
Prevalence of and Factors Associated with Antibiotic Prescriptions in Patients with Acute Lower and Upper Respiratory Tract Infections—A Case-Control Study

Abstract
:1. Introduction
2. Methods
2.1. Data Source
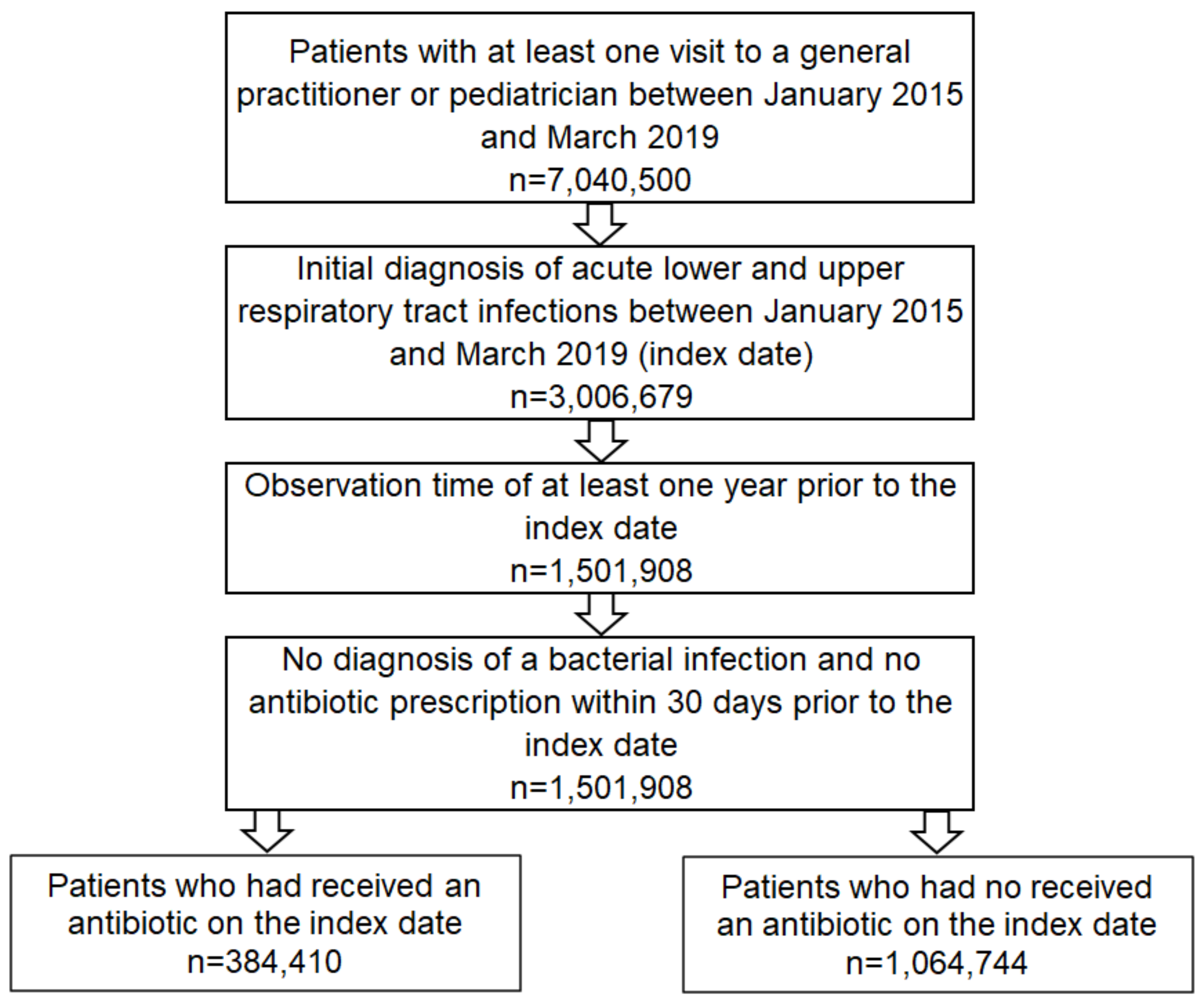
2.2. Study Population
2.3. Study Outcomes and Coviariables
2.4. Statistical Analyses
3. Results
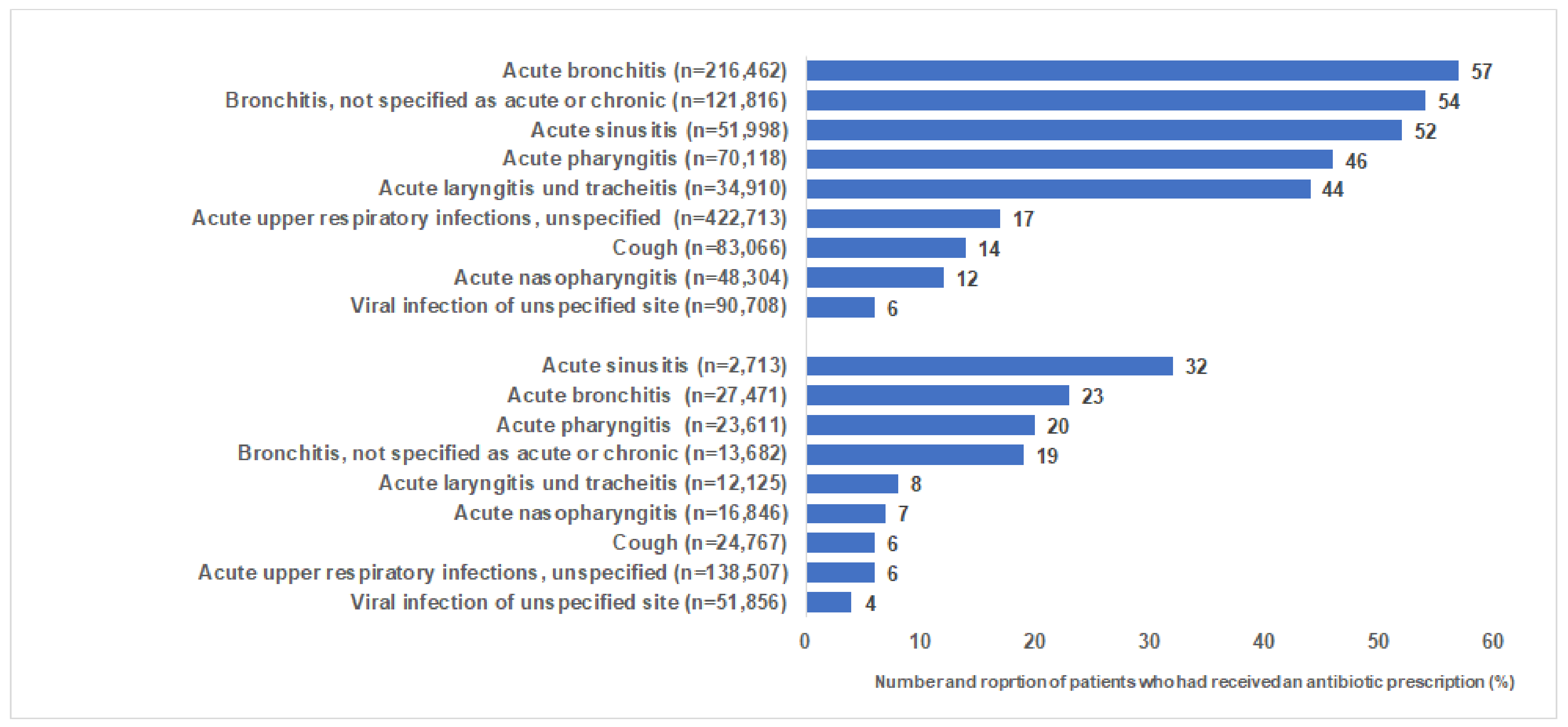
3.1. Prevalence of Antibiotic Use
3.2. Characteristics of Patients with and without Antibiotic Prescription
3.3. Variables Associated with an Antibiotic Prescription
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Allan, G.M.; Arroll, B. Prevention and treatment of the common cold: Making sense of the evidence. CMAJ 2014, 186, 190–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckel, N.; Sarganas, G.; Wolf, I.K.; Knopf, H. Pharmacoepidemiology of common colds and upper respiratory tract infections in children and adolescents in Germany. BMC Pharmacol. Toxicol. 2014, 15, 44. [Google Scholar] [CrossRef] [Green Version]
- Altiner, A.; Bell, J.; Duerden, M.; Essack, S.; Kozlov, R.; Noonan, L.; Oxford, J.; Pignatari, A.C.C.; Sessa, A.; Velden, A. More action, less resistance: Report of the 2014 Summit of the Global Respiratory Infection Partnership. Int. J. Pharm. Pract. 2015, 23, 370–377. [Google Scholar] [CrossRef]
- Köchling, A.; Löffler, C.; Reinsch, S.; Hornung, A.; Böhmer, F.; Altiner, A.; Chenot, J.F. Reduction of antibiotic prescriptions for acute respiratory tract infections in primary care: A systematic review. Implement. Sci. 2018, 13, 47. [Google Scholar] [CrossRef]
- Davies, J.; Davies, D. Origins and evolution of antibiotic resistance. Microbiol. Mol. Biol. Rev. 2010, 74, 417–433. [Google Scholar] [CrossRef] [Green Version]
- Tanday, S. Resisting the use of antibiotics for viral infections. Lancet Respir. Med. 2016, 4, 179. [Google Scholar] [CrossRef]
- Hernando-Amado, S.; Coque, T.M.; Baquero, F.; Martínez, J.L. Antibiotic Resistance: Moving from Individual Health Norms to Social Norms in One Health and Global Health. Front. Microbiol. 2020, 11, 1914. [Google Scholar] [CrossRef]
- Knapp, C.W.; Dolfing, J.; Ehlert, P.A.; Graham, D.W. Evidence of increasing antibiotic resistance gene abundances in archived soils since 1940. Environ. Sci. Technol. 2010, 44, 580–587. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. amr-review.org. 2016. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf. (accessed on 3 April 2021).
