
Population Pharmacokinetics Analysis of Amikacin Initial Dosing Regimen in Elderly Patients

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Clinical Data
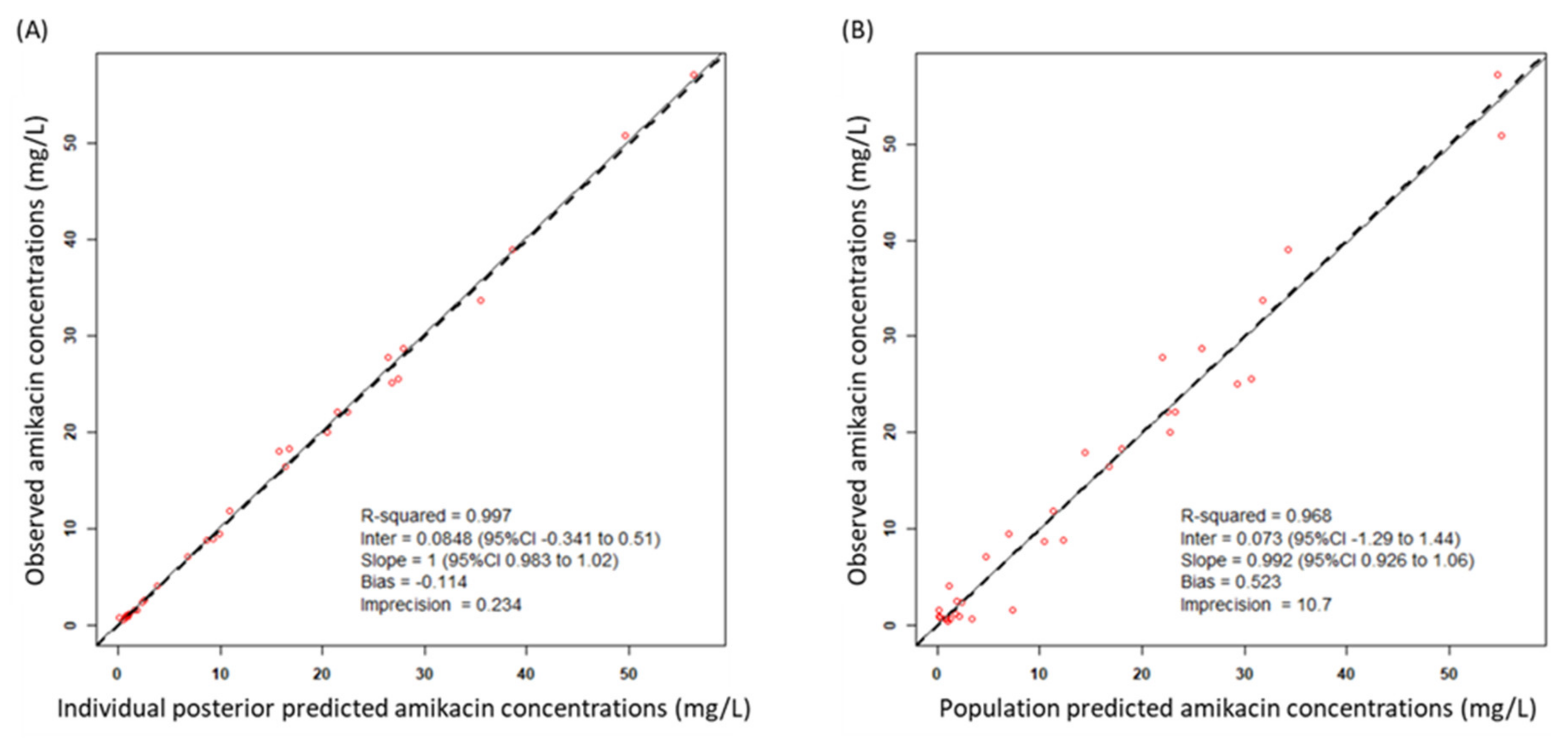
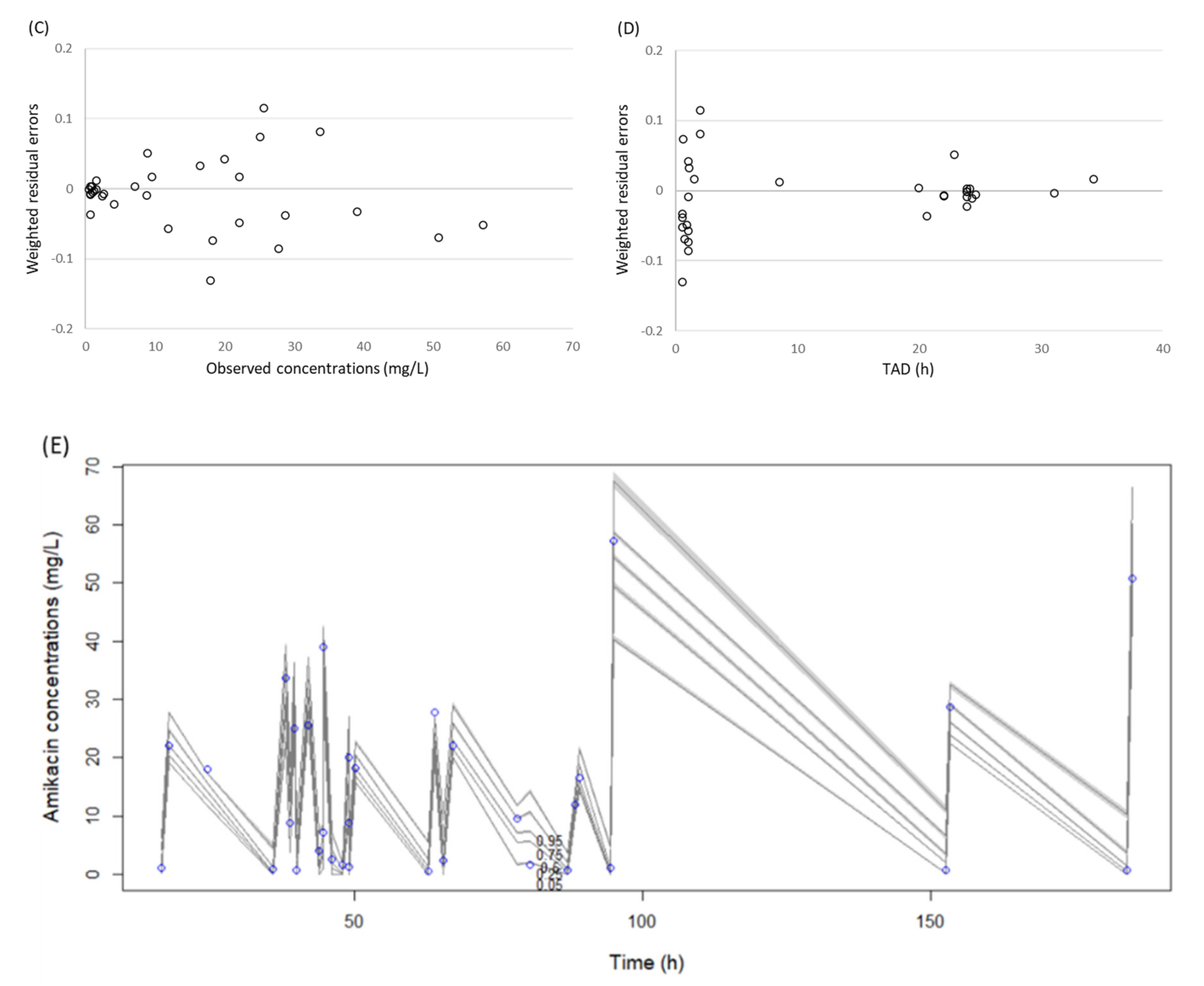
2.2. Pharmacokinetic Modeling
2.3. Probability of Target Attainment (PTA)
2.4. Fractional Target Attainment
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Data Collection
4.3. Population Pharmacokinetic Modeling
4.4. Population Pharmacokinetic Covariate Building
4.5. Model Evaluation
4.6. Assessment of Amikacin Dosing Regimens by Monte Carlo Simulation
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strausbaugh, L.J. Emerging Health Care-Associated Infections in the Geriatric Population. Emerg. Infect. Dis. 2001, 7, 268–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UN World Population Prospects: The 2019 Revision. Available online: https://population.un.org/wpp/ (accessed on 19 January 2021).
