
Comparative Analysis of Gradient Diffusion and Disk Diffusion with Agar Dilution for Susceptibility Testing of Elizabethkingia anophelis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Study Setting and Design
2.3. Agar Dilution Assay
2.4. Disk Diffusion Assay
2.5. Gradient Diffusion Assay
2.6. Susceptibility Interpretation
2.7. Comparative Performance Data
3. Results
3.1. Susceptibility
3.2. MIC Determination
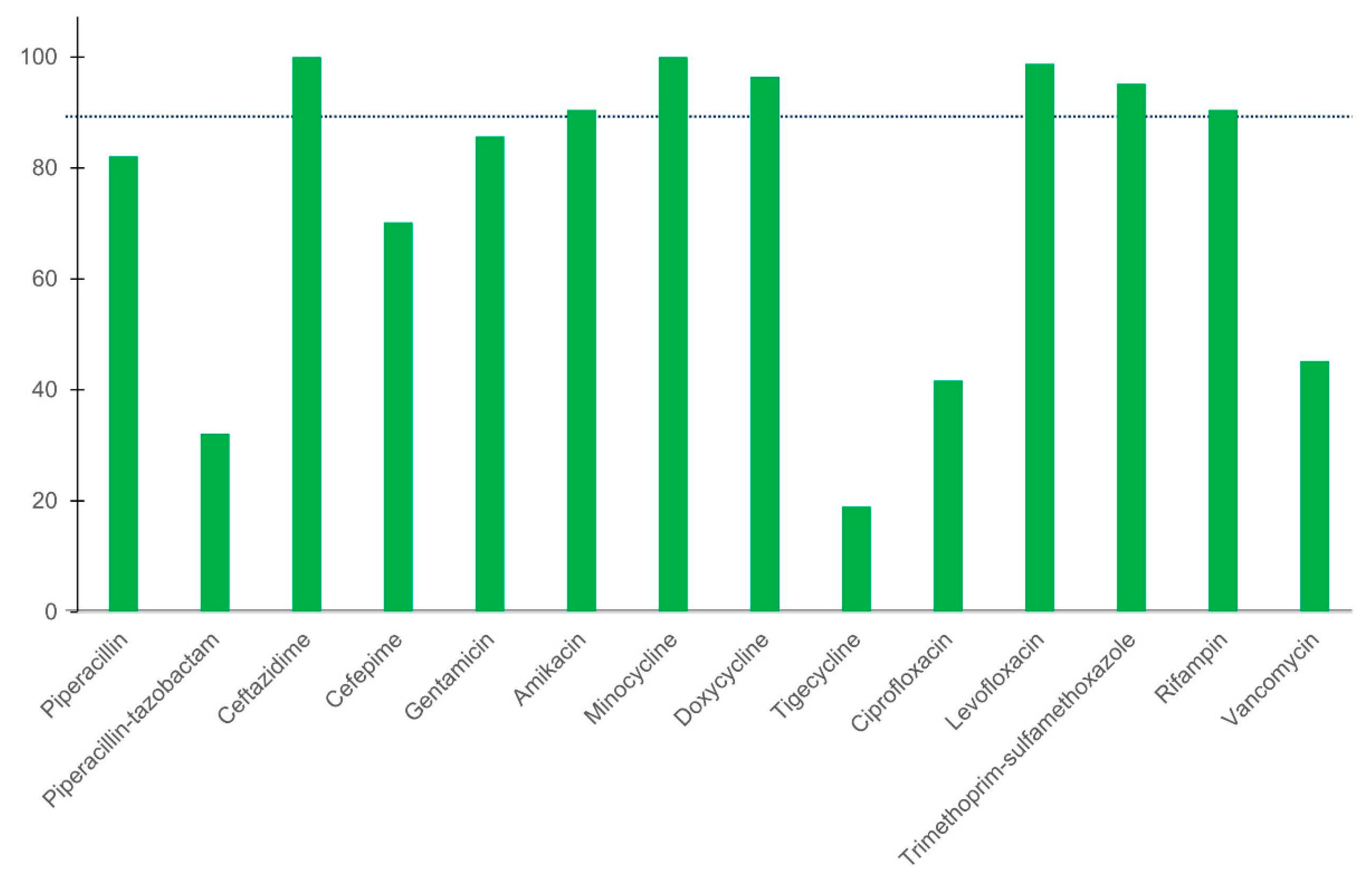
3.3. Discrepancy and Agreement Rates between Disk Diffusion and Agar Dilution Methods
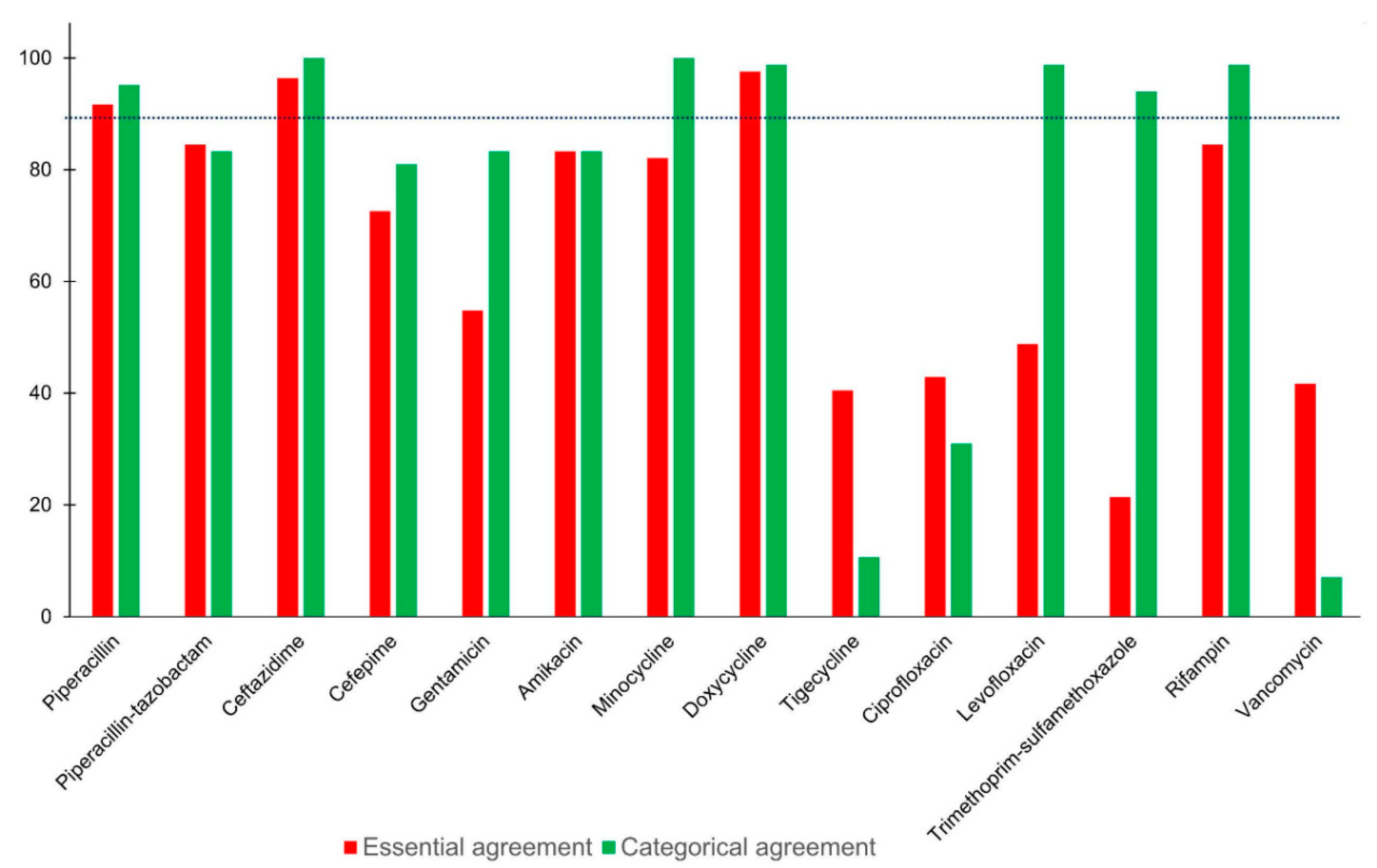
3.4. Discrepancy and Agreement Rates between Etest and Agar Dilution Methods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Henriques, I.S.; Araújo, S.; Azevedo, J.S.N.; Alves, M.S.; Chouchani, C.; Pereira, A.; Correia, A. Prevalence and diversity of carbapenem-resistant bacteria in untreated drinking water in Portugal. Microb. Drug Resist. 2012, 18, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Yung, C.F.; Maiwald, M.; Loo, L.H.; Soong, H.Y.; Tan, C.B.; Lim, P.K.; Li, L.; Tan, N.W.; Chong, C.Y.; Tee, N.; et al. Elizabethkingia anophelis and association with tap water and handwashing, Singapore. Emerg. Infect. Dis. 2018, 24, 1730–1733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyritsi, M.A.; Mouchtouri, V.A.; Pournaras, S.; Hadjichristodoulou, C. First reported isolation of an emerging opportunistic pathogen (Elizabethkingia anophelis) from hospital water systems in Greece. J. Water Health 2018, 16, 164–170. [Google Scholar] [CrossRef] [Green Version]
- King, E.O. Studies on a group of previously unclassified bacteria associated with meningitis in infants. Am. J. Clin. Pathol. 1959, 31, 241–247. [Google Scholar] [CrossRef]
- Nicholson, A.C.; Gulvik, C.A.; Whitney, A.M.; Humrighouse, B.W.; Graziano, J.; Emery, B.; Bell, M.; Loparev, V.; Juieng, P.; Gartin, J.; et al. Revisiting the taxonomy of the genus Elizabethkingia using whole-genome sequencing, optical mapping, and MALDI-TOF, along with proposal of three novel Elizabethkingia species: Elizabethkingia bruuniana sp. nov., Elizabethkingia ursingii sp. nov., and Elizabethkingia occulta sp. nov. Antonie Leeuwenhoek 2018, 111, 55–72. [Google Scholar] [CrossRef]
