
Prevalence and Antibiotic Resistance Profile of Bacterial Pathogens in Aerobic Vaginitis: A Retrospective Study in Italy

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Incidence of AV Positive and Age Patient Distribution
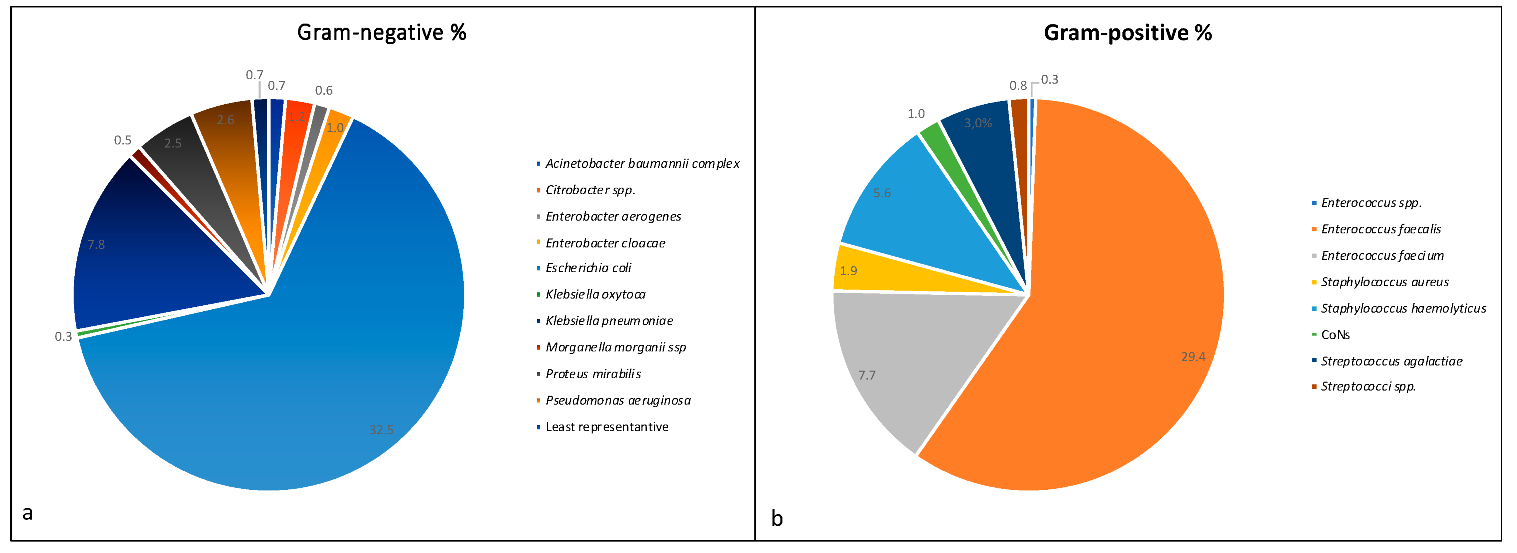
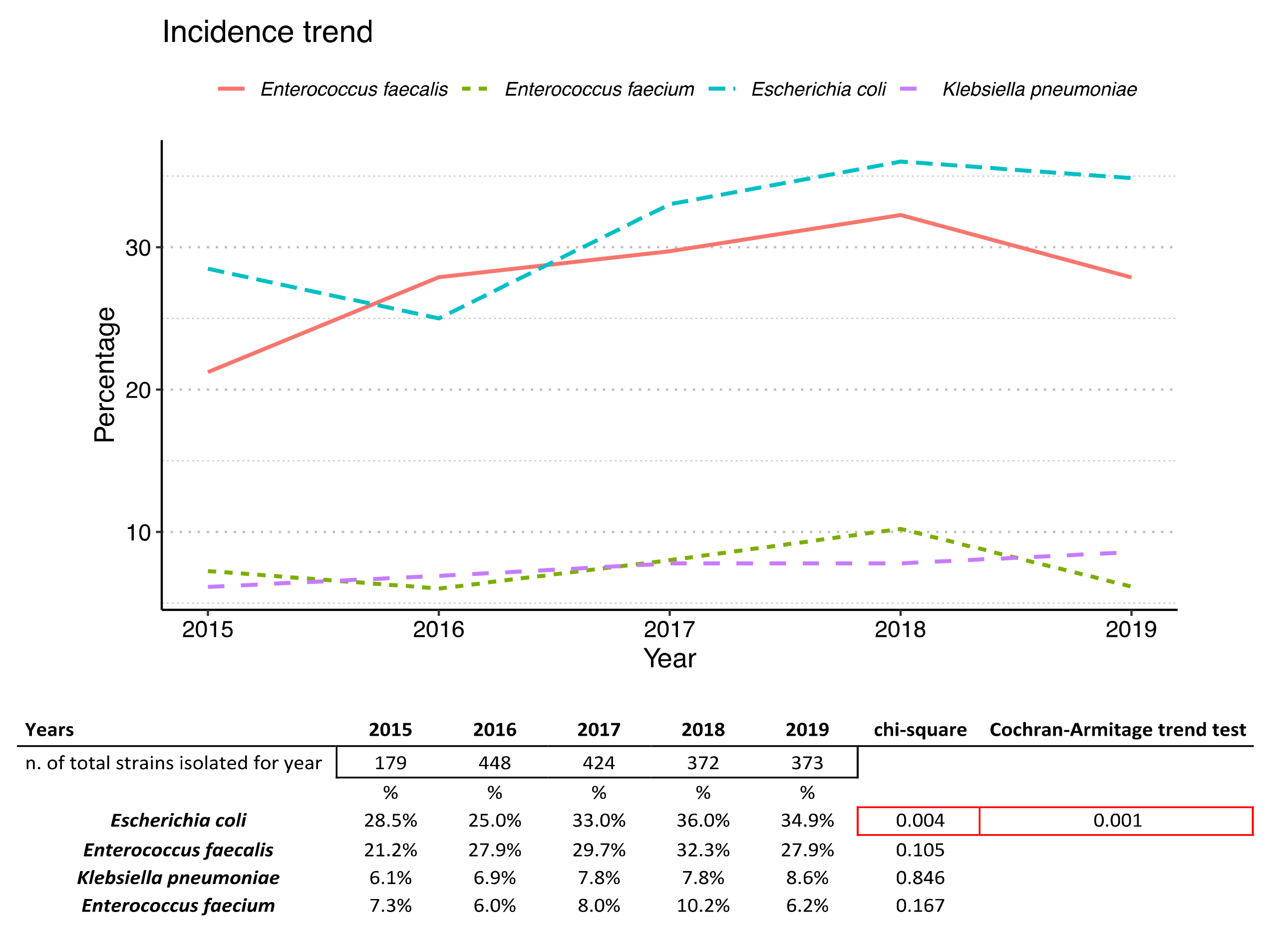
2.2. Prevalence of Isolated Bacteria
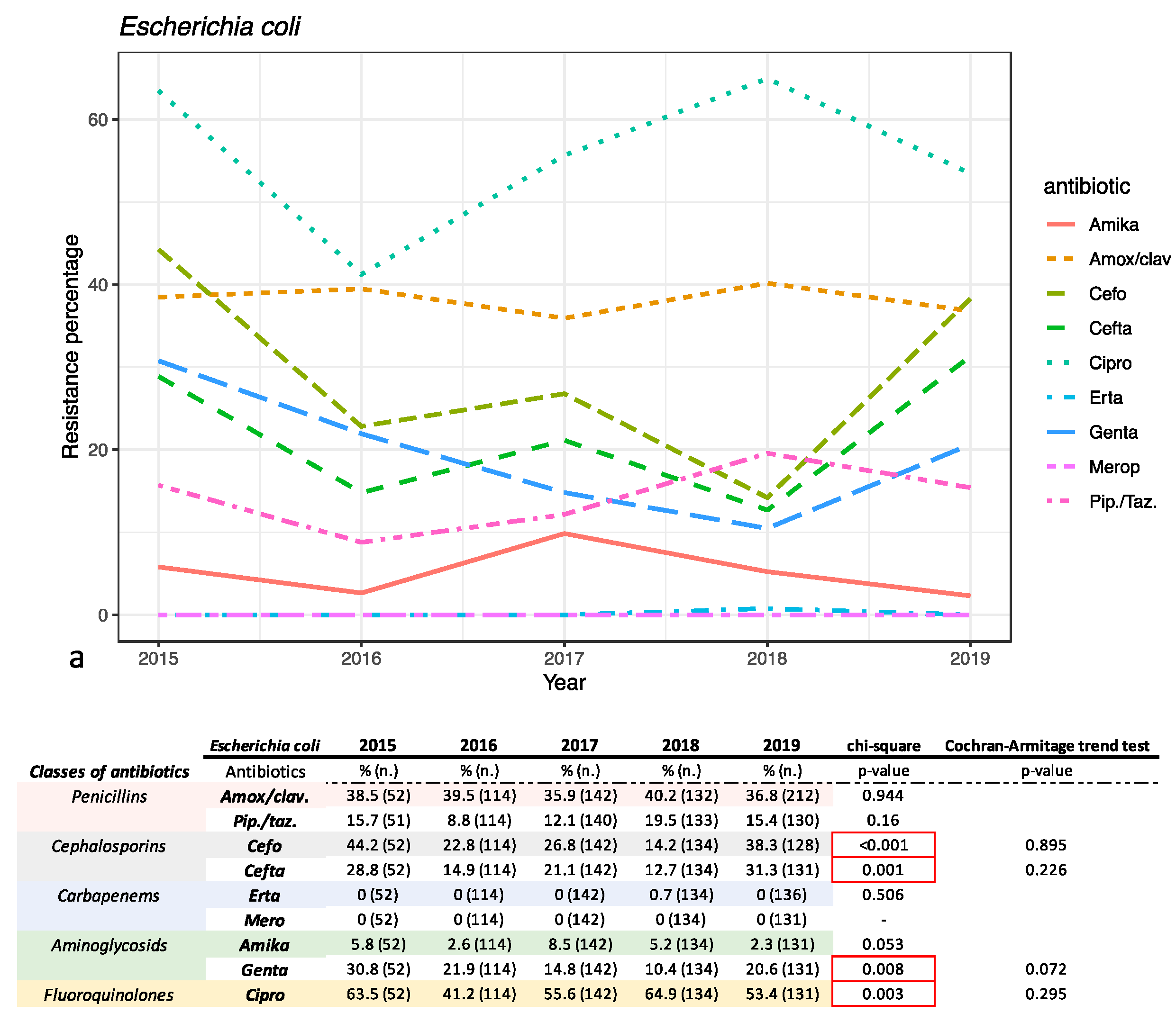
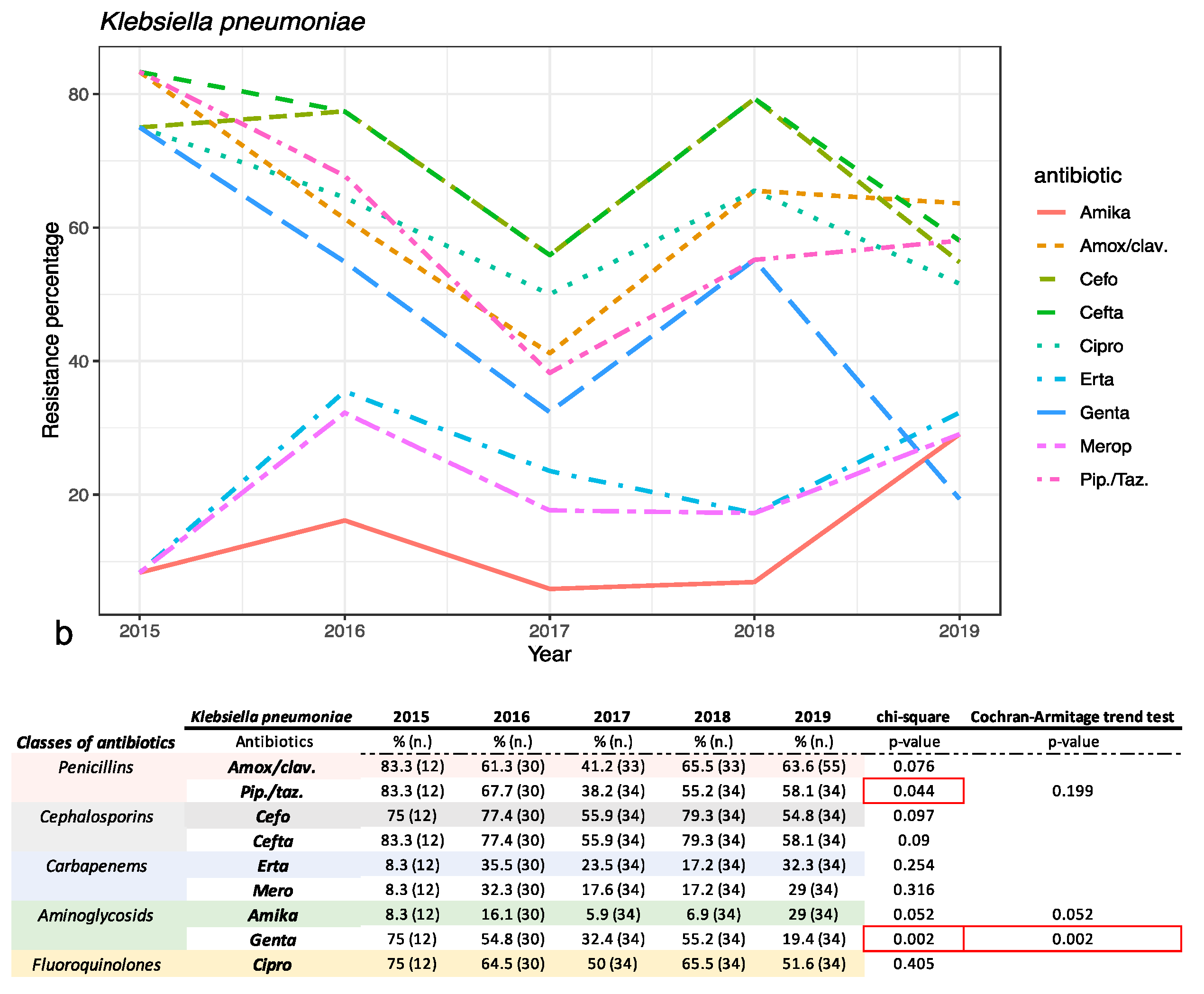
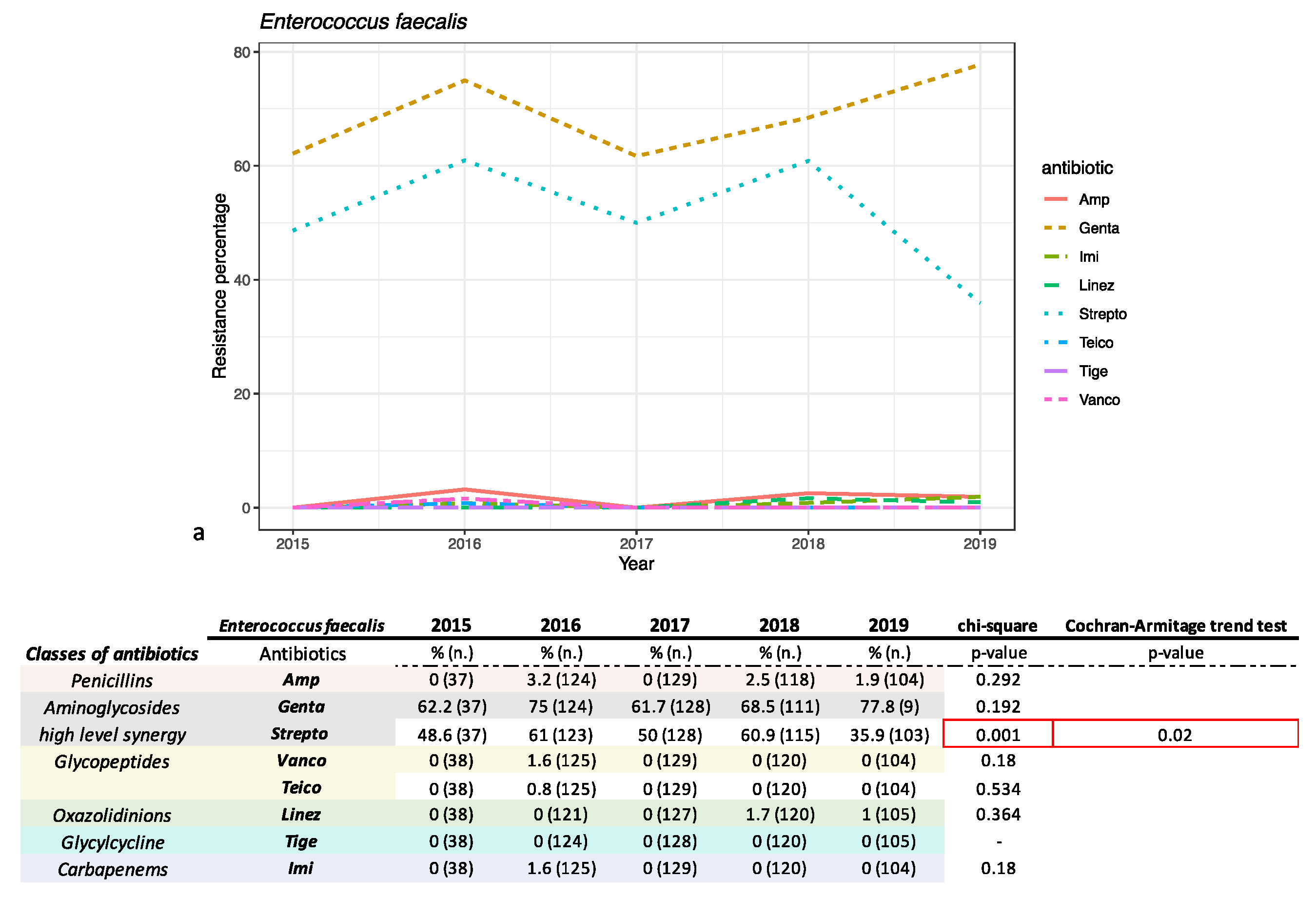
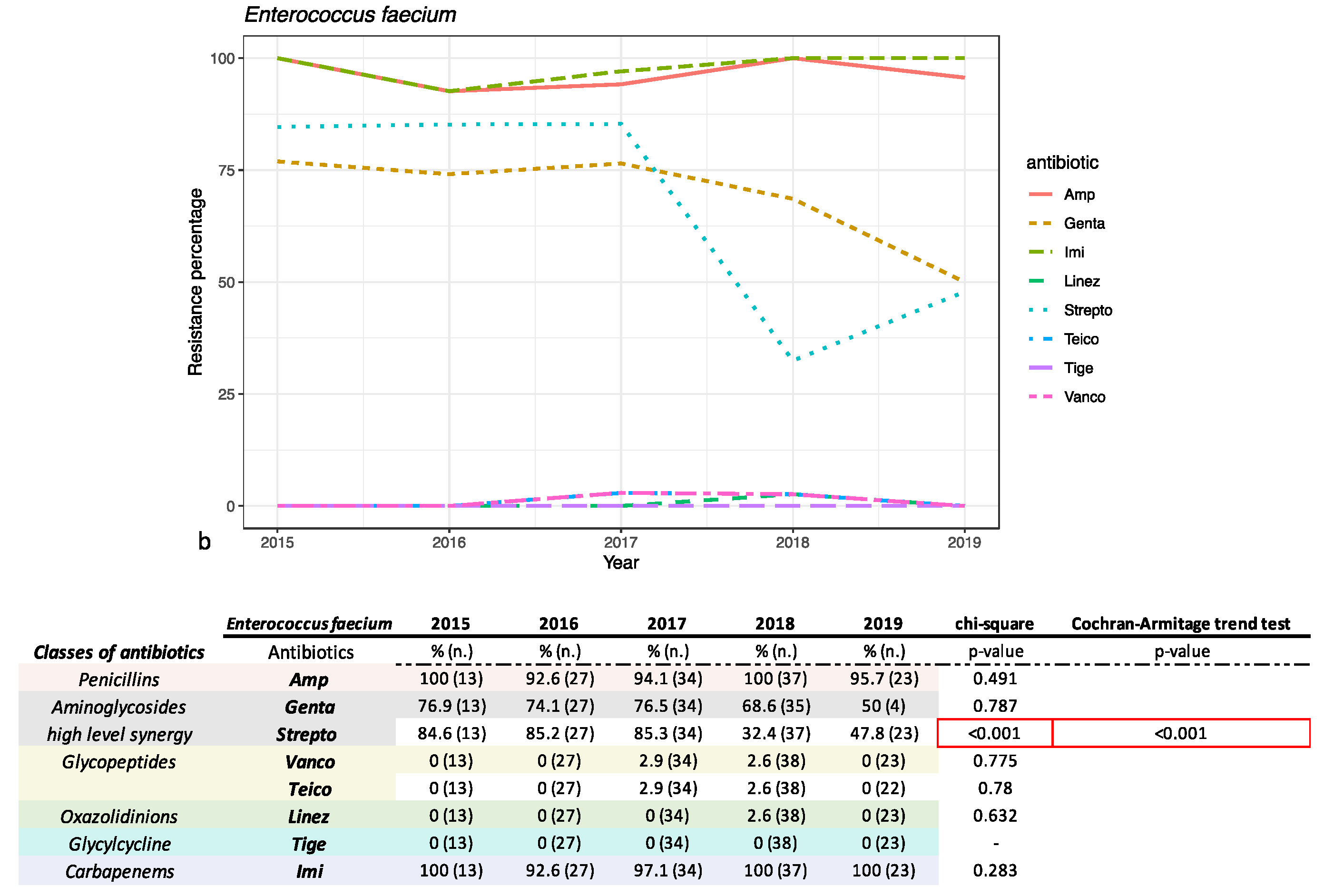
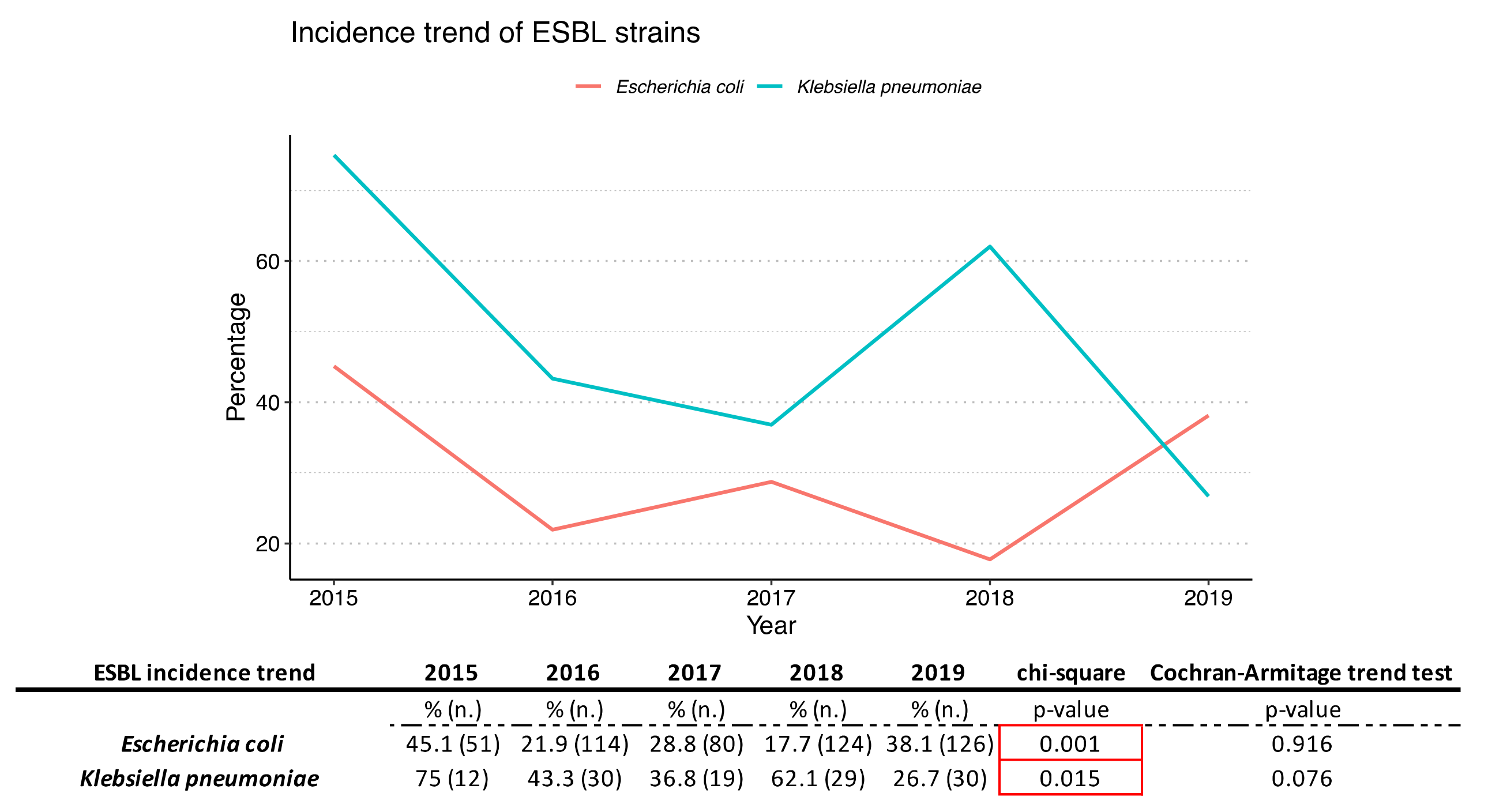
2.3. Antimicrobial Susceptibility Pattern
3. Discussion
4. Materials and Methods
4.1. Samples Collection
4.2. Inclusion and Exclusion Criteria
