
Evaluation of Aerosol Therapy during the Escalation of Care in a Model of Adult Cystic Fibrosis



Abstract
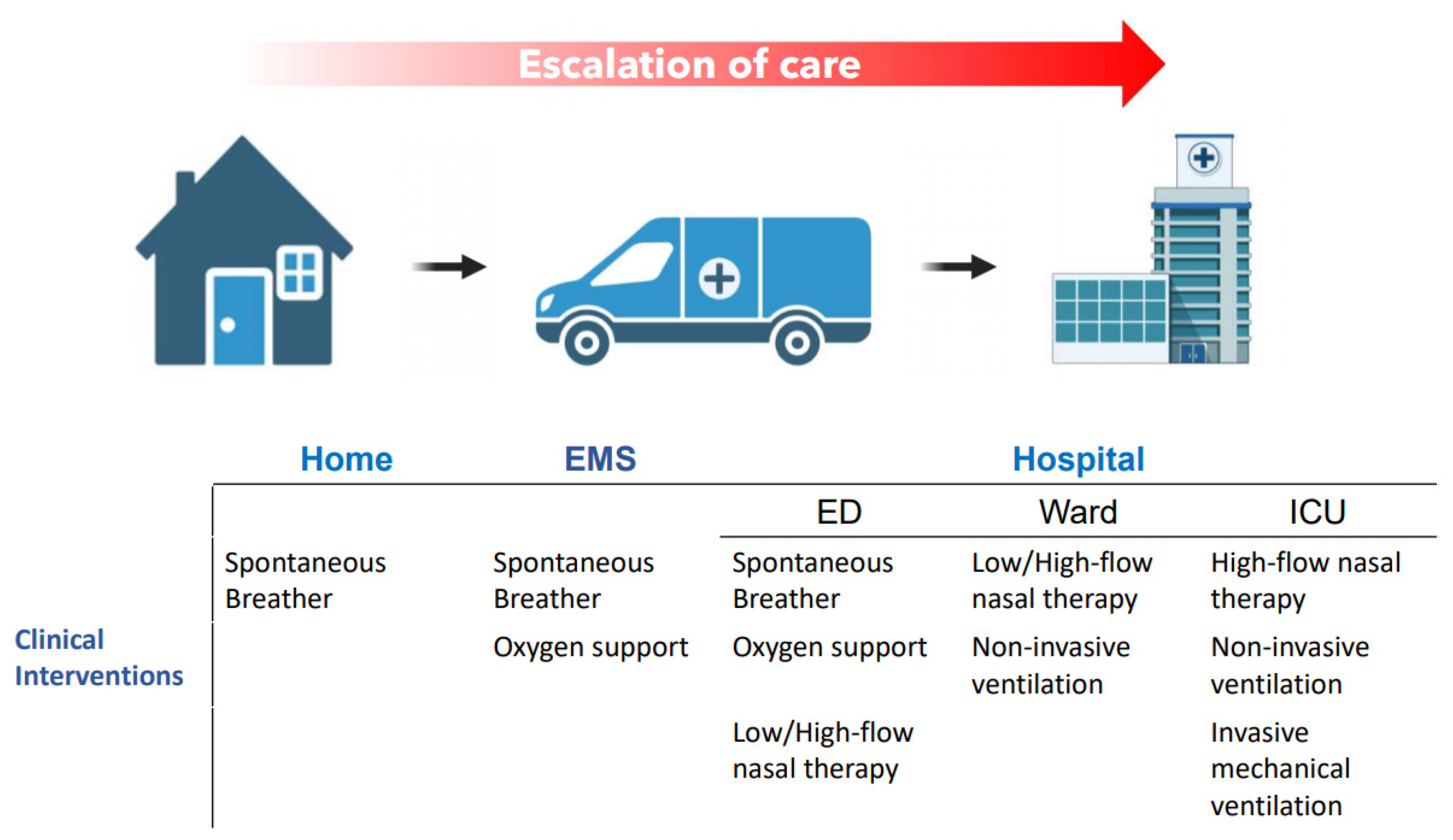
:1. Introduction
2. Results
2.1. Respirable Fraction Aerosol Droplet Size Characterisation
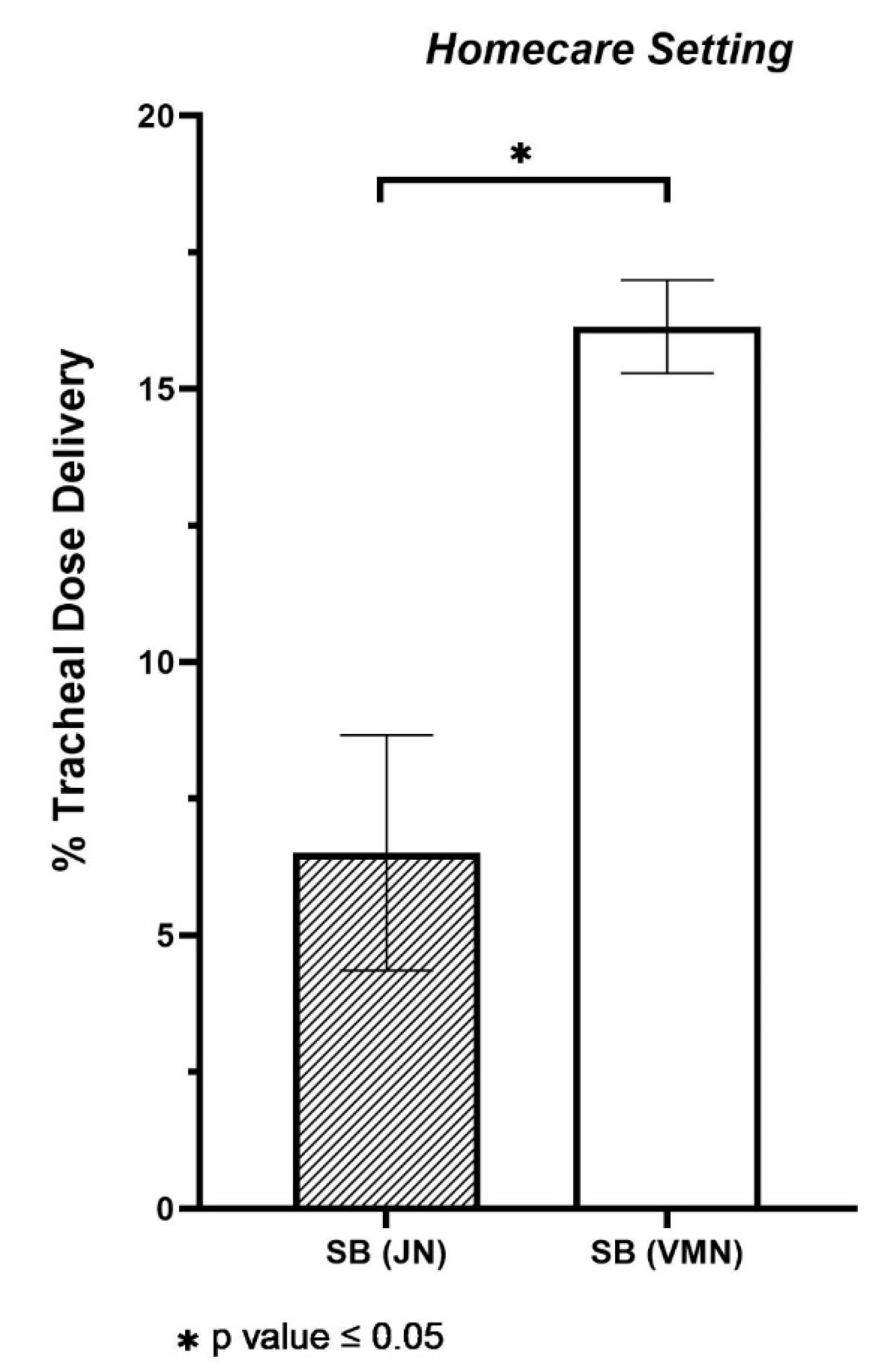
2.2. Simulated Aerosol Delivery during Spontaneous Breathing in the Homecare Setting
2.3. Simulated Aerosol Delivery in the Hospital Setting
2.3.1. Emergency Department
2.3.2. Ward/Intensive Care Unit
3. Discussion
4. Materials and Methods
4.1. Nebulisers
4.2. Respirable Fraction Aerosol Droplet Size Characterisation
4.3. Determination of Tracheal Dose
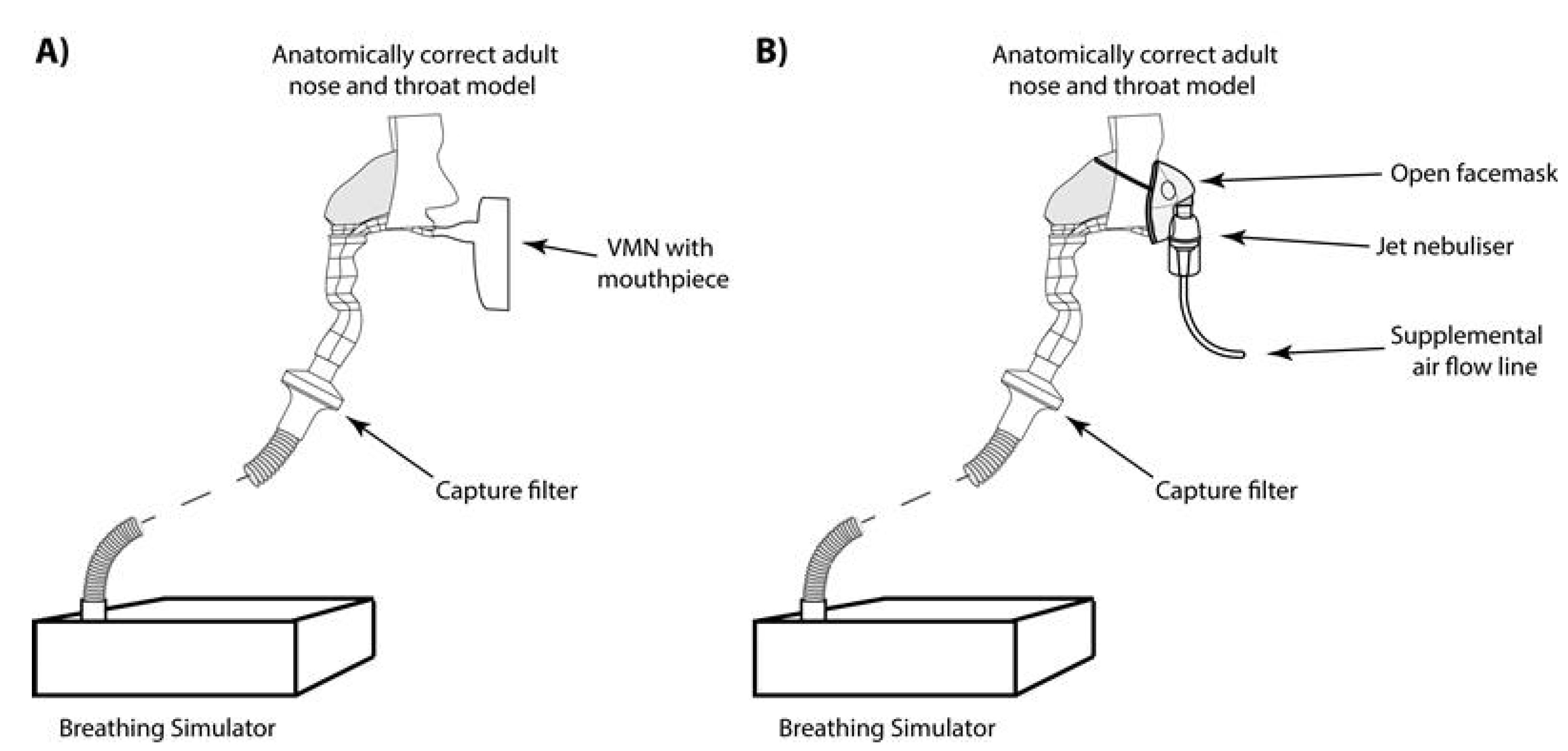
4.4. Simulated Aerosol Delivery during Spontaneous Breathing
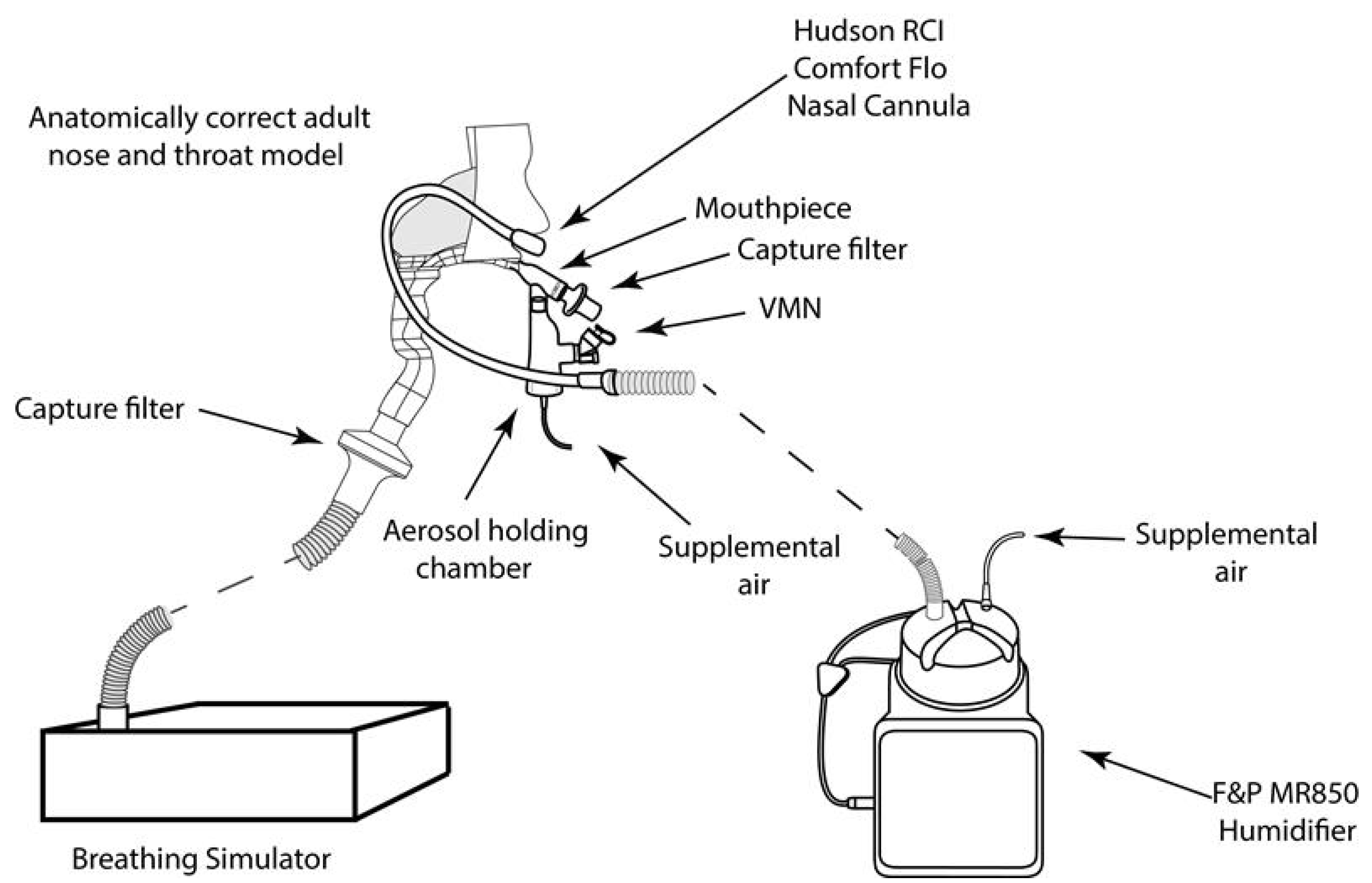
4.5. Simulated Aerosol Delivery during A Non-Invasive Patient Intervention–Nasal Oxygen Support
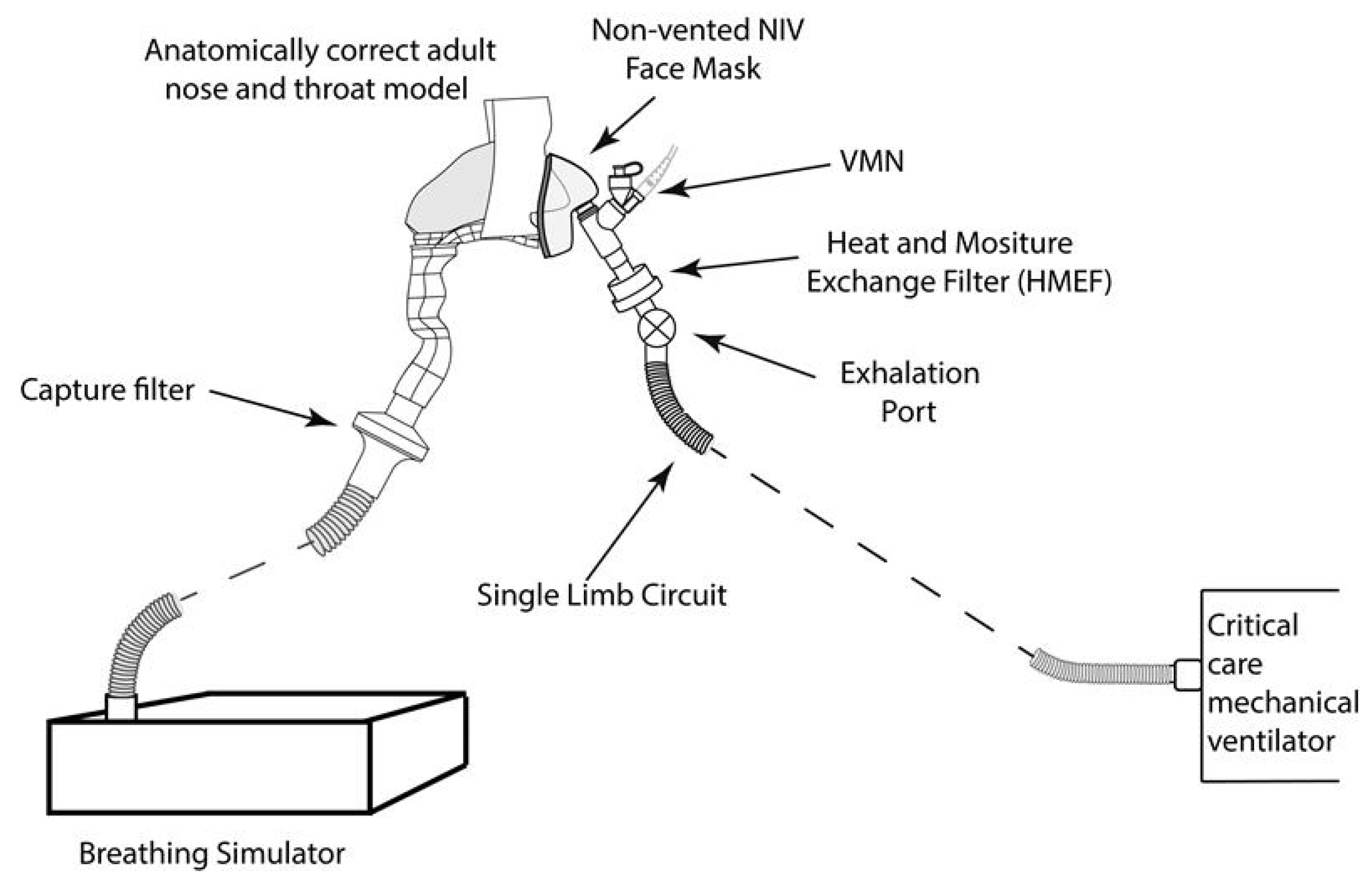
4.6. Simulated Aerosol Delivery during Mask-Mediated Non-Invasive Ventilation (NIV)
4.7. Simulated Aerosol Delivery during Endotracheal Tube-Mediated Invasive Mechanical Ventilation (IMV)