- Kämpfer, P.; Matthews, H.; Glaeser, S.P.; Martin, K.; Lodders, N.; Faye, I. Elizabethkingia anophelis sp. nov., isolated from the midgut of the mosquito Anopheles gambiae. Int. J. Syst. Evol. Microbiol. 2011, 61, 2670–2675. [Google Scholar] [CrossRef] [PubMed]
- Teo, J.; Tan, S.Y.; Tay, M.; Ding, Y.; Kjelleberg, S.; Givskov, M.; Lin, R.T.; Yang, L. First Case of E anophelis outbreak in an intensive-care unit. Lancet 2013, 382, 855–856. [Google Scholar] [CrossRef]
- Chew, K.L.; Cheng, B.; Lin, R.T.; Teo, J.W. Elizabethkingia anophelis is the dominant Elizabethkingia species found in blood cultures in Singapore. J. Clin. Microbiol. 2018, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, S.K.; Chow, W.N.; Foo, C.H.; Curreem, S.O.; Lo, G.C.; Teng, J.L.; Chen, J.H.; Ng, R.H.; Wu, A.K.; Cheung, I.Y.; et al. Elizabethkingia anophelis bacteremia is associated with clinically significant infections and high mortality. Sci. Rep. 2016, 6, 26045. [Google Scholar] [CrossRef] [PubMed]
- Han, M.S.; Kim, H.; Lee, Y.; Kim, M.; Ku, N.S.; Choi, J.Y.; Yong, D.; Jeong, S.H.; Lee, K.; Chong, Y. Relative prevalence and antimicrobial susceptibility of clinical isolates of Elizabethkingia species based on 16S rRNA gene sequencing. J. Clin. Microbiol. 2017, 55, 274–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.N.; Lai, C.H.; Yang, C.H.; Huang, Y.H.; Lin, H.H. Clinical manifestations, molecular characteristics, antimicrobial susceptibility patterns and contributions of target gene mutation to fluoroquinolone resistance in Elizabethkingia anophelis. J. Antimicrob. Chemother. 2018, 73, 2497–2502. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.H.; Perng, C.L.; Jian, M.J.; Cheng, Y.H.; Lee, S.Y.; Sun, J.R.; Shang, H.S. Multicentre study evaluating matrix-assisted laser desorption ionization-time of flight mass spectrometry for identification of clinically isolated Elizabethkingia species and analysis of antimicrobial susceptibility. Clin. Microbiol. Infect. 2019, 25, 340–345. [Google Scholar] [CrossRef] [Green Version]
