
Pharmacokinetics and Pharmacodynamics of Cefepime in Adults with Hematological Malignancies and Febrile Neutropenia after Chemotherapy

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Medication Dosage and Administration
2.3. Blood Sampling
2.4. Drug Measurement
2.5. Pharmacokinetic Modeling
2.6. Pharmacodynamic Evaluation
2.7. Statistical Analysis
3. Results
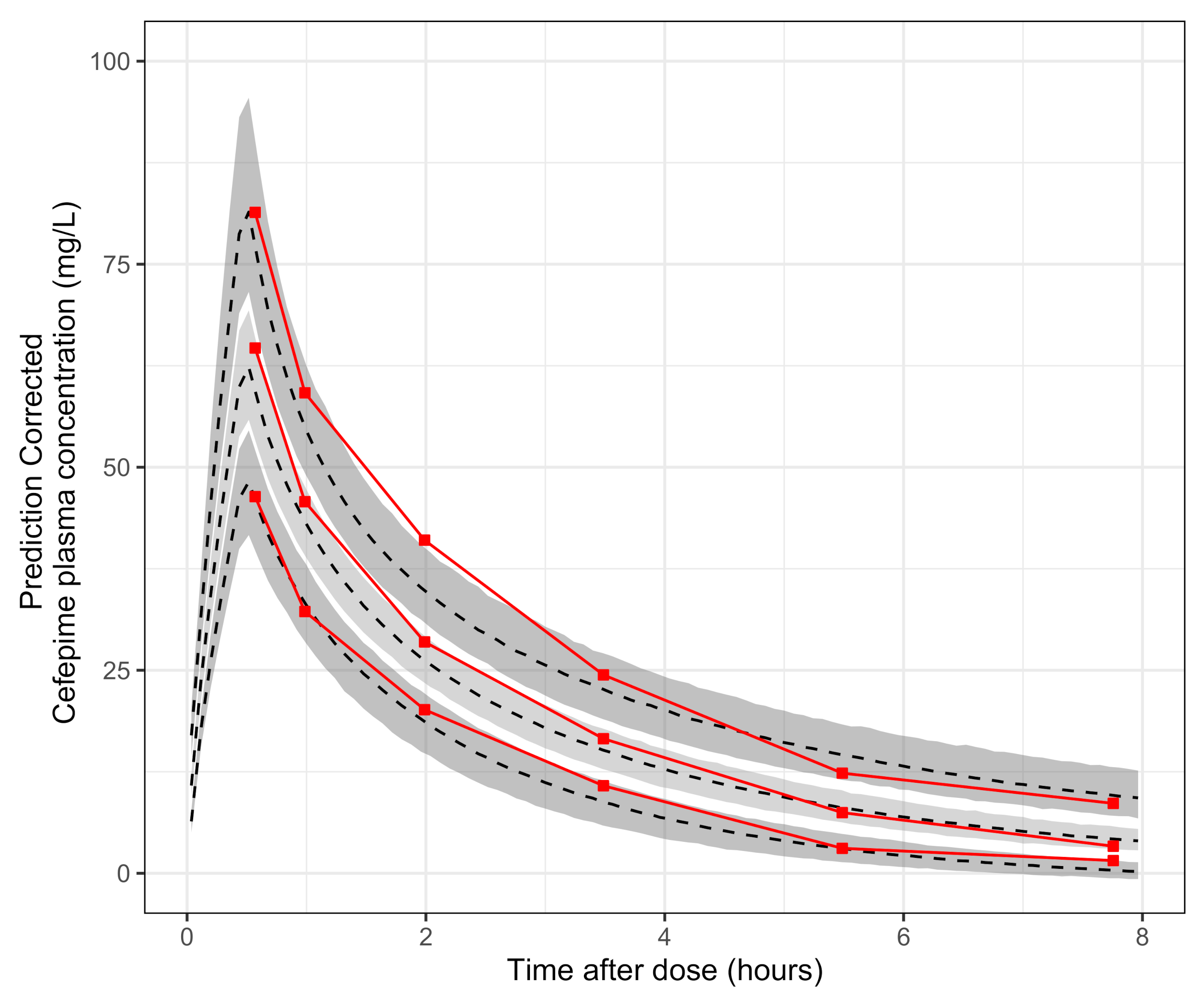
3.1. Pharmacokinetic Results
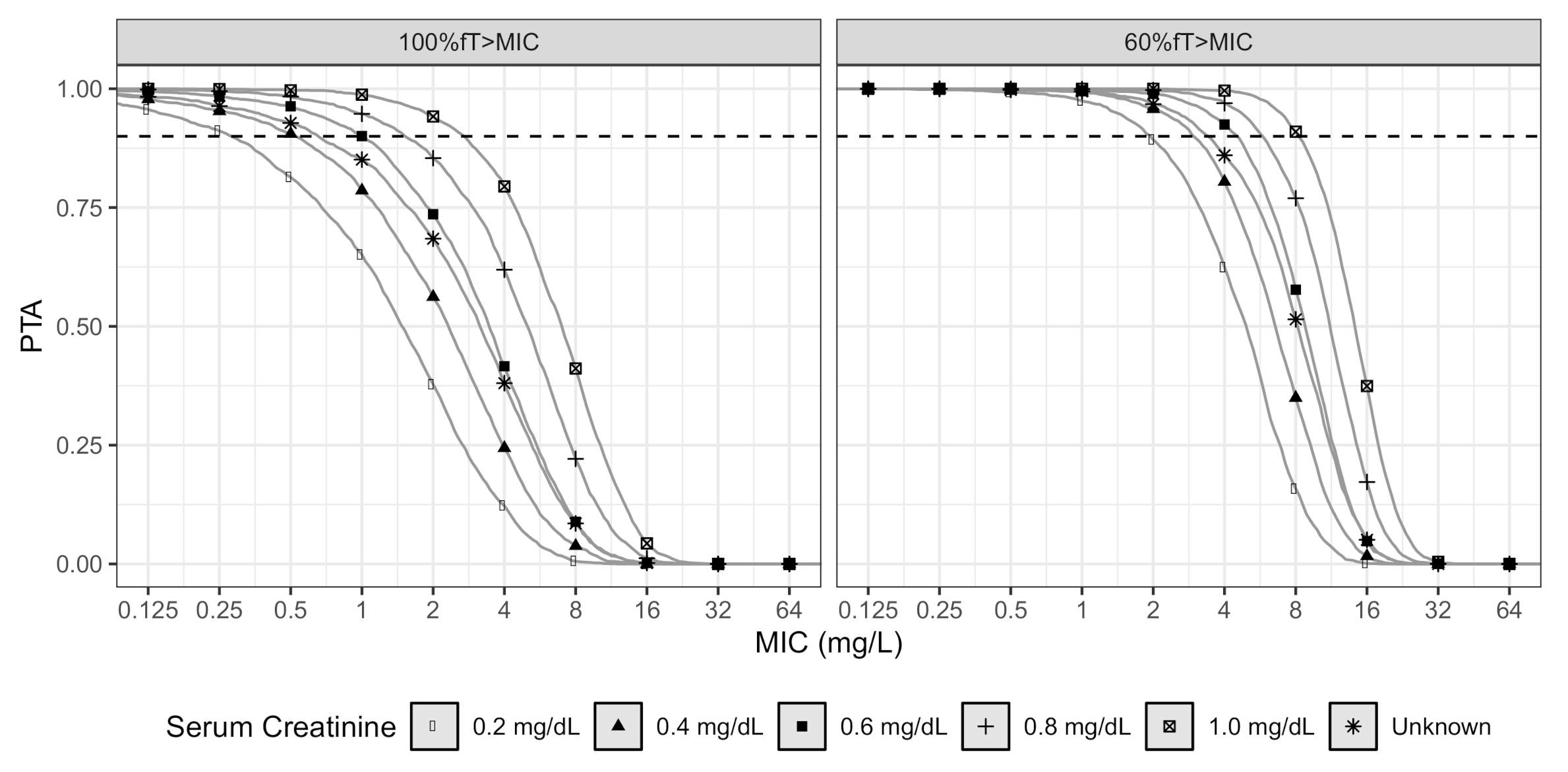
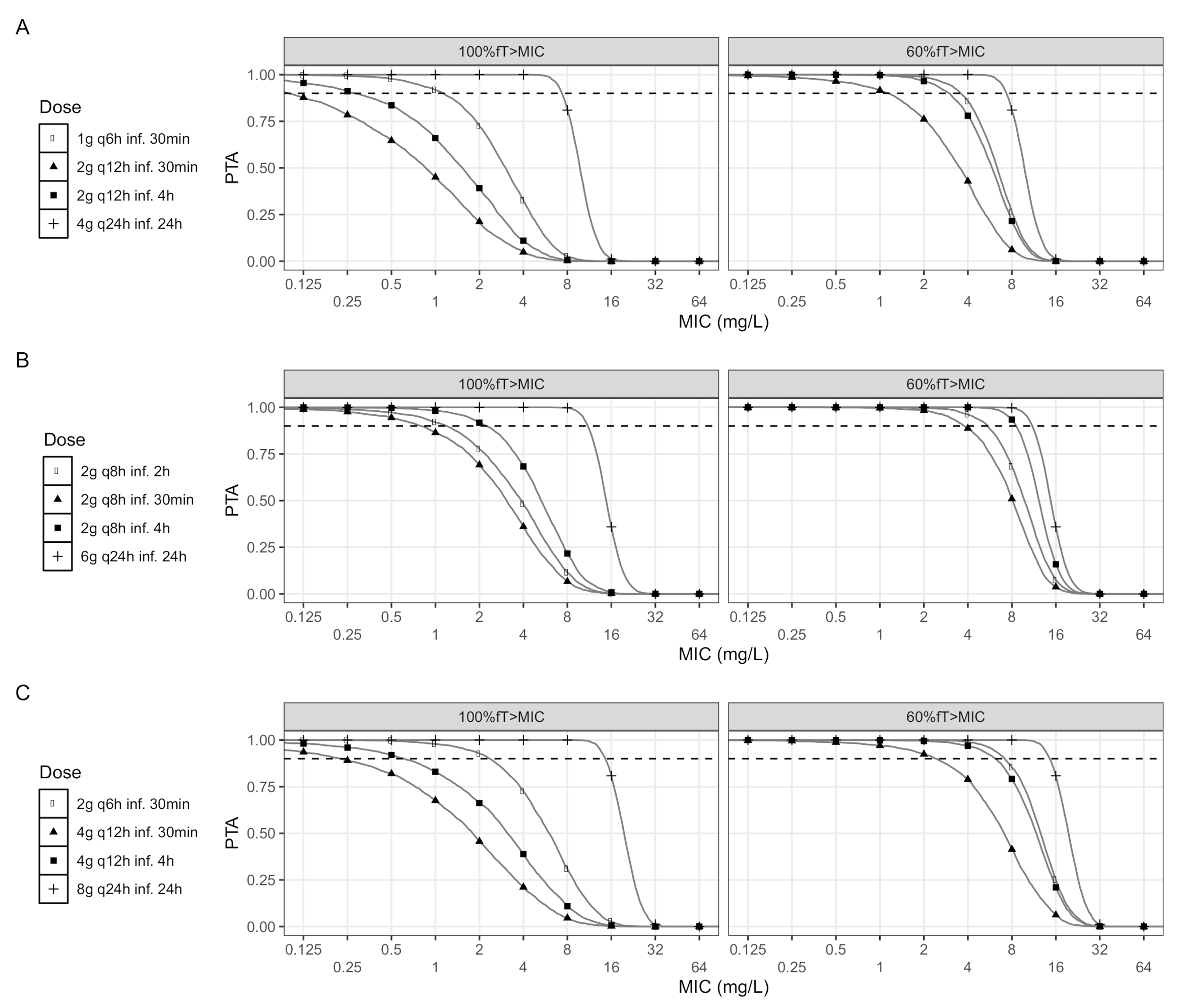
3.2. Pharmacodynamic Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FEP | Cefepime |
| CIFN | chemotherapy-induced febrile neutropenia |
| PK | Pharmacokinetics |
| PK | Pharmacodynamics |
| Volume of distribution | |
| Clearance | |
| Time of free drug concentration above MIC | |
| INC | Instituto Nacional de Cancerología |
| ANC | Absolute neutrophil count |
| Serum creatinine | |
| eGFR | Estimated glomerular filtration rate |
| CV | Coefficient of variation |
| LLOQ | Lower limit of quantification |
| SAEM | Stochastic approach of the expectation–maximization algorithm |
| pcVPC | prediction corrected visual predictive check |
| PTA | Probability of target attainment |
| CFR | Cumulative fraction of response |
References
- Rolston, K.V.I. Neutropenic Fever and Sepsis: Evaluation and Management. In Infectious Complications Cancer Patients; Stosor, V., Zembower, T.R., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2014; pp. 181–202. [Google Scholar] [CrossRef]
