
Phage Targeting Streptococcus mutans In Vitro and In Vivo as a Caries-Preventive Modality

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
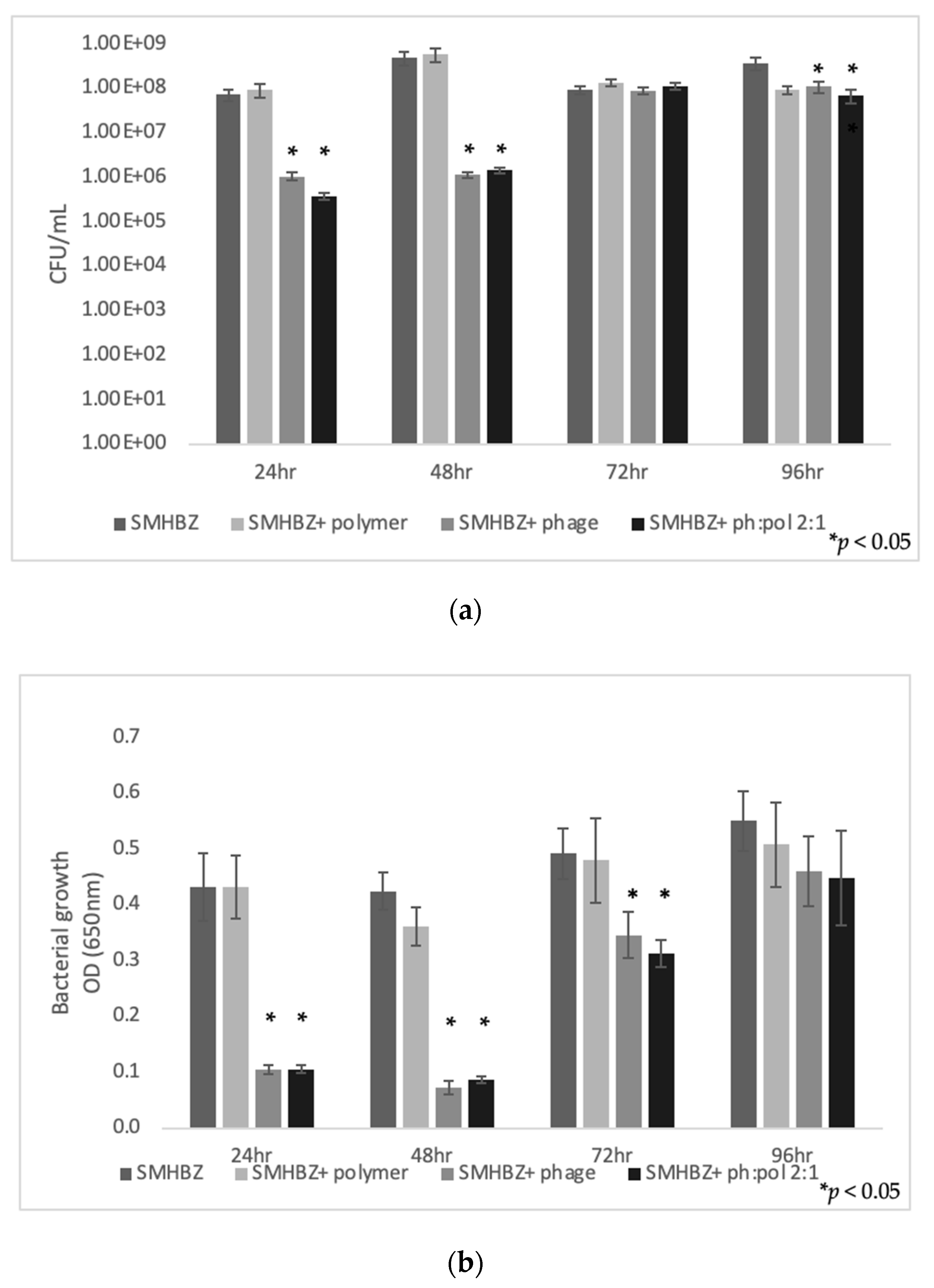
2.1. Assessment of Phage Lytic Activity against Streptococcus Mutans
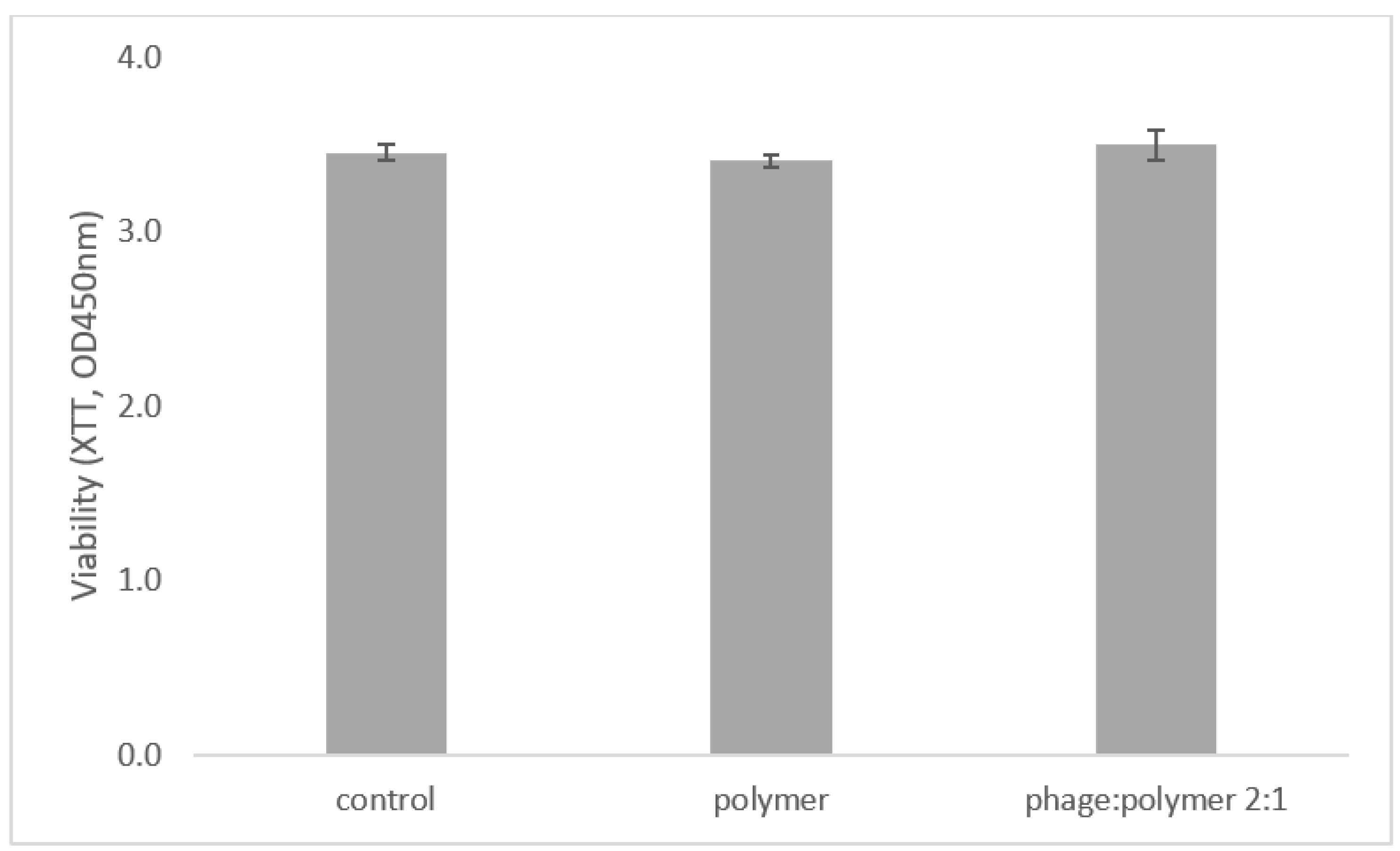
2.2. Phages and Polymer Are Not Toxic to Cells
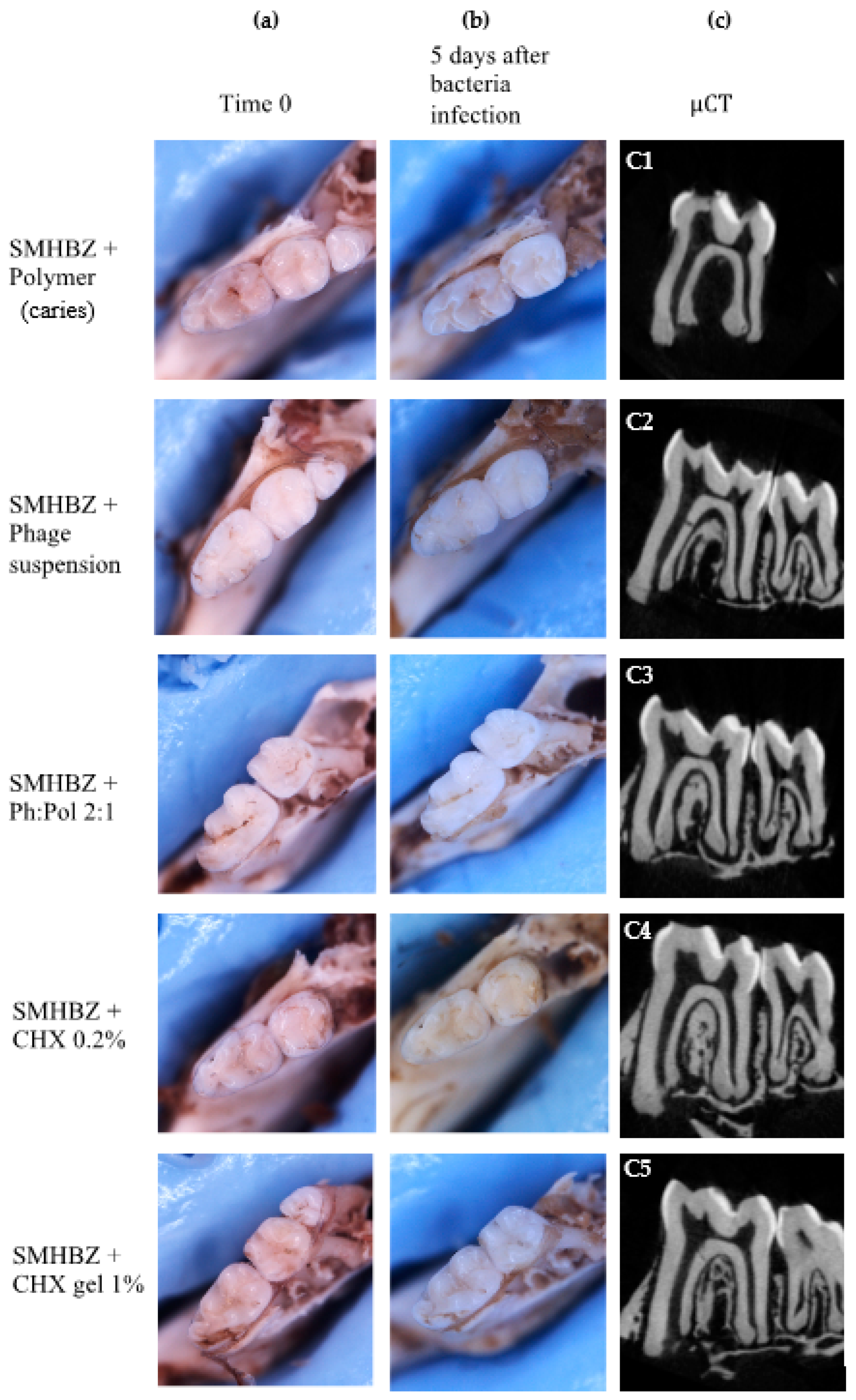
2.3. Phage Lytic Activity against S. mutans Prevented Caries Development In Vitro in Extracted-Jaw Caries Model
2.3.1. Clinical Evaluation
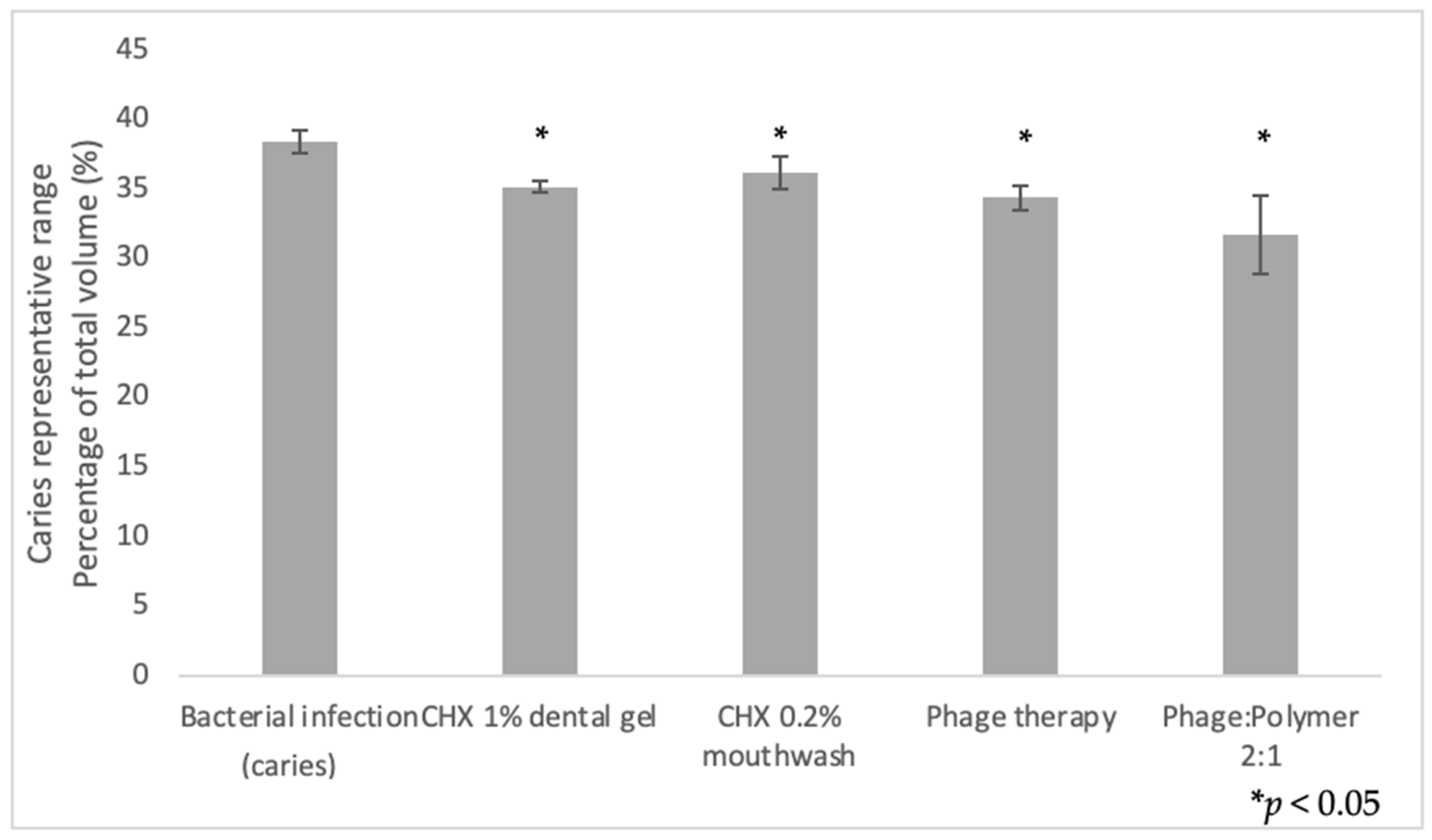
2.3.2. Quantification of Demineralization
2.3.3. Bacterial Outgrowth Evaluation
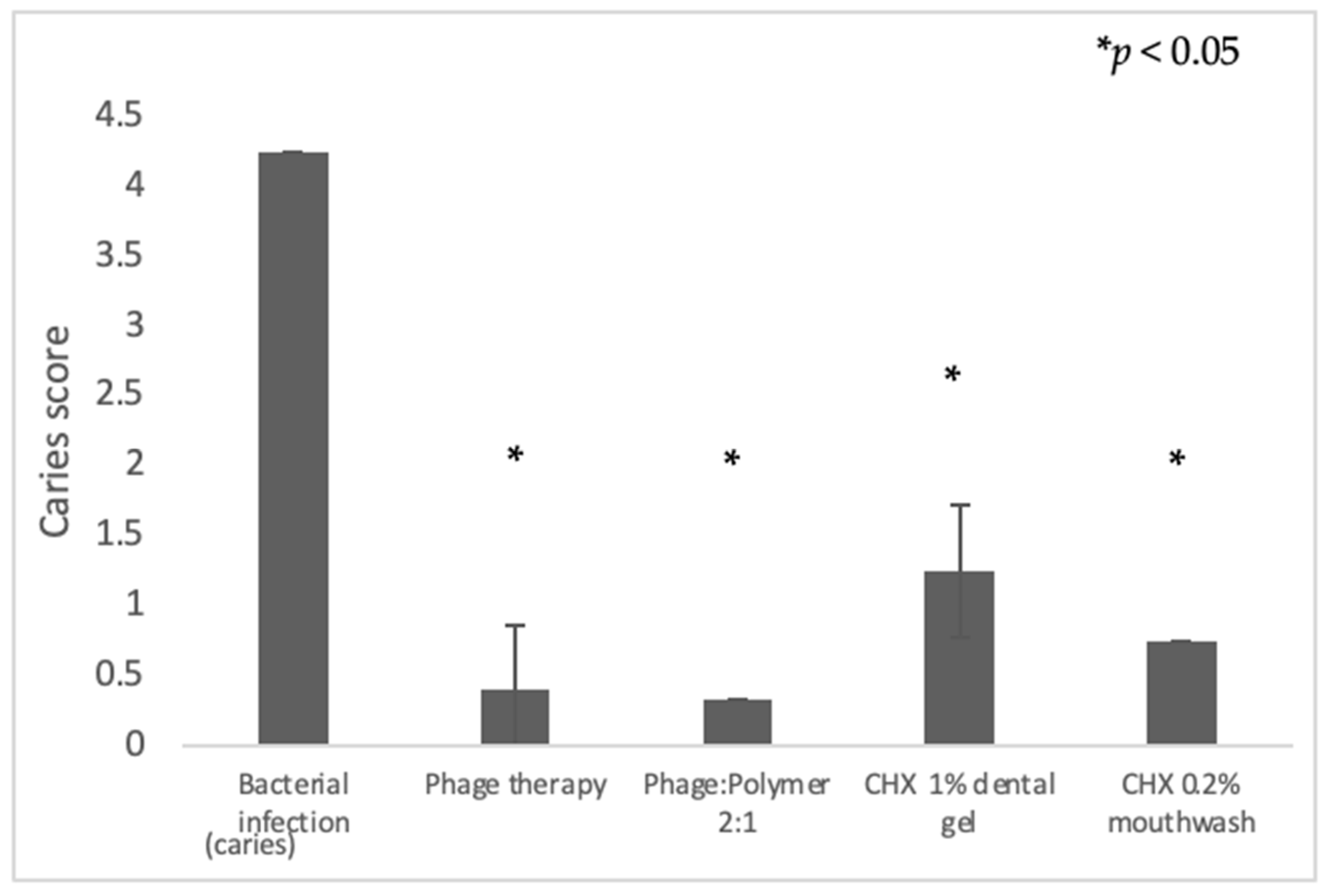
2.3.4. Caries Scoring Using a Novel Scoring Method over Hemi-Sectioned Molars
2.4. Phage Lytic Activity against S. mutans Prevented Caries Development in Experimental In Vivo Caries Model
2.4.1. Clinical Evaluation
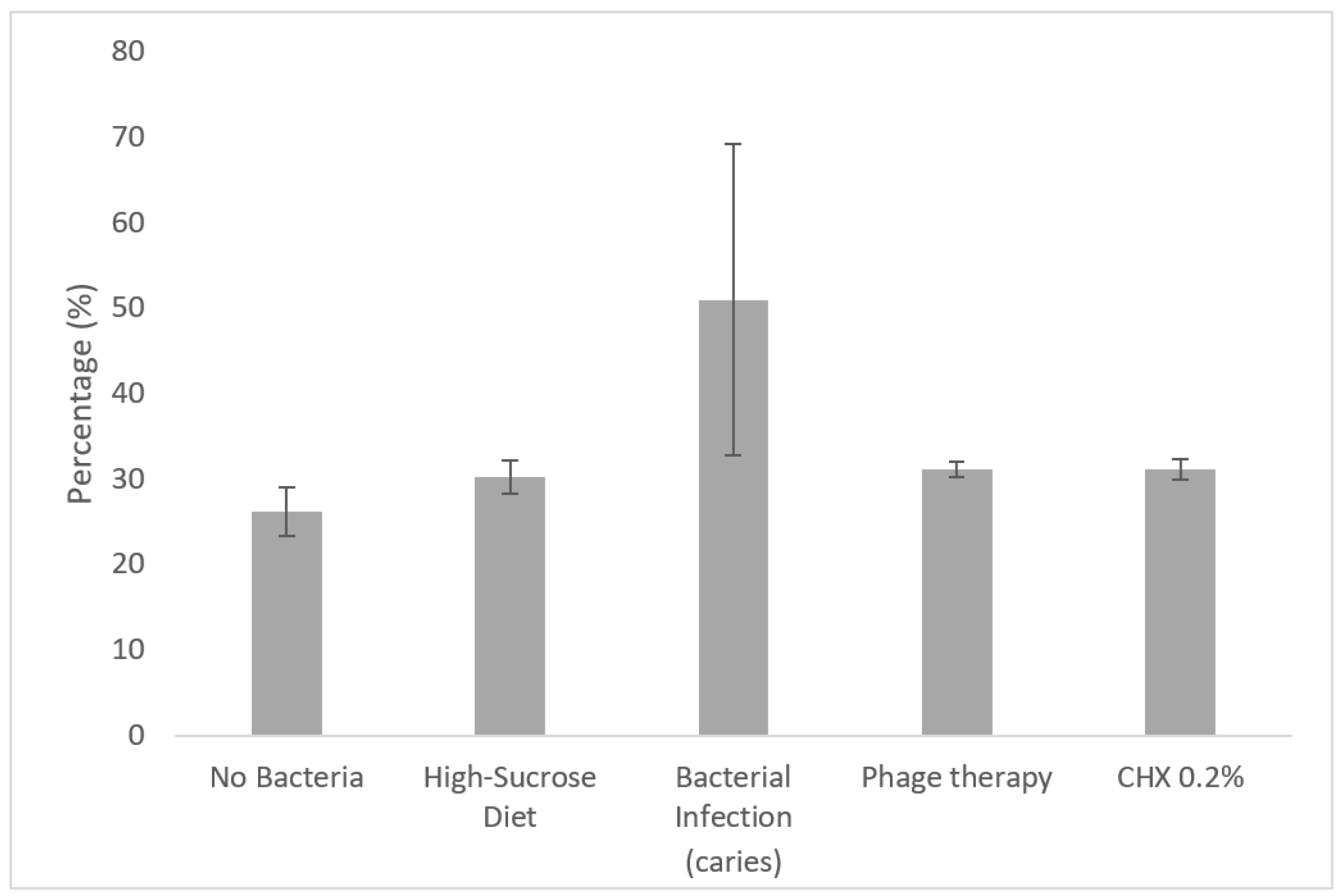
2.4.2. Quantification of Demineralization
3. Discussion
4. Materials and Methods
4.1. Bacterial and Phage Strains
4.2. Formulation
4.3. Phage Lytic Activity against S. mutans In Vitro
4.4. Polymer Toxicity Tests
4.5. Assessment of Phage Lytic Activity against S. mutans In Vitro in Extracted Jaw Caries Model
4.5.1. Preparation of Extracted Jaws
4.5.2. Saliva Sterilization
4.5.3. Caries-Promoting Environment
4.5.4. Anti-Caries Effect of Phage and Chlorhexidine
4.5.5. Photographic Depiction
4.5.6. Micro-Computed Tomography (μCT) Evaluation of Carious Lesions
4.5.7. Evaluation of Viable Count
4.5.8. Caries-Scoring Method for Hemi-Sectioned Molars
4.5.9. Statistical Analysis