4.8. Statistical Analysis
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kerem, B.; Rommens, J.M.; A Buchanan, J.; Markiewicz, D.; Cox, T.K.; Chakravarti, A.; Buchwald, M.; Tsui, L.C. Identification of the cystic fibrosis gene: Genetic analysis. Science 1989, 245, 1073–1080. [Google Scholar] [CrossRef] [Green Version]
- Welsh, M.J.; Smith, A.E. Molecular mechanisms of CFTR chloride channel dysfunction in cystic fibrosis. Cell 1993, 73, 1251–1254. [Google Scholar] [CrossRef]
- Fernandez, E.; De Santi, C.; De Rose, V.; Greene, C.M. CFTR dysfunction in cystic fibrosis and chronic obstructive pulmonary disease. Expert Rev. Respir. Med. 2018, 12, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.L.; Burns, J.L.; Ramsey, B.W. Pathophysiology and Management of Pulmonary Infections in Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2003, 168, 918–951. [Google Scholar] [CrossRef] [PubMed]
- Boucher, R.C. Cystic fibrosis: A disease of vulnerability to airway surface dehydration. Trends Mol. Med. 2007, 13, 231–240. [Google Scholar] [CrossRef]
- Davis, P.B. Cystic Fibrosis Since 1938. Am. J. Respir. Crit. Care Med. 2006, 173, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoenderdos, K.; Condliffe, A. The neutrophil in chronic obstructive pulmonary disease. Am. J. Respir. Cell. Mol. Biol. 2013, 48, 531–539. [Google Scholar] [CrossRef] [PubMed]
- King, P.; Holdsworth, S.; Freezer, N.; Holmes, P. Bronchiectasis. Intern. Med. J. 2006, 36, 729–737. [Google Scholar] [CrossRef]
- Dickinson, K.M.; Collaco, J.M. Cystic fibrosis. Pediatr Rev. Am. Acad. Pediatrics 2021, 42, 55–65. Available online: https://pedsinreview.aappublications.org/content/42/2/55 (accessed on 11 March 2021). [CrossRef]
- Bhatt, J.M. Treatment of pulmonary exacerbations in cystic fibrosis. Eur. Respir. Rev. Eur. Respir. Soc. 2013, 205–216. Available online: http://ow.ly/mK5df (accessed on 12 March 2021). [CrossRef] [Green Version]
- Borsje, P.; De Jongste, J.C.; Tiddens, H.A. Aerosol therapy in cystic fibrosis: A survey of 54 CF centers. Pediatr. Pulmonol. 2000, 30, 368–376. [Google Scholar] [CrossRef]