- Theuretzbacher, U. Pharmacokinetic and pharmacodynamic issues for antimicrobial therapy in patients with cancer. Clin. Infect. Dis. 2012, 54, 1785–1792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; Macdougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, N.J.; Grove, M.E.; Kiel, P.J.; O’Donnell, J.N.; Whited, L.K.; Rose, D.T.; Jones, D.R.; Scheetz, M.H. Population pharmacokinetics of cefepime in febrile neutropenia: Implications for dose-dependent susceptibility and contemporary dosing regimens. Int. J. Antimicrob. Agents 2017, 50, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Whited, L.; Grove, M.; Rose, D.; Rhodes, N.J.; Scheetz, M.H.; O’Donnell, J.N.; Neeb, J.; Thoele, K.; Jones, D.R.; Lowe, C.; et al. Pharmacokinetics of Cefepime in Patients with Cancer and Febrile Neutropenia in the Setting of Hematologic Malignancies or Hematopoeitic Cell Transplantation. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2016, 36, 1003–1010. [Google Scholar] [CrossRef]
- Sime, F.B.; Roberts, M.S.; Tiong, I.S.; Gardner, J.H.; Lehman, S.; Peake, S.L.; Hahn, U.; Warner, M.S.; Roberts, J.A. Adequacy of High-Dose Cefepime Regimen in Febrile Neutropenic Patients with Hematological Malignancies. Antimicrob. Agents Chemother. 2015, 59, 5463–5469. [Google Scholar] [CrossRef] [Green Version]
- Patel, H.B.; Lusk, K.A.; Cota, J.M. The Role of Cefepime in the Treatment of Extended-Spectrum Beta-Lactamase Infections. J. Pharm. Pract. 2019, 32, 458–463. [Google Scholar] [CrossRef]
- Sampol, E.; Jacquet, A.; Viggiano, M.; Bernini, V.; Manelli, J.C.; Lacarelle, B.; Durand, A. Plasma, urine and skin pharmacokinetics of cefepime in burns patients. J. Antimicrob. Chemother. 2000, 46, 315–317. [Google Scholar] [CrossRef] [Green Version]
- Drusano, G.L. Antimicrobial pharmacodynamics: Critical interactions of ‘bug and drug’. Nat. Rev. Microbiol. 2004, 2, 289–300. [Google Scholar] [CrossRef]
- Burgess, S.V.; Mabasa, V.H.; Chow, I.; Ensom, M.H. Evaluating Outcomes of Alternative Dosing Strategies for Cefepime: A Qualitative Systematic Review. Ann. Pharmacother. 2015, 49, 311–322. [Google Scholar] [CrossRef]