- Jackson, M.L.; Neuzil, K.M.; Thompson, W.W.; Shay, D.K.; Yu, O.; Hanson, C.A.; Jackson, L.A. The Burden of Community-Acquired Pneumonia in Seniors: Results of a Population-Based Study. Clin. Infect. Dis. 2004, 39, 1642–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, P.A.; Rapuano, C.; Adrignolo, A.; Shaw, B. Nosocomial Infections Decade-Specific Risk. Infect. Control. 1983, 4, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Defez, C.; Fabbro-Peray, P.; Bouziges, N.; Gouby, A.; Mahamat, A.; Daurès, J.; Sotto, A. Risk factors for multidrug-resistant Pseudomonas aeruginosa nosocomial infection. J. Hosp. Infect. 2004, 57, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Turnheim, K. Drug therapy in the elderly. Exp. Gerontol. 2004, 39, 1731–1738. [Google Scholar] [CrossRef]
- Kumana, C.R.; Yuen, K.Y. Parenteral aminoglycoside therapy. Selection, administration and monitoring. Drugs 1994, 47, 902–913. [Google Scholar] [CrossRef]
- Zelenitsky, S.A.; Harding, G.K.M.; Sun, S.; Ubhi, K.; Ariano, R.E. Treatment and outcome of Pseudomonas aeruginosa bacteraemia: An antibiotic pharmacodynamic analysis. J. Antimicrob. Chemother. 2003, 52, 668–674. [Google Scholar] [CrossRef]
- Moore, R.D.; Lietman, P.S.; Smith, C.R. Clinical Response to Aminoglycoside Therapy: Importance of the Ratio of Peak Concentration to Minimal Inhibitory Concentration. J. Infect. Dis. 1987, 155, 93–99. [Google Scholar] [CrossRef]
- Zaske, D.E.; Strate, R.G.; Kohls, P.R. Amikacin Pharmacokinetics: Wide Interpatient Variation in 98 Patients. J. Clin. Pharmacol. 1991, 31, 158–163. [Google Scholar] [CrossRef]
- Boucher, B.A.; Coffey, B.C.; Kuhl, D.A.; Tolley, E.A.; Fabian, T.C. Algorithm for assessing renal dysfunction risk in critically ill trauma patients receiving aminoglycosides. Am. J. Surg. 1990, 160, 473–480. [Google Scholar] [CrossRef]
- Alqahtani, S.; Abouelkheir, M.; Alsultan, A.; ElSharawy, Y.; Alkoraishi, A.; Osman, R.; Mansy, W. Optimizing Amikacin Dosage in Pediatrics Based on Population Pharmacokinetic/Pharmacodynamic Modeling. Pediatr. Drugs 2018, 20, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Hagihara, M.; Hirai, J.; Sakanashi, D.; Suematsu, H.; Nishiyama, N.; Koizumi, Y.; Yamagishi, Y.; Matsuura, K.; Koizumi, Y. Evaluation of Amikacin Pharmacokinetics and Pharmacodynamics for Optimal Initial Dosing Regimen. Drugs R&D 2017, 17, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Kadomura, S. Therapeutic Drug Monitoring of Antimicrobial Agents. Rinsho byori. Jpn. J. Clin. Pathol. 2016, 64, 1367–1372. [Google Scholar]
- Yu, T.; Stockmann, C.; Healy, D.P.; Olson, J.; Wead, S.; Neely, A.N.; Kagan, R.J.; Spigarelli, M.G.; Sherwin, C.M.T. Determination of Optimal Amikacin Dosing Regimens for Pediatric Patients With Burn Wound Sepsis. J. Burn. Care Res. 2015, 36, e244–e252. [Google Scholar] [CrossRef]
- Guido, P.C.; Perez, M.; Halac, A.; Ferrari, M.; Ibarra, M.; Licciardone, N.; Castaños, C.; Gravina, L.P.; Jimenez, C.; Bournissen, F.G.; et al. Population pharmacokinetics of amikacin in patients with pediatric cystic fibrosis. Pediatr. Pulmonol. 2019, 54, 1801–1810. [Google Scholar] [CrossRef]