4.6. Assessment of Phage Lytic Activity against S. mutans In Vivo in a Murine Caries Model
4.6.1. Mice
4.6.2. Bacterial Infection
4.6.3. Evaluation of Bacterial Outgrowth
4.6.4. Clinical and Radiographical Assessment of Dental Carious Lesion Development
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Featherstone, J.D. Dental caries: A dynamic disease process. Aust. Dent. J. 2008, 53, 286–291. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D. Dental biofilms: Difficult therapeutic targets. Periodontology 2000 2002, 28, 12–55. [Google Scholar] [CrossRef]
- Rugg-Gunn, A. Dental caries: Strategies to control this preventable disease. Acta Med. Acad. 2013, 42, 117–130. [Google Scholar] [CrossRef]
- Karpiński, T.M.; Szkaradkiewicz, A.K. Chlorhexidine--pharmaco-biological activity and application. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 1321–1326. [Google Scholar]
- Loesche, W.J. Role of Streptococcus mutans in human dental decay. Microbiol. Rev. 1986, 50, 353–380. [Google Scholar] [CrossRef] [PubMed]
- Shlezinger, M.; Khalifa, L.; Houri-Haddad, Y.; Coppenhagen-Glazer, S.; Resch, G.; Que, Y.A.; Beyth, S.; Dorfman, E.; Hazan, R.; Beyth, N. Phage Therapy: A New Horizon in the Antibacterial Treatment of Oral Pathogens. Curr. Top. Med. Chem. 2017, 17, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- Rehman, S.; Ali, Z.; Khan, M.; Bostan, N.; Naseem, S. The dawn of phage therapy. Rev. Med. Virol. 2019, 29, e2041. [Google Scholar] [CrossRef] [PubMed]
