
Detection of Multidrug-Resistant Enterobacterales—From ESBLs to Carbapenemases


1
Department of Medical Microbiology and Virology, Carl von Ossietzky University Oldenburg, 26129 Oldenburg, Germany
2
Institute for Medical Microbiology and Virology, Klinikum Oldenburg, 26133 Oldenburg, Germany
3
Institute for Medical Microbiology, Immunology and Hygiene, University Hospital, University of Cologne, 50935 Cologne, Germany
4
German Centre for Infection Research, Partner Site Bonn-Cologne, 50937 Cologne, Germany
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Antibiotics 2021, 10(9), 1140; https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091140
Submission received: 12 August 2021
/
Revised: 3 September 2021
/
Accepted: 10 September 2021
/
Published: 21 September 2021
(This article belongs to the Special Issue Carriage of Multiple Drug Resistant (MDR) Bacteria in Health)
Abstract
:Multidrug-resistant Enterobacterales (MDRE) are an emerging threat to global health, leading to rising health care costs, morbidity and mortality. Multidrug-resistance is commonly caused by different β-lactamases (e.g., ESBLs and carbapenemases), sometimes in combination with other resistance mechanisms (e.g., porin loss, efflux). The continuous spread of MDRE among patients in hospital settings and the healthy population require adjustments in healthcare management and routine diagnostics. Rapid and reliable detection of MDRE infections as well as gastrointestinal colonization is key to guide therapy and infection control measures. However, proper implementation of these strategies requires diagnostic methods with short time-to-result, high sensitivity and specificity. Therefore, research on new techniques and improvement of already established protocols is inevitable. In this review, current methods for detection of MDRE are summarized with focus on culture based and molecular techniques, which are useful for the clinical microbiology laboratory.
1. Intestinal Colonization by Multidrug-Resistant Bacteria and the Impact on Global Health
The dissemination of multidrug-resistant (MDR) bacteria is one of the biggest threats to global health [1,2]. In particular, multidrug-resistant Enterobacterales (MDRE) are a major cause of hospital-acquired infections, which are associated with high morbidity and mortality as well as rising healthcare costs [3,4,5]. On the other hand, Enterobacterales as well as MDRE are part of the normal intestinal microbiota of healthy individuals [6]. The majority of microorganisms in human feces are anaerobic bacteria, but Enterobacterales, which account for only 0.01% of 1013–1014 organisms, are those mainly associated with antibiotic resistance [7].
Colonization-rates with MDRE in healthy adults are mostly studied for extended spectrum β-lactamase (ESBL) and AmpC producing Enterobacterales. Great variations are observed in different regions, with lower rates in some European countries like Hungary (2.6%) and Sweden (7%) and higher rates in countries like Nepal (9.8%), Mozambique (20%) and Taiwan (41.4%) [8,9,10,11,12]. The main risk factors for new colonization with MDRE among the healthy population are travel to high incidence countries and antibiotic use [9,13]. Risk factors for colonization with MDRE upon hospital admission are previous MDR carriage, travel outside Europe and treatment of gastroesophageal reflux disease and in particular antibiotic treatment within the previous six months [14]. Prevalence of colonization is higher among elderly people in long term care facilities, reflecting antibiotic use, chronic wounds, medical devices, dementia and age as important risk factors. As seen in healthy adults, colonization-rates are highest in Asia with 71.6% for ESBL—producing Enterobacterales (ESBLE) and 6.9% for carbapenemase—producing Enterobacterales (CPE). In North America, Europe and Oceania, prevalence is 9%, 12.9% and 6% for ESBLE and 5%, 0.2% and 0.4% for CPE, respectively [15]. The prevalence of CPE can vary substantially between different countries on the same continent [16]. In Germany, low CPE prevalence in intensive care units (ICU) has been reported [17], whereas in other European countries like Romania and Italy, CPE are frequently isolated in ICU patients or long-term acute-care facilities with reports of colonization-rates as high as 21.2% and 28.4%, respectively [18,19].
Among MDR pathogens, WHO has declared carbapenem- and 3rd generation cephalosporin-resistant Enterobacterales as the highest priority for the development of new antibiotics [20]. Surveillance data from the European Centre of Disease Prevention and Control (ECDC) show that the rate of E. coli clinical isolates resistant to 3rd generation cephalosporins has been increasing in European countries since 2015 and ranged from 6.2% in Norway to 38.6% in Bulgaria in 2019. Even higher rates have been observed in Klebsiella pneumoniae (4.3–75.7%). In parallel, the proportion of E. coli and K. pneumoniae with resistance to carbapenems increased sharply by 2019 (range 0–1.6% and 0–58.3% for E. coli and K. pneumoniae, respectively). The prevalence of E. coli and K. pneumoniae isolates resistant to carbapenems or 3rd generation cephalosporins varies widely among EU/EEA countries, with the overall highest resistance rates being reported from Italy, Bulgaria, Greece and Romania [21].
Resistance to 3rd generation cephalosporins and carbapenems is mostly caused by different β-lactamases, with >7000 different β-lactamases known, and more being published almost daily, illustrating the high mutation and adaptation frequency in different bacteria [22]. β-lactamases are classified according to Ambler (classes A to D) based on primary sequence similarities or according to Bush–Jacoby–Medeiros (group 1 to 3), which is a functional classification depending on biochemical function and susceptibility towards β-lactamase inhibitors [23,24]. Group 1 summarizes all cephalosporinases (Ambler class C) that were originally chromosomally encoded. Group 2 includes all other serine β-lactamases and is composed of several subgroups (Ambler classes A and D). Finally, group 3 combines all metallo-β-lactamases (MBLs, Ambler class B) [24].
Extended-spectrum β-lactamases (ESBLs) have been increasingly detected in hospitalized patients and the community since the 1980s and are of great clinical importance. These enzymes are capable of hydrolyzing penicillins, monobactams and 3rd generation cephalosporins. ESBLs belong to Ambler classes A and D in most cases, with those in Ambler class A being mostly sensitive to inhibitors such as clavulanic acid [23]. Relevant examples for β-lactamases in Enterobacterales in each class are shown in Figure 1. Comprehensive details on ESBL-types are beyond the scope of this article but have been excellently reviewed elsewhere [23,24,25].
Infections with ESBL-harboring bacteria have been successfully treated with carbapenems, but the massive use of this antibiotic class accelerated the dissemination of the second important group of β-lactamases, the carbapenemases. These enzymes belong to Ambler classes A, B and D and differ in the resistance pattern they induce [26]. Class A includes serine β-lactamases such as Klebsiella pneumoniae carbapenemase (KPC-2) [27,28], non-metallo carbapenemase (NMC) [29], imipenemase (IMI) [30] and others. Class B carbapenems are metallo-proteins and are capable of hydrolyzing all antibiotics except monobactams [24]. Well-known examples include NDM-1 [31], VIM [32] and IMP [33]. Oxacillinases and OXA-48 derivates are classified as class D carbapenemases. Their hydrolytic activity against carbapenems and some 3rd generation cephalosporins is lower compared to other carbapenemases, and they are not inhibited by clavulanic acid and tazobactam [34].
With the increasing use of antibiotics, the further emergence of MDR Enterobacterales seems inevitable. High consumption of antibiotics in health care and livestock as well as increased mobility represent only two accelerators in the process, which is accompanied by an ongoing evolution of resistance plasmids and mobile genetic elements [35,36]. Nevertheless, several intervention strategies are planned or already implemented to reduce the dissemination of MDRE, i.e., by improved infection control, antimicrobial stewardship programs and by decreasing carbapenem use, e.g., by β-lactam-lactamase-inhibitor combinations [37]. In addition, improved detection of MDRE isolates allows rapid isolation of patients colonized or infected with these organisms and may enable a specific antibiotic therapy after determination of the susceptibility patterns. Both steps can reduce spread of resistances, e.g., in hospital settings. However, not only rapid and sensitive detection methods but also pre-analytical parameters affect results and final treatment success.
2. Detection and Characterization of MDR Enterobacterales
2.1. Preanalytical Considerations
Every clinical laboratory must be able to reliably detect MDR bacteria and provide regular reports on the epidemiology of MDRE in order to guide infection control measures. This baseline epidemiological monitoring uses data from clinical samples in most institutions. For high-risk patients, in outbreak situations and in the epidemic setting, the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) as well as the Healthcare Infection Control Practices Advisory Committee and Center for Diseases Control and Prevention (HICPAC/CDC) guidelines recommend active screening cultures (ASC) for the detection of colonization with MDRE, especially for carbapenemase-producing Enterobacterales (CPE) [38,39].
An often-overlooked issue which impacts the sensitivity of microbiological cultures and in particular ASC are preanalytical factors including appropriate specimens, the collection site as well as the collection device. Stool is considered the gold standard specimen for studying gastrointestinal microbiota and detection of MDRE colonization [40]. Because of the inconvenient sample collection and processing of stool samples, rectal or perianal swabs are the specimen most commonly used for ASC. The ESCMID guideline for the management of multidrug-resistant Gram-negative bacteria (GNB) considers rectal swabs, urine or respiratory secretions as adequate specimen [38]. The HICPAC/CDC guidelines additionally recommend sampling skin lesions, wounds and sputum or endotracheal aspirates, if colonization of the respiratory tract is suspected [39,41]. In a recent study on colonization sites, it has been shown that 14% of ESBL-GNB carriers are not detected by rectal sampling but by sampling of other sites (e.g., urogenital or respiratory). The authors highlight the need to include samples from the site where MDR-GNB were initially detected for follow-up cultures [42]. For the assessment of gastrointestinal colonization, rectal swabs are preferred over perianal swabs as they recover significantly higher quantities of GNB and have a higher sensitivity for the detection of MDRE [43,44]. Additionally, collection devices have an impact on bacterial recovery: Warnke and colleagues tested nylon-flocked, polyurethan-cellular-foam and classic rayon tip swabs for intra-anal and perianal swabbing. The nylon-flocked and polyurethan-cellular-foam tip swabs recovered significantly higher bacterial loads compared to other swabs, thereby increasing sensitivity for MDRE screening [43].
