
Multi-Drug Resistant Organisms Infection Impact on Patients Length of Stay in Respiratory Care Ward


Abstract
:1. Introduction
2. Materials and Methods
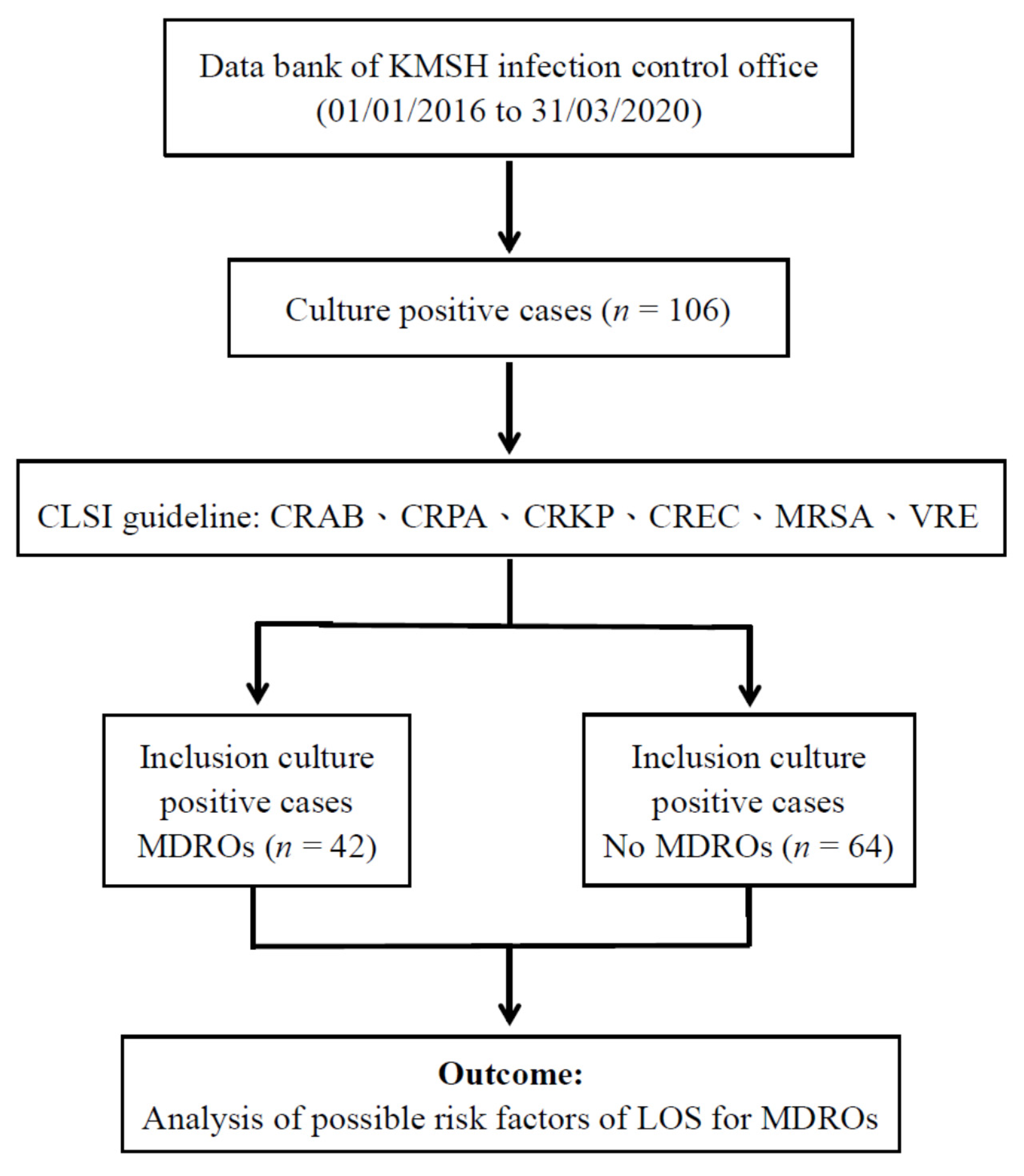
2.1. Research Design and Data Collection
2.2. Antibiotic Susceptibility and Species Identification of Bacterial Isolates
2.3. Definition and Data Collection of Risk Factors
2.4. Statistical Analysis
3. Results
3.1. Research Design and Data Collection
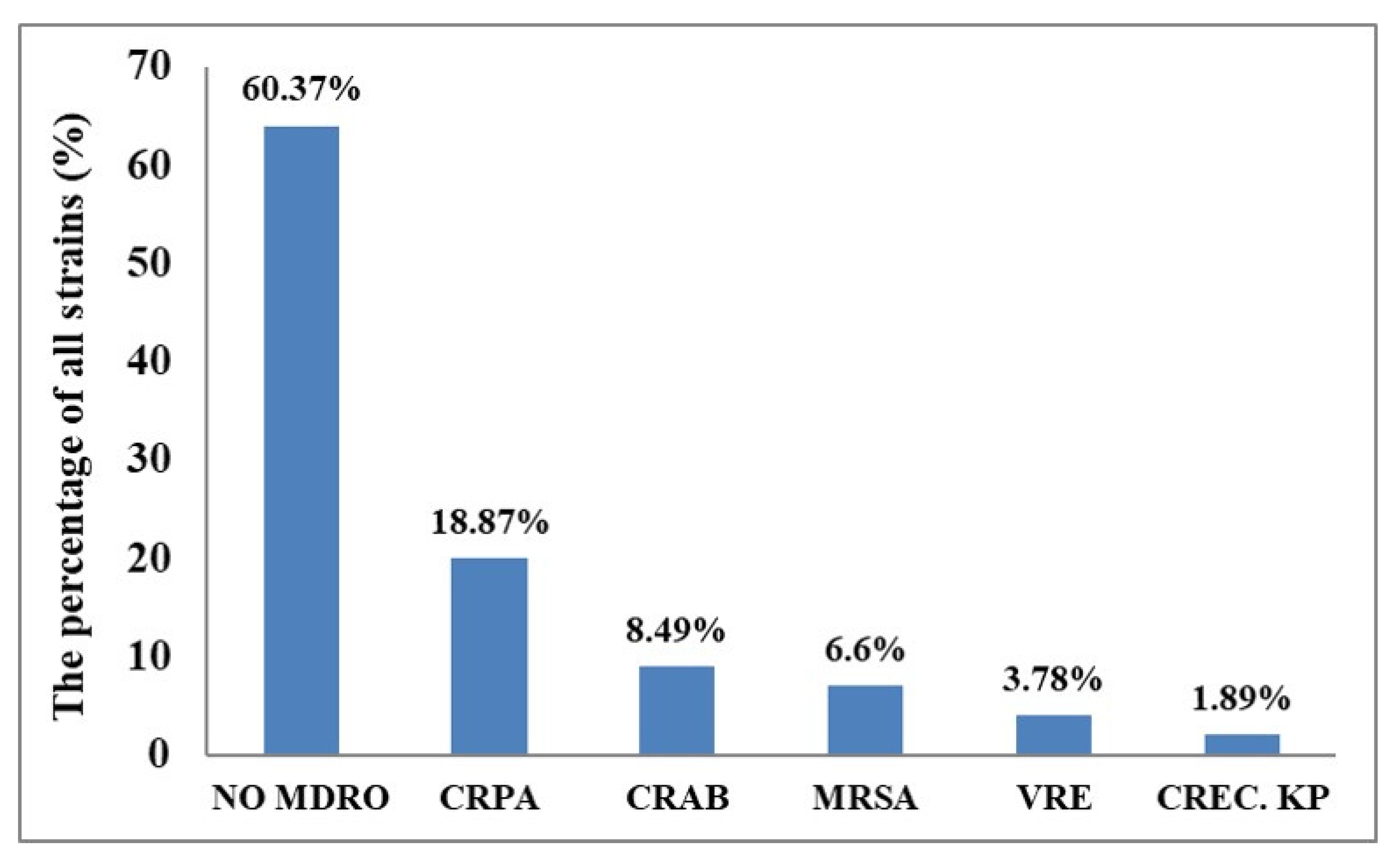
3.2. Case Analysis of MDRO-Infected Patients
3.3. Risk Factor Data Collection
3.4. Factors Affecting the Length of Hospital Stay
3.4.1. Analysis of Variance (One-Way ANOVA)
3.4.2. Multivariate Regression Analysis (Two-Way ANOVA)
3.5. Analysis of Variance (ANOVA) of log LOS of Different Drug-Resistant MDROs
4. Discussion
4.1. MDRO Infection Is a Risk Factor for Prolonged LOS
4.2. Risk Factors Affecting LOS
4.3. Advantages
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chacko, R.; Rajan, A.; Lionel, P.; Thilagavathi, M.; Yadav, B.; Premkumar, J. Oral decontamination techniques and ventilator-associated pneumonia. Br. J. Nurs. 2017, 26, 594–599. [Google Scholar] [CrossRef]
- Ferrer, M.; Torres, A. Epidemiology of ICU-acquired pneumonia. Curr. Opin. Crit. Care 2018, 24, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Brown, W.J. A comparison of bronchoscopic vs blind protected specimen brush sampling in patients with suspected ventilator-associated pneumonia. Chest 1995, 108, 203–207. [Google Scholar] [CrossRef]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Li Bassi, G.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [PubMed]
- Metersky, M.L.; Kalil, A.C. Management of ventilator-associated pneumonia: Guidelines. Clin. Chest Med. 2018, 39, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Arthur, L.E.; Kizor, R.S.; Selim, A.G.; van Driel, M.L.; Seoane, L. Antibiotics for ventilator-associated pneumonia. Cochrane Database Syst. Rev. 2016, 10, CD004267. [Google Scholar] [CrossRef] [PubMed]