- Kern, W.V.; Schaufler, J.; Telschow, C. Antibiotikaverbrauch im ambulanten Bereich. In Bundesamt für Verbraucherschutz und Lebensmittelsicherheit, Paul-Ehrlich-Gesellschaft für Chemotherapie e.V. GERMAP 2015—Bericht über den Antibiotikaverbrauch und die Verbreitung von Antibiotikaresistenzen in der Human- und Veterinärmedizin in Deutschland; Antiinfectives Intelligence: Rheinbach, Germany, 2016. [Google Scholar]
- Zetts, R.M.; Stoesz, A.; Smith, B.A.; Hyun, D.Y. Outpatient Antibiotic Use and the Need for Increased Antibiotic Stewardship Efforts. Pediatrics 2018, 141, e20174124. [Google Scholar] [CrossRef] [Green Version]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Spurling, G.K.; Del Mar, C.B.; Dooley, L.; Foxlee, R. Delayed antibiotics for symptoms and complications of respiratory infections. Cochrane Database Syst. Rev. 2004, 18, CD004417. [Google Scholar]
- Little, P.; Moore, M.; Kelly, J.; Williamson, I.; Leydon, G.; McDermott, L.; Mullee, M.; Stuart, B.; PIPS Investigators. Delayed antibiotic prescribing strategies for respiratory tract infections in primary care: Pragmatic, factorial, randomised controlled trial. BMJ 2014, 348, g1606. [Google Scholar] [CrossRef] [Green Version]
- Faber, M.S.; Heckenbach, K.; Velasco, E.; Eckmanns, T. Antibiotics for the common cold: Expectations of Germany’s general population. Euro Surveill. 2010, 15, 19655. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=1965 (accessed on 3 February 2021). [CrossRef]
- O’Connor, R.; O’Doherty, J.; O’Regan, A.; Dunne, C. Antibiotic use for acute respiratory tract infections (ARTI) in primary care; what factors affect prescribing and why is it important? A narrative review. Ir. J. Med. Sci. 2018, 187, 969–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverman, M.; Povitz, M.; Sontrop, J.M.; Li, L.; Richard, L.; Cejic, S.; Shariff, S.Z. Antibiotic prescribing for nonbacterial acute upper respiratory infections in elderly persons. Ann. Intern. Med. 2017, 166, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, B.H.; Gjelstad, S.; Foshaug, M.; Høye, S. Antibiotic prescribing for acute respiratory tract infections in Norwegian primary care out-of-hours service. Scand. J. Prim. Health Care 2017, 35, 178–185. [Google Scholar] [CrossRef]
- Ackerman, S.L.; Gonzales, R.; Stahl, M.S.; Metlay, J.P. One size does not fit all: Evaluating an intervention to reduce antibiotic prescribing for acute bronchitis. BMC Health Serv. Res. 2013, 4, 462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, M.; Stuart, B.; Little, P.; Smith, S.; Thompson, M.J.; Knox, K.; van den Bruel, A.; Lown, M.; Mant, D. Predictors of pneumonia in lower respiratory tract