
Elizabethkingia Intra-Abdominal Infection and Related Trimethoprim-Sulfamethoxazole Resistance: A Clinical-Genomic Study

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Case Report
2.2. Reported Elizabethkingia Intra-Abdominal Infection in the Literature
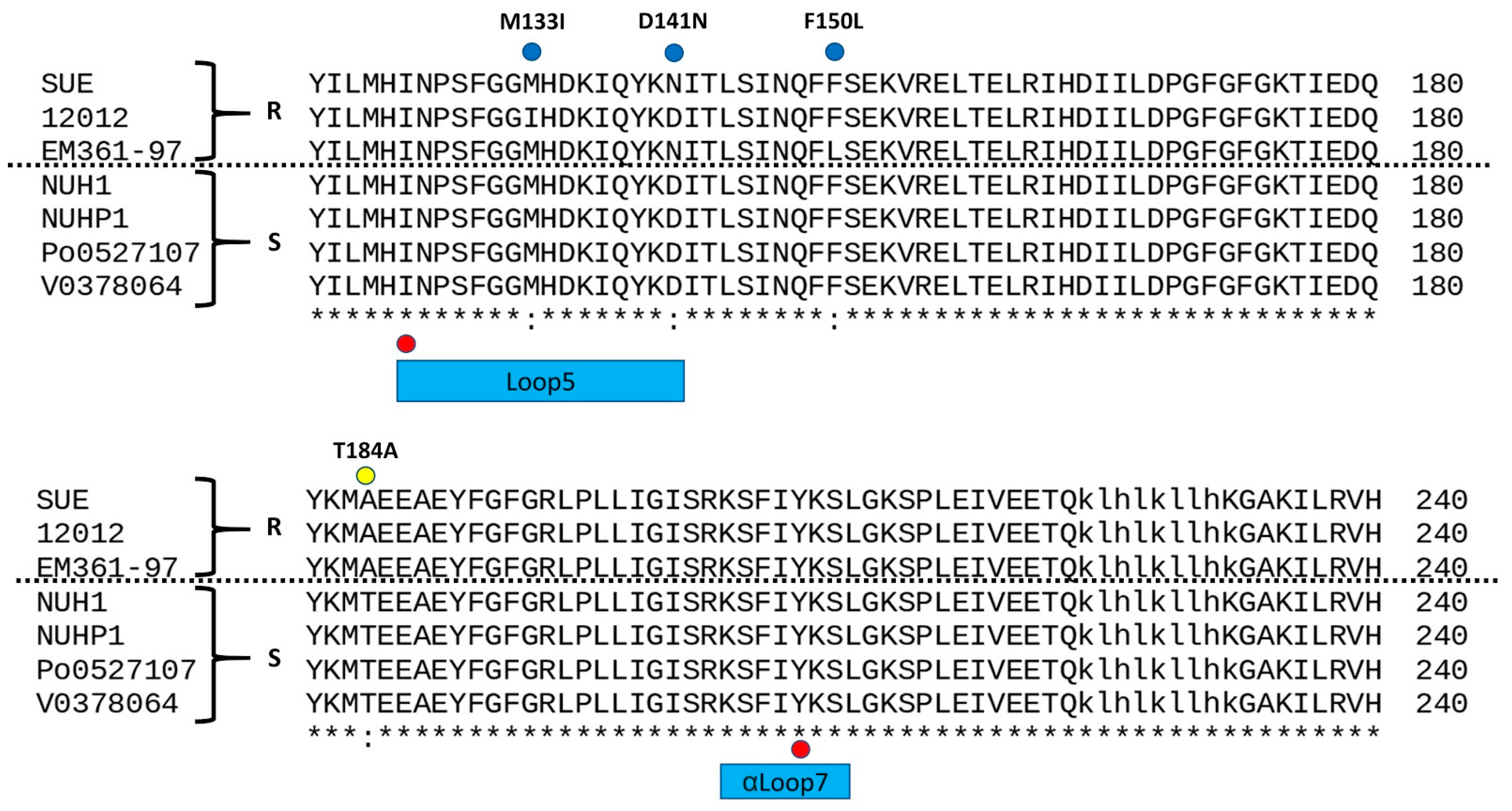
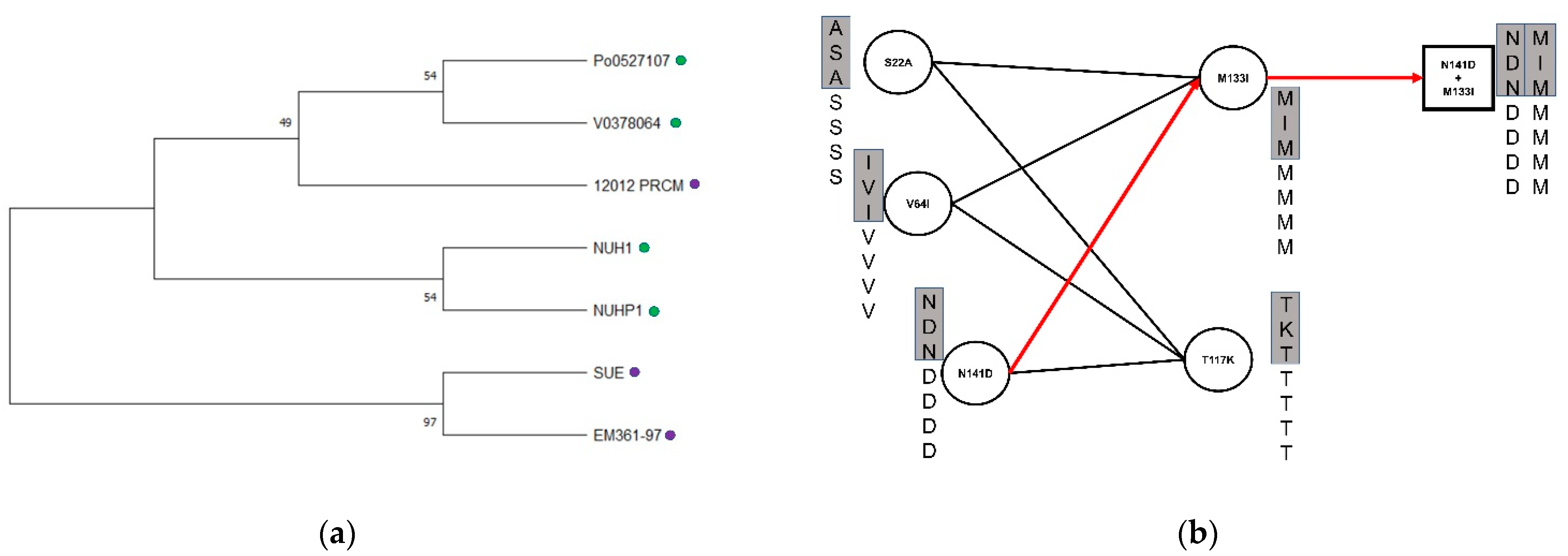
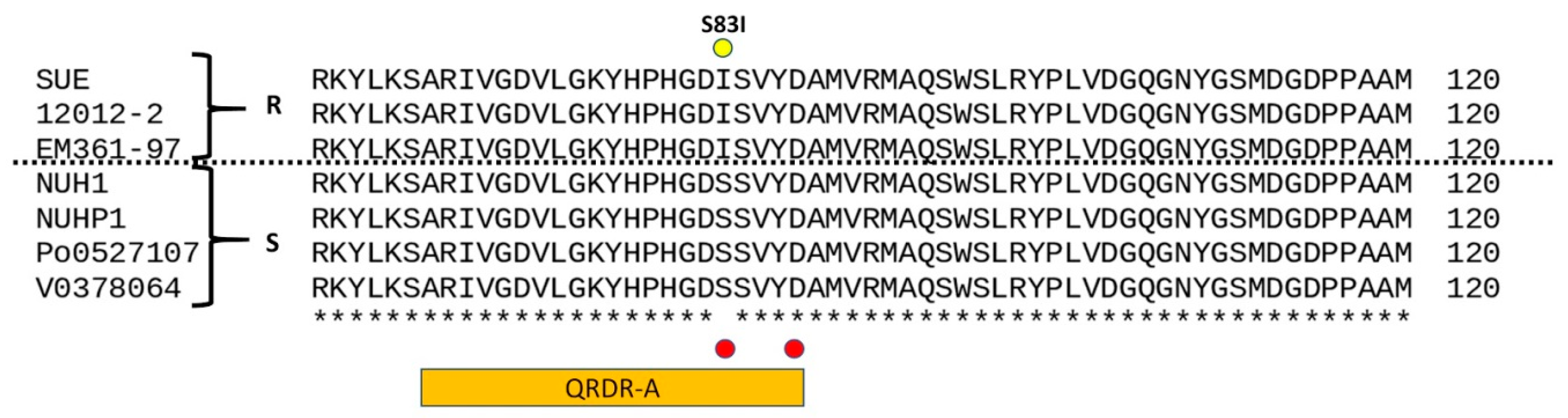
Genomics Revealed Key Mutations Leading to TMP/SMX and Quinolone Resistance
3. Discussion
4. Materials and Methods
4.1. Literature Review
4.2. Whole Genome Sequencing and Bioinformatics Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, K.K.; Kim, M.K.; Lim, J.H.; Park, H.Y.; Lee, S.-T. Transfer of Chryseobacterium meningosepticum and Chryseobacterium miricola to Elizabethkingia gen. nov. as Elizabethkingia meningoseptica comb. nov. and Elizabethkingia miricola comb. nov. Int. J. Syst. Evol. Microbiol. 2005, 55, 1287–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kämpfer, P.; Matthews, H.; Glaeser, S.P.; Martin, K.; Lodders, N.; Faye, I. Elizabethkingia anophelis sp. nov., isolated from the midgut of the mosquito Anopheles gambiae. Int. J. Syst. Evol. Microbiol. 2011, 61, 2670–2675. [Google Scholar] [CrossRef] [PubMed]
- Chew, K.L.; Cheng, B.; Lin, R.T.P.; Teo, J.W.P. Elizabethkingia anophelis is the dominant Elizabethkingia species found in blood cultures in singapore. J. Clin. Microbiol. 2017, 56, e01445-17. [Google Scholar] [CrossRef] [Green Version]
- Han, M.-S.; Kim, H.; Lee, Y.; Kim, M.; Ku, N.S.; Choi, J.Y.; Yong, D.; Jeong, S.H.; Lee, K.; Chong, Y. Relative prevalence and antimicrobial susceptibility of clinical isolates of Elizabethkingia species based on 16S rRNA gene sequencing. J. Clin. Microbiol. 2017, 55, 274–280. [Google Scholar] [CrossRef] [Green Version]
- Teo, J.; Tan, S.Y.-Y.; Tay, M.; Ding, Y.; Kjelleberg, S.; Givskov, M.; Lin, R.T.; Yang, L. First case of E anophelis outbreak in an intensive-care unit. Lancet 2013, 382, 855–856. [Google Scholar] [CrossRef]
- Figueroa Castro, C.E.; Johnson, C.; Williams, M.; VanDerSlik, A.; Graham, M.B.; Letzer, D.; Ledeboer, N.; Buchan, B.W.; Block, T.; Borlaug, G.; et al. Elizabethkingia anophelis: Clinical experience of an academic health system in southeastern wisconsin. Open Forum Infect. Dis. 2017, 4, ofx251. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.-N.; Lai, C.-H.; Yang, C.-H.; Huang, Y.-H. Elizabethkingia infections in humans: From genomics to clinics. Microorganisms 2019, 7, 295. [Google Scholar] [CrossRef] [Green Version]