- Jia, H.; Li, L.; Li, W.; Hou, T.; Ma, H.; Yang, Y.; Wu, A.; Liu, Y.; Wen, J.; Yang, H.; et al. Impact of healthcare-associated infections on length of stay: A study in 68 hospitals in China. Biomed. Res. Int. 2019, 2019, 2590563. [Google Scholar] [CrossRef] [Green Version]
- Zilahi, G.; Artigas, A.; Martin-Loeches, I. What’s new in multidrug-resistant pathogens in the ICU? Ann. Intensive Care 2016, 6, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Al-Mousa, H.H.; Omar, A.A.; Rosenthal, V.D.; Salama, M.F.; Aly, N.Y.; Noweir, M.E.D.; Rebello, F.M.; Narciso, D.M.; Sayed, A.F.; Kurian, A.; et al. Device-associated infection rates, bacterial resistance, length of stay, and mortality in Kuwait: International Nosocomial Infection Consortium findings. Am. J. Infect. Control. 2016, 44, 444–449. [Google Scholar] [CrossRef]
- Anesi, J.A.; Blumberg, E.A.; Han, J.H.; Lee, D.H.; Clauss, H.; Climaco, A.; Hasz, R.; Molnar, E.; Alimenti, D.; West, S.; et al. Risk factors for multidrug-resistant organisms among deceased organ donors. Am. J. Transplant. 2019, 19, 2468–2478. [Google Scholar] [CrossRef]
- Karandikar, M.V.; Milliren, C.E.; Zaboulian, R.; Peiris, P.; Sharma, T.; Place, A.E.; Sandora, T.J. Limiting vancomycin exposure in pediatric oncology patients with febrile neutropenia may be associated with decreased vancomycin-resistant enterococcus incidence. J. Pediatric. Infect. Dis. Soc. 2020, 9, 428–436. [Google Scholar] [CrossRef]
- Ruparelia, N.; Atkins, B.L.; Hemingway, J.; Berendt, A.R.; Byren, I. Pristinamycin as adjunctive therapy in the management of Gram-positive multi-drug resistant organism (MDRO) osteoarticular infection. J. Infect. 2008, 57, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Suarez, J.I.; Zaidat, O.O.; Suri, M.F.; Feen, E.S.; Lynch, G.; Hickman, J.; Georgiadis, A.; Selman, W.R. Length of stay and mortality in neurocritically ill patients: Impact of a specialized neurocritical care team. Crit. Care Med. 2004, 32, 2311–2317. [Google Scholar] [CrossRef]