- Van der Ploeg, J.R. Genome sequence of Streptococcus mutans bacteriophage M102. FEMS Microbiol. Lett. 2007, 275, 130–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delisle, A.L.; Guo, M.; Chalmers, N.I.; Barcak, G.J.; Rousseau, G.M.; Moineau, S. Biology and genome sequence of Streptococcus mutans phage M102AD. Appl. Environ. Microbiol. 2012, 78, 2264–2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalmasso, M.; de Haas, E.; Neve, H.; Strain, R.; Cousin, F.J.; Stockdale, S.R.; Ross, R.P.; Hill, C. Isolation of a Novel Phage with Activity against Streptococcus mutans Biofilms. PLoS ONE 2015, 10, e0138651. [Google Scholar] [CrossRef] [Green Version]
- Ben-Zaken, H.; Kraitman, R.; Coppenhagen-Glazer, S.; Khalifa, L.; Alkalay-Oren, S.; Gelman, D.; Ben-Gal, G.; Beyth, N.; Hazan, R. Isolation and Characterization of Streptococcus mutans Phage as a Possible Treatment Agent for Caries. Viruses 2021, 13, 825. [Google Scholar] [CrossRef]
- Bachrach, G.; Leizerovici-Zigmond, M.; Zlotkin, A.; Naor, R.; Steinberg, D. Bacteriophage isolation from human saliva. Lett. Appl. Microbiol. 2003, 36, 50–53. [Google Scholar] [CrossRef]
- Malik, D.J.; Sokolov, I.J.; Vinner, G.K.; Mancuso, F.; Cinquerrui, S.; Vladisavljevic, G.T.; Clokie, M.R.J.; Garton, N.J.; Stapley, A.G.F.; Kirpichnikova, A. Formulation, stabilisation and encapsulation of bacteriophage for phage therapy. Adv. Colloid Interface Sci. 2017, 249, 100–133. [Google Scholar] [CrossRef] [Green Version]
- Shlezinger, M.; Friedman, M.; Houri-Haddad, Y.; Hazan, R.; Beyth, N. Phages in a thermoreversible sustained-release formulation targeting E. faecalis in vitro and in vivo. PLoS ONE 2019, 