Operative Procedures in Out-of-Hours and General Dental Practices. Antibiotics 2020, 9, 575. [Google Scholar] [CrossRef]
- PHE. Dental Antimicrobial Stewardship Toolkit. Available online: https://www.gov.uk/guidance/dental-antimicrobial-stewardship-toolkit (accessed on 1 November 2021).
- Thompson, W. Antibiotic Prescribing: Towards a reducTion during Urgent NHS Dental Appointments in England (The APTiTUDE Study). Ph.D. Thesis, University of Leeds, Leeds, UK, 2019. [Google Scholar]
- Jones, L.F.; Cooper, E.; Joseph, A.; Allison, R.; Gold, N.; Donald, I.; McNulty, C. Development of an information leaflet and diagnostic flow chart to improve the management of urinary tract infections in older adults: A qualitative study using the Theoretical Domains Framework. BJGP Open 2020, 4, bjgpopen20X101044. [Google Scholar] [CrossRef]
- Human Behvaiour Change Project. Theory & Techniques Tool. Available online: https://theoryandtechniquetool.humanbehaviourchange.org/ (accessed on 1 November 2021).
- NICE. Shared Decision Making NICE Guideline NG197; National Institute for Health & Care Excellence: London, UK, 2021. [Google Scholar]
- NHSE. Commissioning Standard for Urgent Dental Care. Available online: https://www.england.nhs.uk/publication/commissioning-standard-for-urgent-dental-care/ (accessed on 1 November 2021).
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions; Silverback Publishing: Sutton, UK, 2014. [Google Scholar]
- Michie, S.; Van Stralen, M.; West, R. The Behaviour Change Wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carey, R.N.; Connell, L.E.; Johnston, M.; Rothman, A.J.; De Bruin, M.; Kelly, M.P.; Michie, S. Behavior change techniques and their mechanisms of action: A synthesis of links described in published intervention literature. Ann. Behav. Med. 2019, 53, 693–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, L.; Cresswell, K.; Williams, S.; Parsons, S.; Keane, A.; Wilson, C.; Islam, S.; Joseph, O.; Miah, J.; Robinson, E. Innovating public engagement and patient involvement through strategic collaboration and practice. Res. Involv. Engagem. 2019, 5, 1–12. [Google Scholar] [CrossRef]
- Holmes, B.J. On the co-production of research: Why we should say what we mean, mean what we say, and learn as we go. Impact Soc. Sci. Blog 2017. Available online: https://blogs.lse.ac.uk/impactofsocialsciences/2017/09/21/on-the-co-production-of-research-why-we-should-say-what-we-mean-mean-what-we-say-and-learn-as-we-go/ (accessed on 1 November 2021).
- Buckley, B.; Thijssen, D.; Murphy, R.; Graves, L.; Whyte, G.; Gillison, F.; Crone, D.; Wilson, P.; Watson, P. Making a move in exercise referral: Co-development of a physical activity referral scheme. J. Public Health 2018, 40, e586–e593. [Google Scholar] [CrossRef]
- Holmes, B.J.; Best, A.; Davies, H.; Hunter, D.; Kelly, M.P.; Marshall, M.; Rycroft-Malone, J. Mobilising knowledge in complex health systems: A call to action. Evid. Policy 2017, 13, 539–560. [Google Scholar] [CrossRef]
- Boivin, A.; Lehoux, P.; Burgers, J.; Grol, R. What are the key ingredients for effective public involvement in health care improvement and policy decisions? A randomized trial process evaluation. Milbank Q. 2014, 92, 319–350. [Google Scholar] [CrossRef]