- Moran, J.L.; Solomon, P.J. A review of statistical estimators for risk-adjusted length of stay: Analysis of the Australian and New Zealand intensive care adult patient data-base, 2008–2009. BMC Med. Res. Methodol. 2012, 12, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manoukian, S.; Stewart, S.; Dancer, S.; Graves, N.; Mason, H.; McFarland, A.; Robertson, C.; Reilly, J. Estimating excess length of stay due to healthcare-associated infections: A systematic review and meta-analysis of statistical methodology. J. Hosp. Infect. 2018, 100, 222–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, R.E.; Nelson, S.D.; Khader, K.; Perencevich, E.L.; Schweizer, M.L.; Rubin, M.A.; Graves, N.; Harbarth, S.; Stevens, V.W.; Samore, M.H. The magnitude of time-dependent bias in the estimation of excess length of stay attributable to healthcare-associated infections. Infect. Cont. Hosp. Epidemiol. 2015, 36, 1089–1094. [Google Scholar] [CrossRef]
- De Angelis, G.; Murthy, A.; Beyersmann, J.; Harbarth, S. Estimating the impact of healthcare-associated infections on length of stay and costs. Clin. Microbiol. Infect. 2010, 16, 1729–1735. [Google Scholar] [CrossRef] [PubMed]
- Gidal, A.; Barnett, S. Risk Factors Associated With Multidrug-Resistant Pneumonia in Nonhospitalized Patients. Fed. Pract. 2018, 35, 16. [Google Scholar]
- Vasilakopoulou, A.; Karakosta, P.; Vourli, S.; Tarpatzi, A.; Varda, P.; Kostoula, M.; Antoniadou, A.; Pournaras, S. Gastrointestinal Carriage of Vancomycin-Resistant Enterococci and Carbapenem-Resistant Gram-Negative Bacteria in an Endemic Setting: Prevalence, Risk Factors, and Outcomes. Front. Public Health 2020, 8, 55. [Google Scholar] [CrossRef] [Green Version]
- Martin-Loeches, I.; Torres, A.; Rinaudo, M.; Terraneo, S.; de Rosa, F.; Ramirez, P.; Diaz, E.; Fernández-Barat, L.; Libassi, G.; Ferrer, M. Resistance patterns and outcomes in intensive care unit (ICU)-acquired pneumonia. Validation of European Centre for Disease Prevention and Control (ECDC) and the Centers for Disease Control and Prevention (CDC) classification of multidrug resistant organisms. J. Infect. 2015, 70, 213–222. [Google Scholar] [PubMed]