- Perrin, A.; Larsonneur, E.; Nicholson, A.C.; Edwards, D.J.; Gundlach, K.M.; Whitney, A.M.; Gulvik, C.A.; Bell, M.E.; Rendueles, O.; Cury, J.; et al. Evolutionary dynamics and genomic features of the Elizabethkingia anophelis 2015 to 2016 Wisconsin outbreak strain. Nat. Commun. 2017, 8, 15483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, M100, 30th ed.; CLSI: Wayne, PA, USA, 2020. [Google Scholar]
- Clinical and Laboratory Standards Institute. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically, M07, 11th ed.; CLSI: Wayne, PA, USA, 2018. [Google Scholar]
- Kelesidis, T.; Karageorgopoulos, D.E.; Kelesidis, I.; Falagas, M.E. Tigecycline for the treatment of multidrug-resistant Enterobacteriaceae: A systematic review of the evidence from microbiological and clinical studies. J. Antimicrob. Chemother. 2008, 62, 895–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food and Drug Administration (USA). FDA-Identified Interpretive Criteria. 2019. Available online: https://www.fda.gov/drugs/development-resources/tigecycline-injection-products (accessed on 7 July 2020).
- Humphries, R.M.; Ambler, J.; Mitchell, S.L.; Castanheira, M.; Dingle, T.; Hindler, J.A.; Koeth, L.; Sei, K.; CLSI Methods Development and Standardization Working Group of the Subcommittee on Antimicrobial Susceptibility Testing. CLSI methods development and standardization working group best practices for evaluation of antimicrobial susceptibility tests. J. Clin. Microbiol. 2018, 56. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administration (USA). Antimicrobial Susceptibility Test (AST) Systems—Class II Special Controls Guidance for Industry and FDA. 2007. Available online: https://www.fda.gov/medical-devices/guidance-documents-medical-devices-and-radiation-emitting-products/antimicrobial-susceptibility-test-ast-systems-class-ii-special-controls-guidance-industry-and-fda (accessed on 7 July 2020).
