
Antimicrobial Consumption among 66 Acute Care Hospitals in Catalonia: Impact of the COVID-19 Pandemic

 , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Results
2.1. Evolution of COVID-19 Pandemic in Catalonia during 2020
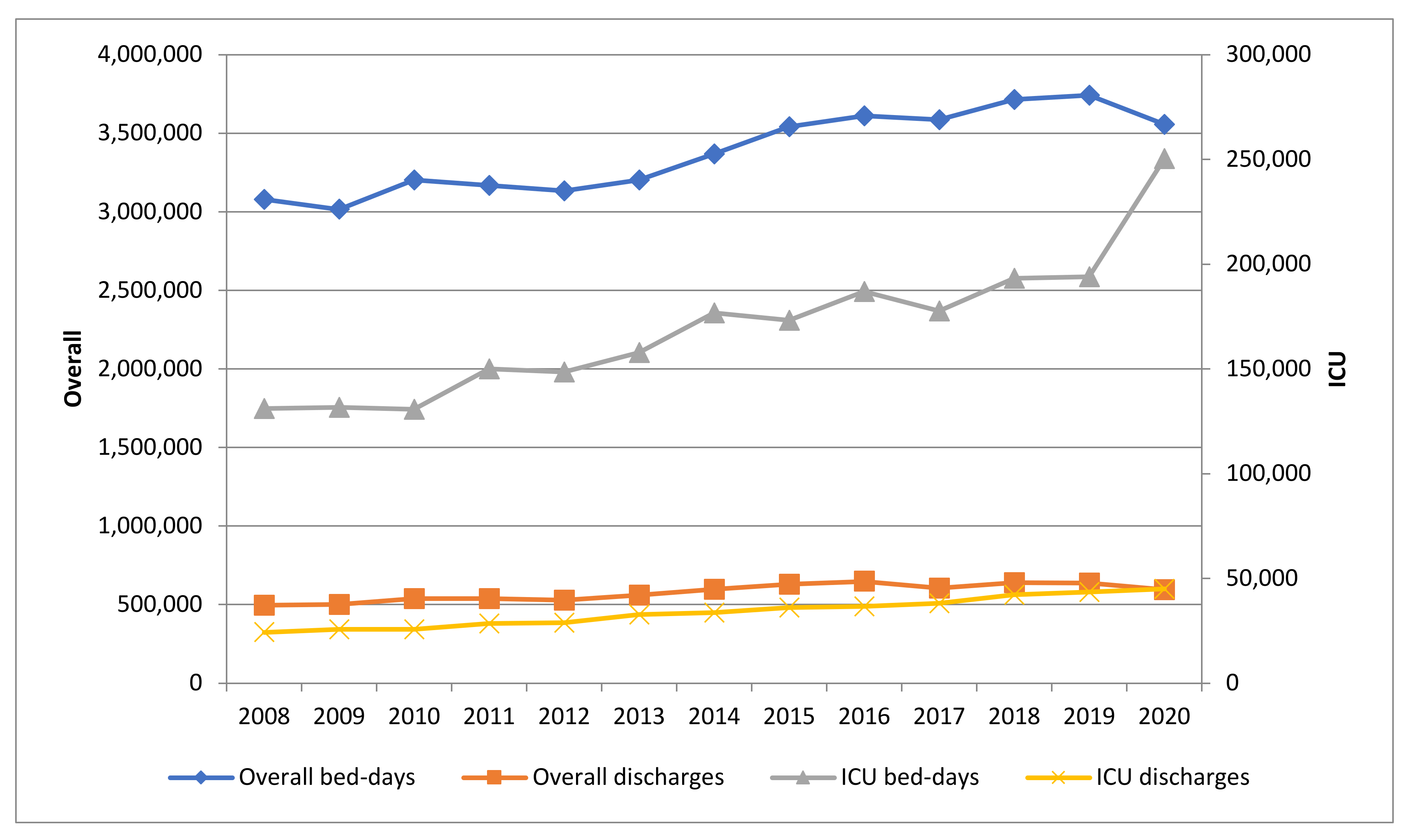
2.2. Evolution of Overall and ICU Bed-Days and Discharges 2008–2020
2.3. Changes in Global Consumption of Anti-Infectives for Systemic Use 2019–2020
2.4. Changes in ICU Consumption of Anti-Infectives for Systemic Use 2019–2020
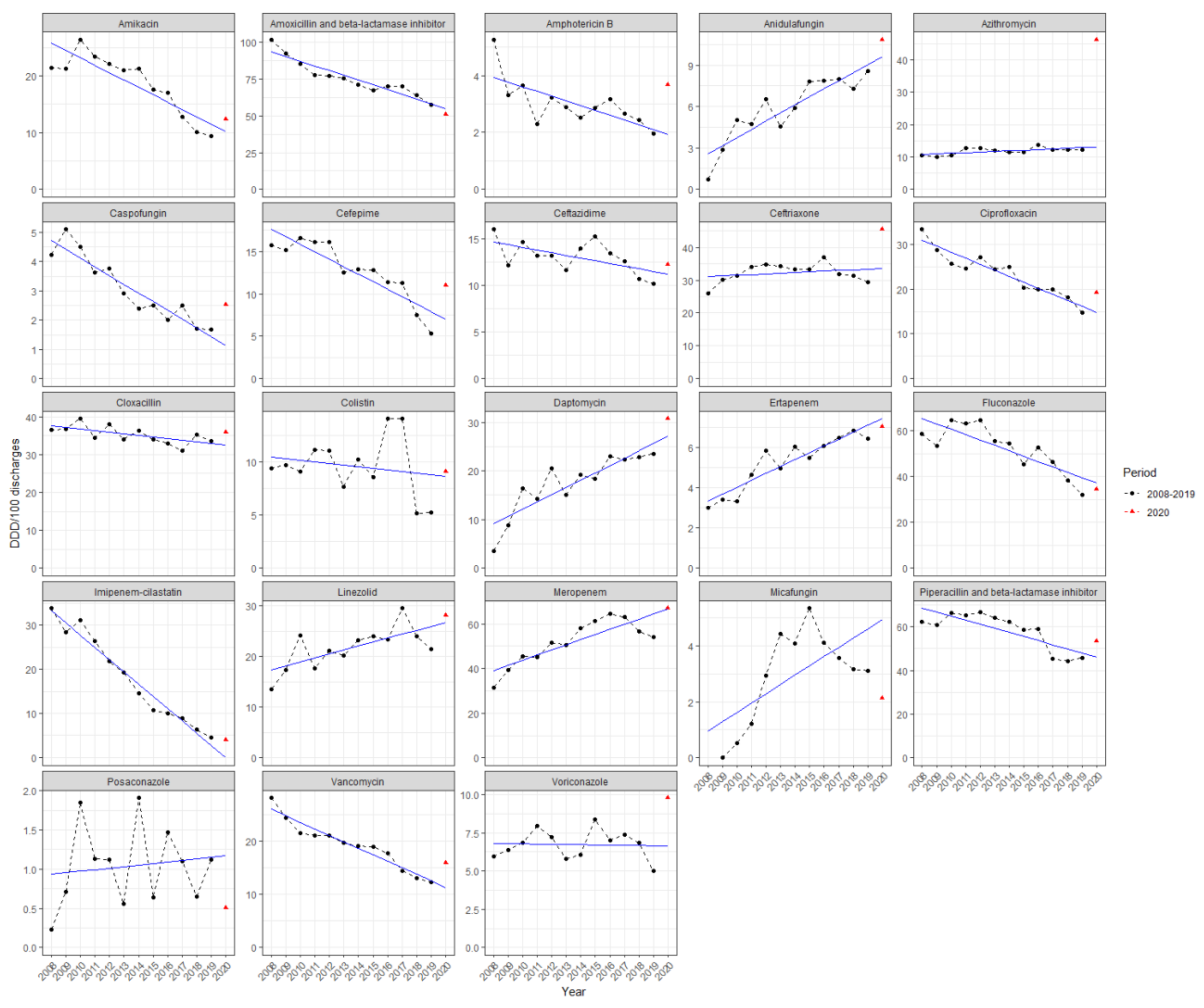
2.5. Comparison between Estimated and Observed ICU Consumption, Expressed in DDD/100 Discharges, in 2020
3. Discussion
4. Materials and Methods
4.1. Setting and Study Design
4.2. Data Collection
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus disease 2019–COVID-19. Clin. Microbiol. Rev. 2020, 33, 1–48. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Grau, S.; Echeverria-Esnal, D.; Gómez-Zorrilla, S.; Navarrete-Rouco, M.E.; Masclans, J.R.; Espona, M.; Gracia-Arnillas, M.P.; Duran, X.; Comas, M.; Horcajada, J.P.; et al. Evolution of antimicrobial consumption during the first wave of covid-19 pandemic. Antibiotics 2021, 10, 132. [Google Scholar] [CrossRef]
