
Is There a Difference in Clinical Features, Microbiological Epidemiology and Effective Empiric Antimicrobial Therapy Comparing Healthcare-Associated and Community-Acquired Vertebral Osteomyelitis?

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics, Clinical Presentation, and Treatment (1)
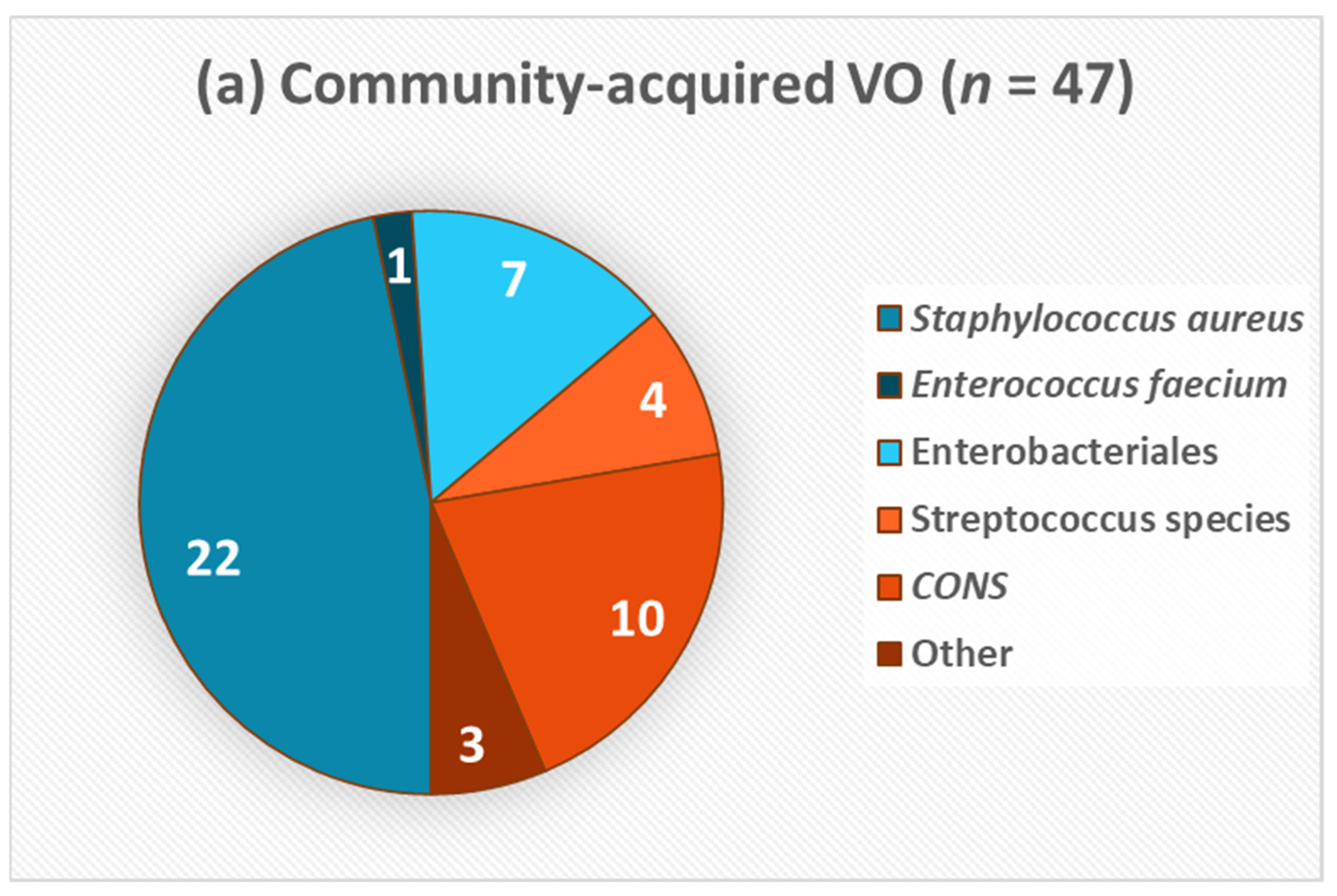
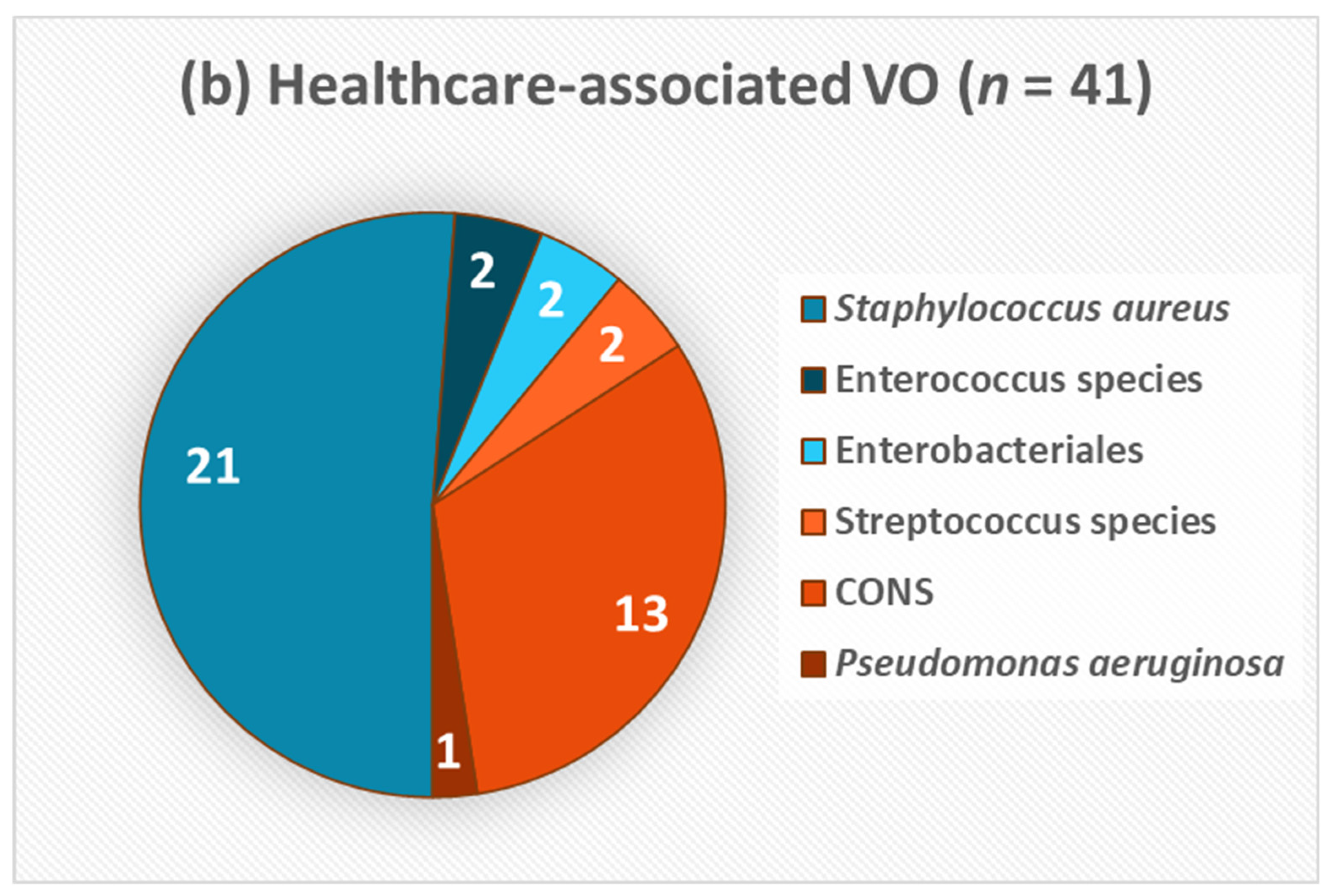
2.2. Aetiology and Microbiological Pattern (2)
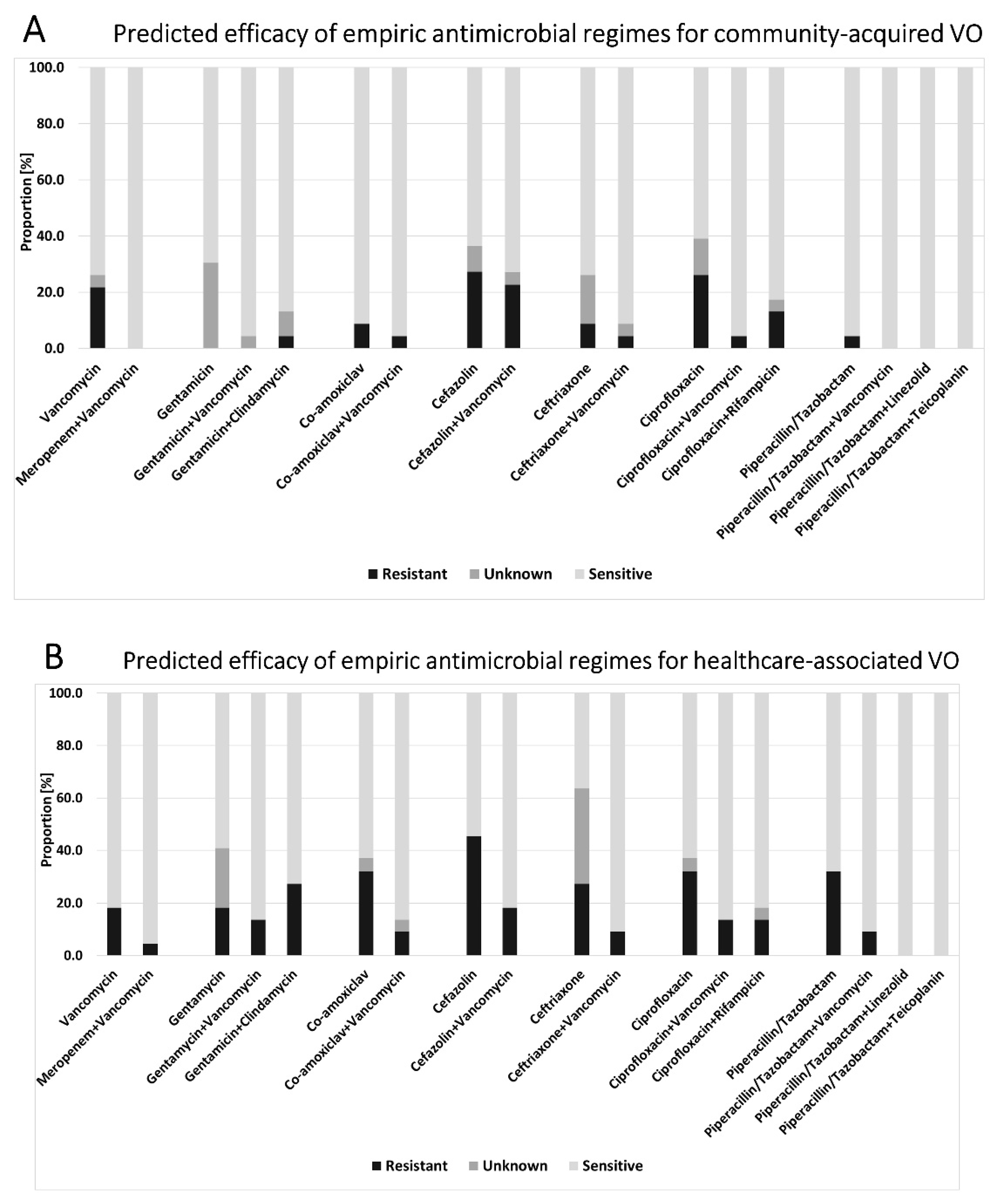
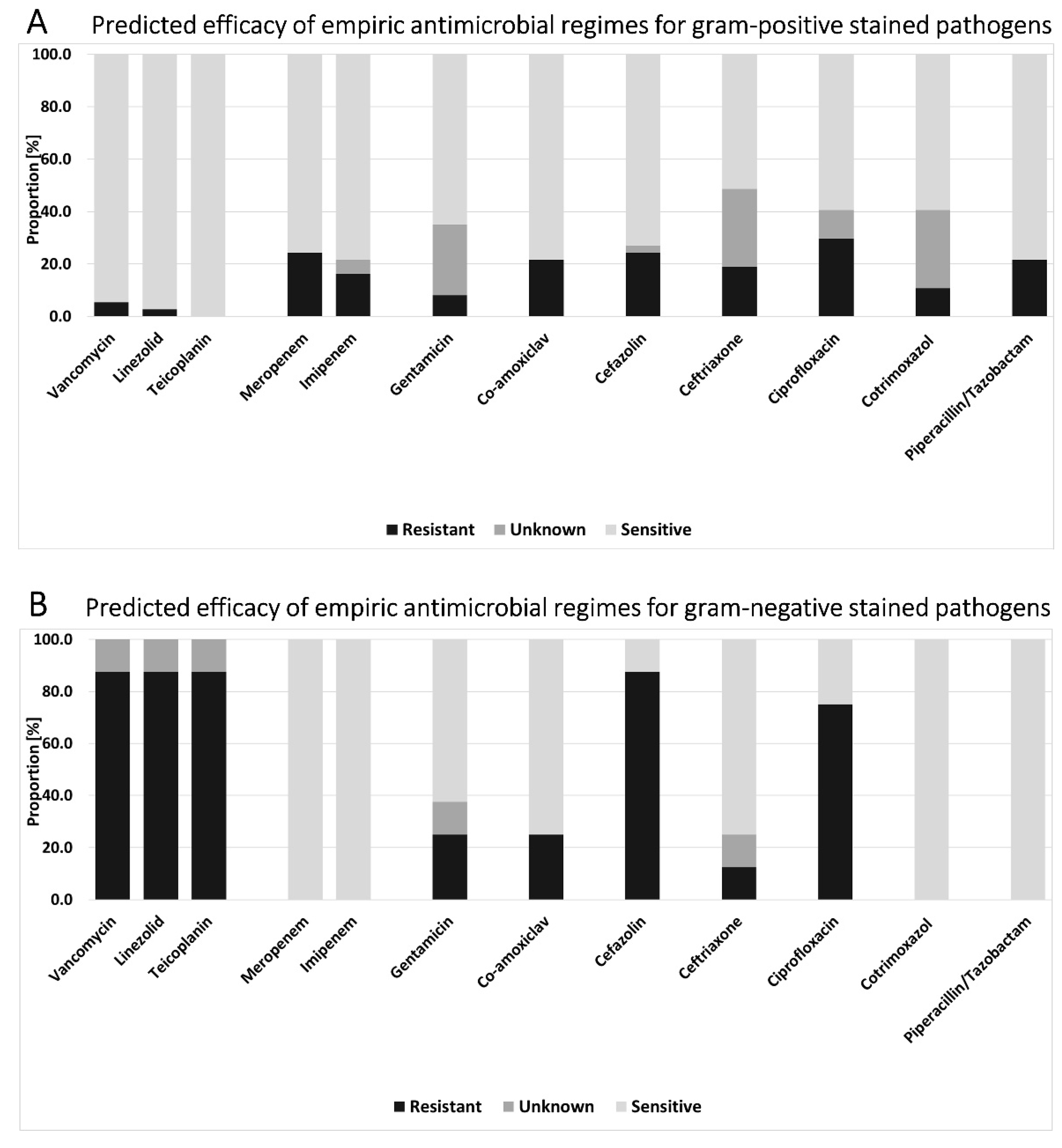
2.3. Antimicrobial Regimes (3)
2.4. Difference of Antibiotic Susceptibility of Pathogens Evidenced in HAVO and CAVO (4)
3. Discussion
3.1. Patient Characteristics and Clinical Presentation and Treatment (1)
3.2. Aetiology and Microbiological Pattern (2)
3.3. Empirical Antibiotic Therapy Regimes and Differences between CAVO and HAVO (3 and 4)
3.4. Limitations
4. Materials and Methods
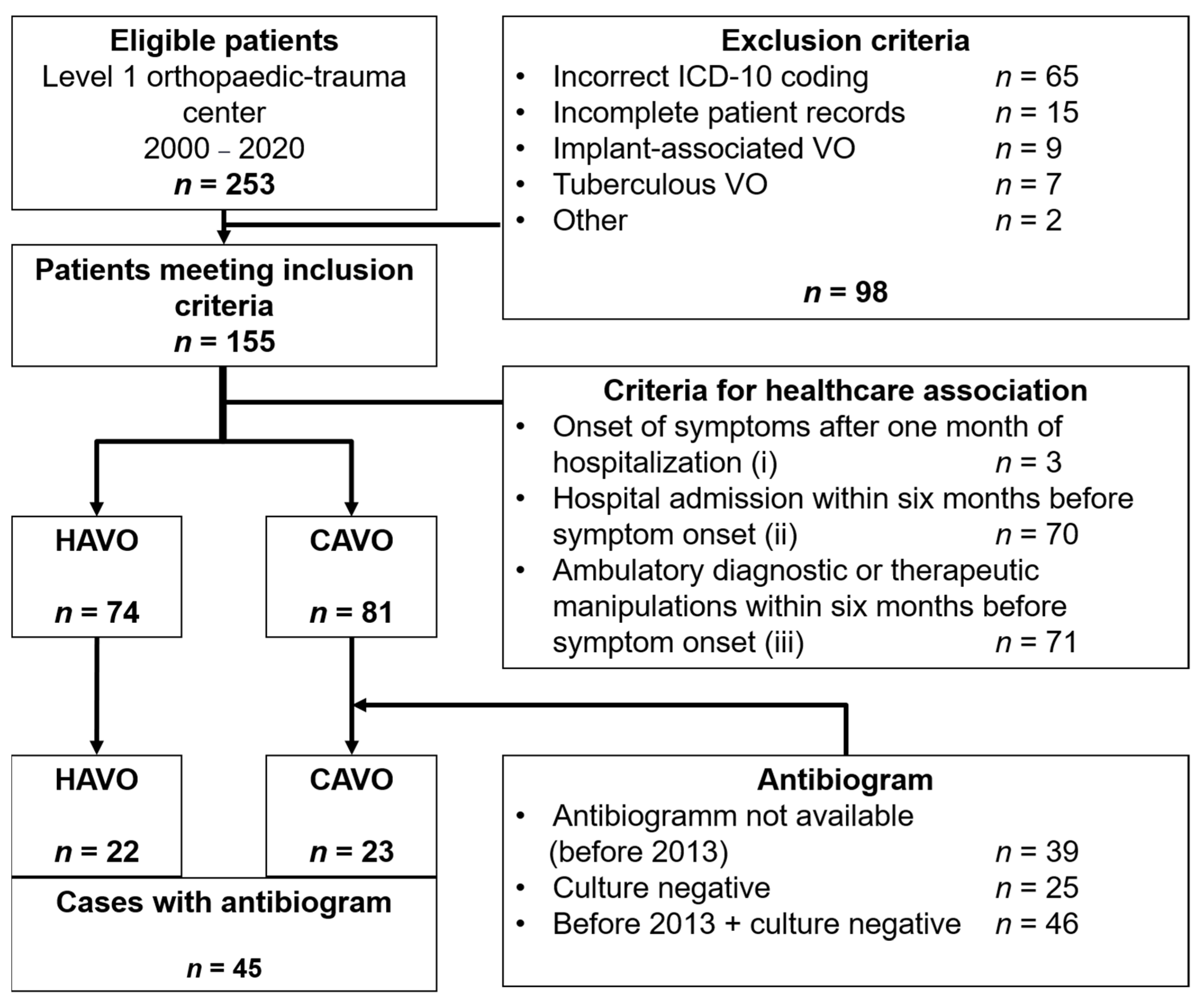
4.1. Patient Identification
- (i)
- Onset of symptoms after one month of hospitalization with no evidence of vertebral osteomyelitis at admission;
- (ii)
- Hospital admission within six months before symptom onset;
- (iii)
- Ambulatory diagnostic or therapeutic manipulations within six months before symptom onset (long-term central venous catheter use, arteriovenous fistula for hemodialysis, invasive intravascular techniques, urological, gynecological or digestive procedures, and cutaneous manipulations).
4.2. Data Collection
4.3. Microbiology
4.4. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grammatico, L.; Baron, S.; Rusch, E.; Lepage, B.; Surer, N.; Desenclos, J.C.; Besnier, J.M. Epidemiology of vertebral osteomyelitis (VO) in France: Analysis of hospital-discharge data 2002–2003. Epidemiol. Infect. 2008, 136, 653–660. [Google Scholar] [CrossRef]