- Bulagonda, E.P.; Manivannan, B.; Mahalingam, N.; Lama, M.; Chanakya, P.P.; Khamari, B.; Jadhao, S.; Vasudevan, M.; Nagaraja, V. Comparative genomic analysis of a naturally competent Elizabethkingia anophelis isolated from an eye infection. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Gao, H.; Lin, N.; Zhang, Y.; Huang, N.; Walker, E.D.; Ming, D.; Chen, S.; Hu, S. The antibiotic resistance and pathogenicity of a multidrug-resistant Elizabethkingia anophelis isolate. Microbiologyopen 2019, 8, e804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janda, J.M.; Lopez, D.L. Mini review: New pathogen profiles: Elizabethkingia anophelis. Diagn. Microbiol. Infect. Dis. 2017, 88, 201–205. [Google Scholar] [CrossRef]
- Lin, J.-N.; Lai, C.-H.; Yang, C.-H.; Huang, Y.-H. Comparison of clinical manifestations, antimicrobial susceptibility patterns, and mutations of fluoroquinolone target genes between Elizabethkingia meningoseptica and Elizabethkingia anophelis isolated in Taiwan. J. Clin. Med. 2018, 7, 538. [Google Scholar] [CrossRef] [Green Version]
- Burnard, D.; Gore, L.; Henderson, A.; Ranasinghe, A.; Bergh, H.; Cottrell, K.; Sarovich, D.S.; Price, E.P.; Paterson, D.L.; Harris, P. Comparative genomics and antimicrobial resistance profiling of Elizabethkingia isolates reveal nosocomial transmission and in vitro susceptibility to fluoroquinolones, tetracyclines, and trimethoprim-sulfamethoxazole. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef]
- Liang, C.-Y.; Yang, C.-H.; Lai, C.-H.; Huang, Y.-H.; Lin, J.-N. Comparative genomics of 86 whole-genome sequences in the six species of the Elizabethkingia genus reveals intraspecific and interspecific divergence. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Musalem, H.M.; Honjol, Y.N.; Tuleimat, L.M.; Al Abbad, S.I.; Alsohaibani, F.I. Elizabethkingia Meningoseptica in a case of biliary tract infection following liver transplantation. Am. J. Case Rep. 2017, 18, 1014–1019. [Google Scholar] [CrossRef] [Green Version]
- Ranjan, S.; Veerappan, I.; Patil, S.; Sethuraman, R. Elizabethkingia meningoseptica peritonitis in continuous ambulatory peritoneal dialysis patient: A rare case report with diagnostic challenges. Indian J. Pathol. Microbiol. 2017, 60, 626. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.-C.; Tsai, T.-J.; Wang, R.; Hsueh, P.-R. Peritonitis caused by Chryseobacterium meningosepticum in a patient undergoing continuous ambulatory peritoneal dialysis. J. Formos. Med. Assoc. 2003, 102, 270–272. [Google Scholar] [PubMed]