14, e0219599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Menéndez, E.; Fernández, L.; Gutiérrez, D.; Rodríguez, A.; Martínez, B.; García, P. Comparative analysis of different preservation techniques for the storage of Staphylococcus phages aimed for the industrial development of phage-based antimicrobial products. PLoS ONE 2018, 13, e0205728. [Google Scholar] [CrossRef]
- Czerninski, R.; Sivan, S.; Steinberg, D.; Gati, I.; Kagan, L.; Friedman, M. A novel sustained-release clotrimazole varnish for local treatment of oral candidiasis. Clin. Oral Investig. 2010, 14, 71–78. [Google Scholar] [CrossRef]
- Czerninski, R.; Pikovsky, A.; Gati, I.; Friedman, M.; Steinberg, D. Comparison of the efficacy of a novel sustained release clotrimazole varnish and clotrimazole troches for the treatment of oral candidiasis. Clin. Oral Investig. 2015, 19, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Park, K.J.; Meißner, T.; Günther, E.; Schmalz, G.; Kottmann, T.; Krause, F.; Haak, R.; Ziebolz, D. Arrest of root caries with an adjuvant chlorhexidine-fluoride varnish over a 12-months observation period: A QLF-analyzed, placebo-controlled, randomized, clinical trial (RCT). Odontology 2021. [Google Scholar] [CrossRef]
- Cao, H.Z.; Wang, S.; Pan, Y. An investigation of the clinical effect of the 0.3% Triclosan varnish on caries prevention of primary teeth. Shanghai Kou Qiang Yi Xue 2007, 16, 8–10. [Google Scholar] [PubMed]
- Göstemeyer, G.; Woike, H.; Paris, S.; Schwendicke, F.; Schlafer, S. Root Caries Preventive Effect of Varnishes Containing Fluoride or Fluoride + Chlorhexidine/Cetylpyridinium Chloride In Vitro. Microorganisms 2021, 9, 737. [Google Scholar] [CrossRef]