- Fantoni, M.; Trecarichi, E.M.; Rossi, B.; Mazzotta, V.; Di Giacomo, G.; Nasto, L.A.; Di Meco, E.; Pola, E. Epidemiological and clinical features of pyogenic spondylodiscitis. Eur. Rev. Med. Pharmacol. Sci. 2012, 16 (Suppl. S2), 2–7. [Google Scholar]
- Jensen, A.; Espersen, F.; Skinhøj, P.; Rosdahl, V.; Frimodt-Møller, N. Increasing frequency of vertebral osteomyelitis following Staphylococcus aureus bacteraemia in Denmark 1980–1990. J. Infect. 1997, 34, 113–118. [Google Scholar] [CrossRef]
- Nickerson, E.K.; Sinha, R. Vertebral osteomyelitis in adults: An update. Br. Med. Bull. 2016, 117, 121–138. [Google Scholar] [CrossRef]
- Kehrer, M.; Pedersen, C.; Jensen, T.G.; Lassen, A.T. Increasing incidence of pyogenic spondylodiscitis: A 14-year population-based study. J. Infect. 2014, 68, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Lang, S.; Rupp, M.; Hanses, F.; Neumann, C.; Loibl, M.; Alt, V. Infections of the spine: Pyogenic spondylodiscitis and implant-associated vertebral osteomyelitis. Unfallchirurg 2021, 124, 489–504. [Google Scholar] [CrossRef]
- Hopkinson, N.; Stevenson, J.; Benjamin, S. A case ascertainment study of septic discitis: Clinical, microbiological and radiological features. QJM 2001, 94, 465–470. [Google Scholar] [CrossRef] [Green Version]
- Duarte, R.M.; Vaccaro, A.R. Spinal infection: State of the art and management algorithm. Eur. Spine J. 2013, 22, 2787–2799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pigrau, C.; Rodriguez-Pardo, D.; Fernández-Hidalgo, N.; Moretó, L.; Pellise, F.; Larrosa, M.N.; Puig-Asensio, M.; Almirante, B. Health care associated hematogenous pyogenic vertebral osteomyelitis: A severe and potentially preventable infectious disease. Medicine 2015, 94, e365. [Google Scholar] [CrossRef]