- Khan, I.D.; Lall, M.; Sen, S.; Ninawe, S.; Chandola, P. Multiresistant Elizabethkingia meningoseptica infections in tertiary care. Med. J. Armed Forces India 2015, 71, 282–286. [Google Scholar] [CrossRef] [Green Version]
- Lau, S.K.; Chow, W.-N.; Foo, C.-H.; Curreem, S.O.; Lo, G.C.-S.; Teng, J.L.; Chen, J.H.; Ng, R.H.; Wu, A.K.; Cheung, I.Y. Eliz-abethkingia anophelis bacteremia is associated with clinically significant infections and high mortality. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Frank, T.; Gody, J.C.; Nguyen, L.B.L.; Berthet, N.; Le Fleche-Mateos, A.; Bata, P.; Rafaï, C.; Kazanji, M.; Breurec, S. First case of Elizabethkingia anophelis meningitis in the Central African Republic. Lancet 2013, 381, 734–737. [Google Scholar] [CrossRef]
- Choi, M.H.; Kim, M.; Jeong, S.J.; Choi, J.Y.; Lee, I.-Y.; Yong, T.-S.; Yong, D.; Jeong, S.H.; Lee, K. Risk Factors for Elizabethkingia acquisition and clinical characteristics of patients, South Korea. Emerg. Infect. Dis. 2019, 25, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.-N.; Lai, C.-H.; Yang, C.-H.; Huang, Y.-H.; Lin, H.-F.; Lin, H.-H. Comparison of four automated microbiology systems with 16S rRNA gene sequencing for identification of Chryseobacterium and Elizabethkingia species. Sci. Rep. 2017, 7, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrin, A.; Larsonneur, E.; Nicholson, A.C.; Edwards, D.J.; Gundlach, K.M.; Whitney, A.M.; Gulvik, C.A.; Bell, M.E.; Rendueles, O.; Cury, J.; et al. Evolutionary dynamics and genomic features of the Elizabethkingia anophelis 2015 to 2016 Wisconsin outbreak strain. Nat. Commun. 2017, 8, 15483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Zhang, X.; Li, D.; Hu, F.; Wang, M.; Guo, Q.; Yang, F. Molecular characteristics and antimicrobial susceptibility profiles of Elizabethkingia clinical isolates in Shanghai, China. Infect. Drug Resist. 2020, 13, 247–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.-C.; Lin, Y.-T.; Wang, F.-D.; Chan, Y.-J.; Yang, T.-C.; Huang, Y.-W. Risk factors and outcome of levofloxacin-resistant Elizabethkingia meningoseptica bacteraemia in adult patients in Taiwan. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1373–1380. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-N.; Lai, C.-H.; Yang, C.-H.; Huang, Y.-H.; Lin, H.-H. Clinical manifestations, molecular characteristics, antimicrobial susceptibility patterns and contributions of target gene mutation to fluoroquinolone resistance in Elizabethkingia anophelis. J. Antimicrob. Chemother. 2018, 73, 2497–2502. [Google Scholar] [CrossRef]
