
Impact of an Antimicrobial Stewardship Program on the Incidence of Carbapenem Resistant Gram-Negative Bacilli: An Interrupted Time-Series Analysis

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
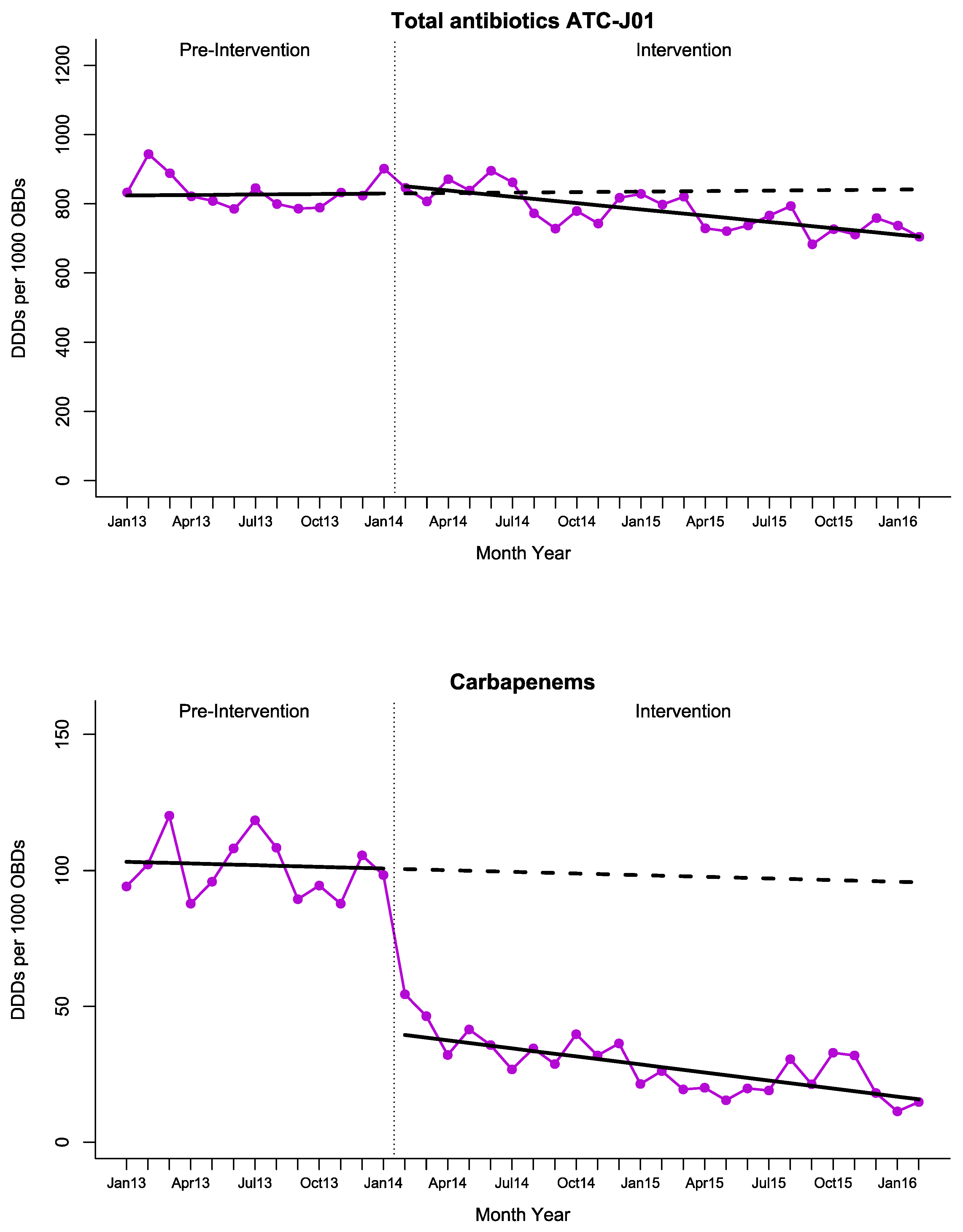
2.1. Antimicrobial Consumption
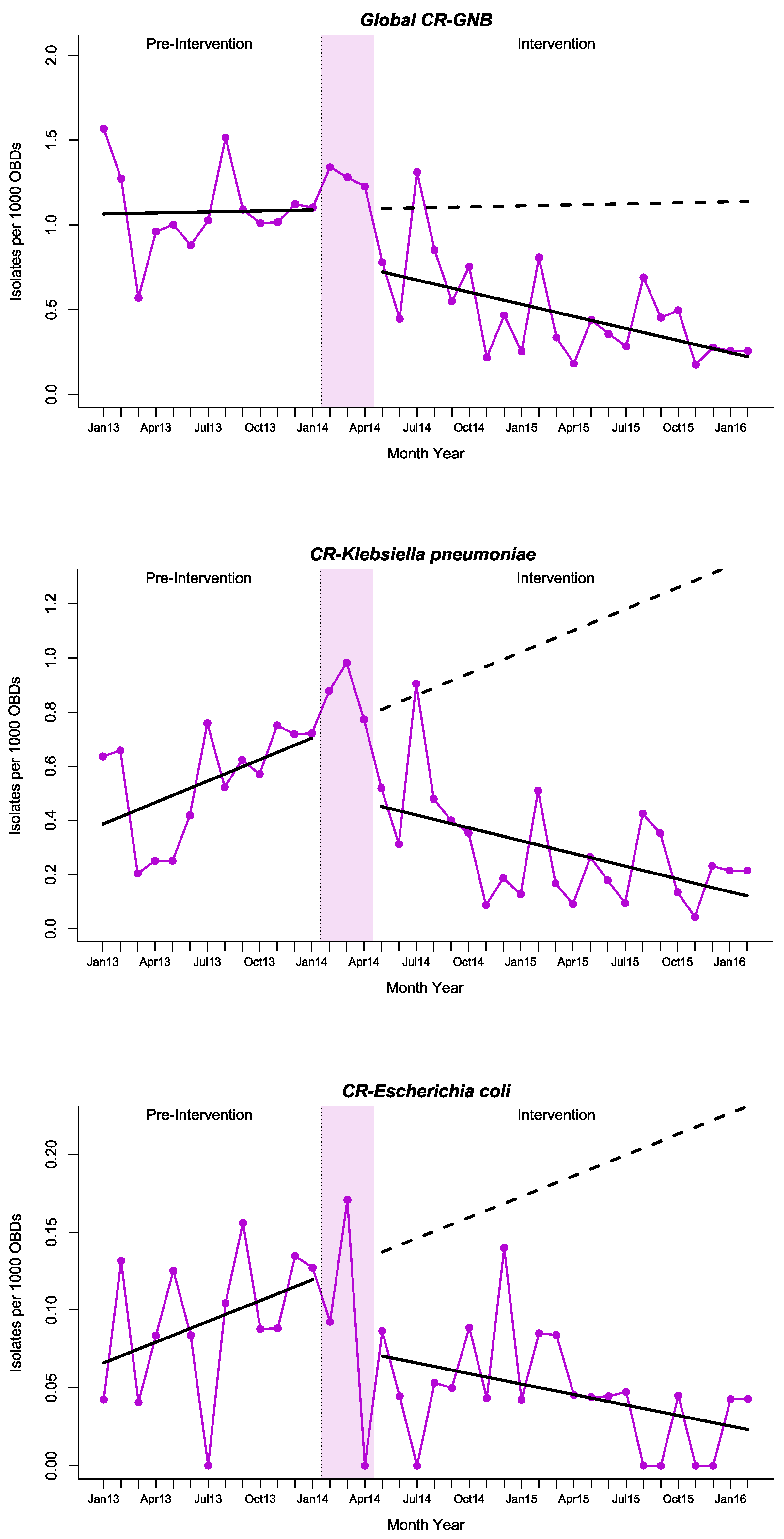
2.2. Carbapenem Resistant
2.3. Impact on Mortality Rates for Sentinel Events
2.4. Changes in Healthcare during the Study Period
2.5. Acceptance of the PROVAUR Program
3. Discussion
4. Materials and Methods
4.1. Study Design and Period
4.2. Study Setting and Population
4.3. Intervention
4.4. Variables and Definitions
4.5. Microbiological Definitions
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef] [PubMed]
- Stewardson, A.J.; Marimuthu, K.; Sengupta, S.; Allignol, A.; El-Bouseary, M.; Carvalho, M.J.; Hassan, B.; Delgado-Ramirez, M.A.; Arora, A.; Bagga, R.; et al. Effect of carbapenem resistance on outcomes of bloodstream infection caused by Enterobacteriaceae in low-income and middle-income countries (PANORAMA): A multinational prospective cohort study. Lancet Infect. Dis. 2019, 19, 601–610. [Google Scholar] [CrossRef]
- Tumbarello, M.; Trecarichi, E.M.; de Rosa, F.G.; Giannella, M.; Giacobbe, D.R.; Bassetti, M.; Losito, A.R.; Bartoletti, M.; del Bono, V.; Corcione, S.; et al. Infections caused by KPC-producing Klebsiella pneumoniae: Differences in therapy and mortality in a multicentre study. J. Antimicrob. Chemother. 2015, 70, 2133–2143. [Google Scholar] [CrossRef]
- Ecdc. Antimicrobial Resistance in the EU/EEA (EARS-Net)—AER for 2019. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe (accessed on 15 January 2021).
