
Quantifying the Gap between Expected and Actual Rates of Antibiotic Prescribing in British Columbia, Canada

Abstract
:1. Introduction
2. Results
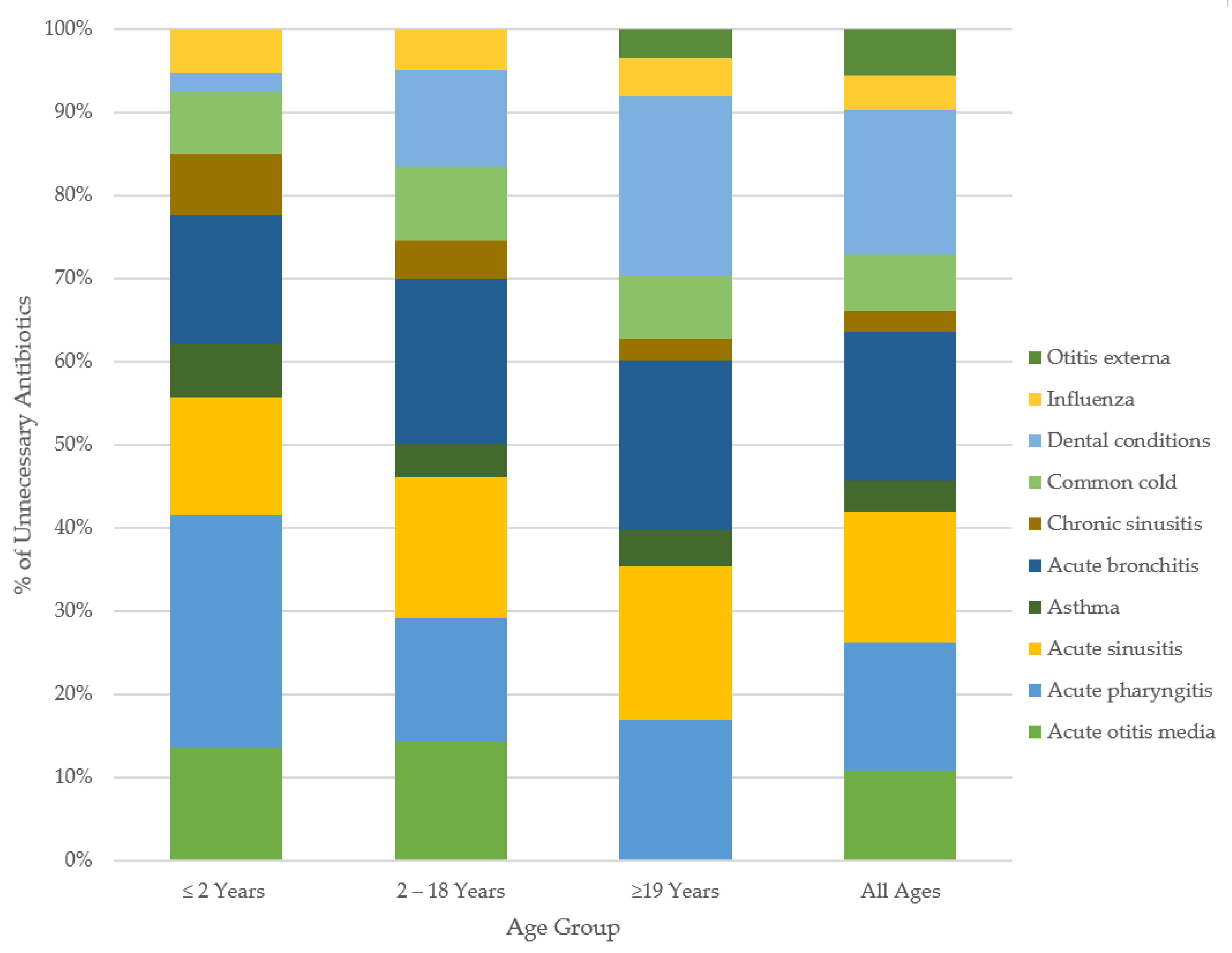
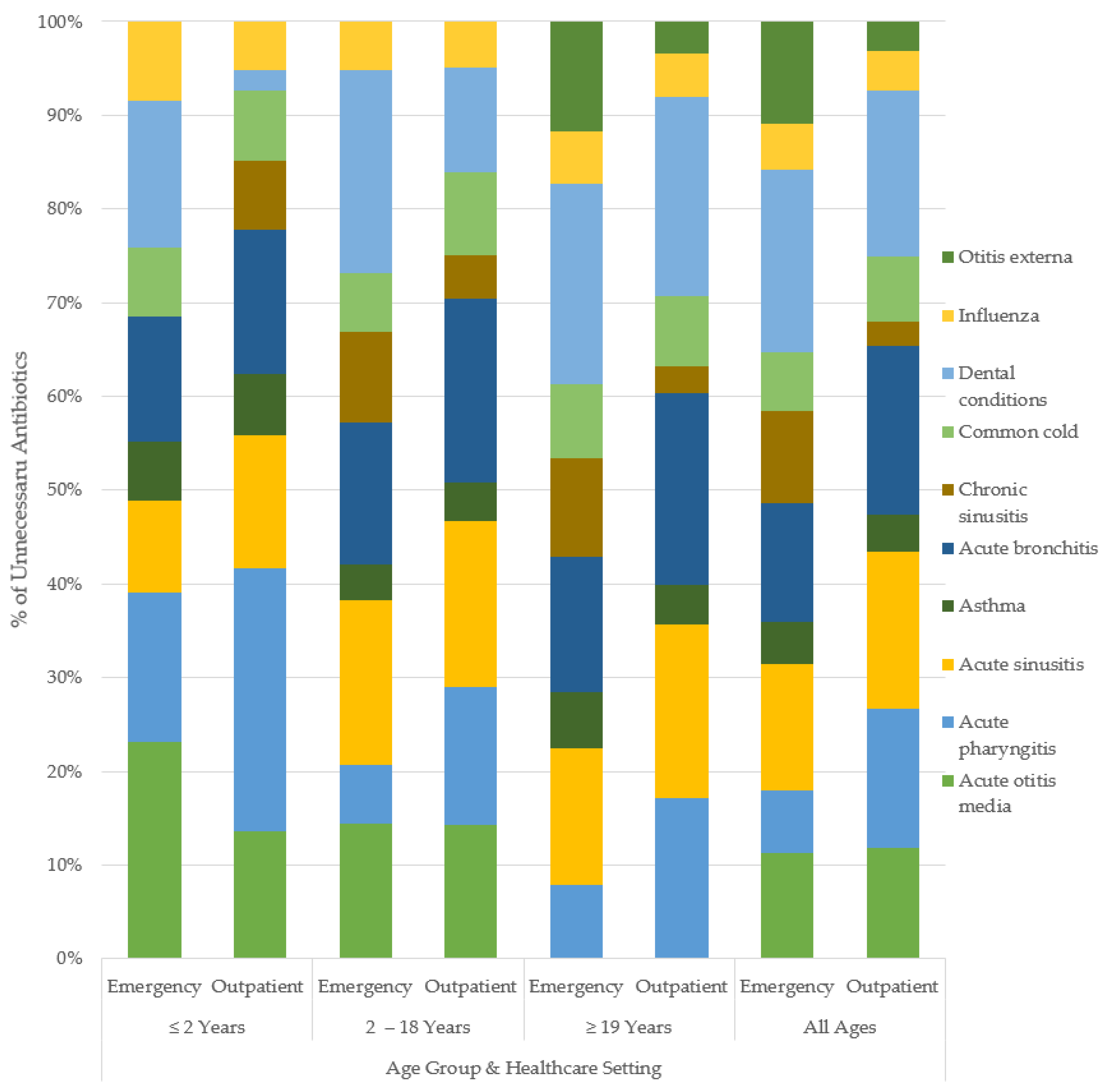
Unnecessary Antibiotic Utilization
3. Discussion
4. Materials and Methods
4.1. Data Sources
4.2. Study Population
4.3. Canadian Expected Prescribing Rates
4.4. Outcomes and Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J.; Bartoces, M.; Enns, E.A.; File, T.M.; Finkelstein, J.A.; Gerber, J.S.; Hyun, D.Y.; Linder, J.A.; et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016, 315, 1864–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolk, F.C.K.; Pouwels, K.B.; Smith, D.R.M.; Robotham, J.V.; Smieszek, T. Antibiotics in primary care in England: Which antibiotics are prescribed and for which conditions? J. Antimicrob. Chemother. 2018, 73, ii2–ii10. [Google Scholar] [CrossRef] [PubMed]
- Davies, S.C. Reducing inappropriate prescribing of antibiotics in English primary care: Evidence and outlook. J. Antimicrob. Chemother. 2018, 73, 833–834. [Google Scholar] [CrossRef]
- Smith, D.R.M.; Dolk, F.C.K.; Pouwels, K.B.; Christie, M.; Robotham, J.V.; Smieszek, T. Defining the appropriateness and inappropriateness of antibiotic prescribing in primary care. J. Antimicrob. Chemother. 2018, 73, ii11–ii18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouwels, K.B.; Dolk, F.C.K.; Pouwels, K.B.; Christie, M.; Robotham, J.V.; Smieszek, T. Actual versus ‘ideal’ antibiotic prescribing for common conditions in English primary care. J. Antimicrob. Chemother. 