- Anthierens, S.; Tonkin-Crine, S.; Douglas, E.; Fernandez-Vandellos, P.; Krawczyk, J.; Llor, C.; Cals, J.W.; Francis, N.A.; Yardley, L.; Coenen, S. General practitioners’ views on the acceptability and applicability of a web-based intervention to reduce antibiotic prescribing for acute cough in multiple European countries: A qualitative study prior to a randomised trial. BMC Fam. Pract. 2012, 13, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouwels, K.B.; Dolk, F.C.K.; Smith, D.R.; Robotham, J.V.; Smieszek, T. Actual versus ‘ideal’antibiotic prescribing for common conditions in English primary care. J. Antimicrob. Chemother. 2018, 73, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Cope, A.L.; Francis, N.A.; Wood, F.; Chestnutt, I.G. Antibiotic prescribing in UK general dental practice: A cross-sectional study. Community Dent. Oral Epidemiol. 2016, 44, 145–153. [Google Scholar] [CrossRef]
- Cabana, M.D.; Rand, C.S.; Powe, N.R.; Wu, A.W.; Wilson, M.H.; Abboud, P.-A.C.; Rubin, H.R. Why don’t physicians follow clinical practice guidelines? A framework for improvement. J. Am. Med. Assoc. 1999, 282, 1458–1465. [Google Scholar] [CrossRef]
- Santarossa, M.; Kilber, E.N.; Wenzler, E.; Albarillo, F.S.; Sterk, E.J. Bundled up: A narrative review of antimicrobial stewardship initiatives and bundles in the emergency department. Pharmacy 2019, 7, 145. [Google Scholar] [CrossRef] [Green Version]
- Jones, L.F.; Hawking, M.K.; Owens, R.; Lecky, D.; Francis, N.A.; Butler, C.; Gal, M.; McNulty, C.A. An evaluation of the TARGET (Treat Antibiotics Responsibly; Guidance, Education, Tools) Antibiotics Toolkit to improve antimicrobial stewardship in primary care—is it fit for purpose? Fam. Pract. 2018, 35, 461–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loffler, C.; Bohmer, F.; Hornung, A.; Lang, H.; Burmeister, U.; Podbielski, A.; Wollny, A.; Kundt, G.; Altiner, A. Dental care resistance prevention and antibiotic prescribing modification-the cluster-randomised controlled DREAM trial. Implement. Sci. 2014, 9, 27. [Google Scholar] [CrossRef] [Green Version]
- Emmott, R.; Barber, S.K.; Thompson, W. Antibiotics and toothache: A social media review. Int. J. Pharm. Pract. 2021, 29, 210–217. [Google Scholar] [CrossRef]
- Kirton, J.; Thompson, W.; Pearce, M.; Brown, J. Ability of the wider dental team to triage patients with acute conditions: A qualitative study. Br. Dent. J. 2020, 228, 103–107. [Google Scholar] [CrossRef]
- Smith, C.M.; Shallcross, L.J.; Dutey-Magni, P.; Conolly, A.; Fuller, C.; Hill, S.; Jhass, A.; Marcheselli, F.; Michie, S.; Mindell, J.S. Incidence, healthcare-seeking behaviours, antibiotic use and natural history of common infection syndromes in England: Results from the Bug Watch community cohort study. BMC Infect. Dis. 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Stivers, T. Managing Patient Pressure to Prescribe Antibiotics in the Clinic. Pediatric Drugs 2021, 23, 437–443. [Google Scholar] [CrossRef]
- Kohut, M.R.; Keller, S.C.; Linder, J.A.; Tamma, P.D.; Cosgrove, S.E.; Speck, K.; Ahn, R.; Dullabh, P.; Miller, M.A.; Szymczak, J.E. The inconvincible patient: How clinicians perceive demand for antibiotics in the outpatient setting. Fam. Pract. 2020, 37, 276–282. [Google Scholar] [CrossRef]
- Hayes, C.V.; Mahon, B.; Sides, E.; Allison, R.; Lecky, D.M.; McNulty, C.A.M. Empowering Patients to Self-Manage Common Infections: Qualitative Study Informing the Development of an Evidence-Based Patient Information Leaflet. Antibiotics 2021, 10, 1113. [Google Scholar] [CrossRef]
- James Lind Alliance. Oral and Dental Health. Available online: https://www.jla.nihr.ac.uk/priority-setting-partnerships/oral-and-dental-health/ (accessed on 1 November 2021).