- Wong, D.; Spellberg, B. Leveraging antimicrobial stewardship into improving rates of carbapenem-resistant Enterobacteriaceae. Virulence 2016, 8, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Faraone, A.; Poggi, A.; Cappugi, C.; Tofani, L.; Riccobono, E.; Giani, T.; Fortini, A. Inappropriate use of carbapenems in an internal medicine ward: Impact of a carbapenem-focused antimicrobial stewardship program. Eur. J. Intern. Med. 2020, 78, 50–57. [Google Scholar] [CrossRef]
- Giacobbe, D.R.; On behalf of the San Martino Antimicrobial Stewardship Group; Del Bono, V.; Mikulska, M.; Gustinetti, G.; Marchese, A.; Mina, F.; Signori, A.; Orsi, A.; Rudello, F.; et al. Impact of a mixed educational and semi-restrictive antimicrobial stewardship project in a large teaching hospital in Northern Italy. Infection 2017, 45, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Salsano, A.; del Puente, F.; Campanini, F.; Mariscalco, G.; Marchese, A.; Viscoli, C.; Santini, F. Puente Reduced Incidence of Carbapenem-Resistant Klebsiella pneumoniae Infections in Cardiac Surgery Patients after Implementation of an Antimicrobial Stewardship Project. Antibiotics 2019, 8, 132. [Google Scholar] [CrossRef] [PubMed]
- García-Martínez, L.; Gracia-Ahulfinger, I.; Machuca, I.; Cantisán, S.; de la Fuente, S.; Natera, C.; Pérez-Nadales, E.; Vidal, E.; Rivero, A.; Rodríguez-Lopez, F.; et al. Impact of the PROVAUR stewardship programme on linezolid resistance in a tertiary university hospital: A before-and-after interventional study. J. Antimicrob. Chemother. 2016, 71, 2606–2611. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.; Peñalva, G.; Gil-Navarro, M.V.; Praena, J.; Lepe, J.A.; Pérez-Moreno, M.A.; Ferrándiz, C.; Aldabó, T.; Aguilar, M.; Olbrich, P.; et al. Long-Term Impact of an Educational Antimicrobial Stewardship Program on Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections: A Quasi-Experimental Study of Interrupted Time-Series Analysis. Clin. Infect. Dis. 2017, 65, 1992–1999. [Google Scholar] [CrossRef] [PubMed]
- Peñalva, G.; Fernández-Urrusuno, R.; Turmo, J.M.; Hernández-Soto, R.; Pajares, I.; Carrión, L.; Vázquez-Cruz, I.; Botello, B.; García-Robredo, B.; Cámara-Mestres, M.; et al. Long-term impact of an educational antimicrobial stewardship programme in primary care on infections caused by extended-spectrum β-lactamase-producing Escherichia coli in the community: An interrupted time-series analysis. Lancet Infect. Dis. 2020, 20, 199–207. [Google Scholar] [CrossRef]
- García-Rodríguez, J.F.; Bardán-García, B.; Peña-Rodríguez, M.F.; Álvarez-Díaz, H.; Mariño-Callejo, A. Meropenem antimicrobial stewardship program: Clinical, economic, and antibiotic resistance impact. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; Marwick, C.; Scott, C.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Cochrane Database of Systematic Reviews Interventions to Improve Antibiotic Prescribing Practices for Hospital Inpatients (Review). Cochrane Database Syst. Rev. 2017. [Google Scholar]
- Bertollo, L.G.; Lutkemeyer, D.S.; Levin, A.S. Are antimicrobial stewardship programs effective strategies for preventing antibiotic resistance? A systematic review. Am. J. Infect. Control. 2018, 46, 824–836. [Google Scholar] [CrossRef]