2.2. Culture Based Methods
2.2.1. Screening with Selective Chromogenic and Non-Chromogenic Media
Selective media are suitable for screening of patient samples for ESBL- and carbapenemase-producing Enterobacterales. Frequently, agars are supplemented with chromogens which allow presumptive species identification using species-specific enzymes, namely, β-galactosidase, β-glucuronidase and deaminase [45].
Several agars are available for ESBL detection, including CHROMagar ESBL (CHROMagar, Paris, France), chromID ESBL agar (bioMérieux, I’Etoile, France), ESBL chromogenic agar (Condalab, Madrid, Spain), chromogenic ESBL agar (SGL, Corby, UK), ESBL ChromoSelect Agar (Merck, Darmstadt, Germany), CHROMagar TM ESBL (Mast Group, Bootle, UK), Chromatic ESBL agar (Liofilchem, Roseto degli Abruzzi, Italy), Brilliance ESBL agar (Oxoid, Basingstoke, UK), BLSE agar (AES Laboratoire, Combourg, France), and others (Table 1). Most chromogenic ESBL screening agars contain an extended-spectrum cephalosporin (e.g., cefpodoxim) and a mixture of antibiotics to inhibit growth of non-ESBL-producing bacteria. Some agars (i.e., CHROMagar ESBL, chromID ESBL and Brilliance ESBL) also contain additional AmpC-inhibitors [45].
Many of these products have been evaluated in different studies. ChromID ESBL agar (bioMérieux, Marcy-I’Etoile, France) and BLSE agar medium (AES Laboratoire, Combourg, France) were challenged with various Enterobacterales from clinical samples (rectal swabs, urine samples and pulmonary aspirates). After 24 h, incubation sensitivity was 88% and 85% for chromID and BLSE agar, respectively. Further 24 h incubation increased sensitivity of chromID to 94% but did not affect performance of BLSE agar. The reason for these differences was likely the choice of cefpodoxime in chromID ESBL but cefotaxime or ceftazidime in BLSE agar. False-positive results were obtained for isolates overproducing a chromosomal cephalosporinase or penicillinase [98]. Sensitivity values comparable to ChromID ESBL were obtained with Brilliance ESBL agar (Oxoid, Basingstoke, UK) [99]. Comparison of CHROMagar, chromID, Brilliance ESBL and BD Drigalski supplemented with ceftazidime demonstrated that sensitivity for ESBL detection ranged from 97.2% to 98.6% (CHROMagar 98.3%, ChromID 97.5%, Brilliance ESBL 98.6%, BD Drigalski 97.2%) and specificity from 57.9% (Brilliance ESBL) to 72.9% (chromID) [100].
In additional to ESBL agars, chromogenic agars for the detection of CPE have become commercially available in the last decade. In a recent study, seven commercially available screening media and in-house agars were investigated [47]. The authors challenged Brilliance CRE (Oxoid, Basingstoke, UK), Chromatic CRE (Liofilchem, Roseto degli Abruzzi, Italy), chromID CARBA and chromID OXA-48 (bioMérieux, Marcy-I’Etoile, France) and McConkey agar supplemented with ertapenem and cloxacillin with a total of 69 carbapenemase-producing isolates and 40 control strains without carbapenemase-production. In addition, three ESBL agars were assessed for CPE detection, namely Chromatic ESBL (Liofilchem, Roseto degli Abruzzi, Italy), chromID ESBL (bioMérieux, Marcy-I’Etoile, France) and Brilliance ESBL (Oxoid, Basingstoke, UK). The authors demonstrated that ESBL screening media are not suitable for detection of OXA-48-like-producing Enterobacterales with low cephalosporin MICs. High specificity and sensitivity for CPE detection was recorded for Brilliance CRE and the in-house agars, whereas chromID CARBA failed to detect 15% of all CPE and 8/20 OXA-48-producing isolates. Because detection of OXA-48-producing Enterobacterales is difficult, the use of the specific chromID OXA-48 agar is beneficial according to the authors, especially in outbreaks of OXA-48 CPE [45]. The results are partly comparable to a study by Simner et al. [48]. Again, the authors demonstrated that CPE detection using ESBL screening media is not useful due to reduced sensitivity and specificity (tested for Colorex C3Gr (EO Labs, Bonnybridge, Scotland) and Brilliance ESBL). In contrast to the previously mentioned study, the authors determined the highest sensitivity and specificity for chromID CARBA, followed by Colorex KPC (EO Labs, Bonnybridge, Scotland) and Brilliance CRE but showed also poorer detection of OXA-48 producers [48] (Table 1).
Pre-enrichment of screening cultures has been proposed as an additional means to increase the sensitivity of MDRE detection. An unselective or semi-selective broth (e.g., MacConkey broth or tryptic soy broth ± antibiotics) is inoculated with the screening sample and incubated overnight before an aliquot is spread on a selective agar. In several studies, pre-enrichment enhanced the detection rate of ESBL or 3rd generation cephalosporin resistant Enterobacterales by 21% to 32% [40,101,102,103]. For surveillance studies and in outbreak situations, the improved performance is advantageous. However, this technique is labor-intensive and increases the turn-around-time (TAT) by one day.
Obviously, the performance of the different chromogenic screening media may vary depending on the type of β-lactamase and the analyzed organism. Therefore, the proper choice of chromogenic agar must be adapted to the specific objectives and the epidemiological landscape of each medical center. While the ease of use and experience in the microbiology laboratories are good arguments in favor of chromogenic agar, this technique has some drawbacks. These include a relatively high frequency of unspecific growth on the plates resulting in considerable subsequent work-up, problems in the detection of some β-lactamases (e.g., OXA-48-like) and lack of information on the type of β-lactamase present. Therefore, additional work-up is required to assess susceptibility and identify the ESBL or carbapenemase variant.
2.2.2. Susceptibility Testing of MDRE
Susceptibility can be assessed by various assays, e.g., disc diffusion according to EUCAST or CLSI, semi-automated susceptibility with commercial assays (e.g., Vitek2 (bioMérieux, Marcy-I’Etoile, France), Phoenix (BD Diagnostics, Sparks, MD, USA) or WalkAway (Beckman-Coulter, Brea, CA, USA)) or broth microdilution.
The sensitivity and specificity of commercially available semi-automatic systems varies widely for detection of ESBLs and carbapenemases [104,105,106,107,108,109]. Screening cut-offs have been defined by EUCAST for isolates, which should be further characterized for ESBL- or carbapenemase production [110].
2.2.3. Confirmation Tests
If the results of susceptibility testing show an ESBL- or CPE-phenotype, confirmation tests are necessary to rule out resistance by other mechanisms (e.g., porin loss in combination with other β-lactamases). A great variety of confirmation tests are available, differing in performance, costs and TAT (Table 1).
2.2.4. Disc Diffusion Assays for Detection of ESBL and Carbapenemase Production
In disc diffusion assays, an antibiotics disc is placed on an agar plate inoculated with the test strains. If the test strain is susceptible to the antibiotic, a growth inhibition zone becomes visible after incubation (Figure 2A). For confirmation of screening results and identification of underlying resistance mechanisms, inhibitor-based disc tests are commonly performed, which are distinguished as double-disc synergy test (DDST) and combined disc test (CDT). In the latter assay, a disc containing an antibiotic and a disc containing the antibiotic and a β-lactamase inhibitor are used. If inhibition diameters are increased by the inhibitor by a certain threshold (e.g., 5 mm for CLSI ESBL test) or more or have a 50% change in zone diameter, ESBL production is indicated [111] (Figure 2C). In contrast, in DDST assays, antibiotic and inhibitor are separated in two individual discs which are placed close to each other (also called disc approximation test, Figure 2D). If a β-lactamase is present, an enlargement of the inhibition zones between the two discs is observed. For ESBL detection, cephalosporins and clavulanate are most often employed [112].
Similarly, inhibitor-based tests can be used for carbapenemase identification. Carbapenemase inhibitors include boronic acid derivates (KPC and Ambler class A carbapenemase and AmpC β-lactamase inhibition), cloxacillin (AmpC inhibition) and zinc chelators such as EDTA and dipicolinic acid (MBL inhibition) [113,114,115]. OXA-48-like producers are difficult to identify by disc tests as there is no specific inhibitor available for class D carbapenemases. As a work-around, resistance to temocillin and piperacillin-tazobactam can be used as an indicator but is not specific for OXA-48-like [116,117].
The faropenem disc test is a highly sensitive screening method for CPE [50,118]. While most CPE show no inhibition zone around the faropenem disc, OXA-48-like Enterobacterales often have a double inhibition zone, which is highly specific. The combination of temocillin and faropenem discs increases specificity for OXA-48-like carbapenemase-producing Enterobacterales [119].
Both CDT and DDST assays are commercially available for screening ESBL- and carbapenemase-producing Enterobacterales. Examples of ESBL tests are Liofilchem ESBL disc kits (Liofilchem, Roseto degli Abruzzi, Italy) and Mastdiscs ESBL detection set (MAST Group, Bootle, UK), while tests for carbapenemase detection are more numerous and include Mastdiscs Carbapenemase Detection Set, Combi Carba Plus (both MAST Group), KPC/MBL & OXA-48 Confirm Kits (Rosco Diagnostica, Taastrup, Denmark) and KPC&MBL&OXA-48 disc kit (Liofilchem, Roseto degli Abruzzi, Italy) [49,50,51]. The latter three tests have been recently evaluated. The test from Rosco diagnostica (ROS) and the Combi Carba plus assay from MAST group (MAST-CDT) detected 86% of carbapenemase-producing strains, while the assay developed by Liofilchem (LIO-CDT) detected 96%. However, false-positive results occurred more frequently with LIO-CDT (6 of 47 carbapenemase negative isolates) than with ROS and MAST-CDT (1 of 47 negative strains each). Classification according to Ambler was correct in 85%, 84% and 96% of CPE for MAST-CDT, ROS-CDT, and LIO-CDT, respectively. Identification of carbapenemases was highly dependent on the carbapenemase-subgroup for all tests. While MAST-CDT and LIO-CDT detected 94% of all class B enzymes, ROS-CDT was more successful in class B detection and LIO-CDT in class D detection (both 100%).