- Dailey, Y.-M.; Humphris, G.; Lennon, M. Reducing patients’ state anxiety in general dental practice: A randomized controlled trial. J. Dent. Res. 2002, 81, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Agnihotry, A.; Thompson, W.; Fedorowicz, Z.; van Zuuren, E.J.; Sprakel, J. Antibiotic use for irreversible pulpitis. Cochrane Database Syst. Rev. 2019, 5, CD004969. [Google Scholar] [CrossRef] [PubMed]
- Cope, A.; Francis, N.; Wood, F.; Chestnutt, I. Systemic antibiotics for symptomatic apical periodontitis and acute apical abscess in adults. Cochrane Database Syst. Rev. 2018, 9, CD010136. [Google Scholar] [CrossRef]
- Shah, S.W.V.; Thompson, W. How did COVID-19 impact on dental antibiotic prescribing across England? Br. Dent. J. 2020, 229, 601–604. [Google Scholar] [CrossRef]
- Rabie, H.; Figueiredo, R. Provision of dental care by public health dental clinicsduring the COVID-19 Pandemic in Alberta Canada. Prim. Dent. J. 2021, 10, 47–54. [Google Scholar] [CrossRef]
- Mian, M.; Teoh, L.; Hopcraft, M. Trends in Dental Medication Prescribing in Australia during the COVID-19 Pandemic. JDR Clin. Transl. Res. 2021, 6, 145–152. [Google Scholar] [CrossRef]
- Kerr, I.; Reed, D.; Brennan, A.-M.; Eaton, K.A. An investigation into possible factors that may impact on the potential for inappropriate prescriptions of antibiotics: A survey of general dental practitioners’ approach to treating adults with acute dental pain. Br. Dent. J. 2021, 1–6. [Google Scholar] [CrossRef]
- Agency, U.H.S. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2021. 2021; in production. [Google Scholar]
- van der Zande, M.M.; Dembinsky, M.; Aresi, G.; van Staa, T.P. General practitioners’ accounts of negotiating antibiotic prescribing decisions with patients: A qualitative study on what influences antibiotic prescribing in low, medium and high prescribing practices. BMC Fam. Pract. 2019, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Asimakopoulou, K.; Newton, J.T. The contributions of behaviour change science towards dental public health practice: A new paradigm. Community Dent. Oral Epidemiol. 2015, 43, 2–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef]
- Lecky, D.M.; Howdle, J.; Butler, C.C.; McNulty, C.A. Optimising management of UTIs in primary care: A qualitative study of patient and GP perspectives to inform the development of an evidence-based, shared decision-making resource. Br. J. Gen. Pract. 2020, 70, e330–e338. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Priority Factors | TDF | BCT |
|---|---|---|
| Antibiotic beliefs | Beliefs about consequences | Information about health consequences Salience of health consequences |
| Competing demands | Environmental context and resources | Prompts and cues Restructuring the social environment Adding objects to the environment |
| Fix the problem | Goals | Goal setting (behaviour) |
| Patient influence | Social influences | Restructuring the social environment |
| Patient management | Skills | Instructions on how to perform the behaviour |
| Peers and colleagues | Social influences | Restructuring the social environment Structuring the physical environment |
| Planning and consent | Beliefs about capabilities | Verbal persuasion about capability |
| Procedure possible | Beliefs about capabilities | Verbal persuasion about capability |
| Professional role | Professional role and identity | Credible source |
| Worksheet Section/Issue | Feedback from Stakeholders | Resulting Modification |
|---|---|---|
| Title and ‘What is this leaflet for? section | Suggested title: ‘Step-by-step guide to fixing your toothache’. Add the dentist’s name. | Title changed accordingly and a space for the dentist’s name (to be written by the clinic’s reception team) was added. |
| ‘Notes’ section | More structure required and located earlier in the worksheet. ‘Provide more structure to this section to get me to think about my problem. And then ask me if I think I might need antibiotics!’ (Patient participant) A dentist participant suggested asking patients about their anxiety which can be a problem in urgent dental appointments. | New section added: ‘Before your appointment’ and included visual analogue scales for pain and anxiety, plus free text for patient’s expectations. |