2018, 73, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Abushaheen, M.A.; Fatani, A.J.; Alosaimi, M.; Mansy, W.; George, M.; Acharya, S.; Rathod, S.; Divakar, D.D.; Jhugroo, C.; Vellappally, S.; et al. Antimicrobial resistance, mechanisms and its clinical significance. Dis. Mon. 2020, 66, 100971. [Google Scholar] [CrossRef] [PubMed]
- Pubic Health Agency of Canada. Canadian Antimicrobial Resistance Surveillance System 2017 Report—Executive Summary. Available online: https://www.canada.ca/en/public-health/services/publications/drugs-health-products/canadian-antimicrobial-resistance-surveillance-system-2017-report-executive-summary.html (accessed on 15 April 2020).
- Rodrigues, A.T.; Roque, F.; Falco, A.; Figueiras, A.; Herdeiro, M.T. Understanding physician antibiotic prescribing behaviour: A systematic review of qualitative studies. Int. J. Antimicrob. Agents 2013, 41, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and Reporting the Delphi Method for Selecting Healthcare Quality Indicators: A Systematic Review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef]
- Humphrey-Murto, S.; Varpio, L.; Wood, T.J.; Gonsalves, C.; Ufholz, L.-A.; Mascioli, K.; Wang, C.; Foth, T. The use of the Delphi and other consensus group methods in medical education research: A review. Acad. Med. 2017, 92, 1491–1498. [Google Scholar] [CrossRef]
- National Centre for Antimicrobial Stewardship and Australian Commission on Safety and Quality in Health Care. Antimicrobial Prescribing Practice in Australian Hospitals: Results of the 2018 Hospital National Antimicrobial Prescribing Survey; ACSQHC: Sydney, Australia, 2020.