- WHO. COVID-19 Weekly Epidemiological Update 35; World Health Organization: Geneva, Switzerland, 2021; pp. 1–3. [Google Scholar]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 illness in native and immunosuppressed states: A clinical–therapeutic staging proposal. J. Hear. Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 10022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1729. [Google Scholar] [CrossRef]
- Russell, C.D.; Fairfield, C.J.; Drake, T.M.; Turtle, L.; Seaton, R.A.; Wootton, D.G.; Sigfrid, L.; Harrison, E.M.; Docherty, A.B.; de Silva, T.I.; et al. Co-infections, secondary infections, and antimicrobial use in patients hospitalised with COVID-19 during the first pandemic wave from the ISARIC WHO CCP-UK study: A multicentre, prospective cohort study. Lancet Microbe 2021, 5247, 1–12. [Google Scholar] [CrossRef]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influenza Other Respi. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef]
- Thorburn, K.; Harigopal, S.; Reddy, V.; Taylor, N.; Van Saene, H.K.F. High incidence of pulmonary bacterial co-infection in children with severe respiratory syncytial virus (RSV) bronchiolitis. Thorax 2006, 61, 611–615. [Google Scholar] [CrossRef] [Green Version]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.P.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 520–531. [Google Scholar] [CrossRef]
- WHO. Clinical Management Clinical Management Living Guidance COVID-19; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Guisado-Gil, A.B.; Infante-Domínguez, C.; Peñalva, G.; Praena, J.; Roca, C.; Navarro-Amuedo, M.D.; Aguilar-Guisado, M.; Espinosa-Aguilera, N.; Poyato-Borrego, M.; Romero-Rodríguez, N.; et