infections: 3C prospective cough complication cohort study. Eur. Respir. J. 2017, 50, 1700434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemiengre, M.B.; van Driel, M.L.; Merenstein, D.; Liira, H.; Mäkelä, M.; De Sutter, A.I. Antibiotics for acute rhinosinusitis in adults. Cochrane Database Syst. Rev. 2018, 9, CD006089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Undeland, D.K.; Kowalski, T.J.; Berth, W.L.; Gundrum, J.D. Appropriately prescribing antibiotics for patients with pharyngitis: A physician-based approach vs a nurse-only triage and treatment algorithm. Mayo Clin. Proc. 2010, 85, 1011–1015. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Ding, C.; Yin, S. Severe pneumonia in the elderly: A multivariate analysis of risk factors. Int. J. Clin. Exp. Med. 2015, 8, 12463–12475. [Google Scholar] [PubMed]
- Kornum, J.B.; Thomsen, R.W.; Riis, A.; Lervang, H.H.; Schønheyder, H.C.; Sørensen, H.T. Diabetes, glycemic control, and risk of hospitalization with pneumonia: A population-based case-control study. Diabetes Care 2008, 31, 1541–1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, J.L.; Evans, S.E. Bacterial Pneumonia in Patients with Cancer: Novel Risk Factors and Management. Clin. Chest Med. 2017, 38, 263–277. [Google Scholar] [CrossRef] [PubMed]
- Petursson, P. GPs’ reasons for “non-pharmacological” prescribing of antibiotics A phenomenological study. Scand. J. Prim. Health Care 2005, 23, 120–125. [Google Scholar] [CrossRef]
- Martin, D.; Konrad, M.; Adarkwah, C.C.; Kostev, K. Reduced antibiotic use after initial treatment of acute respiratory infections with phytopharmaceuticals—A retrospective cohort study. Postgrad. Med. 2020, 132, 412–418. [Google Scholar] [CrossRef] [Green Version]
- Wopker, P.M.; Schwermer, M.; Sommer, S.; Längler, A.; Fetz, K.; Ostermann, T.; Zuzak, T.J. Complementary and alternative medicine in the treatment of acute bronchitis in children: A systematic review. Complement. Ther. Med. 2020, 49, 102217. [Google Scholar] [CrossRef]
- Willcox, M.; Donovan, E.; Hu, X.Y.; Elboray, S.; Jerrard, N.; Roberts, N.; Santer, M. Views regarding use of complementary therapies for acute respiratory infections: Systematic review of qualitative studies. Complement. Ther. Med. 2020, 50, 102382. [Google Scholar] [CrossRef]
- Timmer, A.; Günther, J.; Motschall, E.; Rücker, G.; Antes, G.; Kern, W.V. Pelargonium sidoides extract for treating acute respiratory tract infections. Cochrane Database Syst. Rev. 2013, 22, CD006323. [Google Scholar] [CrossRef]