- Ingram, P.R.; Seet, J.M.; Budgeon, C.A.; Murray, R. Point-prevalence study of inappropriate antibiotic use at a tertiary Australian hospital. Intern. Med. J. 2012, 42, 719–721. [Google Scholar] [CrossRef]
- Salzo, A.; Ripabelli, G.; Sammarco, M.L.; Mariano, A.; Niro, C.; Tamburro, M. Healthcare-Associated infections and antibiotics consumption: A comparison of point prevalence studies and intervention strategies. Hosp Top. 2021, 99, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.H.-C.; Langford, B.; Ha, R.; Garber, G.; Daneman, N.; Johnstone, J.; McIsaac, W.; Sharpe, S.; Tu, K.; Schwartz, K.L. Defining appropriate antibiotic prescribing in primary care: A modified Delphi panel approach. Off. J. Assoc. Med. Microbiol. Infect. Dis. Can. 2020, 5, 61–69. [Google Scholar] [CrossRef] [Green Version]
- O’Doherty, J.; Leader, L.F.W.; O’Regan, A.; Dunne, C.; Puthoopparambil, S.J.; O’Connor, R. Over prescribing of antibiotics for acute respiratory tract infections; a qualitative study to explore Irish general practitioners’ perspectives. BMC Fam. Pract. 2019, 20, 27. [Google Scholar] [CrossRef]
- Schwartz, K.L.; Langford, B.J.; Daneman, N.; Chen, B.; Brown, K.A.; McIsaac, W.; Tu, K.; Candido, E.; Johnstone, J.; Leung, V.; et al. Unnecessary antibiotic prescribing in a Canadian primary care setting: A descriptive analysis using routinely collected electronic medical record data. CMAJ Open 2020, 8, E360–E369. [Google Scholar] [CrossRef] [PubMed]
- Wade, T.; McCormack, S. Interventions to Influence the Use of Antibiotics for Acute Upper Respiratory Tract Infections; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2021. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK572012/ (accessed on 8 September 2021).