- Wolfoviz-Zilberman, A.; Houri-Haddad, Y.; Beyth, N. A Novel Dental Caries Model Replacing, Refining, and Reducing Animal Sacrifice. Appl. Sci. 2021, 11, 7141. [Google Scholar] [CrossRef]
- Park, K.J.; Kroker, T.; Gross, U.; Zimmermann, O.; Krause, F.; Haak, R.; Ziebolz, D. Effectiveness of caries-preventing agents on initial carious lesions within the scope of orthodontic therapy. Korean J. Orthod. 2019, 49, 246–253. [Google Scholar] [CrossRef]
- Yeon, L.S.; Young, L.S. Susceptibility of Oral Streptococci to Chlorhexidine and Cetylpyridinium Chloride. Biocontrol. Sci. 2019, 24, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Buzalaf, M.A.R.; Pessan, J.P.; Honório, H.M.; Ten Cate, J.M. Mechanisms of action of fluoride for caries control. Monogr. Oral Sci. 2011, 22, 97–114. [Google Scholar] [CrossRef]
- Songsiripradubboon, S.; Hamba, H.; Trairatvorakul, C.; Tagami, J. Sodium fluoride mouthrinse used twice daily increased incipient caries lesion remineralization in an in situ model. J. Dent. 2014, 42, 271–278. [Google Scholar] [CrossRef]
- Almeida, L.F.; Marin, L.M.; Martinez-Mier, E.A.; Cury, J.A. Fluoride Dentifrice Overcomes the Lower Resistance of Fluorotic Enamel to Demineralization. Caries Res. 2019, 53, 567–575. [Google Scholar] [CrossRef]
- Khalifa, L.; Brosh, Y.; Gelman, D.; Coppenhagen-Glazer, S.; Beyth, S.; Poradosu-Cohen, R.; Que, Y.A.; Beyth, N.; Hazan, R. Targeting Enterococcus faecalis biofilms with phage therapy. Appl. Environ. Microbiol. 2015, 81, 2696–2705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maske, T.T.; van de Sande, F.H.; Arthur, R.A.; Huysmans, M.C.D.N.; Cenci, M.S. In vitro biofilm models to study dental caries: A systematic review. Biofouling 2017, 33, 661–675. [Google Scholar] [CrossRef] [PubMed]