2.2.5. Modified Hodge Test
The modified Hodge test (MHT) is an additional test for the detection of carbapenemases and based on the inactivation of a carbapenem. A susceptible strain (usually E. coli ATCC 25922) is inoculated onto an agar plate, and a carbapenem disc is placed in the center. The test strains as well as control strains are streaked in lines from the center to the periphery of the plate. If the test strain produces a carbapenemase, the carbapenem is inactivated and the susceptible E. coli strain grows alongside the test strain, which can be observed by cloverleaf-like indentations (Figure 2B). The performance of MHT is lower than that of other inactivation tests, especially for Ambler class B carbapenemases such as NDM-1 (sensitivity 50% without addition of zinc sulfate). Additionally, a low specificity and high numbers of false-positive results are observed in isolates overproducing AmpC or ESBL [52]. Therefore, the CLSI no longer recommends this assay since 2018 [120].
2.2.6. β-Lactam Inactivation Assay (e.g., CIM)
In β-lactam inactivation assays, a susceptible indicator strain is inoculated onto an agar plate and challenged with an antibiotic disc previously incubated in a suspension of the test strain. If the test strain produces a β-lactamase capable of hydrolyzing the drug of interest, the zone of inhibition of the susceptible strain will decrease compared to the control with an untreated antibiotic disc (Figure 2E). The carbapenem inactivation method (CIM) is currently recommended by EUCAST and CLSI for detection of carbapenemases and has a high sensitivity and specificity [110,121].
The original protocol was used for the detection of carbapenemase-producing bacteria and recommended suspending the test strain in 400 µl of water, adding an antibiotic disc, followed by 2 h of incubation at 37 °C [53]. While the principle of this assay is applicable for the detection of ESBLs and carbapenemases in Gram-negative bacteria including nonfermenters, it is most commonly used for carbapenemase detection in Enterobacterales. Both cultured bacteria and blood-culture fluid can be used for the β-lactam inactivation assay [56,122].
The first established CIM protocol was modified in several parameters to improve the performance. In the so-called modified CIM-test (mCIM), the test strain is suspended in tryptic soy broth instead of water, and incubation time of the antibiotic disc in the bacterial suspension was increased from 2 h to 4 h, which improves sensitivity. If the test strains are additionally incubated with the antibiotic disc and either EDTA (eCIM) or EDTA and phenylboronic acid (CIMPlus), the putative Ambler class of the isolate can be identified [123,124]. The addition of zinc sulfate (zCIM test) to tryptic soy broth has been shown to improve the detection of weakly expressed metallo-β-lactamases, e.g., VIM or NDM (Ambler class B) [50,55]. To reduce the time-to-result, Jing et al. developed the rapid carbapenemase detection method (rCDM). In this modified protocol, test strains grown overnight on blood agar are smeared on an imipenem disc and then placed on an agar plate inoculated with a susceptible indicator strain. This test can already be read after an incubation of 5–6 h [57].
All CIM assays perform well with high specificity and sensitivity (81–100% and 97–100%, respectively), but false-positive results can occur in strains with reduced porin expression and overexpression of AmpC β-lactamase or ESBL. In addition, detection of strains with low carbapenemase-activity remains challenging.
2.2.7. Colorimetric Assays
While CIM assays still have a time-to-result of 5 to 20 h, colorimetric assays have been developed for rapid detection of ESBL and carbapenemases. The ESBL-NDP test is employed for detection of ESBL activity. Lysed bacteria are incubated in a medium containing red phenol as pH indicator and supplemented with either cefotaxime, cefotaxime and tazobactam or without antibiotics. Hydrolysis of cefotaxime by ESBL leads to the formation of carboxylic acid which induces a color change from red to yellow. In the case of ESBLs, this reaction can be inhibited by tazobactam (Figure 3). The test was also challenged with spiked blood samples and urine and demonstrated good sensitivity and specificity [125]. The principle of the NDP test (also called NP-test) underlies the commercially available Rapid ESBL Screen kit 98022 (Rosco Diagnostica, Taastrup, Denmark) [126]. Other colorimetric test kits include the β-Lacta test (Bio-Rad, Marnes-La-Coquette, France), but this assay is used for the detection of 3rd generation cephalosporin-resistance and cannot distinguish between carbapenemases and ESBLs [127].
Comparable to the detection of ESBL enzymes by pH decrease, the Carba NP test has been developed for detection of carbapenemases. The hydrolysis of imipenem by a carbapenemase leads to an acidification of a phenol red solution, resulting in color change from red to orange or yellow [128]. The follow-up version Carba NP test II again includes inhibitors (tazobactam and EDTA) to differentiate between Ambler classes [129]. Modified variants of this test are suitable for the detection of CPE in blood cultures [56,58]. A disadvantage of the colorimetric Carba NP assays is the high number of false-negative results for Enterobacterales and Pseudomonas spp. with low hydrolytic activity, such as OXA-48 [130]. In a variation of the assay, this already rapid test (2 h time-to-result) was modified for even faster results by omitting the lysis step (CNPt-direct test) and including the detergent Triton X-100 instead [65]. Improved OXA-48 detection was achieved by Ma et al. who developed the substrate CARBA-H, which provides better enzyme-substrate interaction for OXA-48 and shows strong fluorescence upon cleavage [66].
Due to the increasing number of CPE, a variety of detection kits are commercially available, which include the β-CARBA assay (Biorad, Hercules, CA, USA), NeoRapid CARB (Rosco Diagnostica, Taastrup, Denmark) and CARBA PAcE (Mast Group, Bootle, UK) (Table 1). These tests have been validated in several studies and showed overall good performance. Poor detection of metallo-carbapenemases could be partly improved by use of bacterial material from blood agar instead of MH-agar or supplementation of the growth medium with zinc sulfate [55,56,60,62].
Colorimetric tests provide a rapid indication if the test strain is an ESBL- or carbapenemase producer and tests with inhibitors can identify which Ambler class the enzymes belong to. However, precise identification of the type of ESBL or carbapenemase cannot be achieved using cultural methods and requires molecular techniques.
2.3. Molecular Methods
Molecular methods have the highest sensitivity and specificity for the detection of resistance genes and can be applied to cultured isolates or directly to clinical specimens. They can provide accurate information on the type of ESBL enzyme or carbapenemase and have a relatively short time-to-result. Although molecular methods have the disadvantage of requiring qualified personnel and incur high costs for technical equipment and consumables, the number of laboratories using these techniques is growing. This is due in part to the continuously increasing number of different methods and commercially available assays (Table 1). In particular, ESBL and carbapenemase screenings at hospital admission benefit from rapid results without prior cultivation steps.
2.3.1. PCR, RT-PCR and Microarray Techniques
For simultaneous detection of multiple target genes, multiplex PCR and microarrays are the methods of choice. These assays provide a more comprehensive picture of the resistance landscape of an isolate [131], since many isolates harbor multiple resistance genes [132]. A major advantage of resistance gene detection is that low expression levels and catalytical activities do not impact the result, allowing detection of β-lactamases with low activity [131]. A disadvantage is that only genes which are targeted in the assay can be detected. Therefore, multiplex PCR and microarray assays have to be continuously improved and expanded with the emergence of new resistance genes.
Several in-house multiplex PCR assays have been published [132,133,134,135]. Today, commercially available PCR-assays are available and frequently preferred over in-house tests. In order to detect patients harboring MDR bacteria at hospital admission, it is useful to select assays that can be performed directly from rectal swabs. One example is the ESBL ELITe MGB Kit (ELITechGroup, Puteaux, France). It is a multiplex real-time PCR assay for the detection of CTX-M-genes and can be used on blood cultures or rectal swabs. The assay performed well, showing 100% sensitivity and 96.6% specificity [85]. Another multiplex real-time PCR assay specific for detection of ESBL-producing bacteria is the Check-Direct ESBL Screen for BD MAX (Check-Points Health BV, Wageningen, Netherlands) which can detect the ESBL gene families CTX-M-1, CTX-M-2, CTX-M-9 and SHV-ESBL. However, sensitivity of this assay was 95.2% but only evaluated on a small number of ESBL positive specimens (n = 21). Specificity was slightly higher at 97.6% and modified cut-off values even increased specificity to 98.8% [136].
The number of commercially available PCR-based assays for detection of carbapenemase-producing Enterobacterales is even higher (Table 1). Many of these assays are also suitable for direct detection of CPE from rectal swabs. Checkpoint developed the BD MAX Check-Points CPO-assay for detection of KPC, VIM/IMP, NDM and OXA-48 carbapenemase-producers. In one study, this assay was challenged using 128 rectal swabs, among others, and demonstrated a sensitivity and specificity of 92.8% and 97.8%, respectively. Nevertheless, rare IMP and OXA-48-like producers (IMP-11, IMP-13, IMP-14) were missed by this assay. Results were obtained within 2.5 h for 12 samples at a time [83]. In another study, comparable results were obtained with the BD MAX Check-Points CPO-assay for rectal swabs, which achieved a sensitivity of 96.6–100% and a specificity of 98.3–100%, depending on the type of carbapenemase tested [137]. Another technique is used in the Check-MDR CT103 XL assay (Check Points, Wageningen, The Netherlands), which combines a targeted PCR with array methods for detection. It detects 11 carbapenemases, 19 ESBL groups and subgroups, and additional minor ESBLs, AmpCs and MCR [138]. The predecessor Check-MDR CT103 performed well in the study by Cuzon et al., with sensitivity and specificity of 95–100% and 100%, respectively [84]. Other tests for CPE detection from rectal swabs include the Xpert Carba-R assay for the GeneXpert system (Cepheid, Sunnyvale, California [139,140,141]), the CRE ELITe MGB Kit (ELITechGroup, Puteaux, France [85]), GenePOC/Revogene Carba C assay (Meridian Bioscience, Cincinnati, Ohio [46]), and assays developed by MOBIDIAG for the Amplidiag® Easy system, namely, Amplidiag CarbaR + VRE and Amplidiag CarbaR-MCR assays (Mobidiag Ltd., Espoo, Finland [86,87]).