- McKinnon, P.S.; Paladino, J.A.; Schentag, J.J. Evaluation of area under the inhibitory curve (AUIC) and time above the minimum inhibitory concentration (T>MIC) as predictors of outcome for cefepime and ceftazidime in serious bacterial infections. Int. J. Antimicrob. Agents 2008, 31, 345–351. [Google Scholar] [CrossRef]
- Crandon, J.L.; Bulik, C.C.; Kuti, J.L.; Nicolau, D.P. Clinical pharmacodynamics of cefepime in patients infected with Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2010, 54, 1111–1116. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, N.J.; Kuti, J.L.; Nicolau, D.P.; Van Wart, S.; Nicasio, A.M.; Liu, J.; Lee, B.J.; Neely, M.N.; Scheetz, M.H. Defining Clinical Exposures of Cefepime for Gram-Negative Bloodstream Infections That Are Associated with Improved Survival. Antimicrob. Agents Chemother. 2016, 60, 1401–1410. [Google Scholar] [CrossRef] [Green Version]
- Freifeld, A.G.; Bow, E.J.; Sepkowitz, K.A.; Boeckh, M.J.; Ito, J.I.; Mullen, C.A.; Raad, I.I.; Rolston, K.V.; Young, J.A.H.; Wingard, J.R. Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2011, 52, 427–431. [Google Scholar] [CrossRef] [Green Version]
- Cuervo-Maldonado, S.I.; Bermúdez, C.D.; Enciso, L.; Gómez-Rincón, J.C.; Castillo, J.S.; Sánchez, R.; Ballesteros, M.P.; Buitrago, G.; Gamboa, Ó.A.; Acosta, S.; et al. Guía de práctica clínica para el diagnóstico y el tratamiento de las infecciones bacterianas y micóticas en pacientes oncológicos mayores de 15 años con neutropenia febril posquimioterapia de alto riesgo. Rev. Colomb. Cancerol. 2014, 18, 186–196. [Google Scholar] [CrossRef]