- McHenry, M.C.; Easley, K.A.; Locker, G.A. Vertebral osteomyelitis: Long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2002, 34, 1342–1350. [Google Scholar] [CrossRef]
- Mylona, E.; Samarkos, M.; Kakalou, E.; Fanourgiakis, P.; Skoutelis, A. Pyogenic vertebral osteomyelitis: A systematic review of clinical characteristics. Semin. Arthritis Rheum. 2009, 39, 10–17. [Google Scholar] [CrossRef]
- Renz, N.; Haupenthal, J.; Schuetz, M.A.; Trampuz, A. Hematogenous vertebral osteomyelitis associated with intravascular device-associated infections—A retrospective cohort study. Diagn. Microbiol. Infect. Dis. 2017, 88, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Berbari, E.F.; Kanj, S.S.; Kowalski, T.J.; Darouiche, R.O.; Widmer, A.F.; Schmitt, S.K.; Hendershot, E.F.; Holtom, P.D.; Huddleston, P.M., 3rd; Petermann, G.W.; et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2015, 61, e26–e46. [Google Scholar] [CrossRef] [Green Version]
- Pola, E.; Autore, G.; Formica, V.M.; Pambianco, V.; Colangelo, D.; Cauda, R.; Fantoni, M. New classification for the treatment of pyogenic spondylodiscitis: Validation study on a population of 250 patients with a follow-up of 2 years. Eur. Spine J. 2017, 26, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Company, J.; Pigrau, C.; Fernández-Hidalgo, N.; Rodríguez-Pardo, D.; Falcó, V.; Lung, M.; Pellisé, F.; Almirante, B. Native vertebral osteomyelitis in aged patients: Distinctive features. An observational cohort study. Infection 2018, 46, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Yagdiran, A.; Otto-Lambertz, C.; Lingscheid, K.M.; Sircar, K.; Samel, C.; Scheyerer, M.J.; Zarghooni, K.; Eysel, P.; Sobottke, R.; Jung, N.; et al. Quality of life and mortality after surgical treatment for vertebral osteomyelitis (VO): A prospective study. Eur. Spine J. 2021, 30, 1721–1731. [Google Scholar] [CrossRef]
- Yu, D.; Kim, S.W.; Jeon, I. Antimicrobial therapy and assessing therapeutic response in culture-negative pyogenic vertebral osteomyelitis: A retrospective comparative study with culture-positive pyogenic vertebral osteomyelitis. BMC Infect. Dis. 2020, 20, 939. [Google Scholar] [CrossRef]
- Avenel, G.; Guyader, P.; Fiaux, E.; Alcaix, D.; Zarnitsky, C.; Pouplin-Jardin, S.; Kozyreff-Meurice, M.; Lequerré, T.; Vittecoq, O. Microbiological diagnosis of suspected vertebral osteomyelitis with a focus on the yield of percutaneous needle biopsy: A 10-year cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 297–302. [Google Scholar] [CrossRef]
- Gouliouris, T.; Aliyu, S.H.; Brown, N.M. Spondylodiscitis: Update on diagnosis and management. J. Antimicrob. Chemother. 2010, 65 (Suppl. S3), iii11–iii24. [Google Scholar] [CrossRef] [Green Version]
- Amsilli, M.; Epaulard, O. How is the microbial diagnosis of bacterial vertebral osteomyelitis performed? An 11-year retrospective study. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2065–2076. [Google Scholar] [CrossRef]
- Park, K.-H.; Kim, D.Y.; Lee, Y.-M.; Lee, M.S.; Kang, K.-C.; Lee, J.-H.; Park, S.Y.; Moon, C.; Chong, Y.P.; Kim, S.-H.; et al. Selection of an appropriate empiric antibiotic regimen in hematogenous vertebral osteomyelitis. PLoS ONE 2019, 14, e0211888. [Google Scholar] [CrossRef]