2.3.2. Loop-Mediated Isothermal Amplification Assay (LAMP)
LAMP can circumvent the disadvantages of PCR assays, namely the high costs and negative influence of compounds present in clinical samples which can inhibit DNA polymerase activity. Instead of repetitive temperature cycles like in PCR, only isothermal conditions are required. Good results were obtained with the eazyplex SuperBug CRE system (Amplex Biosystems GmbH, Giessen, Germany), which can detect ESBLs of the CTX-M-1 and CTX-M-9 group, and the carbapenemases KPC, VIM, NDM, OXA-48 and OXA-181. The assay showed 100% concordant results compared to PCR based assays when using cultured E. coli isolates [142]. Comparable results were reported for eazyplex SuperBug CRE on Klebsiella spp. and Pseudomonas aeruginosa isolates [143] and on cultured Enterobacterales and Pseudomonas isolates [82,144]. The assay was also able to detect ESBL-encoding genes in urine samples with high sensitivity (100%) and specificity (97.8%) [145]. A drawback is the lack of detection of IMP-carbapenemases and the small number of studies with clinical specimens, such as rectal swabs.
Molecular methods are advantageous due to their high sensitivity and specificity, but not all diagnostic laboratories are equipped with the appropriate devices and trained personnel. In addition, molecular methods are expensive compared to phenotypic assays. Further developments in the field of molecular diagnostics could circumvent these drawbacks and lead to a more widespread implementation of these techniques in routine laboratories.
2.4. Further Methods
2.4.1. Immunochromatographic Test (ICT)
Most ICTs in the microbiological laboratory are lateral flow double-antibody sandwich assays. After application of the analyte to the sample pad, the antigens (e.g., β-lactamases) migrate along the nitrocellulose membrane by capillary flow. They form a complex with dye-labeled antibodies (e.g., gold particles, latex microspheres) on the conjugate pad and are captured by immobilized antibodies on a nitrocellulose membrane at the test line resulting in a visible band. The control line consists of immobilized anti-IgG antibodies which capture the excess dye-labeled antibodies, thereby serving as a control for the capillary flow (Figure 4). The main advantage of ICTs is that they are easy to use, relatively cheap, do not require additional and costly analyzers and provide a very short time-to-result.
The NG-Test CTX-MULTI (NG biotech, Guipry, France) was developed to detect group CTX-M-1, -2, -8, -9, -25 producing Enterobacterales from bacterial colonies and positive blood cultures [146]. The authors point out that in settings with high 3rd generation cephalosporin resistance due to other resistance mechanisms such as plasmid-mediated AmpC, this test will lack sensitivity. Addressing this restriction, Moguet et al. developed a functional ICT using an incubation step of a bacterial colony with cefotaxime and anti-cefotaxime antibodies to detect expanded cephalosporinase activity regardless of its conferring enzyme (unpublished data).
For carbapenemases, different tests are commercially available and have been extensively studied. The NG-Test CARBA-5 (NG biotech, Guipry, France) detects the most prevalent carbapenemases KPC, OXA-48-like, VIM, IMP, and NDM from bacterial colonies and directly from positive blood cultures with high sensitivity and specificity (84.2–99.2% and 95.3–100%, respectively), (Table 1) [55,69,71,72]. The RESIST-5 O.O.K.N.V. as well as its predecessors RESIST-4 and RESIST-3 (Coris BioConcept, Gembloux, Belgium) can be performed from bacterial colonies as well as directly from positive blood cultures. They detect and differentiate between OXA-48-like, OXA-163 (only RESIST-5), KPC, NDM, and VIM (only RESIST-4 and -5) with high sensitivity and specificity (84.2–100% and 100%, respectively) [55,67,68,69,147]. While the performance for KPC and OXA-48-like carbapenemases is excellent (sensitivity/specificity 100% in most studies), lower sensitivity has been reported for some Ambler class B β-lactamases especially in Proteus spp. and from positive blood cultures [67,147,148]. This can be overcome by adding zinc to the incubation protocol or working with zinc supplemented agar plates [67,149].
Despite the numerous advantages of ICTs, they share the same problems with molecular methods, e.g., only the carbapenemases included in the test design can be detected, and rare carbapenemases are usually missed. To overcome this restriction, Baeza and colleagues proposed an algorithm applying immunochromatographic assays in combination with a subsequent zCIM test for the detection of common and rare carbapenemases (Figure 5). Reaching a sensitivity of 99.3% on a large collection of clinical isolates with common and rare carbapenemases, this algorithm provides a robust and cost-effective tool for carbapenemase confirmation, including uncommon variants [55].
Boattini and colleagues proposed a fast-track workflow for Enterobacterales from positive blood cultures combining the NG-Test CTX-M MULTI and the NG-Test Carba 5 assay after identification of Enterobacterales using the MBT Sepsityper IVD KIT (Bruker DALTONICS, Bremen, Germany). Analyzing a total of 236 episodes of Enterobacterales blood stream infections, a good agreement with conventional phenotypic results was recorded. Time-to-result (defined starting point was the processing of positive BC) for this fast-track workflow was 42 min compared to 38 h for the conventional workflow (identification and AST from overnight cultures) [150]. In practice this means that that therapeutic and antibiotic stewardship interventions can be implemented one to two days earlier with this new protocol, which highlights the potential of ICT used in innovative workflows to accelerate clinical decision making.
2.4.2. Electrochemical Assays
Another way to detect resistance to carbapenems or 3rd generation cephalosporins with little equipment is by employing electrochemical assays. They use disposable sensors with screen printed carbon electrodes in combination with small electronical measuring devices.
Bogaerts and colleagues developed the BYG Carba test for the rapid confirmation of carbapenemase activity. The test measures variations of conductivity on an electro-sensing polymer coated electrode conferred by imipenem hydrolysis. These variations are analyzed in real-time by a portable reader [80]. The test was evaluated with a set of 1181 Enterobacterales and showed a good sensitivity and specificity for the confirmation of carbapenemases from bacterial colonies (96.3% and 99.7%, respectively) [151].
Rochelet and colleagues described a voltammetric assay for the detection of ESBLs. Bacterial isolates are incubated together with nitrocefin, and subsequently, the hydrolysis of nitrocefin into an electroactive product is detected by a voltammetric measurement on a disposable carbon screen-printed sensor [152].
The successor of this principle is the commercially available BL-RED test (Coris BioConcept, Gembloux, Belgium) which is designed for the detection 3rd generation cephalosporin hydrolysis from bacterial culture or directly from positive blood cultures. Durand and colleagues challenged the test with a set of 150 Enterobacterales spiked into blood cultures and reported a good detection of 3rd generation cephalosporin resistance conferred by Ambler class A β-lactamases (sensitivity 83.3% and specificity 99.1%), but the test failed to detect 3rd generation cephalosporin resistance conferred by Ambler classes B, C and D β-lactamases [81].
2.4.3. MALDI-TOF MS
MALDI-TOF MS was a revolution in the field regarding species identification. It is increasingly embraced for the detection of antimicrobial resistance (AMR), and this application will likely become an essential part of the routine laboratory in the near future [153,154]. Regarding the detection of MDR Enterobacterales, there are three promising approaches for MALDI-TOF MS application available: The detection of β-lactamase activity, estimating the effect of antibiotics on the growth of bacteria, and the direct detection of biomarkers (e.g., enzymes or target modifications) associated with AMR (Table 1).
The detection of β-lactamase activity using MALDI-TOF is already available for IVD use in Europe. The principle is to incubate the bacterial isolate in question with an antibiotic. Hydrolysis of the β-lactam antibiotic results in a mass shift of the corresponding antibiotic within the spectrum obtained by MALDI-TOF [155,156]. The MBT STAR-Carba and the STAR-Cepha IVD Kits (Bruker DALTONICS, Bremen, Germany) are two commercially available functional tests for the detection of carbapenem resistance and resistance against 3rd generation cephalosporins with high sensitivity and specificity (98–100% and 97–100%, respectively) [74,75,76,77]. The downside of this approach is that it only detects resistance conferred by hydrolysis of the target antibiotic and therefore yields false-negative results for resistance conferred by other mechanisms, e.g., drug efflux or porin loss.
Another approach for MALDI-TOF MS is to use it as a sensitive instrument for growth detection in presence of defined antibiotic concentrations. For this purpose, Idelevich and colleagues developed the direct-on-target microdroplet growth assay (DOT-MGA) [78]. In this assay a defined bacterial inoculum is incubated together with an antibiotic at the clinical breakpoint concentration directly on a MALDI-TOF MS target. These on-target-microdroplets are incubated in a humidity chamber and analyzed after drying with the MALDI Biotyper (Bruker DALTONICS, Bremen, Germany). Species identification on a target with the antibiotic (score ≥ 1.7) is interpreted as non-susceptible whereas missing species identification (score ≤ 1.7) is interpreted as susceptible to the antibiotic. This technique was shown to have an excellent sensitivity and specificity (100%) for the detection of meropenem resistance in K. pneumoniae after 4 h incubation from culture plates [78] as well as directly from positive blood cultures (sensitivity 91.7%, specificity 100%) [79]. The technique was successfully expanded to detect ESBL and AmpC β-lactamases in Enterobacterales [157]. While this application is still for research-use-only (RUO), it is a very promising approach for the detection of antimicrobial resistance in Enterobacterales as it uses an easy-to-follow protocol, an instrument that is available in many microbiological laboratories and has an acceptable TAT. Moreover, it is independent of the resistance mechanisms and can be applied to any combination of antibiotic and bacterial species.