- Belfayol, L.; Talon, P.; Eveillard, M.; Alet, P.; Fauvette, F. Pharmacokinetics of once-daily amikacin in pediatric patients. Clin. Microbiol. Infect. 1996, 2, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Alhadab, A.A.; Ahmed, M.A.; Brundage, R.C. Amikacin Pharmacokinetic-Pharmacodynamic Analysis in Pediatric Cancer Patients. Antimicrob. Agents Chemother. 2018, 62, 01781-17. [Google Scholar] [CrossRef] [Green Version]
- Kenyon, C.F.; Knoppert, D.C.; Lee, S.K.; Vandenberghe, H.M.; Chance, G.W. Amikacin pharmacokinetics and suggested dosage modifications for the preterm infant. Antimicrob. Agents Chemother. 1990, 34, 265–268. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Smits, A.; Wang, Y.; Renard, M.; Wead, S.; Kagan, R.J.; Healy, D.P.; De Cock, P.; Allegaert, K.; Sherwin, C.M. Impact of Disease on Amikacin Pharmacokinetics and Dosing in Children. Ther. Drug Monit. 2019, 41, 44–52. [Google Scholar] [CrossRef]
- Vogelstein, B.; Kowarski, A.A.; Lietman, P.S. The pharmacokinetics of amikacin in children. J. Pediatr. 1977, 91, 333–339. [Google Scholar] [CrossRef]
- Padovani, E.M.; Pistolesi, C.; Fanos, V.; Messori, A.; Martini, N. Pharmacokinetics of Amikacin in Neonates. Dev. Pharmacol. Ther. 1993, 20, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Burdet, C.; Pajot, O.; Couffignal, C.; Armand-Lefèvre, L.; Foucrier, A.; Laouénan, C.; Wolff, M.; Massias, L.; Mentré, F. Population pharmacokinetics of single-dose amikacin in critically ill patients with suspected ventilator-associated pneumonia. Eur. J. Clin. Pharmacol. 2015, 71, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boidin, C.; Bourguignon, L.; Cohen, S.; Roger, C.; Lefrant, J.-Y.; Roberts, M.S.; Allaouchiche, B.; Lepape, A.; Friggeri, A.; Goutelle, S. Amikacin Initial Dose in Critically Ill Patients: A Nonparametric Approach To Optimize A Priori Pharmacokinetic/Pharmacodynamic Target Attainments in Individual Patients. Antimicrob. Agents Chemother. 2019, 63, 00993-19. [Google Scholar] [CrossRef] [Green Version]
- Illamola, S.; Huynh, H.Q.; Liu, X.; Bhakta, Z.N.; Sherwin, C.M.; Liou, T.G.; Carveth, H.; Young, D.C. Population Pharmacokinetics of Amikacin in Adult Patients with Cystic Fibrosis. Antimicrob. Agents Chemother. 2018, 62, e00877-18. [Google Scholar] [CrossRef] [Green Version]
- Thirion, D.; Pasche, V.; Matouk, E.; Marsot, A. Amikacin nomogram for treatment of adult cystic fibrosis exacerbations based on an external evaluation of a population pharmacokinetic model. Pediatr. Pulmonol. 2020, 55, 1154–1160. [Google Scholar] [CrossRef]
- Debord, J.; Charmes, J.P.; Marquet, P.; Merle, L.; Lachâtre, G. Population pharmacokinetics of amikacin in geriatric patients studied with the NPEM-2 algorithm. Int. J. Clin. Pharmacol. Ther. 1997, 35. [Google Scholar]
- Illamola, S.; Sherwin, C.M.; Van Hasselt, J.G.C. Clinical Pharmacokinetics of Amikacin in Pediatric Patients: A Comprehensive Review of Population Pharmacokinetic Analyses. Clin. Pharmacokinet. 2018, 57, 1217–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aréchiga-Alvarado, N.A.; Medellín-Garibay, S.E.; Milán-Segovia, R.D.C.; Ortiz-Álvarez, A.; Magaña-Aquino, M.; Romano-Moreno, S. Population Pharmacokinetics of Amikacin Administered Once Daily in Patients with Different Renal Functions. Antimicrob. Agents Chemother. 2020, 64, 02178-19. [Google Scholar] [CrossRef]