- Baars, E.W.; Belt-van Zoen, E.; Breitkreuz, T.; Martin, D.; Matthes, H.; von Schoen-Angerer, T.; Soldner, G.; Vagedes, J.; van Wietmarschen, H.; Patijn, O.; et al. Corrigendum to “The Contribution of Complementary and Alternative Medicine to Reduce Antibiotic Use: A Narrative Review of Health Concepts, Prevention, and Treatment Strategies”. Evid. Based Complement. Alternat. Med. 2020, 2020, 7089287. [Google Scholar] [CrossRef]
- Anheyer, D.; Cramer, H.; Lauche, R.; Saha, F.J.; Dobos, G. Herbal Medicine in Children with Respiratory Tract Infection: Systematic Review and Meta-Analysis. Acad. Pediatr. 2018, 18, 8–19. [Google Scholar] [CrossRef]
- Koch, A.K.; Klose PLauche, R.; Cramer, H.; Baasch, J.; Dobos, G.J.; Langhorst, J. A Systematic Review of Phytotherapy for Acute Rhinosinusitis. Forsch. Komplementmed. 2016, 23, 165–169. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Patients with Antibiotic Prescription (%) | Patients without Antibiotic Prescription (%) | p Value |
|---|---|---|---|
| n | 356,045 | 784,050 | |
| Age (Mean, SD) | 51.2 (20.1) | 46.3 (20.7) | <0.001 |
| Age <18 | 4.5 | 7.9 | <0.001 |
| Age 18–40 | 26.5 | 32.4 | |
| Age 41–50 | 16.1 | 16.3 | |
| Age 51–60 | 19.2 | 18.6 | |
| Age 61–70 | 14.3 | 10.6 | |
| Age 71–80 | 12.3 | 8.8 | |
| Age >80 | 7.1 | 5.4 | |
| Female sex (%) | 54.9 | 54.2 | <0.001 |
| Private health insurance coverage (%) | 7.2 | 8.2 | <0.001 |
| Acute lower and upper tract respiratory infection diagnosis (%) | |||
| Viral infection of unspecified site | 1.5 | 10.9 | <0.001 |
| Acute nasopharyngitis | 1.6 | 5.4 | |
| Acute sinusitis | 7.6 | 3.2 | |
| Acute pharyngitis | 9.0 | 4.9 | |
| Acute laryngitis and tracheitis | 4.3 | 2.5 | |
| Acute upper respiratory infections of multiple and unspecified sites (J06) | 19.9 | 44.9 | |
| Acute bronchitis | 34.5 | 11.9 | |
| Bronchitis, not specified as acute or chronic | 18.3 | 7.2 | |
| Cough | 3.3 | 9.1 | |
| Co-Diagnoses (documented prior to or on the index date) (%) | |||
| Diabetes | 6.2 | 4.4 | <0.001 |
| Ischemic heart disease/heart failure | 5.3 | 4.8 | <0.001 |
| Renal failure | 1.5 | 1.2 | <0.001 |
| Cancer | 1.9 | 1.5 | 0.352 |
| COPD | 3.3 | 1.9 | <0.001 |
| Asthma | 3.6 | 2.7 | <0.001 |
| Diagnosis of a bacterial infection within 365–31 days prior to the index date (%) | 0.5 | 0.6 | 0.098 |
| Number of patients per practice and quarter (%) | |||
| ≤1000 | 18.4 | 20.7 | <0.001 |
| 1001–1500 | 34.4 | 38.3 | |
| 1501–2000 | 25.4 | 22.5 | |
| >2000 | 21.8 | 18.5 | |
| Western Germany | 83.3 | 82.4 | <0.001 |
| Proportion of antibiotic prescription on all prescriptions per practice per year | |||