al. Impact of the COVID-19 pandemic on antimicrobial consumption and hospital-acquired candidemia and multidrug-resistant bloodstream infections. Antibiotics 2020, 9, 816. [Google Scholar] [CrossRef] [PubMed]
- Abelenda-Alonso, G.; Padullés, A.; Rombauts, A.; Gudiol, C.; Pujol, M.; Alvarez-Pouso, C.; Jodar, R.; Carratalà, J. Antibiotic prescription during the COVID-19 pandemic: A biphasic pattern. Infect. Control Hosp. Epidemiol. 2020, 41, 1371–1372. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Zorn, B. Antibiotic use in the COVID-19 crisis in Spain. Clin. Microbiol. Infect. 2021, 27, 646–647. [Google Scholar] [CrossRef] [PubMed]
- VINCat Program. Programa de Vigilància de les Infeccions Nosocomials a Catalunya. Generalitat de Catalunya. Departament de Salut. Available online: http://catsalut.gencat.cat/ca/proveidors-professionals/vincat/ (accessed on 13 June 2021).
- Microsoft Power, BI. Available online: https://app.powerbi.com/view?r=eyJrIjoiOGIyNjgzYjctYjA0Ny00ZDRmLWIxNjctM2RkZWZhMDQ0ZjRiIiwidCI6IjNiOTQyN2RjLWQzMGUtNDNiYy04YzA2LWZmNzI1MzY3NmZlYyIsImMiOjh9 (accessed on 30 July 2021).
- Ministerio de Sanidad. Actualización nº 282. Enfermedad por el Coronavirus (COVID-19). Gobierno de España. 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_282_COVID-19.pdf (accessed on 2 August 2021).