- Romano, S.; Gatta, M.D.M.F.D.; Calvo, V.; Mendez, E.; Domínguez-Gil, A.; Lanao, J.M. Influence of Clinical Diagnosis in the Population Pharmacokinetics of Amikacin in Intensive Care Unit Patients. Clin. Drug Investig. 1998, 15, 435–444. [Google Scholar] [CrossRef]
- Romano, S.; De Gatta, M.M.F.; Calvo, M.V.; Caballero, D.; Dominguez-Gil, A.; Lanao, J.M. Population pharmacokinetics of amikacin in patients with haematological malignancies. J. Antimicrob. Chemother. 1999, 44, 235–242. [Google Scholar] [CrossRef]
- Vanhaeverbeek, M.; Siska, G.; Herchuelz, A. Pharmacokinetics of once-daily amikacin in elderly patients. J. Antimicrob. Chemother. 1993, 31, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Tulkens, P.M. Pharmacokinetic and toxicological evaluation of a once-daily regimen versus conventional schedules of netilmicin and amikacin. J. Antimicrob. Chemother. 1991, 27, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Van Der Auwera, P. Pharmacokinetic evaluation of single daily dose amikacin. J. Antimicrob. Chemother. 1991, 27, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Yasuhara, H.; Kobayashi, S.; Sakamoto, K.; Kamijo, K. Pharmacokinetics of Amikacin and Cephalothin in Bedridden Elderly Patients. J. Clin. Pharmacol. 1982, 22, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, A. Altered pharmacokinetics in the elderly. Jpn. J. Clin. Pharmacol. Ther. 2008, 39, 2–5. [Google Scholar] [CrossRef]
- Taniguchi, H. Assessment of fluid status in nutrient management. J. Jap. Soc. Parenter. Enteral Nutr. 2017, 32, 1126-30. [Google Scholar]
- Roger, C.; Wallis, S.C.; Muller, L.; Saissi, G.; Lipman, J.; Lefrant, J.-Y.; Roberts, M.S. Influence of Renal Replacement Modalities on Amikacin Population Pharmacokinetics in Critically Ill Patients on Continuous Renal Replacement Therapy. Antimicrob. Agents Chemother. 2016, 60, 4901–4909. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, B.; Robbins, P.; Livornese, L.L. Use of Antibacterial Agents in Renal Failure. Med. Clin. North Am. 2011, 95, 677–702. [Google Scholar] [CrossRef]
- Prins, J.M.; Büller, H.R.; Speelman, P.; Kuijper, E.J.; Tange, R.A. Once versus thrice daily gentamicin in patients with serious infections. Lancet 1993, 341, 335–339. [Google Scholar] [CrossRef]
- Liu, P.-Y.; Lee, Y.-L.; Lu, M.-C.; Shao, P.-L.; Lu, P.-L.; Chen, Y.-H.; Cheng, S.-H.; Ko, W.-C.; Lin, C.-Y.; Wu, T.-S.; et al. National Surveillance of Antimicrobial Susceptibility of Bacteremic Gram-Negative Bacteria with Emphasis on Community-Acquired Resistant Isolates: Report from the 2019 Surveillance of Multicenter Antimicrobial Resistance in Taiwan (SMART). Antimicrob. Agents Chemother. 2020, 64, 01089-20. [Google Scholar] [CrossRef]
- Ruiz, J.; Ramírez, P.; Company, M.J.; Gordon, M.; Villarreal, E.; Concha, P.; Aroca, M.; Frasquet, J.; Marqués, M.R.; Castellanos-Ortega, Á. Impact of amikacin pharmacokinetic/pharmacodynamic index on treatment response in critically ill patients. J. Glob. Antimicrob. Resist. 2018, 12, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Mise au point sur le bon usage des aminosides administers par voie injectable: Gentamycin, tobramycin, netimicine, amikacin. Available online: https://ansm.sante.fr/var/ansm_site/storage/original/application/f64613ed667c09bcb015026fa39e70a2.pdf (accessed on 19 January 2021).