- Paul, M.; Yahav, D.; Fraser, A.; Leibovici, L. Empirical antibiotic monotherapy for febrile neutropenia: Systematic review and meta-analysis of randomized controlled trials. J. Antimicrob. Chemother. 2006, 57, 176–189. [Google Scholar] [CrossRef]
- Tapliz, R.A.; Kennedy, E.B.; Bow, E.J.; Crew, J.; Gleason, C.; Hawley, D.K.; Langston, A.A.; Nastoupil, L.J.; Rajotte, M.; Rolston, K.; et al. Outpatient Management of Fever and Neutropenia in Adults Treated for Malignancy: American Society of Clinical Oncology and Infectious Diseases Society of America Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1443–1453. [Google Scholar] [CrossRef] [Green Version]
- Kidney Disease Improving Global Outcomes (KDIGO). Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar] [CrossRef] [Green Version]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Peng, Y.; Qi, X.; Guo, X. Child-pugh versus MELD score for the assessment of prognosis in liver cirrhosis a systematic review and meta-analysis of observational studies. Medicine 2016, 95, 1–29. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll. Cardiol. 2017, 70, 776–803. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Lente, F.V.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Hagel, R.B.; Waysek, E.H.; Cort, W.M. High-pressure liquid chromatography analysis of antibiotic susceptibility disks. Antimicrob. Agents Chemother. 1979, 16, 372–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bundtzen, R.W.; Toothaker, R.D.; Nielson, O.S.; Madsen, P.O.; Welling, P.G.; Craig, W.A. Pharmacokinetics of cefuroxime in normal and impaired renal function: Comparison of high-pressure liquid chromatography and microbiological assays. Antimicrob. Agents Chemother. 1981, 19, 443–449. [Google Scholar] [CrossRef] [Green Version]