- Roberts, R.M.; Hersh, A.L.; Shapiro, D.J.; Fleming-Dutra, K.E.; Hicks, L.A. Antibiotic Prescriptions Associated with Dental-Related Emergency Department Visits. Ann. Emerg. Med. 2019, 74, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Marra, F.; George, D.; Chong, M.; Sutherland, S.; Patrick, D.M. Antibiotic prescribing by dentists has increased. J. Am. Dent. Assoc. 2016, 147, 320–327. [Google Scholar] [CrossRef] [Green Version]
- Thompson, W.; Teoh, L.; Hubbard, C.C.; Marra, F.; Patrick, D.M.; Mamun, A.; Campbell, A.; Suda, K.J. Patterns of dental antibiotic prescribing in 2017: Australia, England, United States, and British Columbia (Canada). Infect. Control Hosp. Epidemiol. 2021, 5, 1–8. [Google Scholar] [CrossRef]
- Graber, C.J.; Goetz, M.B. Next steps for antimicrobial stewardship. Lancet Infect. Dis. 2016, 16, 764–765. [Google Scholar] [CrossRef] [Green Version]
- Majumder, M.A.A.; Rahman, S.; Cohall, D.; Bharatha, A.; Singh, K.; Haque, M.; Gittens-St Hilaire, M. Antimicrobial stewardship: Fighting antimicrobial resistance and protecting global public health. Infect. Drug Resist. 2020, 13, 4713–4738. [Google Scholar] [CrossRef]
- Gulliford, M.C.; Prevost, A.T.; Charlton, J.; Juszczyk, D.; Soames, J.; McDermott, L.; Sultana, K.; Wright, M.; Fox, R.; Hay, A.D.; et al. Effectiveness and safety of electronically delivered prescribing feedback and decision support on antibiotic use for respiratory illness in primary care: REDUCE cluster randomised trial. BMJ 2019, 364, l236. [Google Scholar] [CrossRef] [Green Version]
- Cadieux, G.; Tamblyn, R. Accuracy of physician billing claims for identifying acute respiratory infections in primary care. Health Serv. Res. 2008, 43, 2223–2238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tieder, J.S.; Hall, M.; Auger, K.A.; Hain, P.D.; Jerardi, K.E.; Myers, A.L.; Rahman, S.S.; Williams, D.J.; Shah, S.S. Accuracy of administrative billing codes to detect urinary tract infection hospitalizations. Pediatrics. 2011, 128, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, K.L.; Brown, K.A.; Etches, J.; Langford, B.J.; Daneman, N.; Tu, K.; Johnstone, J.; Achonu, C.; Garber, G. Predictors and variability of antibiotic prescribing amongst family physicians. J. Antimicrob. Chemother. 2019, 74, 2098–2105. [Google Scholar] [CrossRef] [PubMed]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Singer, A.C.; Xu, Q.; Keller, V.D.J. Translating antibiotic prescribing into antibiotic resistance in the environment: A hazard characterisation case study. PLoS ONE 2019, 14, e0221568. [Google Scholar] [CrossRef] [Green Version]
- He, M.; Miyajima, F.; Roberts, P.; Ellison, L.; Pickard, D.J.; Martin, M.J.; Connor, T.R.; Harris, S.R.; Fairley, D.; Bamford, K.B.; et al. Emergence and global spread of epidemic healthcare—Associated Clostridium difficile. Nat. Genet. 2013, 45, 109–113. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2014. Annual Report of The European Antimicrobial Resistance Surveillance Network (EARS-Net); ECDC: Stockholm, Sweden, 2015. [Google Scholar]
- Njoku, J.C.; Hermsen, E.D. Antimicrobial stewardship in the intensive care unit: A focus on potential pitfalls. J. Pharm. Pract. 2010, 23, 50–60. [Google Scholar] [CrossRef] [PubMed]
- di Tella, D.; Tamburro, M.; Guerrizio, G.; Fanelli, I.; Sammarco, M.L.; Ripabelli, G. Molecular epidemiological insights into colistin-resistant and carbapenemases-producing clinical Klebsiella pneumoniae isolates. Infect Drug Resist. 2019, 12, 3783–3795. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report 2021; World Health Organization: Geneva, Switzerland, 2021; Licence: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- U.S. Department of Health and Human Services. CDC. Antibiotic Resistance Threats in The United States, 2019; CDC Atlanta: Atlanta, GA, USA, 2019.