Another technique is the direct detection of biomarkers of antimicrobial resistance in mass spectra. Using this approach, the same mass spectra are used for species identification and resistance detection. This could significantly shorten laboratory workflows and is already established for some resistance markers, e.g., for some MRSA strains and for carbapenem resistance in Bacteroides fragiliscfiA pos. [158,159]. The detection of mass spectrometry peaks of some β-lactamases such as TEM-1 [160] and KPC-2 [161,162] was shown to distinguish reliably between resistant and susceptible isolates. Cordavana and colleagues designed an algorithm integrated into the MALDI Biotyper System (Bruker DALTONICS, Bremen, Germany) that enables the automated detection of KPC harboring Klebsiella pneumoniae from cultured colonies as well as directly from positive blood cultures during the routine identification process (sensitivity 85.1%; specificity 100%) [163]. The protocols for Enterobacterales are not yet validated for routine laboratory use but are promising approaches for the near future. For now, biomarkers allow the detection of a few selected resistance determinants, and therefore, confirmation of negative results by phenotypic AST methods is still needed. With better and broader spectra libraries, further resistance mechanisms can likely be detected in the future. Accelerating bioinformatic tools like machine learning will play a crucial role in the construction of those libraries [153].
3. Summary and Future Perspectives
Patients colonized or infected by MDRE can today be more rapidly and reliably identified using assays with shorter turn-around-time and improved sensitivity.
Culture based approaches rely on the cultivation on selective or unselective agars, subsequent susceptibility testing and identification of resistance mechanisms. This workflow will likely remain the standard in the medical microbiology laboratory. This approach permits the subsequent characterization of isolates, e.g., by phenotypic methods or molecular methods including next generation sequencing (NGS). For patient screening using the classical culture approach, we recommend using an ESBL in combination with a CPE agar, as not all CPE can be detected by ESBL screening agars. The use of an enrichment broth is optional but will further improve the detection of MDRE.
The traditional culture-based workflow requires about 2.5 days while using molecular techniques directly from screening specimens only requires a few hours. At the time of writing, PCR techniques are still costly when applied routinely for screening purposes from sample material [164]. Since molecular detection of MDRE has demonstrated excellent sensitivity and specificity, PCR is increasingly used in diagnostic practice as costs per test are decreasing and many commercial assays on different molecular platforms have become available.
Many tests presented in this review have primarily been designed for the confirmation of ESBL and carbapenemase production but have been evaluated for the use directly on clinical specimens, especially blood cultures. The more widespread use of these techniques will accelerate clinical decision making and ultimately improve patient outcomes. Different rapid diagnostic interventions (i.e., rapid ID, rapid AST or the determination of resistance genes) have shown to decrease the time for adequate therapy. For other parameters such as length of stay, overall mortality and cost effectiveness, the picture is less clear. Most studies combine the implementation of rapid diagnostics with antimicrobial stewardship programs making it difficult to assess the genuine impact of new technologies alone [165].
Next generation sequencing (NGS) is increasingly used in microbiological laboratories, mainly in reference institutions and research. The DNA sequence of a bacterial genome can be obtained in a single sequencing run and is very successfully used in the determination of antibiotic resistance genes (ARG) and typing of pathogens in hospital outbreaks. NGS can be employed for in-depth analysis of single isolates but also allows culture-free identification of bacteria and ARG directly from complex samples like stool [166]. New innovative bioinformatics tools not only allow the detection of well-described ARGs but also enable the identification of previously uncharacterized resistance genes from shotgun metagenomic sequencing data of the human microbiota [167]. On the other hand, the genotype of a bacterial isolate does not precisely translate into its resistance phenotype. To date, there is insufficient evidence to infer antibiotic susceptibility from whole genome sequencing data to guide clinical decision making [168].
All these applications make NGS a valuable tool for identification, surveillance and most likely future clinical decision making regarding MDRE. With declining costs for the initial investment in an NGS platform, decreased costs per run and the development of accessible bioinformatics software, this technique will inevitably be incorporated into routine microbiological practice. However, standardization of protocols, quality control issues and bioinformatic capacities are serious obstacles that need to be addressed before a more widespread implementation in clinical microbiology laboratories seems realistic [169].
Overall rapid and reliable detection of MDRE in clinical specimens is a key capacity for every clinical microbiological laboratory. Multidrug resistance in Enterobacterales is a rapidly evolving field with a diverse armamentarium of in-house and commercially available tests as well as fascinating future perspectives.
Funding
P.T. and A.H. have received research funding by Coris BioConcept. A.H. has additionally received research support from GenePOC and speaking fees from Cepheid. The funders had no role in the design of the study; in the collection, analysis or interpretation of data; in the writing of the manuscript or in the decision to publish the results. J.N. declares no conflict of interest.
References
- Roca, I.; Akova, M.; Baquero, F.; Carlet, J.; Cavaleri, M.; Coenen, S.; Cohen, J.; Findlay, D.; Gyssens, I.; Heuer, O.E.; et al. The global threat of antimicrobial resistance: Science for intervention. New Microbes New Infect. 2015, 6, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, N.D.; Temkin, E.; Carmeli, Y. The negative impact of antibiotic resistance. Clin. Microbiol. Infect. 2016, 22, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P. Carbapenemase-producing Enterobacteriaceae: Overview of a major public health challenge. Med. Mal. Infect. 2014, 44, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrancianu, C.O.; Dobre, E.G.; Gheorghe, I.; Barbu, I.; Cristian, R.E.; Chifiriuc, M.C. Present and Future Perspectives on Therapeutic Options for Carbapenemase-Producing Enterobacterales Infections. Microorganisms 2021, 9, 730. [Google Scholar] [CrossRef]
- Mota, R.; Pinto, M.; Palmeira, J.; Goncalves, D.; Ferreira, H. Multidrug-resistant bacteria as intestinal colonizers and evolution of intestinal colonization in healthy university students in Portugal. Access Microbiol. 2021, 3, acmi000182. [Google Scholar] [CrossRef] [PubMed]
- Ruppe, E.; Andremont, A. Causes, consequences, and perspectives in the variations of intestinal density of colonization of multidrug-resistant enterobacteria. Front. Microbiol. 2013, 4, 129. [Google Scholar] [CrossRef] [Green Version]
- Ebrahimi, F.; Mozes, J.; Monostori, J.; Goracz, O.; Fesus, A.; Majoros, L.; Szarka, K.; Kardos, G. Comparison of rates of fecal colonization with extended-spectrum beta-lactamase-producing enterobacteria among patients in different wards, outpatients and medical students. Microbiol. Immunol. 2016, 60, 285–294. [Google Scholar] [CrossRef] [Green Version]
- Angelin, M.; Forsell, J.; Granlund, M.; Evengard, B.; Palmgren, H.; Johansson, A. Risk factors for colonization with extended-spectrum beta-lactamase producing Enterobacteriaceae in healthcare students on clinical assignment abroad: A prospective study. Travel Med. Infect. Dis. 2015, 13, 223–229. [Google Scholar] [CrossRef]
- Maharjan, A.; Bhetwal, A.; Shakya, S.; Satyal, D.; Shah, S.; Joshi, G.; Khanal, P.R.; Parajuli, N.P. Ugly bugs in healthy guts! Carriage of multidrug-resistant and ESBL-producing commensal Enterobacteriaceae in the intestine of healthy Nepalese adults. Infect. Drug Resist. 2018, 11, 547–554. [Google Scholar] [CrossRef] [Green Version]
- Chirindze, L.M.; Zimba, T.F.; Sekyere, J.O.; Govinden, U.; Chenia, H.Y.; Sundsfjord, A.; Essack, S.Y.; Simonsen, G.S. Faecal colonization of E. coli and Klebsiella spp. producing extended-spectrum beta-lactamases and plasmid-mediated AmpC in Mozambican university students. BMC Infect. Dis. 2018, 18, 244. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.S.; Lai, L.C.; Chen, Y.A.; Lin, K.Y.; Chou, Y.H.; Chen, H.C.; Wang, S.S.; Wang, J.T.; Chang, S.C. Colonization with Multidrug-Resistant Organisms Among Healthy Adults in the Community Setting: Prevalence, Risk Factors, and Composition of Gut Microbiome. Front. Microbiol. 2020, 11, 1402. [Google Scholar] [CrossRef] [PubMed]
- Arcilla, M.S.; van Hattem, J.M.; Haverkate, M.R.; Bootsma, M.C.J.; van Genderen, P.J.J.; Goorhuis, A.; Grobusch, M.P.; Lashof, A.M.O.; Molhoek, N.; Schultsz, C.; et al. Import and spread of extended-spectrum beta-lactamase-producing Enterobacteriaceae by international travellers (COMBAT study): A prospective, multicentre cohort study. Lancet Infect. Dis. 2017, 17, 78–85. [Google Scholar] [CrossRef]
- Hamprecht, A.; Rohde, A.M.; Behnke, M.; Feihl, S.; Gastmeier, P.; Gebhardt, F.; Kern, W.V.; Knobloch, J.K.; Mischnik, A.; Obermann, B.; et al. Colonization with third-generation cephalosporin-resistant Enterobacteriaceae on hospital admission: Prevalence and risk factors. J. Antimicrob. Chemother. 2016, 71, 2957–2963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Villodres, A.; Martin-Gandul, C.; Penalva, G.; Guisado-Gil, A.B.; Crespo-Rivas, J.C.; Pachon-Ibanez, M.E.; Lepe, J.A.; Cisneros, J.M. Prevalence and Risk Factors for Multidrug-Resistant Organisms Colonization in Long-Term Care Facilities Around the World: A Review. Antibiotics 2021, 10, 680. [Google Scholar] [CrossRef]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef] [Green Version]
- Maechler, F.; Pena Diaz, L.A.; Schroder, C.; Geffers, C.; Behnke, M.; Gastmeier, P. Prevalence of carbapenem-resistant organisms and other Gram-negative MDRO in German ICUs: First results from the national nosocomial infection surveillance system (KISS). Infection 2015, 43, 163–168. [Google Scholar] [CrossRef]
- Zaha, D.C.; Kiss, R.; Hegedus, C.; Gesztelyi, R.; Bombicz, M.; Muresan, M.; Pallag, A.; Zrinyi, M.; Pall, D.; Vesa, C.M.; et al. Recent Advances in Investigation, Prevention, and Management of Healthcare-Associated Infections (HAIs): Resistant Multidrug Strain Colonization and Its Risk Factors in an Intensive Care Unit of a University Hospital. Biomed. Res. Int 2019, 2019, 2510875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arena, F.; Vannetti, F.; Di Pilato, V.; Fabbri, L.; Colavecchio, O.L.; Giani, T.; Marraccini, C.; Pupillo, R.; Macchi, C.; Converti, F.; et al. Diversity of the epidemiology of carbapenemase-producing Enterobacteriaceae in long-term acute care rehabilitation settings from an area of hyperendemicity, and evaluation of an intervention bundle. J. Hosp. Infect. 2018, 100, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Magrini, E.T.N. Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery, and Development of New Antibiotics; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- ECDC. Antimicrobial Resistance in the EU/EEA (EARS-Net)—Annual Epidemiological Report 2019; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2020.