| ≤4% | 3.0 | 8.6 | <0.001 |
| >4–≤6% | 29.0 | 45.2 | |
| >6–≤8% | 34.8 | 29.6 | |
| >8–≤10% | 19.5 | 11.9 | |
| >10% | 13.7 | 4.7 | |
| Proportion of phytopharmaceutical prescription on all prescriptions per practice per year (%) | |||
| ≤1% | 39.4 | 37.1 | <0.001 |
| >1–≤2% | 18.7 | 17.2 | |
| >2–≤3% | 15.0 | 14.9 | |
| >3–≤4% | 9.9 | 10.0 | |
| >4% | 17.0 | 20.8 |
| Variable | Patients with Antibiotic Prescription (%) | Patients without Antibiotic Prescription (%) | p Value |
|---|---|---|---|
| n | 28,365 | 280,694 | |
| Age (Mean, SD) | 7.9 (4.7) | 7.6 (4.4) | <0.001 |
| Age <18 | <0.001 | ||
| Age 2–5 | 40.2 | 39.1 | |
| Age 6–12 | 38.7 | 44.5 | |
| Age 13–17 | 21.1 | 16.4 | |
| Female sex (%) | 49.4 | 48.4 | 1.000 |
| Private health insurance coverage (%) | 9.6 | 9.5 | 0.635 |
| Acute lower and upper tract respiratory infection diagnosis (%) | |||
| Viral infection of unspecified site | 6.4 | 17.7 | <0.001 |
| Acute nasopharyngitis | 4.2 | 5.6 | <0.001 |
| Acute sinusitis | 3.1 | 0.6 | <0.001 |
| Acute pharyngitis | 16.3 | 6.7 | <0.001 |
| Acute laryngitis and tracheitis | 3.5 | 3.9 | <0.001 |
| Acute upper respiratory infections of multiple and unspecified sites (J06) | 29.8 | 46.0 | <0.001 |
| Acute bronchitis | 22.2 | 7.5 | <0.001 |
| Bronchitis, not specified as acute or chronic | 9.3 | 3.9 | <0.001 |
| Cough | 5.2 | 8.1 | <0.001 |
| Co-Diagnoses (documented prior to or on the index date) (%) | |||
| Diabetes | 0.1 | 0.1 | 0.294 |
| Ischemic heart disease/heart failure | 0.1 | 0.1 | 0.096 |
| Renal failure | 0.0 | 0.0 | 0.723 |
| Cancer | 0.1 | 0.1 | 0.680 |
| COPD | 4.7 | 4.2 | <0.001 |
| Asthma | 3.4 | 2.9 | <0.001 |
| Diagnosis of a bacterial infection within 365–31 days prior to the index date (%) | 7.4 | 6.5 | <0.001 |
| Number of patients per practice and quarter (%) | |||
| ≤1000 | 9.0 | 10.1 | <0.001 |
| 1001–1500 | 34.5 | 37.5 | |
| 1501–2000 | 34.9 | 35.6 | |
| >2000 | 21.6 | 16.8 | |
| Western Germany (%) | 85.6 | 83.0 | <0.001 |
| Proportion of antibiotic prescription on all prescriptions per practice per year (%) | |||
| ≤4% | 0.0 | 1.5 | <0.001 |
| >4–≤6% | 4.5 | 11.4 | |
| >6–≤8% | 14.9 | 23.3 | |
| >8–≤10% | 27.8 | 29.0 | |
| >10% | 52.9 | 34.7 | |
| Proportion of phytopharmaceutical prescription on all prescriptions per practice per year (%) | |||
| ≤1% | 22.5 | 21.0 | <0.001 |
| >1–≤10 | 32.9 | 31.6 | |
| >10–≤15% | 23.8 | 24.2 | |
| >15% | 20.8 | 23.2 |
| Variable | Odds Ratio (95% CI) | p Value * |
|---|---|---|
| Age 18–40 | Reference | |
| Age 41–50 | 1.20 (1.18–1.22) | <0.001 |