- Mogayzel, P.J.; Naureckas, E.T.; Robinson, K.A.; Mueller, G.; Hadjiliadis, D.; Hoag, J.B.; Lubsch, L.; Hazle, L.; Sabadosa, K.; Marshall, B.; et al. Cystic Fibrosis Pulmonary Guidelines. Am. J. Respir. Crit. Care Med. 2013, 187, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Labiris, N.R.; Dolovich, M.B. Pulmonary drug delivery. Part I: Physiological factors affecting therapeutic effectiveness of aerosolized medications. Br. J. Clin. Pharmacol. 2003, 588–599. [Google Scholar] [CrossRef] [PubMed]
- Goss, C.H. Acute Pulmonary Exacerbations in Cystic Fibrosis. Semin. Respir. Crit. Care Med. 2019, 40, 792–803. [Google Scholar] [CrossRef]
- O’Callaghan, C.; White, J.; Jackson, J.; Crosby, D.; Dougill, B.; Bland, H. The Effects of Heliox on the Output and Particle-Size Distribution of Salbutamol Using Jet and Vibrating Mesh Nebulizers. J. Aerosol Med. 2007, 20, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Ehrmann, S. Vibrating Mesh Nebulisers—Can Greater Drug Delivery to the Airways and Lungs Improve Respiratory Outcomes? Eur. Respir. Pulm. Dis. Touch Med. Media 2018, 4, 33. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 203, 24–36. [Google Scholar] [CrossRef]