- Kalluru, S.; Eggers, S.; Barker, A.; Shirley, D.; Sethi, A.K.; Sengupta, S.; Yeptho, K.; Safdar, N. Risk factors for infection with multidrug-resistant organisms in Haryana, India. Am. J. Infect. Control. 2018, 46, 341–345. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Overall (n = 106) | Non-MDROs (n = 64) | MDROs (n = 42) | p-Value |
|---|---|---|---|---|
| n (%)/Mean ± SD | n (%)/Mean ± SD | n (%)/Mean ± SD | ||
| Age (years) | ||||
| >65 | 71 (67.0) | 40 (62.5) | 31 (73.8) | 0.226 |
| other | 35 (33.0) | 24 (37.5) | 11 (26.2) | |
| Sex | ||||
| Male | 55 (51.9) | 32 (50.0) | 23 (54.8) | 0.631 |
| Female | 51 (48.1) | 32 (50.0) | 19 (45.2) | |
| Sample | ||||
| Sputum | 47 (44.3) | 24 (37.5) | 23 (54.8) | 0.110 |
| Urine | 31 (29.2) | 24 (37.5) | 7 (16.7) | |
| Blood | 16 (15.1) | 10 (15.6) | 6 (14.3) | |
| Other | 12 (11.3) | 6 (9.4) | 6 (14.3) | |
| Previous ward | ||||
| None | 65 (61.3) | 39 (60.9) | 26 (61.9) | 0.920 |
| Yes | 41 (38.7) | 25 (39.1) | 16 (38.1) | |
| Type of ward discharged | ||||
| General ward | 26 (24.5) | 17 (26.6) | 9 (21.4) | 0.548 |
| RCW | 80 (75.5) | 47 (73.4) | 33 (78.6) | |
| Nutritional score | 2.2 ± 1.2 | 2.1 ± 1.2 | 2.1 ± 1.2 | 0.407 |
| Antibiotics | ||||
| None | 20 (18.9) | 15 (23.4) | 5 (11.9) | 0.138 |
| Yes | 86 (81.1) | 49 (76.6) | 37 (88.1) | |
| Controlled drugs | ||||
| None | 24 (22.6) | 18 (28.1) | 6 (14.3) | 0.096 |
| Yes | 82 (77.4) | 46 (71.9) | 36 (85.7) | |
| Anti- PsA drugs | ||||
| None | 32 (30.2) | 23 (35.9) | 9 (21.4) | 0.111 |
| Yes | 74 (69.8) | 41 (64.1) | 33 (78.6) | |
| Anti-MRSA drugs | ||||
| None | 65 (61.3) | 46 (71.9) | 19 (45.2) | 0.006 * |
| Yes | 41 (38.7) | 18 (28.1) | 23 (54.8) | |
| Catheterization | ||||
| None | 20 (18.9) | 13 (20.3) | 7 (16.7) | 0.639 |
| Yes | 86 (81.1) | 51 (79.7) | 35 (83.3) | |
| Use of endoscope | ||||
| None | 67 (63.2) | 40 (62.5) | 27 (64.3) | 0.852 |
| Yes | 39 (36.8) | 24 (37.5) | 15 (35.7) | |
| Use of CVC | ||||
| None | 90 (84.9) | 55 (85.9) | 35 (83.3) | 0.714 |