- Fondevilla, E.; Grau, S.; Echeverría-Esnal, D.; Gudiol, F. Antibiotic consumption trends among acute care hospitals in Catalonia (2008–2016): Impact of different adjustments on the results. Expert Rev. Anti. Infect. Ther. 2021, 19, 245–251. [Google Scholar] [CrossRef]
- SEMICYUC Estudio Nacional De Vigilancia De Infección Nosocomial (Envin-Helics) 2020; SEMICYUC: Madrid, Spain, 2020; Available online: https://hws.vhebron.net/envin-helics/Help/COVID19/ENVIN-COVID_Infome_20.pdf (accessed on 25 June 2021).
- Kayaaslan, B.; Eser, F.; Kaya Kalem, A.; Bilgic, Z.; Asilturk, D.; Hasanoglu, I.; Ayhan, M.; Tezer Tekce, Y.; Erdem, D.; Turan, S.; et al. Characteristics of Candidemia in COVID-19 Patients; Increased Incidence, Earlier Occurrence, and Higher Mortality Rates Compared to Non-COVID-19 Patients. Mycoses 2021. [Google Scholar] [CrossRef]
- Estella, Á.; Vidal-Cortés, P.; Rodriguez, A.; Ojeda, D.A.; Martin-Loeches, I.; Díaz, E.; Suberviola, B.; Arnillas, M.G.; González, M.C.; Álvarez-Lerma, F.; et al. Manejo de las complicaciones infecciosas asociadas con la infección por coronavirus en pacientes graves ingresados en UCI. Med. Intensiva 2021. [Google Scholar] [CrossRef]
- Chappell, L.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19—Preliminary Report. N. Engl. J. Med. 2020, 1813–1836. [Google Scholar] [CrossRef]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Johnson, M.D.; Lewis, R.E.; Dodds Ashley, E.S.; Ostrosky-Zeichner, L.; Zaoutis, T.; Thompson, G.R.; Andes, D.R.; Walsh, T.J.; Pappas, P.G.; Cornely, O.A.; et al. Core recommendations for antifungal stewardship: A statement of the mycoses study group education and research consortium. J. Infect. Dis. 2020, 222, S175–S198. [Google Scholar] [CrossRef]
- Cornely, O.A.; Maertens, J.; Bresnik, M.; Ebrahimi, R.; Ullmann, A.J.; Bouza, E.; Heussel, C.P.; Lorttiolary, O.; Rieger, C.; Boehrne, A.; et al. Liposomal amphotericin B as initial therapy for invasive mold infection: A randomized trial comparing a high-loading dose regimen with standard dosing (AmBiLoad Trial). Clin. Infect. Dis. 2007, 44, 1289–1297. [Google Scholar] [CrossRef]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur. Respir. J. 2017, 50. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Petersen, E. COVID-19 is not influenza. Lancet Respir. Med. 2021, 9, 219–220. [Google Scholar] [CrossRef]
- Piroth, L.; Cottenet, J.; Mariet, A.S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; Quantin, C. Comparison of the characteristics, morbidity, and mortality of COVID-19 and seasonal influenza: A nationwide, population-based retrospective cohort study. Lancet Respir. Med. 2021, 9, 251–259. [Google Scholar] [CrossRef]
- De Waele, J.J.; Derde, L.; Bassetti, M. Antimicrobial stewardship in ICUs during the COVID-19 pandemic: Back to the 90s? Intensive Care Med. 2021, 47, 104–106. [Google Scholar] [CrossRef] [PubMed]