- Hutchings, M.I.; Truman, A.W.; Wilkinson, B. Antibiotics: Past, present and future. Curr. Opin. Microbiol. 2019, 51, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, B.P. Resistance to rifampicin: A review. J. Antibiot. 2014, 67, 625–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, I.N.; Gisby, J.; Hemingway, C.P.; Durodie, J.; Macpherson, I. Evaluation of mupirocin E-test for determination of isolate susceptibility: Comparison with standard agar dilution techniques. J. Clin. Microbiol. 1995, 33, 2254–2259. [Google Scholar] [CrossRef] [Green Version]
- Luber, P.; Bartelt, E.; Genschow, E.; Wagner, J.; Hahn, H. Comparison of broth microdilution, E test, and agar dilution methods for antibiotic susceptibility testing of Campylobacter jejuni and Campylobacter coli. J. Clin. Microbiol. 2003, 41, 1062–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, M.S.; Hansford, K.A.; Blaskovich, M.A.; Halai, R.; Cooper, M.A. Glycopeptide antibiotics: Back to the future. J. Antibiot. 2014, 67, 631–644. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Antimicrobial Agent a | Susceptibility Testing Assay | ||
|---|---|---|---|
| Agar Dilution (mg/L) | Disk Diffusion (µg) | Etest (mg/L) | |
| Piperacillin | 2–256 | 100 | 0.016–256 |
| Piperacillin–tazobactam | 2/4–256/4 | 100/10 | 0.016/4–256/4 |
| Ceftazidime | 8–256 | 30 | 0.016–256 |
| Cefepime | 1–128 | 30 | 0.016–256 |
| Gentamicin | 1–128 | 10 | 0.016–256 |
| Amikacin | 2–256 | 30 | 0.016–256 |
| Minocycline | 0.0625–2 | 30 | 0.016–256 |
| Doxycycline | 0.25–16 | 30 | 0.016–256 |
| Tigecycline | 0.25–32 | 15 | 0.016–256 |
| Ciprofloxacin | 0.25–32 | 5 | 0.002–32 |
| Levofloxacin | 0.25–32 | 5 | 0.002–32 |
| Trimethoprim–sulfamethoxazole | 0.5/9.5–32/608 | 1.25/23.75 | 0.002/0.38 – 32/608 |
| Rifampin | 0.25–16 | 5 | 0.016–256 |
| Vancomycin | 2–256 | 30 | 0.016–256 |
| Antimicrobial Agent | Agar Dilution | Disk Diffusion | Etest | ||||||
|---|---|---|---|---|---|---|---|---|---|
| MIC Range | MIC50 | MIC90 | % Sa | % Sa | MIC Range | MIC50 | MIC90 | % Sa | |
| Piperacillin | 128–>256 | >256 | >256 | 0 | 4.8 | 8–>256 | >256 | >256 | 2.4 |
| Piperacillin–tazobactam | 256/4–>256/4 | >256/4 | >256/4 | 0 | 22.6 | 8/4–>256/4 | >256/4 | >256/4 | 4.8 |
| Ceftazidime | 256–>256 | >256 | >256 | 0 | 0 | 48–>256 | >256 | >256 | 0 |
| Cefepime | 32–>128 | >128 | >128 | 0 | 21.4 | 1.5–>256 | >256 | >256 | 2.4 |