| Yes | 16 (15.1) | 9 (14.1) | 7 (16.7) | |
| Use of FOLEY | ||||
| None | 61 (57.5) | 38 (59.4) | 23 (54.8) | 0.638 |
| Yes | 45 (42.5) | 26 (40.6) | 19 (45.2) | |
| Use of ventilator | ||||
| None | 47 (44.3) | 29 (45.3) | 18 (42.9) | 0.803 |
| Yes | 59 (55.7) | 35 (54.7) | 24 (57.1) | |
| LOS a | 375.6 ± 487.9 | 307.3 ± 436.2 | 479.8 ± 546.5 | 0.018 * |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | β (95% CI) | |
| MDROs (Yes vs. None) | 0.62 (0.05, 1.18) | 0.033 * | 0.55 (0.02, 1.09) | 0.037 * |
| Age (>65 years vs. other) | 0.68 (0.10, 1.27) | 0.023 * | 0.25 (−0.34, 0.84) | 0.410 |
| Sex (Female vs. Male) | −0.36 (−0.92, 0.20) | 0.207 | −0.05 (−0.60, 0.50) | 0.857 |
| Sample | ||||
| Other | Ref. | Ref. | ||
| Sputum | 0.81 (−0.12, 1.74) | 0.087 | 0.86 (−0.01, 1.73) | 0.052 |
| Urine | 0.48 (−0.50, 1.46) | 0.331 | 0.82 (−0.17, 1.81) | 0.102 |
| Blood | 1.01 (−0.09, 2.11) | 0.071 | 1.12 (0.11, 2.14) | 0.031 |
| Previous ward (Yes vs. None) | 0.002 (−0.58, 0.58) | 0.993 | 0.26 (−0.35, 0.86) | 0.403 |
| Type of ward discharged (RCW vs. General ward) | 1.52 (0.94, 2.11) | <0.001 * | 1.16 (0.52, 1.80) | <0.001 * |
| Nutritional score | 0.16 (−0.08, 0.40) | 0.196 | −0.06 (−0.30, 0.18) | 0.616 |
| Antibiotics (Yes vs. None) | 0.59 (−0.12, 1.30) | 0.104 | 0.31 (−0.66, 1.28) | 0.530 |
| Controlled drug (Yes vs. None) | 0.60 (−0.07, 1.26) | 0.077 | −0.03 (−1.48, 1.42) | 0.966 |
| Anti-PsA drugs (Yes vs. None) | 0.52 (−0.09, 1.13) | 0.093 | 0.11 (−0.99, 1.21) | 0.844 |
| Anti-MRSA drugs (Yes vs. None) | 0.19 (−0.38, 0.77) | 0.507 | −0.28 (−0.93, 0.37) | 0.400 |
| Catheterization (Yes vs. None) | 1.37 (0.70, 2.04) | <0.001 * | 0.86 (0.03, 1.70) | 0.043 * |
| Use of endoscope (Yes vs. None) | −0.20 (−0.78, 0.39) | 0.507 | −0.22 (−0.90, 0.45) | 0.513 |
| Use of CVC (Yes vs. None) | 0.47 (−0.32, 1.25) | 0.242 | −0.18 (−0.95, 0.60) | 0.651 |
| Use of FOLEY (Yes vs. None) | 0.15 (−0.42, 0.72) | 0.597 | −0.37 (−0.93, 0.19) | 0.189 |
| Use of ventilator (Yes vs. None) | 0.99 (0.46, 1.53) | <0.001 * | 0.54 (−0.18, 1.25) | 0.139 |