- Naas, T.; Oueslati, S.; Bonnin, R.A.; Dabos, M.L.; Zavala, A.; Dortet, L.; Retailleau, P.; Iorga, B.I. Beta-lactamase database (BLDB)—Structure and function. J. Enzyme Inhib. Med. Chem. 2017, 32, 917–919. [Google Scholar] [CrossRef]
- Munita, J.M.; Arias, C.A. Mechanisms of Antibiotic Resistance. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawa, T.; Kooguchi, K.; Moriyama, K. Molecular diversity of extended-spectrum beta-lactamases and carbapenemases, and antimicrobial resistance. J. Intensive Care 2020, 8, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bush, K. Proliferation and significance of clinically relevant beta-lactamases. Ann. N. Y. Acad. Sci. 2013, 1277, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Zhang, H.; Du, H. Carbapenemases in Enterobacteriaceae: Detection and Antimicrobial Therapy. Front. Microbiol. 2019, 10, 1823. [Google Scholar] [CrossRef] [PubMed]
- Arnold, R.S.; Thom, K.A.; Sharma, S.; Phillips, M.; Kristie Johnson, J.; Morgan, D.J. Emergence of Klebsiella pneumoniae carbapenemase-producing bacteria. South. Med. J. 2011, 104, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Yigit, H.; Queenan, A.M.; Anderson, G.J.; Domenech-Sanchez, A.; Biddle, J.W.; Steward, C.D.; Alberti, S.; Bush, K.; Tenover, F.C. Novel carbapenem-hydrolyzing beta-lactamase, KPC-1, from a carbapenem-resistant strain of Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2001, 45, 1151–1161. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, P.; Mariotte, S.; Naas, T.; Labia, R.; Nicolas, M.H. Biochemical properties of a carbapenem-hydrolyzing beta-lactamase from Enterobacter cloacae and cloning of the gene into Escherichia coli. Antimicrob. Agents Chemother. 1993, 37, 939–946. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, B.A.; Bush, K.; Keeney, D.; Yang, Y.; Hare, R.; O’Gara, C.; Medeiros, A.A. Characterization of IMI-1 beta-lactamase, a class A carbapenem-hydrolyzing enzyme from Enterobacter cloacae. Antimicrob. Agents Chemother. 1996, 40, 2080–2086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yong, D.; Toleman, M.A.; Giske, C.G.; Cho, H.S.; Sundman, K.; Lee, K.; Walsh, T.R. Characterization of a new metallo-beta-lactamase gene, bla(NDM-1), and a novel erythromycin esterase gene carried on a unique genetic structure in Klebsiella pneumoniae sequence type 14 from India. Antimicrob. Agents Chemother. 2009, 53, 5046–5054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauretti, L.; Riccio, M.L.; Mazzariol, A.; Cornaglia, G.; Amicosante, G.; Fontana, R.; Rossolini, G.M. Cloning and characterization of blaVIM, a new integron-borne metallo-beta-lactamase gene from a Pseudomonas aeruginosa clinical isolate. Antimicrob. Agents Chemother. 1999, 43, 1584–1590. [Google Scholar] [CrossRef] [Green Version]
- Arakawa, Y.; Murakami, M.; Suzuki, K.; Ito, H.; Wacharotayankun, R.; Ohsuka, S.; Kato, N.; Ohta, M. A novel integron-like element carrying the metallo-beta-lactamase gene blaIMP. Antimicrob. Agents Chemother. 1995, 39, 1612–1615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordmann, P.; Gniadkowski, M.; Giske, C.G.; Poirel, L.; Woodford, N.; Miriagou, V.; European Network on, C. Identification and screening of carbapenemase-producing Enterobacteriaceae. Clin. Microbiol. Infect. 2012, 18, 432–438. [Google Scholar] [CrossRef] [Green Version]
- Larson, E. Community factors in the development of antibiotic resistance. Annu Rev. Public Health 2007, 28, 435–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voor, A.F.; Mourik, K.; Beishuizen, B.; van der Schoor, A.S.; Verbon, A.; Vos, M.C.; Severin, J.A. Acquisition of multidrug-resistant Enterobacterales during international travel: A systematic review of clinical and microbiological characteristics and meta-analyses of risk factors. Antimicrob. Resist. Infect. Control 2020, 9, 71. [Google Scholar] [CrossRef] [PubMed]
- Karaiskos, I.; Giamarellou, H. Carbapenem-Sparing Strategies for ESBL Producers: When and How. Antibiotics 2020, 9, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacconelli, E.; Cataldo, M.A.; Dancer, S.J.; De Angelis, G.; Falcone, M.; Frank, U.; Kahlmeter, G.; Pan, A.; Petrosillo, N.; Rodriguez-Bano, J.; et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clin. Microbiol. Infect. 2014, 20 (Suppl. 1), 1–55. [Google Scholar] [CrossRef] [Green Version]
- CDC. Guidance for control of infections with carbapenem-resistant or carbapenemase-producing Enterobacteriaceae in acute care facilities. MMWR Morb. Mortal Wkly. Rep. 2009, 58, 256–260. [Google Scholar]
- Jazmati, T.; Hamprecht, A.; Jazmati, N. Comparison of stool samples and rectal swabs with and without pre-enrichment for the detection of third-generation cephalosporin-resistant Enterobacterales (3GCREB). Eur. J. Clin. Microbiol. Infect. Dis. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L.; Healthcare Infection Control Practices Advisory, C. Management of multidrug-resistant organisms in health care settings, 2006. Am. J. Infect. Control. 2007, 35, S165–S193. [Google Scholar] [CrossRef]
- Van Prehn, J.; Kaiser, A.M.; van der Werff, S.D.; van Mansfeld, R.; Vandenbroucke-Grauls, C. Colonization sites in carriers of ESBL-producing Gram-negative bacteria. Antimicrob. Resist. Infect. Control 2018, 7, 52. [Google Scholar] [CrossRef] [Green Version]
- Warnke, P.; Johanna Pohl, F.P.; Kundt, G.; Podbielski, A. Screening for Gram-negative bacteria: Impact of preanalytical parameters. Sci. Rep. 2016, 6, 30427. [Google Scholar] [CrossRef] [PubMed]
- Dyakova, E.; Bisnauthsing, K.N.; Querol-Rubiera, A.; Patel, A.; Ahanonu, C.; Tosas Auguet, O.; Edgeworth, J.D.; Goldenberg, S.D.; Otter, J.A. Efficacy and acceptability of rectal and perineal sampling for identifying gastrointestinal colonization with extended spectrum beta-lactamase Enterobacteriaceae. Clin. Microbiol. Infect. 2017, 23, 577.e1–577.e3. [Google Scholar] [CrossRef] [PubMed]
- Sturod, K.; Dahle, U.R.; Berg, E.S.; Steinbakk, M.; Wester, A.L. Evaluation of the ability of four ESBL-screening media to detect ESBL-producing Salmonella and Shigella. BMC Microbiol. 2014, 14, 217. [Google Scholar] [CrossRef] [Green Version]
- Lucena Baeza, L.; Hamprecht, A. A profile of the GenePOC Carba C assay for the detection and differentiation of gene sequences associated with carbapenem-non-susceptibility. Expert Rev. Mol. Diagn. 2020, 20, 757–769. [Google Scholar] [CrossRef] [PubMed]
- Göttig, S.; Walker, S.V.; Saleh, A.; Koroska, F.; Sommer, J.; Stelzer, Y.; Steinmann, J.; Hamprecht, A. Comparison of nine different selective agars for the detection of carbapenemase-producing Enterobacterales (CPE). Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 923–927. [Google Scholar] [CrossRef]
- Simner, P.J.; Gilmour, M.W.; DeGagne, P.; Nichol, K.; Karlowsky, J.A. Evaluation of five chromogenic agar media and the Rosco Rapid Carb screen kit for detection and confirmation of carbapenemase production in Gram-negative bacilli. J. Clin. Microbiol. 2015, 53, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Doyle, D.; Peirano, G.; Lascols, C.; Lloyd, T.; Church, D.L.; Pitout, J.D. Laboratory detection of Enterobacteriaceae that produce carbapenemases. J. Clin. Microbiol. 2012, 50, 3877–3880. [Google Scholar] [CrossRef] [Green Version]
- Sattler, J.; Brunke, A.; Hamprecht, A. Systematic comparison of three commercially available combination disc tests and zCIM for carbapenemase detection in Enterobacterales isolates. J. Clin. Microbiol. 2021, 59, e0314020. [Google Scholar] [CrossRef] [PubMed]
- Pantel, A.; Souzy, D.; Sotto, A.; Lavigne, J.P. Evaluation of Two Phenotypic Screening Tests for Carbapenemase-Producing Enterobacteriaceae. J. Clin. Microbiol. 2015, 53, 3359–3362. [Google Scholar] [CrossRef] [Green Version]
- Girlich, D.; Poirel, L.; Nordmann, P. Value of the modified Hodge test for detection of emerging carbapenemases in Enterobacteriaceae. J. Clin. Microbiol. 2012, 50, 477–479. [Google Scholar] [CrossRef] [Green Version]
- Van der Zwaluw, K.; de Haan, A.; Pluister, G.N.; Bootsma, H.J.; de Neeling, A.J.; Schouls, L.M. The carbapenem inactivation method (CIM), a simple and low-cost alternative for the Carba NP test to assess phenotypic carbapenemase activity in gram-negative rods. PLoS ONE 2015, 10, e0123690. [Google Scholar] [CrossRef] [Green Version]