- Michels, R.; Last, K.; Becker, S.L.; Papan, C. Update on Coagulase-Negative Staphylococci-What the Clinician Should Know. Microorganisms 2021, 9, 830. [Google Scholar] [CrossRef] [PubMed]
- Lopez, J.; Tatar, Z.; Tournadre, A.; Couderc, M.; Pereira, B.; Soubrier, M.; Dubost, J.-J. Characteristics of spontaneous coagulase-negative staphylococcal spondylodiscitis: A retrospective comparative study versus Staphylococcus aureus spondylodiscitis. BMC Infect. Dis. 2017, 17, 683. [Google Scholar] [CrossRef] [PubMed]
- Bucher, E.; Trampuz, A.; Donati, L.; Zimmerli, W. Spondylodiscitis associated with bacteraemia due to coagulase-negative staphylococci. Eur. J. Clin. Microbiol. Infect. Dis. 2000, 19, 118–120. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Mueller, B.; Trampuz, A. Serum procalcitonin for discrimination of blood contamination from bloodstream infection due to coagulase-negative staphylococci. Infection 2007, 35, 352–355. [Google Scholar] [CrossRef] [Green Version]
- Oh, W.S.; Moon, C.; Chung, J.W.; Choo, E.J.; Kwak, Y.G.; Kim, S.-H.; Ryu, S.Y.; Park, S.Y.; Kim, B.-N. Antibiotic Treatment of Vertebral Osteomyelitis caused by Methicillin-Susceptible Staphylococcus aureus: A Focus on the Use of Oral β-lactams. Infect. Chemother. 2019, 51, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Fleege, C.; Wichelhaus, T.A.; Rauschmann, M. Systemic and local antibiotic therapy of conservative and operative treatment of spondylodiscitis. Der Orthop. 2012, 41, 727–735. [Google Scholar] [CrossRef]