- Mohsen, S.; Dickinson, J.A.; Somayaji, R. Update on the adverse effects of antimicrobial therapies in community practice. Can. Fam. Phys. 2020, 66, 651–659. [Google Scholar]
- Do Bugs Need Drugs? Do Bugs Need Drugs. 2021. Available online: http://www.dobugsneeddrugs.org (accessed on 27 August 2021).
- McKay, R.M.; Vrbova, L.; Fuertes, E.; Chong, M.; David, S.; Dreher, K.; Purych, D.; Blondel-Hill, E.; Henry, B.; Marra, F.; et al. Evaluation of the Do Bugs Need Drugs? program in British Columbia: Can we curb antibiotic prescribing? Can. J. Infect. Dis. Med. Microbiol. 2011, 22, 19–24. [Google Scholar] [CrossRef]
- Saatchi, A.; Morris, A.M.; Patrick, D.M.; Mccormack, J.; Reyes, R.C.; Morehouse, P.; Reid, J.; Shariff, S.; Povitz, M.; Silverman, M.; et al. Outpatient antibiotic use in British Columbia, Canada: Reviewing major trends since 2000. JAC-Antimicrob. Resist. 2021, 3, dlab116. [Google Scholar] [CrossRef] [PubMed]
- BC Stats. Population Estimates, Province of British Columbia. 2020. Available online: https://www2.gov.bc.ca/gov/content/data/statistics/people-population-community/population/population-estimates (accessed on 6 November 2020).
- BC Ministry of Health. PharmaNet. V2; BC Ministry of Health: BC, Canada, Data Extract. Data Stewardship Committee. 2020. Available online: http://www.popdata.bc.ca/data (accessed on 1 November 2021).
- British Columbia Ministry of Health. Medical Services Plan (MSP) Payment Information File. V2; Population Data BC: BC, Canada, Data Extract. MOH. 2011. Available online: http://www.popdata.bc.ca/data (accessed on 1 November 2021).
- Canadian Institute for Health Information. National Ambulatory Care Reporting System. V2; Population Data BC: BC, Canada, Data Extract. MOH. 2020; Available online: http://www.popdata.bc.ca/data (accessed on 1 November 2021).
- British Columbia Ministry of Health. Consolidation File (MSP Registration & Premium Billing). V2; Population Data BC: BC, Canada, Data Extract. MOH. 2020. Available online: http://www.popdata.bc.ca/data (accessed on 1 November 2021).
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D.; Burnand, B.; LaCalle, J.R. The Rand/Ucla Appropriateness Method User’s Manual; Fitch, K., Ed.; Rand Corporation: Santa Monica, CA, USA, 2001. [Google Scholar]
- WHO Collaborating Centre for Drug Statistics Methodology and Folkehelseinstituttet (Noruega). Guidelines for ATC Classification and DDD Assignment 2011; Norwegian Institute of Public Health: Oslo, Norway, 2010; Available online: http://www.whocc.no/filearchive/publications/2011guidelines.pdf (accessed on 3 May 2019).
- CDC. International Classification of Diseases, Ninth Revision (ICD-9). 2019. Available online: https://www.cdc.gov/nchs/icd/icd9.html (accessed on 28 April 2019).
- Ministry of Health. Diagnostic Code Descriptions (ICD-9), Province of British Columbia. 2021. Available online: https://www2.gov.bc.ca/gov/content/health/practitionerprofessional-resources/msp/physicians/diagnostic-code-descriptions-icd-9 (accessed on 3 May 2019).