| Age 51–60 | 1.25 (1.23–1.27) | <0.001 |
| Age 61–70 | 1.55 (1.52–1.58) | <0.001 |
| Age 71–80 | 1.56 (1.53–1.59) | <0.001 |
| Age >80 | 1.40 (1.37–1.44) | <0.001 |
| Female | Reference | |
| Male | 0.99 (0.98–1.00) | 0.088 |
| Statutory health insurance | Reference | |
| Private health insurance | 0.89 (0.87–0.91) | <0.001 |
| Acute upper respiratory infections of multiple and unspecified sites | Reference | |
| Viral infection of unspecified site | 0.32 (0.32–0.33) | <0.001 |
| Acute nasopharyngitis | 0.66 (0.64–0.68) | <0.001 |
| Acute sinusitis | 5.32 (5.21–5.44) | <0.001 |
| Acute pharyngitis | 4.18 (4.10–4.27) | <0.001 |
| Acute laryngitis and tracheitis | 3.87 (3.77–3.98) | <0.001 |
| Acute bronchitis | 6.01 (5.93–6.10) | <0.001 |
| Bronchitis, not specified as acute or chronic | 5.22 (5.13–5.30) | <0.001 |
| Cough | 0.77 (0.75–0.79) | <0.001 |
| Co-Diagnoses (documented prior to or on the index date) | ||
| Diabetes | 1.07 (1.05–1.09) | <0.001 |
| Ischemic heart disease/heart failure | 1.01 (0.98–1.03) | 0.492 |
| Renal failure | 0.90 (0.86–0.93) | <0.001 |
| Cancer | 0.97 (0.93–1.00) | 0.061 |
| COPD | 1.24 (1.20–1.27) | <0.001 |
| Asthma | 1.13 (1.10–1.16) | <0.001 |
| Diagnosis of a bacterial infection within 365–30 days prior to the index date | 1.00 (0.93–1.07) | 0.894 |
| Number of patients per practice and quarter | ||
| ≤1000 | Reference | |
| 1001–1500 | 1.03 (1.02–1.05) | <0.001 |
| 1501–2000 | 1.03 (1.01–1.04) | <0.001 |
| >2000 | 1.08 (1.06–1.10) | <0.001 |
| Western Germany | 0.73 (0.72–0.74) | <0.001 |
| Eastern Germany | Reference | |
| Proportion of antibiotic prescription on all prescriptions per practice per year | ||
| ≤4 | Reference | |
| >4–≤6 | 2.16 (2.10–2.21) | <0.001 |
| >6–≤8 | 3.95 (3.84–4.05) | <0.001 |
| >8–≤10 | 5.23 (5.09–5.38) | <0.001 |
| >10 | 9.93 (9.62–10.24) | <0.001 |
| Proportion of phytopharmaceutical prescription on all prescriptions per practice per year | ||
| ≤1 | Reference | |
| >1–≤2 | 0.89 (0.88–0.90) | <0.001 |
| >2–≤3 | 0.64 (0.63–0.66) | <0.001 |
| >3–≤4 | 0.66 (0.64–0.68) | <0.001 |
| >4 | 0.44 (0.43–0.46) | <0.001 |
| Variable | Odds Ratio (95% CI) | p Value * |
|---|---|---|
| Age 2–5 | Reference | |
| Age 6–12 | 0.85 (0.82–0.88) | <0.001 |
| Age 13–17 | 1.21 (1.16–1.26) | <0.001 |
| Female sex | Reference | |
| Male sex | 0.94 (0.91–0.97) | <0.001 |
| Statutory health insurance coverage | Reference | |
| Private health insurance coverage | 1.03 (0.98–1.09) | 0.289 |
| Acute lower and upper respiratory tract infection diagnosis | ||