- Afshinnekoo, E.; Bhattacharya, C.; Burguete-García, A.; Castro-Nallar, E.; Deng, Y.; Desnues, C.; Dias-Neto, E.; Elhaik, E.; Iraola, G.; Jang, S.; et al. COVID-19 drug practices risk antimicrobial resistance evolution. Lancet Microbe 2021, 2, e135–e136. [Google Scholar] [CrossRef]
- Stevens, M.P.; Patel, P.K.; Nori, P. Involving antimicrobial stewardship programs in COVID-19 response efforts: All hands on deck. Infect. Control Hosp. Epidemiol. 2020, 41, 744–745. [Google Scholar] [CrossRef] [Green Version]
- Buehrle, D.J.; Decker, B.K.; Wagener, M.M.; Adalja, A.; Singh, N.; McEllistrem, M.C.; Nguyen, M.H.; Clancy, C.J. Antibiotic Consumption and Stewardship at a Hospital outside of an Early Coronavirus Disease 2019 Epicenter. Antimicrob. Agents Chemother. 2020, 64. [Google Scholar] [CrossRef] [PubMed]
- Khor, W.P.; Olaoye, O.; D’arcy, N.; Krockow, E.M.; Elshenawy, R.A.; Rutter, V.; Ashiru-Oredope, D. The need for ongoing antimicrobial stewardship during the COVID-19 pandemic and actionable recommendations. Antibiotics 2020, 9, 904. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.M. Antimicrobial Stewardship Programs: Appropriate Measures and Metrics to Study their Impact. Curr. Treat. Options Infect. Dis. 2014, 6, 101–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| DDD/100 Bed-Days | DDD/100 Discharges | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Service | ATC Classification | 2019 | 2020 | Variation (%) | p | 2019 | 2020 | Variation (%) | p | |
| Overall | J01 Antibacterials for systemic use | 69.38 | 70.99 | 2.31 | <0.001 | 407.41 | 424.30 | 4.15 | <0.001 | |
| J01C Penicillins | 23.63 | 21.70 | −8.18 | <0.001 | 138.76 | 129.69 | −6.53 | <0.001 | ||
| J01CR Combinations of penicillins. incl. beta-lactamase inhibitors | 18.26 | 16.80 | −7.98 | <0.001 | 107.23 | 100.44 | −6.33 | <0.001 | ||
| J01DBCDE Cephalosporins | 14.10 | 15.19 | 7.78 | <0.001 | 82.78 | 90.82 | 9.71 | <0.001 | ||
| J01DD Third-generation cephalosporins | 7.56 | 9.51 | 25.72 | <0.001 | 44.40 | 56.82 | 27.97 | <0.001 | ||
| J01DE Fourth-generation cephalosporins | 0.64 | 0.65 | 2.05 | 0.03 | 3.75 | 3.89 | 3.87 | <0.001 | ||
| J01DH Carbapenems | 5.01 | 5.16 | 2.93 | <0.001 | 29.41 | 30.82 | 4.77 | <0.001 | ||
| J01DI Other cephalosporins and penems | 0.29 | 0.37 | 29.00 | <0.001 | 1.68 | 2.20 | 31.32 | <0.001 | ||
| J01FA Macrolides | 3.26 | 6.69 | 105.40 | <0.001 | 19.13 | 40.00 | 109.08 | <0.001 | ||
| J01G Aminoglycoside antibacterials | 1.82 | 1.63 | −10.72 | <0.001 | 10.69 | 9.71 | −9.12 | <0.001 | ||
| J01M Quinolone antibacterials | 8.48 | 7.20 | −15.01 | <0.001 | 49.77 | 43.06 | −13.49 | <0.001 | ||
| J01X Other antibacterials | 8.89 | 9.39 | 5.72 | <0.001 | 52.18 | 56.15 | 7.61 | <0.001 | ||