- Pierce, V.M.; Simner, P.J.; Lonsway, D.R.; Roe-Carpenter, D.E.; Johnson, J.K.; Brasso, W.B.; Bobenchik, A.M.; Lockett, Z.C.; Charnot-Katsikas, A.; Ferraro, M.J.; et al. Modified Carbapenem Inactivation Method for Phenotypic Detection of Carbapenemase Production among Enterobacteriaceae. J. Clin. Microbiol. 2017, 55, 2321–2333. [Google Scholar] [CrossRef] [Green Version]
- Baeza, L.L.; Pfennigwerth, N.; Greissl, C.; Gottig, S.; Saleh, A.; Stelzer, Y.; Gatermann, S.G.; Hamprecht, A. Comparison of five methods for detection of carbapenemases in Enterobacterales with proposal of a new algorithm. Clin. Microbiol. Infect. 2019, 25, 1286.e9–1286.e15. [Google Scholar] [CrossRef] [Green Version]
- Meier, M.; Hamprecht, A. Systematic Comparison of Four Methods for Detection of Carbapenemase-Producing Enterobacterales Directly from Blood Cultures. J. Clin. Microbiol. 2019, 57, e00709-19. [Google Scholar] [CrossRef] [Green Version]
- Jing, X.; Min, X.; Zhang, X.; Gong, L.; Wu, T.; Sun, R.; Chen, L.; Liu, R.; Zeng, J. The Rapid Carbapenemase Detection Method (rCDM) for Rapid and Accurate Detection of Carbapenemase-Producing Enterobacteriaceae and Pseudomonas aeruginosa. Front. Cell Infect. Microbiol. 2019, 9, 371. [Google Scholar] [CrossRef] [PubMed]
- Dortet, L.; Brechard, L.; Poirel, L.; Nordmann, P. Rapid detection of carbapenemase-producing Enterobacteriaceae from blood cultures. Clin. Microbiol. Infect. 2014, 20, 340–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dortet, L.; Agathine, A.; Naas, T.; Cuzon, G.; Poirel, L.; Nordmann, P. Evaluation of the RAPIDEC(R) CARBA NP, the Rapid CARB Screen(R) and the Carba NP test for biochemical detection of carbapenemase-producing Enterobacteriaceae. J. Antimicrob. Chemother. 2015, 70, 3014–3022. [Google Scholar] [CrossRef] [Green Version]
- Bernabeu, S.; Dortet, L.; Naas, T. Evaluation of the beta-CARBA test, a colorimetric test for the rapid detection of carbapenemase activity in Gram-negative bacilli. J. Antimicrob. Chemother. 2017, 72, 1646–1658. [Google Scholar] [CrossRef]
- Mancini, S.; Kieffer, N.; Poirel, L.; Nordmann, P. Evaluation of the RAPIDEC(R) CARBA NP and beta-CARBA(R) tests for rapid detection of Carbapenemase-producing Enterobacteriaceae. Diagn Microbiol. Infect. Dis. 2017, 88, 293–297. [Google Scholar] [CrossRef]
- Sattler, J.; Brunke, A.; Hamprecht, A. Evaluation of CARBA PAcE, a novel rapid test for detection of carbapenemase-producing Enterobacterales. J. Med. Microbiol. 2021, 70, 001290. [Google Scholar] [CrossRef] [PubMed]
- Pires, J.; Novais, A.; Peixe, L. Blue-carba, an easy biochemical test for detection of diverse carbapenemase producers directly from bacterial cultures. J. Clin. Microbiol. 2013, 51, 4281–4283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novais, A.; Brilhante, M.; Pires, J.; Peixe, L. Evaluation of the Recently Launched Rapid Carb Blue Kit for Detection of Carbapenemase-Producing Gram-Negative Bacteria. J. Clin. Microbiol. 2015, 53, 3105–3107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasteran, F.; Tijet, N.; Melano, R.G.; Corso, A. Simplified Protocol for Carba NP Test for Enhanced Detection of Carbapenemase Producers Directly from Bacterial Cultures. J. Clin. Microbiol. 2015, 53, 3908–3911. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.W.; Ng, K.K.; Yam, B.H.; Ho, P.L.; Kao, R.Y.; Yang, D. Rapid Broad Spectrum Detection of Carbapenemases with a Dual Fluorogenic-Colorimetric Probe. J. Am. Chem. Soc. 2021, 143, 6886–6894. [Google Scholar] [CrossRef]
- Hamprecht, A.; Vehreschild, J.J.; Seifert, H.; Saleh, A. Rapid detection of NDM, KPC and OXA-48 carbapenemases directly from positive blood cultures using a new multiplex immunochromatographic assay. PLoS ONE 2018, 13, e0204157. [Google Scholar] [CrossRef] [Green Version]
- Greissl, C.; Saleh, A.; Hamprecht, A. Rapid detection of OXA-48-like, KPC, NDM, and VIM carbapenemases in Enterobacterales by a new multiplex immunochromatographic test. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 331–335. [Google Scholar] [CrossRef]
- Han, R.; Guo, Y.; Peng, M.; Shi, Q.; Wu, S.; Yang, Y.; Zheng, Y.; Yin, D.; Hu, F. Evaluation of the Immunochromatographic NG-Test Carba 5, RESIST-5 O.O.K.N.V., and IMP K-SeT for Rapid Detection of KPC-, NDM-, IMP-, VIM-type, and OXA-48-like Carbapenemase Among Enterobacterales. Front. Microbiol. 2020, 11, 609856. [Google Scholar] [CrossRef]
- Takissian, J.; Bonnin, R.A.; Naas, T.; Dortet, L. NG-Test Carba 5 for Rapid Detection of Carbapenemase-Producing Enterobacterales from Positive Blood Cultures. Antimicrob. Agents Chemother. 2019, 63, e00011-19. [Google Scholar] [CrossRef] [Green Version]
- Boutal, H.; Vogel, A.; Bernabeu, S.; Devilliers, K.; Creton, E.; Cotellon, G.; Plaisance, M.; Oueslati, S.; Dortet, L.; Jousset, A.; et al. A multiplex lateral flow immunoassay for the rapid identification of NDM-, KPC-, IMP- and VIM-type and OXA-48-like carbapenemase-producing Enterobacteriaceae. J. Antimicrob. Chemother. 2018, 73, 909–915. [Google Scholar] [CrossRef]
- Hopkins, K.L.; Meunier, D.; Naas, T.; Volland, H.; Woodford, N. Evaluation of the NG-Test CARBA 5 multiplex immunochromatographic assay for the detection of KPC, OXA-48-like, NDM, VIM and IMP carbapenemases. J. Antimicrob. Chemother. 2018, 73, 3523–3526. [Google Scholar] [CrossRef]
- Hoyos-Mallecot, Y.; Riazzo, C.; Miranda-Casas, C.; Rojo-Martin, M.D.; Gutierrez-Fernandez, J.; Navarro-Mari, J.M. Rapid detection and identification of strains carrying carbapenemases directly from positive blood cultures using MALDI-TOF MS. J. Microbiol. Methods 2014, 105, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Akyar, I.; Kaya Ayas, M.; Karatuna, O. Performance Evaluation of MALDI-TOF MS MBT STAR-BL Versus In-House Carba NP Testing for the Rapid Detection of Carbapenemase Activity in Escherichia coli and Klebsiella pneumoniae Strains. Microb. Drug Resist. 2019, 25, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Anantharajah, A.; Tossens, B.; Olive, N.; Kabamba-Mukadi, B.; Rodriguez-Villalobos, H.; Verroken, A. Performance Evaluation of the MBT STAR((R))-Carba IVD Assay for the Detection of Carbapenemases with MALDI-TOF MS. Front. Microbiol. 2019, 10, 1413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordovana, M.; Abdalla, M.; Ambretti, S. Evaluation of the MBT STAR-Carba Assay for the Detection of Carbapenemase Production in Enterobacteriaceae and Hafniaceae with a Large Collection of Routine Isolates from Plate Cultures and Patient-Derived Positive Blood Cultures. Microb. Drug Resist. 2020, 26, 1298–1306. [Google Scholar] [CrossRef]
- Dortet, L.; Tande, D.; de Briel, D.; Bernabeu, S.; Lasserre, C.; Gregorowicz, G.; Jousset, A.B.; Naas, T. MALDI-TOF for the rapid detection of carbapenemase-producing Enterobacteriaceae: Comparison of the commercialized MBT STAR(R)-Carba IVD Kit with two in-house MALDI-TOF techniques and the RAPIDEC(R) CARBA NP. J. Antimicrob. Chemother. 2018, 73, 2352–2359. [Google Scholar] [CrossRef] [Green Version]
- Idelevich, E.A.; Sparbier, K.; Kostrzewa, M.; Becker, K. Rapid detection of antibiotic resistance by MALDI-TOF mass spectrometry using a novel direct-on-target microdroplet growth assay. Clin. Microbiol. Infect. 2018, 24, 738–743. [Google Scholar] [CrossRef] [Green Version]
- Idelevich, E.A.; Storck, L.M.; Sparbier, K.; Drews, O.; Kostrzewa, M.; Becker, K. Rapid Direct Susceptibility Testing from Positive Blood Cultures by the Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry-Based Direct-on-Target Microdroplet Growth Assay. J. Clin. Microbiol. 2018, 56, e00913-18. [Google Scholar] [CrossRef] [Green Version]
- Bogaerts, P.; Yunus, S.; Massart, M.; Huang, T.D.; Glupczynski, Y. Evaluation of the BYG Carba Test, a New Electrochemical Assay for Rapid Laboratory Detection of Carbapenemase-Producing Enterobacteriaceae. J. Clin. Microbiol. 2016, 54, 349–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durand, C.; Boudet, A.; Lavigne, J.P.; Pantel, A. Evaluation of Two Methods for the Detection of Third Generation Cephalosporins Resistant Enterobacterales Directly from Positive Blood Cultures. Front. Cell Infect. Microbiol. 2020, 10, 491. [Google Scholar] [CrossRef]