- Schweitzer, V.A.; van Heijl, I.; van Werkhoven, C.H.; Islam, J.; Hendriks-Spoor, K.D.; Bielicki, J.; Bonten, M.J.M.; Walker, A.S.; Llewelyn, M.J. The quality of studies evaluating antimicrobial stewardship interventions: A systematic review. Clin. Microbiol. Infect. 2019, 25, 555–561. [Google Scholar] [CrossRef]
- Cano, A.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Gracia-Ahufinger, I.; Pérez-Nadales, E.; Causse, M.; Castón, J.J.; Guzman-Puche, J.; Torre-Giménez, J.; Kindelán, L.; et al. Risks of Infection and Mortality Among Patients Colonized with Klebsiella pneumoniae Carbapenemase–Producing, K. pneumoniae: Validation of Scores and Proposal for Management. Clin. Infect. Dis. 2018, 66, 1204–1210. Available online: https://pubmed.ncbi.nlm.nih.gov/29126110/ (accessed on 13 September 2020). [CrossRef] [PubMed]
- Machuca, I.; Gutiérrez-Gutiérrez, B.; Gracia-Ahufinger, I.; Espinar, F.R.; Cano, Á.; Guzmán-Puche, J.; Pérez-Nadales, E.; Natera, C.; Rodríguez, M.; León, R.; et al. Mortality Associated with Bacteremia Due to Colistin-Resistant Klebsiella pneumoniae with High-Level Meropenem Resistance: Importance of Combination Therapy without Colistin and Carbapenems. Antimicrob. Agents Chemother. 2017, 61, 61. [Google Scholar] [CrossRef] [PubMed]
- Mathers, A.J.; Peirano, G.; Pitout, J.D.D. The Role of Epidemic Resistance Plasmids and International High-Risk Clones in the Spread of Multidrug-Resistant Enterobacteriaceae. Clin. Microbiol. Rev. 2015, 28, 565–591. [Google Scholar] [CrossRef]
- López-Cerero, L.; Egea, P.; Gracia-Ahufinger, I.; González-Padilla, M.; Rodríguez-López, F.; Rodríguez-Baño, J.; Pascual, A. Characterisation of the first ongoing outbreak due to KPC-3-producing Klebsiella pneumoniae (ST512) in Spain. Int. J. Antimicrob. Agents 2014, 44, 538–540. [Google Scholar] [CrossRef]
- Schuts, E.C.; Hulscher, M.E.J.E.; Mouton, J.W.; Verduin, C.M.; Cohen Stuart, J.W.T.; Overdiek, H.W.P.M.; van der Linden, P.D.; Natsch, S.; Hertogh, C.M.P.M.; Wolfs, T.F.W.; et al. Current Evidence on Hospital Antimicrobial Stewardship Objectives: A Systematic Review and Meta-Analysis. Artic Lancet Infect. Dis. 2016, 16, 847. Available online: https://pubmed.ncbi.nlm.nih.gov/26947617/ (accessed on 25 September 2020). [CrossRef]
- Peterson, L. Squeezing the antibiotic balloon: The impact of antimicrobial classes on emerging resistance. Clin. Microbiol. Infect. 2005, 11, 4–16. Available online: pmc/articles/PMC7128169/?report=abstract (accessed on 9 November 2020). [CrossRef] [PubMed]
- Rojo-Martín, M.D.; Peñalva, G.; Pinto, C.; Salcedo, I.; Fernández-Urrusuno, R.; Cabeza, J.; Alcántara, J.; Neth, O.; Porras, P.; Bautista, J.; et al. The PIRASOA programme: Design, structure, organisation and indicators of a comprehensive regional Institutional Programme for the Prevention and Control of Healthcare-Associated Infections and Antimicrobial Stewardship for Hospitals and Primary Care Setti. WwwProtocolsIo. 2018. Available online: https://www.protocols.io/view/the-pirasoa-programme-design-structure-organisatio-r3bd8in/abstract. (accessed on 15 May 2021).