4.3. Bacterial Culture
4.4. Bacterial Identification and Antibiotic Susceptibility Test
4.5. Data Analysis
4.5.1. Ethical Consideration Statement
4.5.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vásquez, A.; Jakobsson, T. Vaginal lactobacillus flora of healthy Swedish women. J. Clin. Microbiol. 2002, 40, 2746–2749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravel, J.; Gajer, P. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108, 4680–4687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltani, S.; Hammami, R. Bacteriocins as a new generation of antimicrobials: Toxicity aspects and regulations. FEMS Microbiol. Rev. 2021, 45, fuaa039. [Google Scholar] [CrossRef]
- Plisko, O.; Zodzika, J. Aerobic Vaginitis-Underestimated Risk Factor for Cervical Intraepithelial Neoplasia. Diagnostics 2021, 11, 97. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Bellen, G. Aerobic vaginitis: No longer a stranger. Res. Microbiol. 2017, 168, 845–858. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Pinto, F. Isolation, characterization and analysis of pro-inflammatory potential of Klebsiella pneumoniae outer membrane vesicles. Microb. Pathog. 2019, 136, 103719. [Google Scholar] [CrossRef]
- Sangeetha, K.T.; Saroj, G. A study of aerobic bacterial pathogens associated with vaginitis in reproductive age group women (15–45 years) and their sensitivity pattern. IJRMS 2015, 3, 2268–2273. [Google Scholar]