| J01XA Glycopeptide antibacterials | 2.56 | 2.75 | 7.43 | <0.001 | 15.01 | 16.42 | 9.36 | <0.001 | ||
| J01XB Polymyxins | 0.39 | 0.34 | −12.96 | <0.001 | 2.28 | 2.02 | −11.40 | <0.001 | ||
| J01XX Other antibacterials | 3.70 | 4.01 | 8.45 | <0.001 | 21.72 | 23.98 | 10.39 | <0.001 | ||
| J02A Antimycotics for systemic use | 3.11 | 3.43 | 10.25 | <0.001 | 18.24 | 20.47 | 12.22 | <0.001 | ||
| J02AB Imidazole derivatives | 0.00 | 0.00 | −81.25 | <0.001 | 0.03 | 0.01 | −80.99 | <0.001 | ||
| J02AC Triazole derivatives | 2.61 | 2.81 | 7.85 | <0.001 | 15.31 | 16.81 | 9.78 | <0.001 | ||
| J02AX Other antimycotics for systemic use | 0.39 | 0.44 | 14.62 | <0.001 | 2.27 | 2.64 | 16.67 | <0.001 | ||
| ICU | J01 Antibacterials for systemic use | 114.23 | 112.77 | −1.28 | <0.001 | 508.18 | 627.21 | 23.42 | <0.001 | |
| J01C Penicillins | 32.92 | 27.40 | −16.78 | <0.001 | 146.46 | 152.38 | 4.04 | <0.001 | ||
| J01CR Combinations of penicillins. incl. beta-lactamase inhibitors | 23.24 | 18.74 | −19.35 | <0.001 | 103.37 | 104.23 | 0.84 | 0.21 | ||
| J01DBCDE Cephalosporins | 17.26 | 18.20 | 5.46 | <0.001 | 76.80 | 101.26 | 31.84 | <0.001 | ||
| J01DD Third-generation cephalosporins | 12.11 | 13.78 | 13.82 | <0.001 | 53.87 | 76.66 | 42.30 | <0.001 | ||
| J01DE Fourth-generation cephalosporins | 1.20 | 1.98 | 65.04 | <0.001 | 5.35 | 11.03 | 106.35 | <0.001 | ||
| J01DH Carbapenems | 14.66 | 14.02 | −4.32 | <0.001 | 65.20 | 77.99 | 19.62 | <0.001 | ||
| J01DI Other cephalosporins and penems | 0.87 | 1.19 | 36.09 | <0.001 | 3.88 | 6.60 | 70.13 | <0.001 | ||
| J01FA Macrolides | 7.62 | 13.60 | 78.44 | <0.001 | 33.90 | 75.62 | 123.09 | <0.001 | ||
| J01G Aminoglycoside antibacterials | 4.11 | 3.88 | −5.64 | <0.001 | 18.30 | 21.58 | 17.97 | <0.001 | ||
| J01M Quinolone antibacterials | 9.33 | 8.18 | −12.39 | <0.001 | 41.52 | 45.48 | 9.54 | <0.001 | ||
| J01X Other antibacterials | 19.34 | 19.67 | 1.69 | 0.01 | 86.04 | 109.38 | 27.13 | <0.001 | ||
| J01XA Glycopeptide antibacterials | 5.41 | 5.65 | 4.49 | <0.001 | 24.07 | 31.45 | 30.64 | <0.001 | ||
| J01XB Polymyxins | 1.17 | 1.64 | 40.27 | <0.001 | 5.20 | 9.11 | 75.36 | <0.001 | ||
| J01XX Other antibacterials | 10.46 | 10.82 | 3.40 | <0.001 | 46.55 | 60.18 | 29.28 | <0.001 | ||
| J02A Antimycotics for systemic use | 12.35 | 11.81 | −4.35 | <0.001 | 54.93 | 65.68 | 19.58 | <0.001 | ||
| J02AB Imidazole derivatives | 0.00 | 0.00 | - | - | 0.00 | 0.00 | - | - | ||
| J02AC Triazole derivatives | 8.91 | 8.36 | −6.17 | <0.001 | 39.62 | 46.48 | 17.31 | <0.001 | ||
| J02AX Other antimycotics for systemic use | 3.00 | 2.79 | −6.96 | <0.001 | 13.36 | 15.54 | 16.33 | <0.001 | ||
| ICU DDD/100 Bed-Days | ICU DDD/100 Discharges | |||||||
|---|---|---|---|---|---|---|---|---|