- Canadian Institute for Health Information. Canadian Coding Standards for Version 2018 ICD-10-CA and CCI; CIHI: Ottawa, ON, Canada, 2018. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Outpatient Care Setting 2000–2018 | Emergency Care Setting 2012–2018 | |
|---|---|---|
| Total number of patients | 3,240,894 | 249,691 |
| Average patients per year | 405,685 | 41,422 |
| Age (years) | ||
| Mean | 41.62 | 45.17 |
| Standard Deviation | 25.44 | 24.95 |
| <2 Years | 378,927 (4.92%) | 14,600 (5.04%) |
| 2–18 Years | 1,520,761 (19.73%) | 40,057 (13.81%) |
| ≥19 Years | 5,808,328 (75.35%) | 235,297 (81.15%) |
| Sex | ||
| Female | 4,792,943 (62.18%) | 165,137 (56.95%) |
| Male | 2,914,119 (37.81%) | 124,807 (43.04%) |
| Income Quintile | ||
| Quintile 1 (lowest) | 1,644,735 (21.34%) | 71,376 (24.62%) |
| Quintile 2 | 1,589,201 (20.62%) | 61,103 (21.07%) |
| Quintile 3 | 1,516,110 (19.67%) | 56,650 (19.54%) |
| Quintile 4 | 1,465,429 (19.01%) | 52,771 (18.2%) |
| Quintile 5 (highest) | 1,349,927 (17.51%) | 43,419 (14.97%) |
| Missing | 133,309 (1.73%) | 3498 (1.21%) |
| Geographic Region | ||
| Rural | 1,274,318 (16.53%) | 10,800 (3.72%) |
| Urban | 6,139,403 (79.65%) | 268,037 (92.44%) |
| Missing | 294,295 (3.82%) | 11,117 (3.83%) |
| Health Authority | ||
| Interior | 1,259,910 (16.35%) | 4879 (1.68%) |
| Fraser | 2,968,609 (38.51%) | 164,177 (56.62%) |
| Vancouver Coastal | 1,648,260 (21.38%) | 88,229 (30.43%) |
| Vancouver Island | 1,314,339 (17.05%) | 21,634 (7.46%) |
| Northern | 493,305 (6.4%) | 9912 (3.42%) |
| Missing | 15,968 (0.21%) | 768 (0.26%) |
| Classification | Diagnosis | Outpatient Care Setting 1 | Emergency Care Setting 2 | ||
|---|---|---|---|---|---|
| Prescriptions Issued 3 | Total Physician Visits 4 | Prescriptions Issued | Total Physician Visits | ||
| Tier 1: Always indicated (100%) | Pneumonia | 1,048,153 (3.65%) | 2,525,744 (3.25%) | 69,424 (14.12%) | 97,538 (19.84%) |
| Pyelonephritis | 200,042 (0.70%) | 395,291 (0.51%) | 24,453 (4.97%) | 31,131 (6.33%) | |
| Non-Purulent SSTI | 2,668,652 (9.30%) | 4,762,565 (6.13%) | 132,539 (26.96%) | 180,189 (36.65%) | |
| Reproductive tract | 367,126 (1.28%) | 2,502,766 (3.22%) | 2576 (0.52%) | 2754 (0.56%) | |
| Urinary tract infections (aged ≤18 y) | 560,958 (1.96%) | 957,393 (1.23%) | 13,388 (2.72%) | 16,034 (3.26%) | |
| Tier 2a: Frequently indicated (51–99%) | Urinary tract infections (aged >18 y) | 6,140,403 (21.41%) | 9,724,013 (12.51%) | 99,168 (20.17%) | 118,149 (24.03%) |
| Prostatitis | 110,482 (0.39%) | 381,996 (0.49%) | 1713 (0.35%) | 2312 (0.47%) | |
| Epididymo-orchitis | 73,955 (0.26%) | 173,088 (0.22%) | 5268 (1.07%) | 6947 (1.41%) | |
| Tier 2b: Sometimes indicated (21–50%) | Purulent SSTI | 1,443,819 (5.03%) | 6,964,320 (8.96%) | 33,650 (6.84%) | 51,538 (10.48%) |
| Acute Otitis Media | 2,343,863 (8.17%) | 3,899,643 (5.02%) | 23,823 (4.85%) | 31,265 (6.36%) | |