- Jian, M.-J.; Cheng, Y.-H.; Chung, H.-Y.; Cheng, Y.-H.; Yang, H.-Y.; Hsu, C.-S.; Perng, C.-L.; Shang, H.-S. Fluoroquinolone re-sistance in carbapenem-resistant Elizabethkingia anophelis: Phenotypic and genotypic characteristics of clinical isolates with topoisomerase mutations and comparative genomic analysis. J. Antimicrob. Chemother. 2019, 74, 1503–1510. [Google Scholar] [CrossRef]
- Correia, S.; Poeta, P.; Hébraud, M.; Capelo, J.L.; Igrejas, G. Mechanisms of quinolone action and resistance: Where do we stand? J. Med. Microbiol. 2017, 66, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Wang, D.; Wang, Y.; Yan, H.; Shi, L.; Zhou, L.-J. Occurrence of antimicrobial resistance genes sul and dfrA12 in hospital environmental isolates of Elizabethkingia meningoseptica. World J. Microbiol. Biotechnol. 2012, 28, 3097–3102. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. | Location | Age | Sex | Underlining Disease | Clinical Presentation | Culture- Positive Specimens | Elizabethkingia Speices | Method for Identification | References |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Taichung, Taiwan | 69 | M | Autoimmune protein losing enteropathy, with ascites, pleural effusion | Fever, abdominal distention, Spontaneous bacterial peritonitis | Blood and ascites | E. anophelis | Whole genome sequencing | NA |
| 2 | Wisconsin, USA | 84 | M | Chronic HCV infection, cirrhosis, Type 2 DM, alcohol abuse | Abdominal distention, fever, Suspected spontaneous bacterial peritonitis | blood and ascites | E. anophelis | Verigene system /MALDI-ToF MS | [6] |
| 3 | Saudi Arabia | 55 | F | Type 2 DM, liver cirrhosis, s/p liver transplantation. with post-transplant anastomotic biliary stricture and bile leakage, s/p PTBD | RUQ abdominal pain, no fever. Intra-abdominal infection with subphrenic fluid accumulation | Bile * | E. meningoseptica | NA | [14] |
| 4 | Hongkong, China | 52 | M | biliary pancreatitis, recurrent pyogenic cholangitis, cirrhosis with biliary stent | Acute cholangitis | Blood | E. meningoseptica | 16S rRNA gene sequence analysis | [18] |