- Penfold, R.B.; Zhang, F. Use of Interrupted Time Series Analysis in Evaluating Health Care Quality Improvements. Acad. Pediatr. 2013, 13, S38–S44. [Google Scholar] [CrossRef] [PubMed]
- De Kraker, M.E.; Abbas, M.; Huttner, B.; Harbarth, S. Good epidemiological practice: A narrative review of appropriate scientific methods to evaluate the impact of antimicrobial stewardship interventions. Clin. Microbiol. Infect. 2017, 23, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. Available online: https://pubmed.ncbi.nlm.nih.gov/10649300/ (accessed on 4 October 2020). [CrossRef]
- Seah, V.X.F.; Ong, R.Y.L.; Lim, A.S.Y.; Chong, C.Y.; Tan, N.W.H.; Thoon, K.C. Impact of a Carbapenem Antimicrobial Stewardship Program on Patient Outcomes. Antimicrob. Agents Chemother. 2017, 61, e00736-17. [Google Scholar] [CrossRef] [PubMed]
- Cano, Á.; Guzmán-Puche, J.; García-Gutiérrez, M.; Castón, J.J.; Gracia-Ahufinger, I.; Pérez-Nadales, E.; Recio, M.; Natera, A.M.; Marfil-Pérez, E.; Martínez-Martínez, L.; et al. Use of carbapenems in the combined treatment of emerging ceftazidime/avibactam-resistant and carbapenem-susceptible KPC-producing Klebsiella pneumoniae infections: Report of a case and review of the literature. J. Glob. Antimicrob. Resist. 2020, 22, 9–12. [Google Scholar] [CrossRef] [PubMed]
- An, E.F.; Cedu, L.E.; Patient, A.; Patient, A.; Patient, T. Hand Hygiene Technical Reference Manual. Available online: https://apps.who.int/iris/bitstream/handle/10665/44196/9789241598606_eng.pdf?sequence=1&isAllowed=y (accessed on 15 May 2021).
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L. 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings. Am. J. Infect. Control. 2007, 35, S65–S164. [Google Scholar] [CrossRef]
- Servicio Andaluz de Salud. Conjunto mínimo básico de datos al alta hospitalaria: Grupos relacionados por el diagnóstico. Andalucía 2019. Available online: https://ws027.sspa.juntadeandalucia.es/contenidos/publicaciones/Datos/734/pdf/conj_mini_datos_2019.pdf (accessed on 4 October 2020). (In Spanish).
- Testing EC on AS. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 3.1, 2013. Available online: http://www.eucast.org/clinical_breakpoints/%5Cnhttp://www.eucast.org/eucast_disk_diffusion_test/ (accessed on 15 May 2021).
- López-Lozano, J.-M.; Monnet, D.L.; Yagüe, A.; Burgos, A.; Gonzalo, N.; Campillos, P.; Saez, M. Modelling and forecasting antimicrobial resistance and its dynamic relationship to antimicrobial use: A time series analysis. Int. J. Antimicrob. Agents 2000, 14, 21–31. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Outcomes | Regression Intercept | Pre-Intervention Trend | Change in Level a | Change in Trend b | Absolute Effect c | Relative Effect (%) c |
|---|---|---|---|---|---|---|
| Total antibiotics (ATC-J01) | 823.7 | 0.472 (−2.999, 3.943) | 26.72 (3.210, 50.22) | −6.531 (−9.696, −3.365) | −136.5 (−237.2, −35.94) | −16.22 (−25.64, −6.809) |
| Carbapenems | 103.4 | −0.203 (−1.221, 0.815) | −60.32 (−68.83,−51.80) | −0.783 (−1.749, 0.182) | −79.90 (−110.6, −49.13) | −83.51 (−87.23, −79.79) |
| Third- and fourth-generation cephalosporins | 67.94 | 2.168 (0.690, 3.645) | 5.205 (−8.088, 18.50) | −1.896 (−3.473, −0.318) | −42.19 (−88.98, 4.585) | −28.07 (−49.03, −7.106) |
| β-lactams and β-lactamase inhibitors | 237.2 | −4.049 (−4.981, −3.118) | 49.06 (42.46, 55.65) | 3.623 (2.777, 4.469) | 139.6 (112.5, 166.8) | 167.6 (63.81, 271.4) |
| Quinolones | 162.1 | −0.391 (−1.233, 0.451) | 7.290 (−4.924, 19.50) | −1.217 (−2.134, −0.299) | −23.13 (−53.21, 6.953) | −15.71 (−32.83, 1.411) |