- Respiratory care committee of Chinese Thoracic Society. Expert consensus on protective measures related to respiratory therapy in patients with severe coronavirus infection. Zhonghua Jie He He Hu Xi Za Zhi 2020, 17, E020. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/32077661 (accessed on 11 March 2021).
- AARC. American Association for Respiratory Care (AARC) 2020. Available online: https://www.aarc.org/wp-content/uploads/2020/03/guidance-document-SARS-COVID19.pdf (accessed on 11 March 2021).
- Kulkarni, A.P.; Kumar, G.P.; Gopal, P.B. Airway Management and Related Procedures in Critically Ill COVID-19 Patients: Position Statement of the Indian Society of Critical Care Medicine. Indian J. Crit. Care Med. 2020, 24, 630–642. [Google Scholar] [CrossRef]
- Gómez, C.C.; Rodríguez, Ó.P.; Torné, M.L.; Santaolalla, C.E.; Jiménez, J.F.M.; Fernández, J.G. Clinical Consensus Recommendations Regarding Non-Invasive Respiratory Support in the Adult Patient with Acute Respiratory Failure Secondary to SARS-CoV-2 infection. Arch. Bronconeumol. 2020, 56, 11–18. Available online: https://pubmed.ncbi.nlm.nih.gov/32336563/ (accessed on 11 March 2021).