| Pharyngitis (aged ≤2 y) | 81,486 (0.28%) | 105,334 (0.14%) | 619 (0.13%) | 1267 (0.26%) | |
| Tier 2c: Rarely indicated (1–20%) | Acute sinusitis | 2,635,709 (9.19%) | 3,990,765 (5.13%) | 6281 (1.28%) | 8949 (1.82%) |
| Chronic sinusitis | 404,106 (1.41%) | 1,883,735 (2.42%) | 535 (0.11%) | 1068 (0.22%) | |
| Bronchitis | 3,406,425 (11.88%) | 5,746,837 (7.39%) | 14,981 (3.05%) | 26,263 (5.34%) | |
| Dental Conditions | 353,089 (1.23%) | 649,259 (0.84%) | 19,911 (4.05%) | 25,275 (5.14%) | |
| Otitis Externa (aged >18 y) | 210,929 (0.74%) | 2,121,058 (2.73%) | 2874 (0.58%) | 6707 (1.36%) | |
| Pharyngitis (aged >2 y) | 1,696,442 (5.91%) | 2,264,601 (2.91%) | 20,718 (4.21%) | 36,475 (7.42%) | |
| Tier 3: Never indicated (0%) | Asthma | 837,508 (2.92%) | 7,493,929 (9.64%) | 7875 (1.6%) | 45,529 (9.26%) |
| Common Cold | 3,746,608 (13.06%) | 18,788,085 (24.16%) | 6685 (1.36%) | 27,361 (5.57%) | |
| Influenza | 218,802 (0.76%) | 1,803,191 (2.32%) | 4150 (0.84%) | 21,578 (4.39%) | |
| Otitis Externa (aged ≤18 y) | 134,164 (0.47%) | 620,984 (0.80%) | 971 (0.20%) | 2339 (0.48%) | |
| Overall | All Indications 5 | 28,682,721 | 77,754,597 | 491,602 | 740,668 |
| Diagnoses | Age (yr); Number of Outpatient Care Visits | Age (yr); Number of Emergency Care Visits | Age (yr); Outpatient Prescribing rate/% Unnecessary 1 | Age (yr); Emergency Prescribing rate/% Unnecessary | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <2 | 2–18 | ≥19 | All Ages | <2 | 2–18 | ≥19 | All Ages | <2 | 2–18 | ≥19 | All Ages | <2 | 2–18 | ≥19 | All Ages | |
| Acute otitis media | 731,530 | 1,797,583 | - | 2,529,113 | 6546 | 16,367 | - | 31,265 | 68.8/28.6 | 66.0/36.0 | - | 60.1/33.9 | 84.6/44.6 | 73.4/43.3 | - | 76.2/43.6 |
| Acute pharyngitis | 105,334 | 1,047,467 | 1,217,134 | 2,369,935 | 1267 | 10,950 | 25,525 | 37,742 | 77.4/59.4 | 77.3/37.3 | 72.8/44.8 | 75.0/42.2 | 48.9/30.9 | 58.6/18.6 | 56.0/28.0 | 56.5/25.4 |
| Acute sinusitis | 57,725 | 435,409 | 3,497,631 | 3,990,765 | 86 | 584 | 8279 | 8949 | 49.7/29.7 | 62.7/44.7 | 66.7/48.7 | 66.0/47.8 | 38.9/18.9 | 72.8/52.8 | 70.5/52.5 | 70.3/52.2 |
| Asthma | 306,349 | 1,873,975 | 5,313,605 | 7,493,929 | 4148 | 14,629 | 26,752 | 45,529 | 14.0/14.0 | 10.2/10.2 | 11.3/11.3 | 11.2/11.2 | 12.0/12.0 | 11.3/11.3 | 21.4/21.4 | 17.3/17.3 |
| Bronchitis | 380,898 | 946,026 | 4,419,913 | 5,746,837 | 1665 | 2350 | 22,248 | 26,263 | 37.5/32.5 | 57.8/49.8 | 61.5/53.5 | 59.3/51.5 | 30.8/25.8 | 53.2/45.2 | 59.4/51.4 | 57.0/49.2 |
| Chronic sinusitis | 3055 | 73,952 | 1,806,728 | 1,883,735 | - | 42 | 1031 | 1073 | 29.5/15.5 | 25.4/11.4 | 21.3/7.3 | 21.5/7.5 | - | 42.9/28.9 | 51.9/37.9 | 51.5/37.5 |
| Common cold | 1,572,357 | 3,501,575 | 13,714,153 | 18,788,085 | 3550 | 5654 | 18,157 | 27,361 | 15.8/15.8 | 22.5/22.5 | 19.7/19.7 | 19.9/19.9 | 14.3/14.3 | 18.9/18.9 | 28.1/28.1 | 24.4/24.4 |