- Silva, E.; Díaz, J.A.; Arias, M.J.; Hernández, A.P.; de la Torre, A. Comparative in vitro study of the antimicrobial activities of different commercial antibiotic products for intravenous administration. BMC Clin. Pharmacol. 2010, 10, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lixoft SAS. Monolix Version 2019R1. 2019. Available online: http://lixoft.com/products/monolix/ (accessed on 22 February 2020).
- Beal, S.L. Ways to fit a PK model with some data below the quantification limit. J. Pharmacokinet. Pharmacodyn. 2001, 28, 481–504. [Google Scholar] [CrossRef] [PubMed]
- Delattre, M.; Lavielle, M.; Poursat, M.A. A note on BIC in mixed-effects models. Electron. J. Stat. 2014, 8, 456–475. [Google Scholar] [CrossRef]
- Lixoft. Monolix 2019 User Guide. 2019. Available online: https://monolix.lixoft.com/single-page/ (accessed on 22 February 2020).
- Nguyen, T.H.; Mouksassi, M.S.; Holford, N.; Al-Huniti, N.; Freedman, I.; Hooker, A.C.; John, J.; Karlsson, M.O.; Mould, D.R.; Perez Ruixo, J.J.; et al. Model evaluation of continuous data pharmacometric models: Metrics and graphics. CPT Pharmacometrics Syst. Pharmacol. 2017, 6, 87–109. [Google Scholar] [CrossRef]
- Barbhaiya, R.H.; Forgue, S.T.; Gleason, C.R.; Knupp, C.A.; Pittman, K.A.; Weidler, D.J.; Movahhed, H.; Tenney, J.; Martin, R.R. Pharmacokinetics of cefepime after single and multiple intravenous administrations in healthy subjects. Antimicrob. Agents Chemother. 1992, 36, 552–557. [Google Scholar] [CrossRef] [Green Version]
- Eddelbuettel, D.; Sanderson, C. RcppArmadillo: Accelerating R with high-performance C++ linear algebra. Comput. Stat. Data Anal. 2014, 71, 1054–1063. [Google Scholar] [CrossRef] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Available online: https://eucast.org/clinical_breakpoints/ (accessed on 30 March 2020).