- Usmani, O.S.; Biddiscombe, M.F.; Barnes, P.J. Regional Lung Deposition and Bronchodilator Response as a Function of β2-Agonist Particle Size. Am. J. Respir. Crit. Care Med. 2005, 172, 1497–1504. [Google Scholar] [CrossRef]
- Steckel, H.; Eskandar, F. Factors affecting aerosol performance during nebulization with jet and ultrasonic nebulizers. Eur. J. Pharm. Sci. 2003, 19, 443–455. [Google Scholar] [CrossRef]
- Ghazanfari, T.; Elhissi, A.M.; Ding, Z.; Taylor, K.M. The influence of fluid physicochemical properties on vibrating-mesh nebulization. Int. J. Pharm. 2007, 339, 103–111. [Google Scholar] [CrossRef]
- Mc Callion, O.N.M.; Patel, M.J. Viscosity effects on nebulisation of aqueous solutions. Int. J. Pharm. 1996, 130, 245–249. [Google Scholar] [CrossRef]
- Najlah, M.; Vali, A.; Taylor, M.; Arafat, B.T.; Ahmed, W.; Phoenix, D.A.; Taylor, K.M.; Elhissi, A. A study of the effects of sodium halides on the performance of air-jet and vibrating-mesh nebulizers. Int. J. Pharm. 2013, 456, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, J.N.; Hatley, R.H.; Denyer, J.; Von Hollen, D. Mesh nebulizers have become the first choice for new nebulized pharmaceutical drug developments. Ther. Deliv. 2018, 9, 121–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pritchard, J.N. Nebulized drug delivery in respiratory medicine: What does the future hold? Ther. Deliv. 2017, 8, 391–399. [Google Scholar] [CrossRef]
- Rosenfeld, M.; Emerson, J.; Astley, S.; Joy, P.; Williams-Warren, J.; Standaert, T.A.; Yim, D.L.; Crist, D.; Thykkuttathil, M.; Torrence, M.; et al. Home nebulizer use among patients with cystic fibrosis. J. Pediatr. 1998, 132, 125–131. [Google Scholar] [CrossRef]
- Nickerson, C.; Von Hollen, D.; Garbin, S.; Doty, K.; Jasko, J.; Cain, C. Preference and quality of life of adult chronic obstructive lung disease (COPD) patients when using a novel mesh nebulizer compared to traditional jet nebulizer (TJN). Airway Pharmacol. Treat. 2020, 56, 640. [Google Scholar] [CrossRef]
- Dugernier, J.; Hesse, M.; Vanbever, R.; Depoortere, V.; Roeseler, J.; Michotte, J.-B.; Laterre, P.-F.; Jamar, F.; Reychler, G. SPECT-CT Comparison of Lung Deposition using a System combining a Vibrating-mesh Nebulizer with a Valved Holding Chamber and a Conventional Jet Nebulizer: A Randomized Cross-over Study. Pharm. Res. 2016, 34, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Adorni, G.; Seifert, G.; Buttini, F.; Colombo, G.; Stecanella, L.A.; Krämer, I.; Rossi, A. Aerosolization Performance of Jet Nebulizers and Biopharmaceutical Aspects. Pharmaceutics 2019, 11, 406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrath, J.A.; O’Sullivan, A.; Bennett, G.; O’Toole, C.; Joyce, M.; Byrne, M.A.; MacLoughlin, R. Investigation of the Quantity of Exhaled Aerosols Released into the Environment during Nebulisation. Pharmaceutics 2019, 11, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurley, P.; Smye, S.; Cunliffe, H. Assessment of Antibiotic Aerosol Generation Using Commercial Jet Nebulizers. J. Aerosol Med. 1994, 7, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.P.; Pellow, P.G.; Clay, M.M.; Clarke, S.W. Evaluation of jet nebulisers for use with gentamicin solution. Thorax 1985, 40, 671–676. [Google Scholar] [CrossRef] [Green Version]
- Bell, S.C.; Mall, M.A.; Gutierrez, H.; Macek, M.; Madge, S.; Davies, J.C. The future of cystic fibrosis care: A global perspective. Lancet Respir. Med. 2020, 65–124. Available online: https://pubmed.ncbi.nlm.nih.gov/31570318/ (accessed on 13 January 2021).
- Smyth, A.R.; Bell, S.C.; Bojcin, S.; Bryon, M.; Duff, A.; Flume, P.; Kashirskaya, N.; Munck, A.; Ratjen, F.; Schwarzenberg, S.J.; et al. European Cystic Fibrosis Society Standards of Care: Best Practice guidelines. J. Cyst. Fibros. 2014, 13, S23–S42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunne, R.B.; Shortt, S. Comparison of bronchodilator administration with vibrating mesh nebulizer and standard jet nebulizer in the emergency department. Am. J. Emerg. Med. 2018, 36, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Moody, G. Comparison of Vibrating Mesh Nebulizer Versus Jet Nebulizer in the Pediatric Asthma Patient: A Randomized Controlled Trial. Respir. Care 2019, 64, 3217971. [Google Scholar]
- Cantu, T.; Jenkins, L. Quality Improvement Project to Compare Vibrating Mesh Nebulizer Therapy with Hour Long Jet Nebulizer Therapy for Albuterol Delivery in Asthma and Reactive Airway Disorder Patients in a Pediatric Emergency Department. Respir. Care 2019, 64, 3238888. [Google Scholar]