| Dental Conditions | 18,444 | 93,420 | 537,395 | 649,259 | 234 | 2473 | 22,568 | 25,275 | 8.5/4.5 | 32.3/28.3 | 59.8/55.8 | 58.4/50.4 | 34.2/30.2 | 68.5/64.5 | 80.4/76.4 | 78.8/74.8 |
| Epididymo-orchitis | - | 11,874 | 159,596 | 171,470 | - | 658 | 6274 | 6932 | - | 33.3/0.0 | 43.8/0.0 | 42.3/0.0 | - | 62.5/0.0 | 77.3/0.0 | 75.8/0.0 |
| Influenza | 94,316 | 382,918 | 1,325,957 | 1,803,191 | 789 | 3497 | 17,292 | 21,578 | 11.0/11.0 | 12.3/12.3 | 12.2/12.2 | 12.1/12.1 | 16.3/16.3 | 15.7/15.7 | 20.1/20.1 | 19.2/19.2 |
| Non-purulent SSTI | 72,825 | 443,730 | 4,246,010 | 4,762,565 | 1426 | 8698 | 170,065 | 180,189 | 44.2/0.0 | 58.4/0.0 | 56.0/0.0 | 56.0/0.0 | 81.5/0.0 | 83.7/0.0 | 73.0/0.0 | 73.6/0.0 |
| Otitis externa | - | - | 2,121,058 | 2,121,058 | - | - | 6707 | 6707 | - | - | 9.9/8.9 | 9.9/8.9 | - | - | 42.9/41.9 | 42.9/41.9 |
| Pneumonia | 99,460 | 215,402 | 2,210,882 | 2,525,744 | 7219 | 12,909 | 77,410 | 97,538 | 57.2/0.0 | 64.9/0.0 | 38.5/0.0 | 41.5/0.0 | 84.7/0.0 | 92.3/0.0 | 66.4/0.0 | 71.2/0.0 |
| Prostatitis | - | - | 379,608 | 379,608 | - | - | 2312 | 2312 | - | - | 34.0/0.0 | 34.0/0.0 | - | - | 74.1/0.0 | 74.1/0.0 |
| Purulent SSTI | 106,928 | 571,744 | 6,285,648 | 6,964,320 | 1145 | 5257 | 45,136 | 51,538 | 33.0/0.0 | 39.4/0.0 | 18.8/0.0 | 20.7/0.0 | 64.3/14.3 | 63.6/13.6 | 65.5/35.5 | 65.3/32.8 |
| Pyelonephritis | 15,826 | 31,366 | 348,099 | 395,291 | 157 | 1742 | 29,232 | 31,131 | 43.8/0.0 | 54.1/0.0 | 50.6/0.0 | 50.6/0.0 | 89.8/0.0 | 87.9/0.0 | 77.9/0.0 | 78.5/0.0 |
| Reproductive tract infections | 6443 | 126,475 | 2,369,848 | 2,502,766 | - | 169 | 2585 | 2754 | 6.5/0.0 | 16.1/0.0 | 14.6/0.0 | 14.7/0.0 | - | 93.9/0.0 | 93.6/0.0 | 93.5/0.0 |
| Urinary tract infections | 98,858 | 858,535 | 9,724,013 | 10,681,406 | 4528 | 11,506 | 118,149 | 134,183 | 42.8/0.0 | 60.4/0.0 | 63.1/0.0 | 62.7/0.0 | 80.8/0.0 | 84.6/0.0 | 83.9/0.0 | 83.9/0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saatchi, A.; Yoo, J.-W.; Schwartz, K.L.; Silverman, M.; Morris, A.M.; Patrick, D.M.; McCormack, J.; Marra, F. Quantifying the Gap between Expected and Actual Rates of Antibiotic Prescribing in British Columbia, Canada. Antibiotics 2021, 10, 1428. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111428
Saatchi A, Yoo J-W, Schwartz KL, Silverman M, Morris AM, Patrick DM, McCormack J, Marra F. Quantifying the Gap between Expected and Actual Rates of Antibiotic Prescribing in British Columbia, Canada. Antibiotics. 2021; 10(11):1428. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111428
Chicago/Turabian StyleSaatchi, Ariana, Ji-Won Yoo, Kevin L. Schwartz, Michael Silverman, Andrew M. Morris, David M. Patrick, James McCormack, and Fawziah Marra. 2021. "Quantifying the Gap between Expected and Actual Rates of Antibiotic Prescribing in British Columbia, Canada" Antibiotics 10, no. 11: 1428. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111428