- Huguet, F.; Leguay, T.; Raffoux, E.; Thomas, X.; Beldjord, K.; Delabesse, E.; Chevallier, P.; Buzyn, A.; Delannoy, A.; Chalandon, Y.; et al. Pediatric-inspired therapy in adults with philadelphia chromosome-negative acute lymphoblastic leukemia: The GRAALL-2003 study. J. Clin. Oncol. 2009, 27, 911–918. [Google Scholar] [CrossRef] [Green Version]
- Kantarjian, H.; Thomas, D.; O’Brien, S.; Cortes, J.; Giles, F.; Jeha, S.; Bueso-Ramos, C.E.; Pierce, S.; Shan, J.; Koller, C.; et al. Long-term follow-up results of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (Hyper-CVAD), a dose-intensive regimen, in adult acute lymphocytic leukemia. Cancer 2004, 101, 2788–2801. [Google Scholar] [CrossRef]
- Tam, V.H.; Mckinnon, P.S.; Akins, R.L.; Drusano, G.L.; Rybak, M.J. Pharmacokinetics and Pharmacodynamics of Cefepime in Patients with Various Degrees of Renal Function. Antimicrob. Agents Chemother. 2003, 47, 1853–1861. [Google Scholar] [CrossRef] [Green Version]
- Roos, J.F.; Bulitta, J.; Lipman, J.; Kirkpatrick, C.M.J. Pharmacokinetic-pharmacodynamic rationale for cefepime dosing regimens in intensive care units. J. Antimicrob. Chemother. 2006, 58, 987–993. [Google Scholar] [CrossRef]
- Horita, N.; Shibata, Y.; Watanabe, H.; Namkoong, H.; Kaneko, T. Comparison of antipseudomonal β-lactams for febrile neutropenia empiric therapy: Systematic review and network meta-analysis. Clin. Microbiol. Infect. 2017, 23, 723–729. [Google Scholar] [CrossRef] [Green Version]
- Kim, P.W.; Wu, Y.T.; Cooper, C.; Rochester, G.; Valappil, T.; Wang, Y.; Kornegay, C.; Nambiar, S. Meta-Analysis of a Possible Signal of Increased Mortality Associated with Cefepime Use. Clin. Infect. Dis. 2010, 51, 381–389. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing, Twenty-Fifth Informational Supplement; Number January; CLSI: Wayne, PA, USA, 2015; pp. 1–236. [Google Scholar]
- Barbhaiya, R.H.; Knupp, C.A.; Thomas Forgue, S.; Matzke, G.R.; Guay, D.R.; Pittman, K.A. Pharmacokinetics of cefepime in subjects with renal insufficiency. Clin. Pharmacol. Ther. 1990, 48, 268–276. [Google Scholar] [CrossRef]
- Cronqvist, J.; Nilsson-Ehle, I.; Oqvist, B.; Norrby, S.R. Pharmacokinetics of cefepime dihydrochloride arginine in subjects with renal impairment. Antimicrob. Agents Chemother. 1992, 36, 2676–2680. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age (years) [median (IQR)] | 39.0 (30.0, 49.5) |
| Sex [n (%)] | |
| Female | 5 (33.3) |
| Male | 10 (66.7) |
| Body weight (kg) [median (IQR)] | 65 (60.5, 72.0) |
| Height (cm) [median (IQR)] | 170 (160, 175) |
| BMI (kg/m) [median (IQR)] | 23.9 (23.1, 25.8) |
| Serum creatinine (mg/dL) [median (IQR)] | 0.54 (0.48, 0.57) |
| eGFR () [median (IQR)] | 129 (118.9, 138.8) |
| Albumin (g/dL) [median (IQR)] | 3.4 (3.21, 3.66) |
| Total protein (g/dL) [median (IQR)] | 5.9 (5.46, 6.1) |
| Antibiotic given in the previous month [n (%)] | |
| Yes | 4 (28.6) |
| No | 11 (71.4) |
| Concomitant antimicrobial prophylaxis [n (%)] | |
| Trimethoprim-Sulfametoxazole | 3 (20.0) |
| Acyclovir | 6 (40.0) |
| Fluconazole | 2 (13.3) |
| Nystatin | 2 (13.3) |