| Sum of Squares | Degrees of Freedom | Mean Sum of Squares | F | Significance (p) | |
|---|---|---|---|---|---|
| Between Group | 21.665 | 4 | 5.416 | 3.412 | 0.018 |
| Within Group | 58.741 | 37 | 1.588 | ||
| Sum | 80.406 | 41 |
| Dependent Variable | MDRO a | Mean Difference | Standard Error | Significance (p) | Post-Hoc Test | |
|---|---|---|---|---|---|---|
| Log LOS | 1 | 2 | −1.24785 | 0.86948 | 0.725 | |
| 3 | −1.21241 | 1.15022 | 0.890 | |||
| 4 | 0.29371 | 0.82943 | 0.998 | |||
| 5 | −1.35252 | 0.78011 | 0.563 | |||
| Log LOS | 2 | 1 | 1.24785 | 0.86948 | 0.725 | |
| 3 | 0.03545 | 1.01025 | 1.000 | |||
| 4 | 1.54156 | 0.62093 | 0.211 | |||
| 5 | −0.10467 | 0.55333 | 1.000 | |||
| Log LOS | 3 | 1 | 1.21241 | 1.15022 | 0.890 | |
| 2 | −0.03545 | 1.01025 | 1.000 | |||
| 4 | 1.50612 | 0.97599 | 0.668 | |||
| 5 | −0.14012 | 0.93444 | 1.000 | |||
| Log LOS | 4 | 1 | −0.29371 | 0.82943 | 0.998 | |
| 2 | −1.54156 | 0.62093 | 0.211 | 5 > 4 | ||
| 3 | −1.50612 | 0.97599 | 0.668 | |||
| 5 | −1.64623 * | 0.48800 | 0.037 * | |||
| Log LOS | 5 | 1 | 1.35252 | 0.78011 | 0.563 | |
| 2 | 0.10467 | 0.55333 | 1.000 | |||
| 3 | 0.14012 | 0.93444 | 1.000 | 5 > 4 | ||
| 4 | 1.64623 * | 0.48800 | 0.037 * | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-P.; Tasi, X.-W.; Chang, K.; Cao, X.-D.; Chen, J.-R.; Liao, C.-S. Multi-Drug Resistant Organisms Infection Impact on Patients Length of Stay in Respiratory Care Ward. Antibiotics 2021, 10, 608. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050608
Chen Y-P, Tasi X-W, Chang K, Cao X-D, Chen J-R, Liao C-S. Multi-Drug Resistant Organisms Infection Impact on Patients Length of Stay in Respiratory Care Ward. Antibiotics. 2021; 10(5):608. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050608
Chicago/Turabian StyleChen, Yi-Ping, Xian-Wen Tasi, Ko Chang, Xuan-Di Cao, Jung-Ren Chen, and Chien-Sen Liao. 2021. "Multi-Drug Resistant Organisms Infection Impact on Patients Length of Stay in Respiratory Care Ward" Antibiotics 10, no. 5: 608. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050608