- Premaraj, T.S.; Rohani, N.; Covey, D.; Premaraj, S. In vitro evaluation of surface properties of Pro Seal((R)) and Opal((R)) Seal(TM) in preventing white spot lesions. Orthod Craniofac Res 2017, 20 Suppl 1, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Montasser, M.A.; El-Wassefy, N.A.; Taha, M. In vitro study of the potential protection of sound enamel against demineralization. Prog Orthod 2015, 16, 12. [Google Scholar] [CrossRef] [Green Version]
- Caldeira, E.M.; Telles, V.; Mattos, C.T.; Nojima, M. Surface morphologic evaluation of orthodontic bonding systems under conditions of cariogenic challenge. Braz. Oral Res. 2019, 33, e029. [Google Scholar] [CrossRef]
- Sabel, N.; Robertson, A.; Nietzsche, S.; Norén, J.G. Demineralization of enamel in primary second molars related to properties of the enamel. Sci. World J. 2012, 2012, 587254. [Google Scholar] [CrossRef] [Green Version]
- Lazzari, V.; Tafforeau, P.; Aguilar, J.-P.; Michaux, J. Topographic maps applied to comparative molar morphology: The case of murine and cricetine dental plans (Rodentia, Muroidea). Paleobiology 2016, 34, 46–64. [Google Scholar] [CrossRef]
- Hartles, R.L. Experimental dental caries in the rat. Proc. R. Soc. Med. 1960, 53, 528–531. [Google Scholar] [CrossRef] [Green Version]
- Khalifa, L.; Gelman, D.; Shlezinger, M.; Dessal, A.L.; Coppenhagen-Glazer, S.; Beyth, N.; Hazan, R. Defeating Antibiotic- and Phage-Resistant Enterococcus faecalis Using a Phage Cocktail in Vitro and in a Clot Model. Front. Microbiol. 2018, 9, 326. [Google Scholar] [CrossRef] [Green Version]