| Gentamicin | 8–>128 | >128 | >128 | 0 | 9.5 | 3–>256 | 64 | >256 | 13.1 |
| Amikacin | 32–>256 | >256 | >256 | 0 | 6 | 12–>256 | >256 | >256 | 3.6 |
| Minocycline | 0.125–1 | 0.25 | 0.25 | 100 | 100 | 0.023–0.38 | 0.125 | 0.19 | 100 |
| Doxycycline | 1–16 | 2 | 4 | 97.6 | 98.8 | 0.5–16 | 1 | 2 | 97.6 |
| Tigecycline | 2–32 | 8 | 16 | 4.8 | 56 | 0.125–8 | 1.5 | 3 | 77.4 |
| Ciprofloxacin | 1–>32 | 2 | >32 | 8.3 | 51.2 | 0.038–>32 | 0.5 | >32 | 75 |
| Levofloxacin | 0.5–>32 | 2 | 32 | 78.6 | 79.8 | 0.038–>32 | 0.38 | >32 | 79.8 |
| Trimethoprim–sulfamethoxazole | 2/38–32/608 | 8/152 | 16/304 | 1.2 | 1.2 | 0.38/7.22–>32/608 | >32/608 | >32/608 | 4.8 |
| Rifampin | <0.25–>16 | 0.5 | 1 | 95.2 | 85.7 | 0.125–>32 | 0.38 | 0.75 | 94 |
| Vancomycin | 8–256 | 32 | 64 | 0 | 25 | 3 –3 2 | 8 | 16 | 9.5 |
| Antimicrobial Agent | Technique | Isolate no. of MIC log2 Dilutions Differ from the Agar Dilution | Essential Agreement (%) | Interpretive Errors (%) | Categorical Agreement (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤−3 | −2 | −1 | 0 | +1 | +2 | ≥+3 | Very Major | Major | Minor | ||||
| Piperacillin | Disk diffusion | – | – | – | – | – | – | – | – | 4.8 | N/A | 13.1 | 82.1 |
| Etest | 4 | 1 | 1 | 55 | 21 | 2 | 0 | 91.7 | 2.4 | N/A | 2.4 | 95.2 | |
| Piperacillin–tazobactam | Disk diffusion | – | – | – | – | – | – | – | – | 22.6 | N/A | 45.2 | 32.1 |
| Etest | 7 | 5 | 3 | 48 | 20 | 1 | 0 | 84.5 | 4.8 | N/A | 11.9 | 83.3 | |
| Ceftazidime | Disk diffusion | – | – | – | – | – | – | – | – | 0 | N/A | 0 | 100 |
| Etest | 3 | 0 | 1 | 77 | 3 | 0 | 0 | 96.4 | 0 | N/A | 0 | 100 | |
| Cefepime | Disk diffusion | – | – | – | – | – | – | – | – | 21.4 | N/A | 8.3 | 70.2 |
| Etest | 19 | 4 | 3 | 58 | 0 | 0 | 0 | 72.6 | 2.4 | N/A | 16.7 | 81 | |
| Gentamicin | Disk diffusion | – | – | – | – | – | – | – | – | 9.6 | N/A | 4.8 | 85.7 |
| Etest | 17 | 21 | 19 | 25 | 2 | 0 | 0 | 54.8 | 13.3 | N/A | 3.6 | 83.3 | |
| Amikacin | Disk diffusion | – | – | – | – | – | – | – | – | 4.8 | N/A | 4.8 | 90.5 |
| Etest | 3 | 8 | 9 | 45 | 16 | 3 | 0 | 83.3 | 3.6 | N/A | 13.1 | 83.3 | |
| Minocycline | Disk diffusion | – | – | – | – | – | – | – | – | 0 | 0 | 0 | 100 |