- Park, K.-H.; Cho, O.H.; Jung, M.; Suk, K.-S.; Lee, J.H.; Park, J.S.; Ryu, K.N.; Kim, S.-H.; Lee, S.-O.; Choi, S.-H.; et al. Clinical characteristics and outcomes of hematogenous vertebral osteomyelitis caused by gram-negative bacteria. J. Infect. 2014, 69, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E.; De Angelis, G.; Cataldo, M.A.; Mantengoli, E.; Spanu, T.; Pan, A.; Corti, G.; Radice, A.; Stolzuoli, L.; Antinori, S.; et al. Antibiotic Usage and Risk of Colonization and Infection with Antibiotic-Resistant Bacteria: A Hospital Population-Based Study. Antimicrob. Agents Chemother. 2009, 53, 4264–4269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangaraj, G.; Cleveland, K.; Gelfand, M. Comparative Analysis of Daptomycin and Vancomycin in the Treatment of Vertebral Osteomyelitis. Infect. Dis. Clin. Pract. 2014, 22, 219–222. [Google Scholar] [CrossRef]
- Fleege, C.; Rauschmann, M.; Arabmotlagh, M.; Rickert, M. Development and current use of local antibiotic carriers in spondylodiscitis. Orthopäde 2020, 49, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Ledermann, H.P.; Schweitzer, M.E.; Morrison, W.B.; Carrino, J.A. MR Imaging Findings in Spinal Infections: Rules or Myths? Radiology 2003, 228, 506–514. [Google Scholar] [CrossRef]
- Jevtic, V. Vertebral infection. Eur. Radiol. Suppl. 2004, 14, E43–E52. [Google Scholar] [CrossRef] [PubMed]
- Park, K.H.; Cho, O.H.; Lee, J.H.; Park, J.S.; Ryu, K.N.; Park, S.Y.; Lee, Y.M.; Chong, Y.P.; Kim, S.H.; Lee, S.O.; et al. Optimal Duration of Antibiotic Therapy in Patients with Hematogenous Vertebral Osteomyelitis at Low Risk and High Risk of Recurrence. Clin. Infect. Dis. 2016, 62, 1262–1269. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- EUCAST: AST of Bacteria n.d. Available online: https://www.eucast.org/ast_of_bacteria/ (accessed on 8 November 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (n = 155) | CAVO (n = 81) | HAVO (n = 74) |