| ‘Do I need antibiotics?’ section | Essential section. Advised locating where it could be read by patients whilst waiting to see the dentist without being the primary focus of the worksheet. | Relocated after the ‘Before your appointment’ section. |
| ‘What is causing my dental problem?’ section | Diagrams essential to help explain the cause of symptoms to patients, but could be clearer: ‘…don’t need to be a double tooth. Just include a healthy one at the top.’ (Patient participant) | The diagrams were simplified in line with the advice. |
| Issue of credibility | Credible source essential. A dentist participant noted ‘It needs to look official. Good quality paper. And can you add the NHS logo?’ | Permission was obtained to use the recognisable ‘Antibiotics Don’t Cure Toothache’ logo from the UK dental antimicrobial stewardship toolkit, and the Crystal Mark added credibility to the worksheet. |
| Issue of format | Concerns about a digital version included digital exclusion. Concerns about a paper-based version included colour printing, as some dental practices only have black and white printers. | A paper-based format with colours which are clear when printed in either colour or black and white. |
| Issue of dentist’s ability | Training need identified: ‘…training to teach dentists how to explain things like antibiotic-related colitis.’ (Dentist participant) | During implementation, the on-line training package to accompany the worksheet would cover this skill. |
| Section | Content | BCT |
|---|---|---|
| 1. What is this leaflet for? | Reception completes Section 1 and hands the worksheet to the patient, thus engaging them in optimising urgent dental care. | Restructuring the social environment Adding objects to the environment |
| 2. Before your appointment | Patient completes their pain, anxiety and other information, and hands the worksheet to the dentist, thus prompting the dentist to dedicate time to understanding the patient perspective. | Prompts and cues |
| 3. Do I need antibiotics? | Provides information about the risks of antibiotics. ‘Antibiotics Don’t Cure Toothache’ branding adds credibility | Information about health consequences Salience of health consequences Credible source |
| 4. What is causing my toothache or abscess? | Environment restructured so the patient expects to be told a diagnosis. Diagrams nudging and assisting the dentist to explain the diagnosis. | Restructuring the social environment Prompts and cues |
| 5. Fixing your toothache or abscess | Prompts the dentist to explain treatment options and share decision-making. Empowers the patient. The Crystal Mark adds credibility to the workbook. | Prompts and cues Credible source |
| 6. When should I get further help? | Provides safety netting advice (Information about what to do if the treatment provided fails). Referencing the Medicines and Healthcare products Regulatory Agency adds credibility. | Information about health consequences Credible source |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thompson, W.; Sandoe, J.; Pavitt, S.; Walsh, T.; Byrne-Davis, L. Co-Developing an Antibiotic Stewardship Tool for Dentistry: Shared Decision-Making for Adults with Toothache or Infection. Antibiotics 2021, 10, 1345. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111345
Thompson W, Sandoe J, Pavitt S, Walsh T, Byrne-Davis L. Co-Developing an Antibiotic Stewardship Tool for Dentistry: Shared Decision-Making for Adults with Toothache or Infection. Antibiotics. 2021; 10(11):1345. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111345
Chicago/Turabian StyleThompson, Wendy, Jonathan Sandoe, Sue Pavitt, Tanya Walsh, and Lucie Byrne-Davis. 2021. "Co-Developing an Antibiotic Stewardship Tool for Dentistry: Shared Decision-Making for Adults with Toothache or Infection" Antibiotics 10, no. 11: 1345. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111345