| ATC Classification | 2019 | 2020 | Variation (%) | p | 2019 | 2020 | Variation (%) | p |
| J02AA01 Amphotericin B | 0.44 | 0.66 | 50.34 | <0.001 | 1.95 | 3.67 | 87.98 | <0.001 |
| J01GB06 Amikacin | 2.12 | 2.22 | 4.91 | 0.02 | 9.43 | 12.37 | 31.16 | <0.001 |
| J01CR02 Amoxicillin and beta-lactamase inhibitor | 12.94 | 9.13 | −29.42 | <0.001 | 57.58 | 50.81 | −11.76 | <0.001 |
| J02AX06 Anidulafungin | 1.93 | 1.95 | 1.40 | 0.52 | 8.57 | 10.86 | 26.77 | <0.001 |
| J01FA10 Azithromycin | 2.77 | 8.32 | 200.01 | <0.001 | 12.34 | 46.28 | 275.09 | <0.001 |
| J02AX04 Caspofungin | 0.38 | 0.45 | 20.13 | <0.001 | 1.68 | 2.52 | 50.18 | <0.001 |
| J01DE01 Cefepime | 1.20 | 1.98 | 65.04 | <0.001 | 5.35 | 11.03 | 106.35 | <0.001 |
| J01DI02 Ceftaroline fosamil | 0.43 | 0.31 | −28.21 | <0.001 | 1.91 | 1.71 | −10.25 | 0.03 |
| J01DD02 Ceftazidime | 2.28 | 2.20 | −3.89 | 0.05 | 10.17 | 12.21 | 20.16 | <0.001 |
| J01DD52 Ceftazidime and beta-lactamase inhibitor | 0.33 | 0.58 | 77.11 | <0.001 | 1.46 | 3.23 | 121.47 | <0.001 |
| J01DI54 Ceftolozane and beta-lactamase inhibitor | 0.44 | 0.88 | 98.22 | <0.001 | 1.97 | 4.89 | 147.81 | <0.001 |
| J01DD04 Ceftriaxone | 6.61 | 8.19 | 24.07 | <0.001 | 29.38 | 45.58 | 55.11 | <0.001 |
| J01MA02 Ciprofloxacin | 3.31 | 3.47 | 4.72 | 0.01 | 14.73 | 19.28 | 30.92 | <0.001 |
| J01CF02 Cloxacillin | 7.56 | 6.45 | −14.69 | <0.001 | 33.62 | 35.86 | 6.66 | <0.001 |
| J01XB01 Colistin | 1.17 | 1.64 | 40.27 | <0.001 | 5.20 | 9.11 | 75.36 | <0.001 |
| J01XA04 Dalbavancin | 0.00 | 0.00 | 57.14 | 0.68 | 0.00 | 0.01 | 96.67 | 0.53 |
| J01XX09 Daptomycin | 5.26 | 5.53 | 5.13 | <0.001 | 23.42 | 30.78 | 31.44 | <0.001 |
| J01DH03 Ertapenem | 1.45 | 1.27 | −12.83 | <0.001 | 6.46 | 7.04 | 8.99 | <0.001 |
| J02AC01 Fluconazole | 7.19 | 6.17 | −14.12 | <0.001 | 31.98 | 34.34 | 7.37 | <0.001 |
| J01DH51 Imipenem-cilastatin | 1.02 | 0.70 | −31.62 | <0.001 | 4.54 | 3.89 | −14.50 | <0.001 |
| J02AC05 Isavuconazole | 0.34 | 0.29 | −14.33 | <0.001 | 1.52 | 1.63 | 7.10 | 0.20 |
| J01XX08 Linezolid | 4.81 | 5.06 | 5.01 | <0.001 | 21.42 | 28.12 | 31.28 | <0.001 |
| J01DH02 Meropenem | 12.18 | 12.06 | −1.02 | 0.24 | 54.19 | 67.06 | 23.75 | <0.001 |
| J02AX05 Micafungin | 0.70 | 0.39 | −44.67 | <0.001 | 3.10 | 2.14 | −30.81 | <0.001 |
| J01CR05 Piperacillin and beta-lactamase inhibitor | 10.29 | 9.61 | −6.68 | <0.001 | 45.79 | 53.43 | 16.68 | <0.001 |
| J02AC04 Posaconazole | 0.25 | 0.09 | −63.53 | <0.001 | 1.12 | 0.51 | −54.39 | <0.001 |
| J01XA01 Vancomycin | 2.76 | 2.87 | 3.83 | 0.04 | 12.30 | 15.97 | 29.81 | <0.001 |
| J02AC03 Voriconazole | 1.12 | 1.76 | 56.92 | <0.001 | 4.99 | 9.80 | 96.17 | <0.001 |
| ICU DDD/100 Discharges | ||||
|---|---|---|---|---|
| Estimated 2020 Consumption | Observed 2020 Consumption | Variation (%) | Prediction Intervals | |