|---|---|---|---|
| Demographic data | |||
| Sex (male) | 88 (56.8%) | 41 (50.6%) | 47 (63.5%) |
| Age (years) | 66.1 ± 12.4 | 66.6 ± 12.9 | 65.6 ± 11.9 |
| BMI (kg/m2) | 29.0 ± 8.2 | 29.9 ± 9.0 | 28.4 ± 7.7 |
| CCI | 1 [0–8] (1.8 ± 1.8) | 1 [0–7] (1.5 ± 1.6) | 2 [0–8] (2.1 ± 1.9) |
| Location | |||
| Cervical spine | 12 (7.7%) | 8 (9.9%) | 4 (5.4%) |
| Thoracic spine | 57 (36.8%) | 34 (42.0%) | 23 (31.1%) |
| Lumbar spine | 74 (47.7%) | 35 (43.2%) | 39 (52.7%) |
| Multifocal | 12 (7.7%) | 4 (4.9%) | 8 (10.8%) |
| Duration of symptoms (days) | 63.7 ± 82.2 | 56.9 ± 64.2 | 69.9 ± 96.9 |
| Hospitalization (days) | 36.3 ± 36.3 | 32.3 ± 23.0 | 40.6 ± 46.5 |
| In-hospital deaths | 20 (12.9%) | 9 (11.1%) | 11 (14.9%) |
| Microbiologic results | |||
| Culture-negative | 67 (43.2%) | 34 (41.9%) | 33 (44.6%) |
| Antibiogram available | 45 (29.0%) | 23 (28.4%) | 22 (29.7%) |
| Positive blood culture | 70 (45.2%) | 35 (43.2%) | 35 (47.3%) |
| CAVO (n = 9) | HAVO (n = 11) | |||||
|---|---|---|---|---|---|---|
| Reason | n | % | Age [years] | n | % | Age [years] |
| Cardiovascular arrest | 2 | 22.2 | 65; 74 | 2 | 18.2 | 66; 79 |
| Multi-organ failure | 3 | 33.3 | 69; 75; 77 | 4 | 36.4 | 50; 71; 71; 74 |
| Sepsis (with multi-organ failure) | 3 | 33.3 | 74; 83; 83 | - | - | - |
| Drug intoxication | 1 | 11.1 | 32 | - | - | - |
| Respiratory insufficiency | - | - | - | 1 | 9.1 | 69 |
| Graft versus host disease | - | - | - | 1 | 9.1 | 67 |
| Fungal pneumonia | - | - | - | 1 | 9.1 | 63 |
| Not documented | - | - | - | 2 | 18.2 | 79; 85 |
| Mean age | 70.1 ± 15.4 | Mean age | 70.4 ± 9.4 | |||