- Caille, V.; Ehrmann, S.; Boissinot, E.; Perrotin, D.; Diot, P.; Dequin, P.-F. Influence of Jet Nebulization and Oxygen Delivery on the Fraction of Inspired Oxygen: An Experimental Model. J. Aerosol Med. Pulm. Drug Deliv. 2009, 22, 255–261. [Google Scholar] [CrossRef]
- Forde, É.; Kelly, G.; Sweeney, L.; Fitzgerald-Hughes, D.; MacLoughlin, R.; Devocelle, M. Vibrating Mesh Nebulisation of Pro-Antimicrobial Peptides for Use in Cystic Fibrosis. Pharmaceutics 2019, 11, 239. [Google Scholar] [CrossRef] [Green Version]
- Alcoforado, L.; Ari, A.; Barcelar, J.D.M.; Brandão, S.C.S.; Fink, J.B.; De Andrade, A.D. Impact of Gas Flow and Humidity on Trans-Nasal Aerosol Deposition via Nasal Cannula in Adults: A Randomized Cross-Over Study. Pharmaceutics 2019, 11, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, G.; Joyce, M.; Sweeney, L.; MacLoughlin, R. In Vitro Determination of the Main Effects in the Design of High-Flow Nasal Therapy Systems with Respect to Aerosol Performance. Pulm. Ther. 2018, 4, 73–86. [Google Scholar] [CrossRef] [Green Version]
- Réminiac, F.; Vecellio, L.; Mac Loughlin, R.; Le Pennec, D.; Cabrera, M.; Vourc’H, N.H.; Fink, J.B.; Ehrmann, S. Nasal high flow nebulization in infants and toddlers: An in vitro and in vivo scintigraphic study. Pediatr. Pulmonol. 2016, 52, 337–344. [Google Scholar] [CrossRef] [PubMed]
- McGrath, J.A.; O’Toole, C.; Bennett, G.; Joyce, M.; Byrne, M.A.; MacLoughlin, R. Investigation of Fugitive Aerosols Released into the Environment during High-Flow Therapy. Pharmaceutics 2019, 11, 254. [Google Scholar] [CrossRef] [Green Version]
- Mirabelli, M.C.; Zock, J.-P.; Plana, E.; Antó, J.M.; Benke, G.; Blanc, P.D.; Dahlman-Höglund, A.; Jarvis, D.L.; Kromhout, H.; Lillienberg, L.; et al. Occupational risk factors for asthma among nurses and related healthcare professionals in an international study. Occup. Environ. Med. 2007, 64, 474–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beach, J.R.; Campbell, M.; Andrews, D.J. Exposure of health care workers to pentamidine isethionate. Occup. Med. 1999, 49, 243–245. [Google Scholar] [CrossRef] [Green Version]
- Tsai, R.J.; Boiano, J.M.; Steege, A.L.; Sweeney, M.H. Precautionary Practices of Respiratory Therapists and Other Health-Care Practitioners Who Administer Aerosolized Medications. Respir. Care 2015, 60, 1409–1417. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Fink, J.B.; MacLoughlin, R.; Dhand, R. A narrative review on trans-nasal pulmonary aerosol delivery. Crit. Care 2020, 24, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Filho, V.C.; Alcoforado, L.; Rattes, C.; Paiva, D.N.; Brandão, S.C.S.; Fink, J.B.; de Andrade, A.D. A mesh nebulizer is more effective than jet nebulizer to nebulize bronchodilators during non-invasive ventilation of subjects with COPD: A randomized controlled trial with radiolabeled aerosols. Respir. Med. 2019, 153, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Dugernier, J.; Reychler, G.; Wittebole, X.; Roeseler, J.; Depoortere, V.; Sottiaux, T.; Michotte, J.-B.; Vanbever, R.; Dugernier, T.; Goffette, P.; et al. Aerosol delivery with two ventilation modes during mechanical ventilation: A randomized study. Ann. Intensiv. Care 2016, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Fauroux, B.; Itti, E.; Pigeot, J.; Isabey, D.; Meignan, M.; Ferry, G. Optimization of aerosol deposition pressure support in children with cystic fibrosis: An experimental and clinical study. Am. J. Respir. Crit. Care Med. 2000, 162, 2265–2271. Available online: https://pubmed.ncbi.nlm.nih.gov/11112150/ (accessed on 14 March 2021).
- Ari, A.; Atalay, O.T.; Harwood, R.; Sheard, M.M.; A Aljamhan, E.; Fink, J.B. Influence of nebulizer type, position, and bias flow on aerosol drug delivery in simulated pediatric and adult lung models during mechanical ventilation. Respir. Care 2010, 55, 281–289. [Google Scholar]
- O’Toole, C.; McGrath, J.A.; Joyce, M.; Bennett, G.; Byrne, M.A.; MacLoughlin, R. Fugitive Aerosol Therapy Emissions during Mechanical Ventilation: In Vitro Assessment of the Effect of Tidal Volume and Use of Protective Filters. Aerosol Air Qual. Res. 2020, 20, 2604–2613. [Google Scholar] [CrossRef]
- Joyce, M.; McGrath, J.A.; Mac Giolla Eain, M.; O’Sullivan, A.; Byrne, M.; MacLoughlin, R. Nebuliser Type Influences Both Patient-Derived Bioaerosol Emissions and Ventilation Parameters during Mechanical Ventilation. Pharmaceutics 2021, 13, 199. Available online: https://0-www-mdpi-com.brum.beds.ac.uk/1999-4923/13/2/199 (accessed on 11 March 2021). [CrossRef]