- Khalifa, L.; Coppenhagen-Glazer, S.; Shlezinger, M.; Kott-Gutkowski, M.; Adini, O.; Beyth, N.; Hazan, R. Complete Genome Sequence of Enterococcus Bacteriophage EFLK1. Genome announcements 2015, 3. [Google Scholar] [CrossRef] [Green Version]
- Roehm, N.W.; Rodgers, G.H.; Hatfield, S.M.; Glasebrook, A.L. An improved colorimetric assay for cell proliferation and viability utilizing the tetrazolium salt XTT. J. Immunol. Methods 1991, 142, 257–265. [Google Scholar] [CrossRef]
- Scudiero, D.A.; Shoemaker, R.H.; Paull, K.D.; Monks, A.; Tierney, S.; Nofziger, T.H.; Currens, M.J.; Seniff, D.; Boyd, M.R. Evaluation of a soluble tetrazolium/formazan assay for cell growth and drug sensitivity in culture using human and other tumor cell lines. Cancer Res. 1988, 48, 4827–4833. [Google Scholar] [PubMed]
- Kalfas, S.; Rundegren, J. Biological qualities of saliva sterilized by filtration or ethylene oxide treatment. Oral Microbiol. Immunol. 1991, 6, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Goldman, E.; Reich, E.; Abramovitz, I.; Klutstein, M. Inducing Apical Periodontitis in Mice. J. Vis. Exp. 2019. [Google Scholar] [CrossRef] [PubMed]
- Keyes, P.H. Dental caries in the molar teeth of rats. I. Distribution of lesions induced by high-carbohydrate low-fat diets. J. Dent. Res. 1958, 37, 1077–1087. [Google Scholar] [CrossRef] [PubMed]