| Aminoglycosides | 20.336 | −0.304 (−0.862, 0.255) | 4.617 (−0.302, 9.536) | 0.044 (−0.567, 0.654) | 5.711 (−12.08, 23.50) | 64.94 (−292.1, 422.0) |
| Outcomes | Regression Intercept | Pre-Intervention Trend | Change in Level a | Change in Trend b | Absolute Effect c | Relative Effect (%) c |
|---|---|---|---|---|---|---|
| Global CR-GNB | 1.063 | 0.002 (−0.025, 0.028) | −0.349 (−0.629, −0.068) | −0.026 (−0.053, 0.002) | −0.915 (−1.743, −0.087) | −80.46 (−90.49, −70.43) |
| Klebsiella pneumoniae | 0.359 | 0.026 (0.0007, 0.052) | −0.316 (−0.609, −0.022) | −0.042 (−0.070, −0.014) | −1.244 (−2.060, −0.427) | −91.15 (−105.5, −76.76) |
| Other Enterobacteriaceae | 0.137 | 0.001 (−0.003, 0.005) | −0.053 (−0.094, −0.013) | −0.004 (−0.008, 0.0005) | −0.133 (−0.257, −0.008) | −75.11 (−85.64, −64.58) |
| Escherichia coli | 0.061 | 0.004 (−0.0009, 0.009) | −0.060 (−0.121, 0.0006) | −0.007 (−0.012, −0.0008) | −0.207 (−0.376, −0.039) | −89.93 (−107.0, −72.83) |
| Proteus mirabilis | 0.023 | −0.0001 (−0.003, 0.003) | −0.006 (−0.044, 0.031) | −0.0002 (−0.003, 0.003) | −0.011 (−0.109, 0.088) | −60.07 (−279.2, 159.1) |
| Klebsiella aerogenes/ Enterobacter cloacae | 0.015 | 0.0004 (−0.002, 0.003) | −0.006 (−0.029, 0.017) | −0.0007 (−0.003, 0.002) | −0.022 (−0.096, 0.051) | −68.72 (−113.52, −23.92) |
| Pseudomonas aeruginosa | 0.258 | −0.011 (−0.019, −0.003) | 0.079 (−0.002, 0.161) | 0.008 (−0.0004, 0.017) | 0.260 (0.0009, 0.520) | −146.5 (−263.2, −29.84) |
| Acinetobacter baumannii | 0.333 | −0.016 (−0.023, −0.010) | −0.025 (−0.088, 0.037) | 0.014 (0.007, 0.020) | 0.283 (0.089, 0.477) | −96.25 (−110.9, −81.64) |
| Year | Number of K. pneumoniae Isolates | Number of CR-Producing K. pneumoniae | Resistance Proportion (%) |
|---|---|---|---|
| 2013 | 222 | 142 | 64% |
| 2014 | 249 | 146 | 58.6% |
| 2015 | 160 | 57 | 35.6% |
| 2016 * | 27 | 10 | 37% |
| Regression Intercept | Pre-Intervention Trend | Change in Level a | Change in Trend b | Absolute Effect c | Relative Effect (%) c |
|---|---|---|---|---|---|
| 0.103 | −0.004 (−0.009, 0.001) | −0.010 (−0.057, 0.036) | 0.004 (−0.0006, 0.009) | 0.105 (−0.061, 0.272) | −190.9 (−612.4, 230.6) |
|
| Periods | Activity |
|---|---|
| Pre-intervention |
|
| Intervention |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Viñau, T.; Peñalva, G.; García-Martínez, L.; Castón, J.J.; Muñoz-Rosa, M.; Cano, Á.; Recio, M.; Cisneros, J.M.; Pérez-Nadales, E.; Rumbao Aguirre, J.; et al. Impact of an Antimicrobial Stewardship Program on the Incidence of Carbapenem Resistant Gram-Negative Bacilli: An Interrupted Time-Series Analysis. Antibiotics 2021, 10, 586. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050586
López-Viñau T, Peñalva G, García-Martínez L, Castón JJ, Muñoz-Rosa M, Cano Á, Recio M, Cisneros JM, Pérez-Nadales E, Rumbao Aguirre J, et al. Impact of an Antimicrobial Stewardship Program on the Incidence of Carbapenem Resistant Gram-Negative Bacilli: An Interrupted Time-Series Analysis. Antibiotics. 2021; 10(5):586. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050586
Chicago/Turabian StyleLópez-Viñau, Teresa, Germán Peñalva, Lucrecia García-Martínez, Juan José Castón, Montserrat Muñoz-Rosa, Ángela Cano, Manuel Recio, José Miguel Cisneros, Elena Pérez-Nadales, José Rumbao Aguirre, and et al. 2021. "Impact of an Antimicrobial Stewardship Program on the Incidence of Carbapenem Resistant Gram-Negative Bacilli: An Interrupted Time-Series Analysis" Antibiotics 10, no. 5: 586. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050586