- Hibbitts, A.; O’Mahony, A.; Forde, E.; Nolan, L.; Ogier, J.; Desgranges, S.; Darcy, R.; MacLoughlin, R.; O’Driscoll, C.; Cryan, S.-A.; et al. Early-Stage Development of Novel Cyclodextrin-siRNA Nanocomplexes Allows for Successful Postnebulization Transfection of Bronchial Epithelial Cells. J. Aerosol Med. Pulm. Drug Deliv. 2014, 27, 466–477. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, L.; McCloskey, A.P.; Higgins, G.; Ramsey, J.M.; Cryan, S.-A.; MacLoughlin, R. Effective nebulization of interferon-γ using a novel vibrating mesh. Respir. Res. 2019, 20, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moody, G.B.; Ari, A. Quantifying continuous nebulization via high flow nasal cannula and large volume nebulizer in a pediatric model. Pediatr. Pulmonol. 2020, 55, 2596–2602. [Google Scholar] [CrossRef] [PubMed]
- Rygg, A.; Longest, P.W. Absorption and Clearance of Pharmaceutical Aerosols in the Human Nose: Development of a CFD Model. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 416–431. [Google Scholar] [CrossRef]
- Golshahi, L.; Longest, P.W.; Azimi, M.; Syed, A.; Hindle, M. Intermittent Aerosol Delivery to the Lungs During High-Flow Nasal Cannula Therapy. Respir. Care 2014, 59, 1476–1486. [Google Scholar] [CrossRef]
- Hart, N.; Polkey, M.I.; Clément, A.; Boulé, M.; Moxham, J.; Lofaso, F.; Fauroux, B. Changes in Pulmonary Mechanics with Increasing Disease Severity in Children and Young Adults with Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2002, 166, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Tiddens, H.; Koopman, L.; Lambert, R.; Elliott, W.M.; Hop, W.; Van Der Mark, T.W.; De Boer, W.J.; De Jongste, J. Cartilaginous airway wall dimensions and airway resistance in cystic fibrosis lungs. Eur. Respir. J. 2000, 15, 735–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouby, J.J.; Sole-Lleonart, C.; Rello, J.; Monsel, A.; Constantin, J.M.; Bouglé, A. Ventilator-associated pneumonia caused by multidrug-resistant Gram-negative bacteria: Understanding nebulization of aminoglycosides and colistin. Intensive Care Med. 2020, 46, 766–770. Available online: https://pubmed.ncbi.nlm.nih.gov/31915838/ (accessed on 10 March 2021).
- Galindo-Filho, V.C.; Ramos, M.E.; Rattes, C.S.F.; Barbosa, A.K.; Brandão, D.C.; Brandão, S.C.S.; Fink, J.B.; De Andrade, A.D. Radioaerosol Pulmonary Deposition Using Mesh and Jet Nebulizers During Noninvasive Ventilation in Healthy Subjects. Respir. Care 2015, 60, 1238–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Concentration | Manufacturer | VMD (μm) | Flow Rate (mL/min) | FPF (%) <5 μm | FPF (%) <3 μm | FPF (%) 1–5 μm |
|---|---|---|---|---|---|---|---|
| Saline | 0.9% | BBraun, Ireland | 4.43 ± 0.01 | 0.45 ± 0.01 | 57.45 ± 0.08 | 28.59 ± 0.07 | 56.05 ± 0.03 |
| Salbutamol | 2.5 mg/2.5 mL | GlaxoSmithKline | 4.07 ± 0.43 | 0.46 ± 0.01 | 61.38 ± 0.38 | 34.66 ± 0.25 | 56.11 ± 0.59 |
| Genticin | 80 mg/2 mL | Amdipharm | 4.21 ± 0.01 | 0.48 ± 0.01 | 59.77 ± 0.07 | 32.49 ± 0.21 | 55.87 ± 0.34 |
| Tobramycin | 80 mg/2 mL | Hospira | 4.25 ± 0.01 | 0.47 ± 0.01 | 59.28 ± 0.10 | 31.85 ± 0.11 | 56.15 ± 0.27 |
| Likacin | 500 mg/2 mL | TitoLare | 4.78 ± 0.01 | 0.51 ± 0.01 | 52.08 ± 0.08 | 31.25 ± 0.04 | 43.11 ± 0.13 |
| Colistin | 0.25 million IU/4 mL | Teva | 4.05 ± 0.03 | 0.21 ± 0.01 | 57.97 ± 0.43 | 39.45 ± 0.51 | 44.97 ± 0.53 |
| Simulated Aerosol Delivery Test Scenario | Nebuliser Type | Interface | Simulated Breath Parameters |
|---|---|---|---|
| Spontaneous breathing (SB) | VMN | Mouthpiece | Vt 410 mL RR 22 BPM I:E Ratio 1:2 [62,63] |
| JN | Open facemask | ||
| Non-invasive patient intervention nasal oxygen | VMN | Nasal cannula with LFNT at 10 LPM | |
| VMN | Nasal cannula with HFNT at 60 LPM | ||
| Non-invasive ventilation (NIV) | VMN | Non-vented NIV mask | |
| Invasive mechanical ventilation (IMV) | VMN | Endotracheal tube | Vt 550 mL RR 13 BPM I:E Ratio 1:2 [64] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández Fernández, E.; Joyce, M.; O’Sullivan, A.; MacLoughlin, R. Evaluation of Aerosol Therapy during the Escalation of Care in a Model of Adult Cystic Fibrosis. Antibiotics 2021, 10, 472. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050472
Fernández Fernández E, Joyce M, O’Sullivan A, MacLoughlin R. Evaluation of Aerosol Therapy during the Escalation of Care in a Model of Adult Cystic Fibrosis. Antibiotics. 2021; 10(5):472. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050472
Chicago/Turabian StyleFernández Fernández, Elena, Mary Joyce, Andrew O’Sullivan, and Ronan MacLoughlin. 2021. "Evaluation of Aerosol Therapy during the Escalation of Care in a Model of Adult Cystic Fibrosis" Antibiotics 10, no. 5: 472. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050472