| J02AA01 Amphotericin B | 1.93 | 3.67 | 90.16 | [0.28 to 3.57] |
| J01GB06 Amikacin | 10.17 | 12.37 | 21.63 | [3 to 17.34] |
| J01CR02 Amoxicillin and beta-lactamase inhibitor | 54.96 | 50.81 | −7.55 | [43.43 to 66.49] |
| J02AX06 Anidulafungin | 9.64 | 10.86 | 12.66 | [6.77 to 12.52] |
| J01FA10 Azithromycin | 13.03 | 46.28 | 255.18 | [10.66 to 15.41] |
| J02AX04 Caspofungin | 1.14 | 2.52 | 121.05 | [0.05 to 2.23] |
| J01DE01 Cefepime | 7.02 | 11.03 | 57.12 | [2.84 to 11.19] |
| J01DD02 Ceftazidime | 11.22 | 12.21 | 8.82 | [7.28 to 15.16] |
| J01DD04 Ceftriaxone | 33.59 | 45.58 | 35.70 | [25.9 to 41.29] |
| J01MA02 Ciprofloxacin | 14.78 | 19.28 | 30.45 | [10.21 to 19.35] |
| J01CF02 Cloxacillin | 32.39 | 35.86 | 10.71 | [27.45 to 37.33] |
| J01XB01 Colistin | 8.65 | 9.11 | 5.32 | [0.98 to 16.32] |
| J01XX09 Daptomycin | 27.08 | 30.78 | 13.66 | [18.92 to 35.24] |
| J01DH03 Ertapenem | 7.46 | 7.04 | −5.63 | [6.05 to 8.88] |
| J02AC01 Fluconazole | 37.17 | 34.34 | −7.61 | [20.93 to 53.4] |
| J01DH51 Imipenem-cilastatin | 0.0 | 3.89 | NA | [−5.22 to 5.01] |
| J01XX08 Linezolid | 26.73 | 28.12 | 5.20 | [18.44 to 35.03] |
| J01DH02 Meropenem | 66.79 | 67.06 | 0.40 | [51.71 to 81.87] |
| J02AX05 Micafungin | 4.93 | 2.14 | −56.59 | [1.28 to 8.58] |
| J01CR05 Piperacillin and beta-lactamase inhibitor | 46.21 | 53.43 | 15.62 | [32.52 to 59.9] |
| J02AC04 Posaconazole | 1.17 | 0.51 | −56.41 | [−0.23 to 2.57] |
| J01XA01 Vancomycin | 11.32 | 15.97 | 41.08 | [7.97 to 14.67] |
| J02AC03 Voriconazole | 6.65 | 9.80 | 47.37 | [4.03 to 9.27] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grau, S.; Hernández, S.; Echeverría-Esnal, D.; Almendral, A.; Ferrer, R.; Limón, E.; Horcajada, J.P.; on behalf of the Catalan Infection Control Antimicrobial Stewardship Program (VINCat-PROA). Antimicrobial Consumption among 66 Acute Care Hospitals in Catalonia: Impact of the COVID-19 Pandemic. Antibiotics 2021, 10, 943. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10080943
Grau S, Hernández S, Echeverría-Esnal D, Almendral A, Ferrer R, Limón E, Horcajada JP, on behalf of the Catalan Infection Control Antimicrobial Stewardship Program (VINCat-PROA). Antimicrobial Consumption among 66 Acute Care Hospitals in Catalonia: Impact of the COVID-19 Pandemic. Antibiotics. 2021; 10(8):943. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10080943
Chicago/Turabian StyleGrau, Santiago, Sergi Hernández, Daniel Echeverría-Esnal, Alexander Almendral, Ricard Ferrer, Enric Limón, Juan Pablo Horcajada, and on behalf of the Catalan Infection Control Antimicrobial Stewardship Program (VINCat-PROA). 2021. "Antimicrobial Consumption among 66 Acute Care Hospitals in Catalonia: Impact of the COVID-19 Pandemic" Antibiotics 10, no. 8: 943. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10080943