- Vidyasagar, V. Estimation of incidence of Aerobic vaginitis in women presenting with symptoms of vaginitis. Indian J. Obstet. Gynecol. Res. 2021, 8, 82–85. [Google Scholar] [CrossRef]
- Kaambo, E.; Africa, C. Vaginal Microbiomes Associated with Aerobic Vaginitis and Bacterial Vaginosis. Front. Public Health 2018, 6, 78. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Vereecken, A. Definition of a type of abnormal vaginal flora that is distinct from bacterial vaginosis: Aerobic vaginitis. BJOG 2002, 109, 34–43. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Bellen, G. Aerobic vaginitis in pregnancy. BJOG 2011, 118, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Tansarli, G.S.; Kostaras, E.K. Prevalence and treatment of aerobic vaginitis among non-pregnant women: Evaluation of the evidence for an underestimated clinical entity. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Larsen, B.; Monif, G.R. Understanding the bacterial flora of the female genital tract. Clin. Infect. Dis. 2001, 32, e69–e77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, C.; Wu, W. Diagnostic and therapeutic advancements for aerobic vaginitis. Arch. Gynecol. Obstet. 2015, 291, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Kaambo, E.; Africa, C.W.J. The threat of aerobic vaginitis to pregnancy and neonatal morbidity. Afr. J. Reprod. Health 2017, 21, 109. [Google Scholar] [CrossRef] [Green Version]