- Matsuki, Y.; Yajima, M.; Tsukamoto, T.; Watanabe, T.; Watanabe, S. Effect of nutritional status on the clinical efficacy of once-daily dosing regimens of amikacin sulfate in elderly patients. Jap. J. Infect. Prevent. Control 2018, 33, 7–14. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Gault, H. Prediction of Creatinine Clearance from Serum Creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Hirayama, S.; Kikuchi, R.; Inoue, S.; Tsukahara, D.; Suemitsu, Y.; Kobayashi, Y.; Sugiyama, Y.; Hasegawa, H.; Kouzaki, K.; Inoue, G.; et al. Creatinine clearance estimation in the extremely elderly subjects. Nihon Ronen Igakkai Zasshi 2007, 44, 90–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janmahasatian, S.; Duffull, S.B.; Ash, S.; Ward, L.C.; Byrne, N.M.; Green, B. Quantification of Lean Bodyweight. Clin. Pharmacokinet. 2005, 44, 1051–1065. [Google Scholar] [CrossRef]
- Neely, M.M.; Van Guilder, M.G.; Yamada, W.M.; Schumitzky, A.; Jelliffe, R.W. Accurate Detection of Outliers and Subpopulations With Pmetrics, a Nonparametric and Parametric Pharmacometric Modeling and Simulation Package for R. Ther. Drug Monit. 2012, 34, 467–476. [Google Scholar] [CrossRef] [Green Version]
- Tatarinova, T.; Neely, M.; Bartroff, J.; Van Guilder, M.; Yamada, W.; Bayard, D.; Jelliffe, R.; Leary, R.; Chubatiuk, A.; Schumitzky, A. Two general methods for population pharmacokinetic modeling: Non-Parametric adaptive grid and non-parametric Bayesian. J. Pharmacokinet. Pharmacodyn. 2013, 40, 189–199. [Google Scholar] [CrossRef] [Green Version]
- Ette, E.I. Stability and Performance of a Population Pharmacokinetic Model. J. Clin. Pharmacol. 1997, 37, 486–495. [Google Scholar] [CrossRef]
- Moore, R.D.; Smith, C.R.; Lietman, P.S. Association of aminoglycoside plasma levels with therapeutic outcome in gram-negative pneumonia. Am. J. Med. 1984, 77, 657–662. [Google Scholar] [CrossRef]
- Stratford, B.; Dixson, S.; Cobcroft, A. Serum levels of gentamicin and tobramycin after slow intravenous bolus injection. Lancet 1974, 303, 378–379. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing—EUCAST. Available online: http://eucast.org (accessed on 28 February 2020).