| Etest | 2 | 13 | 42 | 24 | 3 | 0 | 0 | 82.1 | 0 | 0 | 0 | 100 | |
| Doxycycline | Disk diffusion | – | – | – | – | – | – | – | – | 100 | 0 | 1.2 | 96.4 |
| Etest | 0 | 2 | 32 | 43 | 7 | 0 | 0 | 97.6 | 0 | 0 | 1.2 | 98.8 | |
| Tigecycline | Disk diffusion | – | – | – | – | – | – | – | – | 50.9 | 0 | 48 | 19 |
| Etest | 25 | 25 | 29 | 5 | 0 | 0 | 0 | 40.5 | 71.7 | 0 | 44 | 10.7 | |
| Ciprofloxacin | Disk diffusion | – | – | – | – | – | – | – | – | 15.2 | 0 | 52.4 | 41.7 |
| Etest | 18 | 30 | 16 | 19 | 1 | 0 | 0 | 42.9 | 39.4 | 0 | 53.6 | 31 | |
| Levofloxacin | Disk diffusion | – | – | – | – | – | – | – | – | 0 | 0 | 1.2 | 98.8 |
| Etest | 13 | 20 | 26 | 9 | 6 | 0 | 0 | 48.8 | 0 | 0 | 1.2 | 98.8 | |
| Trimethoprim–sulfamethoxazole | Disk diffusion | – | – | – | – | – | – | – | – | 1.2 | 100 | 2.4 | 95.2 |
| Etest | 3 | 2 | 6 | 8 | 4 | 22 | 39 | 21.4 | 4.8 | 100 | 0 | 94 | |
| Rifampin | Disk diffusion | – | – | – | – | – | – | – | – | 0 | 0 | 9.5 | 90.5 |
| Etest | 0 | 0 | 14 | 38 | 19 | 13 | 0 | 84.5 | 0 | 0 | 1.2 | 98.8 | |
| Vancomycin | Disk diffusion | – | – | – | – | – | – | – | – | 25.3 | NA | 32.1 | 45.2 |
| Etest | 8 | 41 | 33 | 2 | 0 | 0 | 0 | 41.7 | 5.3 | NA | 88.1 | 7.1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, C.-T.; Lai, C.-H.; Huang, Y.-H.; Yang, C.-H.; Lin, J.-N. Comparative Analysis of Gradient Diffusion and Disk Diffusion with Agar Dilution for Susceptibility Testing of Elizabethkingia anophelis. Antibiotics 2021, 10, 450. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10040450
Chiu C-T, Lai C-H, Huang Y-H, Yang C-H, Lin J-N. Comparative Analysis of Gradient Diffusion and Disk Diffusion with Agar Dilution for Susceptibility Testing of Elizabethkingia anophelis. Antibiotics. 2021; 10(4):450. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10040450
Chicago/Turabian StyleChiu, Chien-Tung, Chung-Hsu Lai, Yi-Han Huang, Chih-Hui Yang, and Jiun-Nong Lin. 2021. "Comparative Analysis of Gradient Diffusion and Disk Diffusion with Agar Dilution for Susceptibility Testing of Elizabethkingia anophelis" Antibiotics 10, no. 4: 450. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10040450