| Pathogen | CAVO (n = 23) | HAVO (n = 22) |
|---|---|---|
| Staphylococcus aureus | 11 (47.8%) | 10 (45.5%) |
| Coagulase-negative staphylococci | 2 (8.7%) | 6 (27.3%) |
| Streptococcus species | 2 (8.7%) | 2 (9.1%) |
| Enterobactericales | 5 (21.7%) | 2 (9.1%) |
| Enterococcus species | 1 (4.3%) (E. faecium) | 2 (9.1%) |
| Other | 2 (8.7%) (Haemophilus parainfluenzae; Cutibacterium avidum) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lang, S.; Frömming, A.; Walter, N.; Freigang, V.; Neumann, C.; Loibl, M.; Ehrenschwender, M.; Alt, V.; Rupp, M. Is There a Difference in Clinical Features, Microbiological Epidemiology and Effective Empiric Antimicrobial Therapy Comparing Healthcare-Associated and Community-Acquired Vertebral Osteomyelitis? Antibiotics 2021, 10, 1410. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111410
Lang S, Frömming A, Walter N, Freigang V, Neumann C, Loibl M, Ehrenschwender M, Alt V, Rupp M. Is There a Difference in Clinical Features, Microbiological Epidemiology and Effective Empiric Antimicrobial Therapy Comparing Healthcare-Associated and Community-Acquired Vertebral Osteomyelitis? Antibiotics. 2021; 10(11):1410. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111410
Chicago/Turabian StyleLang, Siegmund, Astrid Frömming, Nike Walter, Viola Freigang, Carsten Neumann, Markus Loibl, Martin Ehrenschwender, Volker Alt, and Markus Rupp. 2021. "Is There a Difference in Clinical Features, Microbiological Epidemiology and Effective Empiric Antimicrobial Therapy Comparing Healthcare-Associated and Community-Acquired Vertebral Osteomyelitis?" Antibiotics 10, no. 11: 1410. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111410