- Velusamy, S.K.; Markowitz, K.; Fine, D.H.; Velliyagounder, K. Human lactoferrin protects against Streptococcus mutans-induced caries in mice. Oral Dis. 2016, 22, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Culp, D.J.; Robinson, B.; Cash, M.N.; Bhattacharyya, I.; Stewart, C.; Cuadra-Saenz, G. Salivary mucin 19 glycoproteins: Innate immune functions in Streptococcus mutans-induced caries in mice and evidence for expression in human saliva. J. Biol. Chem. 2015, 290, 2993–3008. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Bi, Y.; Shang, X.; Wang, M.; Linden, S.B.; Li, Y.; Nelson, D.C.; Wei, H. Antibiofilm Activities of a Novel Chimeolysin against Streptococcus mutans under Physiological and Cariogenic Conditions. Antimicrob. Agents Chemother. 2016, 60, 7436–7443. [Google Scholar] [CrossRef] [PubMed] [Green Version]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolfoviz-Zilberman, A.; Kraitman, R.; Hazan, R.; Friedman, M.; Houri-Haddad, Y.; Beyth, N. Phage Targeting Streptococcus mutans In Vitro and In Vivo as a Caries-Preventive Modality. Antibiotics 2021, 10, 1015. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10081015
Wolfoviz-Zilberman A, Kraitman R, Hazan R, Friedman M, Houri-Haddad Y, Beyth N. Phage Targeting Streptococcus mutans In Vitro and In Vivo as a Caries-Preventive Modality. Antibiotics. 2021; 10(8):1015. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10081015
Chicago/Turabian StyleWolfoviz-Zilberman, Amit, Reut Kraitman, Ronen Hazan, Michael Friedman, Yael Houri-Haddad, and Nurit Beyth. 2021. "Phage Targeting Streptococcus mutans In Vitro and In Vivo as a Caries-Preventive Modality" Antibiotics 10, no. 8: 1015. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10081015