| 5 | Hongkong, China | 89 | F | Hypertension, Atrial fibrillation, painless obstructive jaundice on palliative stenting | Biliary tract infection with sepsis | Blood | E. meningoseptica | 16S rRNA gene sequence analysis | [18] |
| 6 | Tamil Nadu, India | 72 | M | Type 2 DM, hypertension, ESRD under CAPD for 22 months | Abdominal pain, and cloudy CAPD fluid. CAPD peritonitis | CAPD fluid | E. meningoseptica | Vitek-2 compact | [15] |
| 7 | Taipei, Taiwan | 54 | F | ESRD under CAPD for eight years | Turbid CAPD fluid, abdominal pain and fever. CAPD peritonitis with Tenckhoff tube infection | CAPD fluid | E. meningoseptica (previously Chryseobacterium meningoseptica) | API and Vitek test system | [16] |
| 8 | New Delhi, India | 8 | F | ESRD since 18 m/o, under CAPD for six years | CAPD peritonitis | CAPD fluid | Elizabethkingia meningoseptica | Vitek system and Vitek AST-N090 card | [17] |
| 9 | New Delhi, India | 23 | F | s/p Medical Termination of Pregnancy by suction and evacuation for suspected blighted ovum or missed abortion | Postposture fever and bleeding. Peritonitis, secondary to uterine perforation | blood culture * 2 set | Elizabethkingia meningoseptica | Vitek system and Vitek AST-N090 card | [17] |
| No. | Elizabethkingia spp. | Clinical Presentation | Antibiotic Susceptibility (Susceptible Drugs) | Antibiotic Use | Removal of Catheter | Survival |
|---|---|---|---|---|---|---|
| 1 | E. anophelis | Spontaneous bacterial peritonitis | Pipercacillin/tazobactam, Cefepime, Cefoperazone/sulbactam; TMP/SMX * | TMP/SMX+ Levofloxacin, then Piperacillin/tazobactam | No catheter | Expired |
| 2 | E. anophelis | Suspected spontaneous bacterial peritonitis | Ciprofloxacin, Piperacillin/tazobactam, TMP/SMX, Cefepime | Ciprofloxacin and Piperacillin/tazobactam | No catheter | Survived |
| 3 | E. meningoseptica | Intra-abdominal infection with subphrenic fluid accumulation | Ciprofloxacin, Minocycline, Tigecycline, TMP/SMX | Ciprofloxacin and metronidazole | NA | Survived |
| 4 | E. meningoseptica | Acute cholangitis | NA | Levofloxacin and metronidazole | NA | Survived |
| 5 | E. meningoseptica | Biliary tract infection with sepsis | NA | Levofloxacin | NA | Survived |
| 6 | E. meningoseptica | CAPD peritonitis | Cefoperazone/sulbactam, Ciprofloxacin, Levofloxacin, Minocycline, TMP/SMX | PO TMP/SMX + IV Cefoperazone/sulbactam, then shift to PO Minocycline + IV Cefoperazone/sulbactam | Removal of CAPD tube. | Survived |