- Sianou, A.; Galyfos, G. Prevalence of vaginitis in different age groups among females in Greece. J. Obstet. Gynaecol. 2017, 37, 790–794. [Google Scholar] [CrossRef]
- Nahar, D.; Soni, G. Bacterial Etiology and their antibiogram in aerobic vaginitis patients at tertiary care hospital. Int. J. Sci. Study 2016, 4, 103–110. [Google Scholar]
- Zarbo, G.; Coco, L. Aerobic Vaginitis during Pregnancy. Res. Obstet. Gynecol. 2013, 2, 7–11. [Google Scholar]
- Gajdács, M.; Urbán, E. Epidemiology and resistance trends of Staphylococcus aureus isolated from vaginal samples: A 10-year retrospective study in Hungary. Acta Dermatovenerol. Alp. Pannonica Adriat. 2019, 28, 143–147. [Google Scholar] [CrossRef] [Green Version]
- Wójkowska-Mach, J.; Pomorska-Wesołowska, M. Prevalence and Antimicrobial Susceptibility Profiles of Microorganisms Associated with Lower Reproductive Tract Infections in Women from Southern Poland-Retrospective Laboratory-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 335. [Google Scholar] [CrossRef]
- Petrillo, P.; Pignataro, D. Current Evidence on the Ocular Surface Microbiota and Related Diseases. Microorganisms 2020, 13, 1033. [Google Scholar] [CrossRef]
- Instituto Superiore di Sanita. Rapporto AR-ISS—I dati. 2019. Available online: www.epicentro.iss.it/antibiotico-resistenza/ar-iss-rapporto (accessed on 11 August 2021).