| Ivermectin | 1 (6.7) |
| Metronidazole | 1 (6.7) |
| Voriconazole | 1 (6.7) |
| None | 4 (26.7) |
| Malignancy [n (%)] | |
| Lymphoma | 3 (20.0) |
| Lymphoid leukemia | 7 (46.7) |
| Myeloid leukemia | 4 (26.7) |
| Multiple myeloma | 1 (6.7) |
| ANC (/) [median (IQR)] | 30 (20, 95) |
| Therapy cycle [n (%)] | |
| 1 | 11 (73.3) |
| 2 | 3 (20.0) |
| >3 | 1 (6.7) |
| FN associated chemotherapy [n (%)] | |
| GRAALL | 4 (26.7) |
| HyperCVAD | 2 (13.3) |
| Another chemotherapy | 9 (60.0) |
| Parameter | Estimated Value | RSE (%) | Bootstrap Median (95% CI) |
|---|---|---|---|
| Structural Model | |||
| 20.6 | 19.67 | 20.72 (11.96, 33.54) | |
| −0.415 | 44.08 | −0.42 (−0.80, 0.17) | |
| 23.8 | 9.47 | 24.04 (19.74, 28.99) | |
| 23.4 | - | - | |
| 13.3 | 28.38 | 12.79 (7.13, 22.59) | |
| Interindividual variability | |||
| 22.70 | 19.15 | 21.2 (14.07, 26.5) | |
| 30.60 | 25.66 | 28.6 (0.000, 46.2) | |
| 120.30 | 39.14 | 97.9 (0.008, 291.3) | |
| 93.90 | 30.44 | 86.9 (0.000, 160.8) | |
| Residual Error | |||
| Additive | 1.86 | 11.11 | 1.89 (1.40, 2.40) |
| Dose | Therapy | Microorganism | ||
|---|---|---|---|---|
| ECO | KPN | PSA | ||
| Target: | ||||
| 2 g q8h tinf 30 min | Empirical | 0.899 | 0.610 | 0.396 |
| Directed | 0.984 | 0.957 | 0.626 | |
| 2 g q8h tinf 2 h | Empirical | 0.910 | 0.631 | 0.463 |
| Directed | 0.993 | 0.974 | 0.719 | |
| 2 g q8h tinf 4 h | Empirical | 0.920 | 0.657 | 0.565 |
| Directed | 0.998 | 0.991 | 0.849 | |
| 6 g q24h tinf 24 h | Empirical | 0.942 | 0.749 | 0.820 |
| Directed | 1.000 | 1.000 | 1.000 | |
| Target: | ||||
| 2 g q8h tinf 30 min | Empirical | 0.928 | 0.686 | 0.663 |
| Directed | 0.999 | 0.997 | 0.939 | |
| 2 g q8h tinf 2 h | Empirical | 0.933 | 0.706 | 0.724 |
| Directed | 1.000 | 1.000 | 0.981 | |
| 2 g q8h tinf 4 h | Empirical | 0.939 | 0.730 | 0.785 |
| Directed | 1.000 | 1.000 | 1.000 | |
| 6 g q24h tinf 24 h | Empirical | 0.942 | 0.749 | 0.820 |
| Directed | 1.000 | 1.000 | 1.000 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Álvarez, J.C.; Cuervo, S.I.; Silva, E.; Díaz, J.A.; Jiménez, L.L.; Parra, D.S.; Gómez, J.C.; Sánchez, R.; Cortés, J.A. Pharmacokinetics and Pharmacodynamics of Cefepime in Adults with Hematological Malignancies and Febrile Neutropenia after Chemotherapy. Antibiotics 2021, 10, 504. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050504
Álvarez JC, Cuervo SI, Silva E, Díaz JA, Jiménez LL, Parra DS, Gómez JC, Sánchez R, Cortés JA. Pharmacokinetics and Pharmacodynamics of Cefepime in Adults with Hematological Malignancies and Febrile Neutropenia after Chemotherapy. Antibiotics. 2021; 10(5):504. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050504
Chicago/Turabian StyleÁlvarez, José C., Sonia I. Cuervo, Edelberto Silva, Jorge A. Díaz, Lorena L. Jiménez, Daniel S. Parra, Julio C. Gómez, Ricardo Sánchez, and Jorge A. Cortés. 2021. "Pharmacokinetics and Pharmacodynamics of Cefepime in Adults with Hematological Malignancies and Febrile Neutropenia after Chemotherapy" Antibiotics 10, no. 5: 504. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050504