| Viral infection of unspecified site | 0.57 (0.54–0.61) | <0.001 |
| Acute nasopharyngitis | 1.20 (1.12–1.29) | <0.001 |
| Acute sinusitis | 7.14 (6.44–7.91) | <0.001 |
| Acute pharyngitis | 3.57 (3.39–3.75) | <0.001 |
| Acute laryngitis and tracheitis | 1.43 (1.32–1.55) | <0.001 |
| Acute upper respiratory infections of multiple and unspecified sites (J06) | Reference | |
| Acute bronchitis | 4.55 (4.35–4.76) | <0.001 |
| Bronchitis, not specified as acute or chronic | 3.43 (3.23–3.64) | <0.001 |
| Cough | 1.18 (1.11–1.26) | <0.001 |
| Co-Diagnoses (documented prior to or on the index date) | ||
| Diabetes | 0.89 (0.59–1.32) | 0.552 |
| Ischemic heart disease/heart failure | 1.75 (1.10–2.78) | 0.033 |
| Renal failure | 1.07 (0.24–4.83) | 0.926 |
| Cancer | 1.81 (1.15–2.86) | 0.019 |
| COPD | 1.10 (1.03–1.18) | 0.005 |
| Asthma | 0.88 (0.82–0.95) | 0.002 |
| Diagnosis of a bacterial infection within 365–30 days prior to the index date | 1.09 (1.03–1.16) | 0.002 |
| Number of patients per practice and quarter | ||
| ≤1000 | Reference | |
| 1001–1500 | 1.14 (1.07–1.21) | <0.001 |
| 1501–2000 | 1.20 (1.13–1.27) | <0.001 |
| >2000 | 1.35 (1.26–1.43) | <0.001 |
| Eastern Germany | Reference | |
| Western Germany | 1.07 (1.02–1.13) | 0.006 |
| Proportion of antibiotic prescription on all prescriptions per practice per year | ||
| >4–≤6 | Reference | |
| >6–≤8 | 1.62 (1.49–1.75) | <0.001 |
| >8–≤10 | 2.41 (2.24–2.60) | <0.001 |
| >10 | 4.00 (3.71–3.30) | <0.001 |
| Proportion of phytopharmaceutical prescription on all prescriptions per practice per year | ||
| ≤1 | Reference | |
| >1–≤10 | 0.20 (0.18–0.23) | <0.001 |
| >10–≤15 | 0.24 (0.87–0.97) | <0.001 |
| >15 | 0.26 (0.23–0.30) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kern, W.V.; Kostev, K. Prevalence of and Factors Associated with Antibiotic Prescriptions in Patients with Acute Lower and Upper Respiratory Tract Infections—A Case-Control Study. Antibiotics 2021, 10, 455. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10040455
Kern WV, Kostev K. Prevalence of and Factors Associated with Antibiotic Prescriptions in Patients with Acute Lower and Upper Respiratory Tract Infections—A Case-Control Study. Antibiotics. 2021; 10(4):455. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10040455
Chicago/Turabian StyleKern, Winfried V., and Karel Kostev. 2021. "Prevalence of and Factors Associated with Antibiotic Prescriptions in Patients with Acute Lower and Upper Respiratory Tract Infections—A Case-Control Study" Antibiotics 10, no. 4: 455. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10040455