| 7 | E. meningoseptica (previously Chryseobacterium meningoseptica) | CAPD peritonitis with Tenckhoff tube infection | Gentamicin, Ciprofloxacin, Piperacillin-tazobactam, Levofloxacin | Piperacillin-tazobactam, then shift to Levofloxacin | Removal of CAPD tube. | Survived |
| 8 | E. meningoseptica | CAPD peritonitis | Cefoperazone-sulbactam and nalidixic acid | Cefoperazone-sulbactam | NA | Survived |
| 9 | E. meningoseptica | Peritonitis, secondary to uterine perforation | TMP/SMX | TMP/SMX, Piperacillin- tazobactam, amikacin, teicoplanin and metronidazole | No catheter | Survived |
| Strains | Genome Size | Genes | Sequencing Technology | TMP/SMX | Quinolone | Status | Assembly Number |
|---|---|---|---|---|---|---|---|
| SUE | 4,201,198 bp | 3869 | Nanopore; Illumina MiSeq | 160 R | ≥4 R | Circ. | GCA_014702245.1 |
| 12012 | 4,023,312 bp | 3700 | Illumina MiSeq | >2/38 R | >2 R | Linear | GCA_001482795.1 |
| EM361-97 | 4,077,699 bp | 3752 | Illumina HiSeq | >4/76 R | >2 R | Linear | GCA_001703835.1 |
| NUH1 | 4,334,661 bp | 4031 | Illumina MiSeq | S | S | Linear | GCA_000495995.1 |
| NUHP1 | 4,369,828 bp | 4034 | Illumina | S | S | Linear | GCA_000495935.2 |
| Po0527107 | 4,032,057 bp | 3717 | Illumina HiSeq-2000 | S | S | Linear | GCA_000689515.1 |
| V0378064 | 4,036,754 bp | 3804 | Illumina HiSeq-2001 | S | I | Linear | GCA_000689455.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teng, L.-C.; Wang, J.-M.; Lu, H.-Y.; Mao, Y.-C.; Lai, K.-L.; Tseng, C.-H.; Huang, Y.-T.; Liu, P.-Y. Elizabethkingia Intra-Abdominal Infection and Related Trimethoprim-Sulfamethoxazole Resistance: A Clinical-Genomic Study. Antibiotics 2021, 10, 173. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10020173
Teng L-C, Wang J-M, Lu H-Y, Mao Y-C, Lai K-L, Tseng C-H, Huang Y-T, Liu P-Y. Elizabethkingia Intra-Abdominal Infection and Related Trimethoprim-Sulfamethoxazole Resistance: A Clinical-Genomic Study. Antibiotics. 2021; 10(2):173. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10020173
Chicago/Turabian StyleTeng, Ling-Chiao, Jiunn-Min Wang, Hsueh-Yin Lu, Yan-Chiao Mao, Kuo-Lung Lai, Chien-Hao Tseng, Yao-Ting Huang, and Po-Yu Liu. 2021. "Elizabethkingia Intra-Abdominal Infection and Related Trimethoprim-Sulfamethoxazole Resistance: A Clinical-Genomic Study" Antibiotics 10, no. 2: 173. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10020173