{kind=link}
{kind=link}
| Parameter | Mean ± SD | Median [Range] |
|---|---|---|
| Male/female | 6/9 | - |
| Age (year) | 80.6 ± 7.3 | 80.0 [71–95] |
| Weight (kg) | 44.8 ± 8.9 | 42.6 [32.5–67.3] |
| Lean body weight (kg) | 35.5 ± 8.1 | 34.6 [24.6–51.1] |
| BMI (kg/m2) | 19.1 ± 3.0 | 19.7 [14.9–25.6] |
| Ideal body weight (kg) | 51.9 ± 7.4 | 51.5 [40.1–68.1] |
| Albumin (g/dL) | 2.5 ± 0.4 | 2.4 [1.7–3.2] |
| Serum creatinine (mg/dL) | 0.84 ± 0.77 | 0.59 [0.32–3.39] |
| CCr * (mL/min) | 52.9 ± 22.8 | 52.1 [10.9–94.9] |
| AST (U/L) | 46 ± 58 | 31 [6–243] |
| ALT (U/L) | 32 ± 23 | 26 [7–91] |
| BUN (mg/dL) | 24.8 ± 19.7 | 16.4 [6.8–71.6] |
| Total bilirubin (mg/dL) | 1.10 ± 0.88 | 0.65 [0.38–3.16] |
| Duration of amikacin therapy (days) | 9 ± 6 | 7 [3–20] |
| Amikacin dosage (mg/day) | 440 ± 226 | 400 [200–1000] |
| Amikacin dosage (mg/kg/day) | 9.6 ± 3.6 | 9.4 [4.3–17.7] |
| Infusion time (h) | 0.67 ± 0.41 | 0.5 [0.5–1.0] |
| Mean | SD | Median | SE | CV% | Var | Shrink% | |
|---|---|---|---|---|---|---|---|
| CL (L/h) | 2.25 | 0.78 | 2.19 | 0.24 | 34.6 | 2.19 | 4.20 |
| V (L) | 18.0 | 3.4 | 17.1 | 1.0 | 18.9 | 17.1 | 17.22 |
| (A). q24h |
 |
| (B). q48h |
 |
| (C). q72h |
 |
| (A). q24h | |||||||||||
| Dose regimen (mg) | |||||||||||
| 200 | 400 | 600 | 800 | 1000 | 1200 | 1400 | 1600 | 1800 | 2000 | ||
| CCr | 10 | 32.6 | 68.0 | 77.2 | 88.9 | 93.5 | 93.9 | 95.7 | 98.1 | 98.7 | 99.3 |
| 20 | 16.9 | 49.9 | 76.3 | 81.1 | 90.9 | 93.6 | 93.8 | 95.2 | 96.9 | 98.6 | |
| 30 | 10.0 | 41.9 | 75.7 | 77.1 | 85.4 | 93.3 | 93.6 | 93.9 | 95.3 | 96.7 | |
| 40 | 8.5 | 40.1 | 70.4 | 76.4 | 82.2 | 90.8 | 93.6 | 93.6 | 94.3 | 95.8 | |
| 50 | 8.3 | 39.9 | 65.1 | 76.4 | 79.8 | 88.3 | 93.3 | 93.6 | 93.9 | 94.9 | |
| 60 | 8.3 | 39.9 | 62.3 | 76.3 | 77.9 | 86.9 | 92.4 | 93.6 | 93.7 | 94.4 | |
| 70 | 8.3 | 39.8 | 59.8 | 76.2 | 77.0 | 85.8 | 91.6 | 93.6 | 93.7 | 94.1 | |
| 80 | 8.2 | 39.3 | 58.0 | 75.5 | 76.6 | 84.9 | 91.1 | 93.3 | 93.6 | 93.9 | |
| 90 | 8.0 | 38.2 | 55.9 | 74.5 | 76.5 | 83.9 | 90.7 | 92.7 | 93.6 | 93.8 | |
| (B). q48h | |||||||||||
| Dose regimen (mg) | |||||||||||
| 200 | 400 | 600 | 800 | 1000 | 1200 | 1400 | 1600 | 1800 | 2000 | ||
| CCr | 10 | 18.2 | 51.3 | 76.4 | 81.5 | 91.5 | 93.6 | 93.9 | 95.4 | 97.0 | 98.6 |
| 20 | 8.9 | 40.6 | 72.1 | 76.4 | 83.5 | 91.9 | 93.6 | 93.7 | 94.6 | 96.1 | |
| 30 | 8.4 | 40.0 | 64.8 | 76.3 | 79.3 | 88.7 | 92.6 | 93.6 | 94.0 | 94.9 | |
| 40 | 8.4 | 39.8 | 62.2 | 76.3 | 77.4 | 87.4 | 91.5 | 93.5 | 93.9 | 94.5 | |