- Tempera, G.; Furneri, P.M. Management of aerobic vaginitis. Gynecol. Obstet. Investig. 2010, 70, 244–249. [Google Scholar] [CrossRef]
- Dell’Annunziata, F.; Ilisso, C.P. Outer Membrane Vesicles Derived from Klebsiella pneumoniae Influence the miRNA Expression Profile in Human Bronchial Epithelial BEAS-2B Cells. Microorganisms 2020, 8, 1985. [Google Scholar] [CrossRef] [PubMed]
- Tempera, G.; Abbadessa, G. Topical kanamycin: An effective therapeutic option in aerobic vaginitis. J. Chemother. 2006, 18, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Foessleitner, P.; Gasser, J. Vaginal colonization of extended-spectrum beta-lactamase-producing bacteria during pregnancy: An observational study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 246, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Buonocore, C.; Tedesco, P. Characterization of a New Mixture of Mono-Rhamnolipids Produced by Pseudomonas gessardii Isolated from Edmonson Point (Antarctica). Mar. Drugs 2020, 20, 269. [Google Scholar] [CrossRef]
- Kim, Y.A.; Lee, K. Risk factors and molecular features of sequence type (ST) 131 extended-Spectrum-β-lactamase-producing Escherichia coli in community-onset female genital tract infections. BMC Infect. Dis. 2018, 18, 250. [Google Scholar] [CrossRef]
- IBM. IBM SPSS Statistics. Available online: www.spss.com (accessed on 11 August 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Samples (n.) | 2015 | 2016 | 2017 | 2018 | 2019 | 2015–2019 | Incidence % |
|---|---|---|---|---|---|---|---|
| Positive samples | 117 | 286 | 275 | 234 | 264 | 1176 | 56.8% |
| Negative samples | 118 | 188 | 203 | 163 | 221 | 893 | 43.2% |
| Total samples | 235 | 474 | 478 | 397 | 485 | 2069 |
| Age Group | % of Incidence |
|---|---|
| 10–14 | 0.6% |
| 15–24 | 7.2% |
| 25–34 | 15.2% |
| 35–44 | 17.9% |
| 45–54 | 14.1% |
| 55–64 | 26.5% |
| 65–80 | 15.0% |
| 81–95 | 3.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serretiello, E.; Santella, B.; Folliero, V.; Iervolino, D.; Santoro, E.; Manente, R.; Dell’Annunziata, F.; Sperlongano, R.; Crudele, V.; De Filippis, A.; et al. Prevalence and Antibiotic Resistance Profile of Bacterial Pathogens in Aerobic Vaginitis: A Retrospective Study in Italy. Antibiotics 2021, 10, 1133. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091133
Serretiello E, Santella B, Folliero V, Iervolino D, Santoro E, Manente R, Dell’Annunziata F, Sperlongano R, Crudele V, De Filippis A, et al. Prevalence and Antibiotic Resistance Profile of Bacterial Pathogens in Aerobic Vaginitis: A Retrospective Study in Italy. Antibiotics. 2021; 10(9):1133. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091133
Chicago/Turabian StyleSerretiello, Enrica, Biagio Santella, Veronica Folliero, Domenico Iervolino, Emanuela Santoro, Roberta Manente, Federica Dell’Annunziata, Rossella Sperlongano, Valeria Crudele, Anna De Filippis, and et al. 2021. "Prevalence and Antibiotic Resistance Profile of Bacterial Pathogens in Aerobic Vaginitis: A Retrospective Study in Italy" Antibiotics 10, no. 9: 1133. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091133