| 50 | 8.0 | 38.3 | 60.4 | 74.6 | 76.8 | 86.5 | 91.2 | 92.7 | 93.8 | 94.3 | |
| 60 | 7.7 | 36.7 | 58.8 | 73.4 | 76.6 | 85.6 | 91.0 | 91.9 | 93.7 | 94.1 | |
| 70 | 7.6 | 36.1 | 57.0 | 72.6 | 76.5 | 84.7 | 90.7 | 91.6 | 93.6 | 94.0 | |
| 80 | 7.6 | 36.0 | 55.7 | 72.5 | 76.5 | 83.6 | 90.5 | 91.5 | 93.6 | 93.9 | |
| 90 | 7.6 | 36.0 | 54.1 | 72.5 | 76.4 | 82.7 | 90.1 | 91.5 | 93.3 | 93.8 | |
| (C). q72h | |||||||||||
| Dose regimen (mg) | |||||||||||
| 200 | 400 | 600 | 800 | 1000 | 1200 | 1400 | 1600 | 1800 | 2000 | ||
| CCr | 10 | 11.1 | 43.1 | 75.8 | 77.2 | 87.1 | 93.3 | 93.6 | 94.1 | 95.6 | 97.1 |
| 20 | 8.7 | 40.3 | 66.7 | 76.3 | 80.2 | 89.3 | 92.7 | 93.7 | 94.0 | 95.0 | |
| 30 | 8.5 | 39.7 | 64.0 | 75.9 | 77.9 | 88.1 | 91.5 | 93.4 | 93.9 | 94.4 | |
| 40 | 7.9 | 37.2 | 61.9 | 73.2 | 77.1 | 86.9 | 91.4 | 91.6 | 93.8 | 94.2 | |
| 50 | 7.8 | 36.4 | 60.1 | 72.4 | 76.8 | 86.2 | 91.2 | 91.6 | 93.7 | 94.1 | |
| 60 | 7.7 | 36.2 | 58.8 | 72.3 | 76.6 | 85.5 | 90.9 | 91.6 | 93.6 | 94.0 | |
| 70 | 7.6 | 36.2 | 57.1 | 72.2 | 76.5 | 84.5 | 90.7 | 91.6 | 93.4 | 93.9 | |
| 80 | 7.6 | 36.2 | 55.7 | 72.2 | 76.4 | 83.8 | 90.5 | 91.6 | 93.2 | 93.8 | |
| 90 | 7.6 | 36.2 | 53.8 | 72.2 | 76.4 | 82.9 | 90.1 | 91.6 | 93.0 | 93.8 | |
| Renal Function | CCr | Recommended Dose Regimen |
|---|---|---|
| Kidney failure | 10 | NA |
| 20 | NA | |
| Severe impairment | 30 | NA |
| 40 | 1800 mg q72h | |
| Moderate impairment | 50 | 1800 mg q72h |
| 60 | 1800 mg q48h | |
| Mild impairment | 70 | 1800 mg q48h |
| 80 | 1800 mg q48h | |
| Normal | 90 | 1800 mg q48h |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, H.; Parker, S.L.; Roberts, J.A.; Hagihara, M.; Asai, N.; Yamagishi, Y.; Paterson, D.L.; Mikamo, H. Population Pharmacokinetics Analysis of Amikacin Initial Dosing Regimen in Elderly Patients. Antibiotics 2021, 10, 100. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10020100
Kato H, Parker SL, Roberts JA, Hagihara M, Asai N, Yamagishi Y, Paterson DL, Mikamo H. Population Pharmacokinetics Analysis of Amikacin Initial Dosing Regimen in Elderly Patients. Antibiotics. 2021; 10(2):100. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10020100
Chicago/Turabian StyleKato, Hideo, Suzanne L. Parker, Jason A. Roberts, Mao Hagihara, Nobuhiro Asai, Yuka Yamagishi, David L. Paterson, and Hiroshige Mikamo. 2021. "Population Pharmacokinetics Analysis of Amikacin Initial Dosing Regimen in Elderly Patients" Antibiotics 10, no. 2: 100. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10020100