- Garcia-Fernandez, S.; Morosini, M.I.; Marco, F.; Gijon, D.; Vergara, A.; Vila, J.; Ruiz-Garbajosa, P.; Canton, R. Evaluation of the eazyplex(R) SuperBug CRE system for rapid detection of carbapenemases and ESBLs in clinical Enterobacteriaceae isolates recovered at two Spanish hospitals. J. Antimicrob. Chemother. 2015, 70, 1047–1050. [Google Scholar] [CrossRef] [Green Version]
- Girlich, D.; Oueslati, S.; Bernabeu, S.; Langlois, I.; Begasse, C.; Arangia, N.; Creton, E.; Cotellon, G.; Sauvadet, A.; Dortet, L.; et al. Evaluation of the BD MAX Check-Points CPO Assay for the Detection of Carbapenemase Producers Directly from Rectal Swabs. J. Mol. Diagn. 2020, 22, 294–300. [Google Scholar] [CrossRef] [Green Version]
- Cuzon, G.; Naas, T.; Bogaerts, P.; Glupczynski, Y.; Nordmann, P. Evaluation of a DNA microarray for the rapid detection of extended-spectrum beta-lactamases (TEM, SHV and CTX-M), plasmid-mediated cephalosporinases (CMY-2-like, DHA, FOX, ACC-1, ACT/MIR and CMY-1-like/MOX) and carbapenemases (KPC, OXA-48, VIM, IMP and NDM). J. Antimicrob. Chemother. 2012, 67, 1865–1869. [Google Scholar] [CrossRef] [Green Version]
- Girlich, D.; Bernabeu, S.; Fortineau, N.; Dortet, L.; Naas, T. Evaluation of the CRE and ESBL ELITe MGB(R) kits for the accurate detection of carbapenemase- or CTX-M-producing bacteria. Diagn. Microbiol. Infect. Dis. 2018, 92, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Oueslati, S.; Girlich, D.; Dortet, L.; Naas, T. Evaluation of the Amplidiag CarbaR+VRE Kit for Accurate Detection of Carbapenemase-Producing Bacteria. J. Clin. Microbiol. 2018, 56, e01092-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girlich, D.; Bernabeu, S.; Grosperrin, V.; Langlois, I.; Begasse, C.; Arangia, N.; Creton, E.; Cotellon, G.; Sauvadet, A.; Dortet, L.; et al. Evaluation of the Amplidiag CarbaR+MCR Kit for Accurate Detection of Carbapenemase-Producing and Colistin-Resistant Bacteria. J. Clin. Microbiol. 2019, 57, e01800-18. [Google Scholar] [CrossRef] [Green Version]
- Dortet, L.; Fusaro, M.; Naas, T. Improvement of the Xpert Carba-R Kit for the Detection of Carbapenemase-Producing Enterobacteriaceae. Antimicrob. Agents Chemother. 2016, 60, 3832–3837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tojo, M.; Fujita, T.; Ainoda, Y.; Nagamatsu, M.; Hayakawa, K.; Mezaki, K.; Sakurai, A.; Masui, Y.; Yazaki, H.; Takahashi, H.; et al. Evaluation of an automated rapid diagnostic assay for detection of Gram-negative bacteria and their drug-resistance genes in positive blood cultures. PLoS ONE 2014, 9, e94064. [Google Scholar] [CrossRef] [PubMed]
- Verroken, A.; Despas, N.; Rodriguez-Villalobos, H.; Laterre, P.F. The impact of a rapid molecular identification test on positive blood cultures from critically ill with bacteremia: A pre-post intervention study. PLoS ONE 2019, 14, e0223122. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, T.M.; Juang, P.; Weaver, K.; Kollef, M.H.; Betthauser, K.D. Outcomes of Macrolide Deescalation in Severe Community-acquired Pneumonia. Clin. Ther. 2019, 41, 2540–2548. [Google Scholar] [CrossRef]
- Huang, T.D.; Melnik, E.; Bogaerts, P.; Evrard, S.; Glupczynski, Y. Evaluation of the ePlex Blood Culture Identification Panels for Detection of Pathogens in Bloodstream Infections. J. Clin. Microbiol. 2019, 57, e01597-18. [Google Scholar] [CrossRef] [Green Version]
- Burrack-Lange, S.C.; Personne, Y.; Huber, M.; Winkler, E.; Weile, J.; Knabbe, C.; Gorig, J.; Rohde, H. Multicenter assessment of the rapid Unyvero Blood Culture molecular assay. J. Med. Microbiol. 2018, 67, 1294–1301. [Google Scholar] [CrossRef] [PubMed]
- Kaase, M.; Szabados, F.; Wassill, L.; Gatermann, S.G. Detection of carbapenemases in Enterobacteriaceae by a commercial multiplex PCR. J. Clin. Microbiol. 2012, 50, 3115–3118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceyssens, P.J.; Garcia-Graells, C.; Fux, F.; Botteldoorn, N.; Mattheus, W.; Wuyts, V.; De Keersmaecker, S.; Dierick, K.; Bertrand, S. Development of a Luminex xTAG(R) assay for cost-effective multiplex detection of beta-lactamases in Gram-negative bacteria. J. Antimicrob. Chemother. 2016, 71, 2479–2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogaerts, P.; Hamels, S.; de Mendonca, R.; Huang, T.D.; Roisin, S.; Remacle, J.; Markine-Goriaynoff, N.; de Longueville, F.; Pluster, W.; Denis, O.; et al. Analytical validation of a novel high multiplexing real-time PCR array for the identification of key pathogens causative of bacterial ventilator-associated pneumonia and their associated resistance genes. J. Antimicrob. Chemother. 2013, 68, 340–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashton, P.M.; Nair, S.; Dallman, T.; Rubino, S.; Rabsch, W.; Mwaigwisya, S.; Wain, J.; O’Grady, J. MinION nanopore sequencing identifies the position and structure of a bacterial antibiotic resistance island. Nat. Biotechnol. 2015, 33, 296–300. [Google Scholar] [CrossRef] [Green Version]
- Reglier-Poupet, H.; Naas, T.; Carrer, A.; Cady, A.; Adam, J.M.; Fortineau, N.; Poyart, C.; Nordmann, P. Performance of chromID ESBL, a chromogenic medium for detection of Enterobacteriaceae producing extended-spectrum beta-lactamases. J. Med. Microbiol. 2008, 57, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.D.; Bogaerts, P.; Berhin, C.; Guisset, A.; Glupczynski, Y. Evaluation of Brilliance ESBL agar, a novel chromogenic medium for detection of extended-spectrum-beta- lactamase-producing Enterobacteriaceae. J. Clin. Microbiol. 2010, 48, 2091–2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grohs, P.; Tillecovidin, B.; Caumont-Prim, A.; Carbonnelle, E.; Day, N.; Podglajen, I.; Gutmann, L. Comparison of five media for detection of extended-spectrum Beta-lactamase by use of the wasp instrument for automated specimen processing. J. Clin. Microbiol. 2013, 51, 2713–2716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kluytmans-van den Bergh, M.F.; Verhulst, C.; Willemsen, L.E.; Verkade, E.; Bonten, M.J.; Kluytmans, J.A. Rectal Carriage of Extended-Spectrum-Beta-Lactamase-Producing Enterobacteriaceae in Hospitalized Patients: Selective Preenrichment Increases Yield of Screening. J. Clin. Microbiol. 2015, 53, 2709–2712. [Google Scholar] [CrossRef] [Green Version]
- Jazmati, N.; Hein, R.; Hamprecht, A. Use of an Enrichment Broth Improves Detection of Extended-Spectrum-Beta-Lactamase-Producing Enterobacteriaceae in Clinical Stool Samples. J. Clin. Microbiol. 2016, 54, 467–470. [Google Scholar] [CrossRef] [Green Version]
- Jazmati, N.; Jazmati, T.; Hamprecht, A. Importance of pre-enrichment for detection of third-generation cephalosporin-resistant Enterobacteriaceae (3GCREB) from rectal swabs. Eur J. Clin. Microbiol. Infect. Dis. 2017, 36, 1847–1851. [Google Scholar] [CrossRef] [PubMed]
- Farber, J.; Moder, K.A.; Layer, F.; Tammer, I.; Konig, W.; Konig, B. Extended-spectrum Beta-lactamase detection with different panels for automated susceptibility testing and with a chromogenic medium. J. Clin. Microbiol. 2008, 46, 3721–3727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiegand, I.; Geiss, H.K.; Mack, D.; Sturenburg, E.; Seifert, H. Detection of extended-spectrum beta-lactamases among Enterobacteriaceae by use of semiautomated microbiology systems and manual detection procedures. J. Clin. Microbiol. 2007, 45, 1167–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinar, M.J.; Rocha, R.; Ribeiro, M.; Goncalves Rodrigues, A.; Pina-Vaz, C. Extended-spectrum beta-lactamases of Escherichia coli and Klebsiella pneumoniae screened by the VITEK 2 system. J. Med. Microbiol. 2011, 60, 756–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, M.; Gatermann, S.; Pfeifer, Y.; Reischl, U.; Gessner, A.; Jantsch, J. Evaluation of the automated BD Phoenix CPO Detect panel in combination with the beta-CARBA assay for detection and classification of carbapenemase-producing Enterobacterales. J. Microbiol. Methods 2019, 156, 29–33. [Google Scholar] [CrossRef]
- Jonas, D.; Reuter, S.; Klassen, S.; Weber, S.; Buck, M.; Giani, T.; Rossolini, G.M.; Grundmann, H. Evaluation of the BD Phoenix CPO detect panel for prediction of Ambler class carbapenemases. Sci. Rep. 2021, 11, 13150. [Google Scholar] [CrossRef]
- He, Q.; Chen, W.; Huang, L.; Lin, Q.; Zhang, J.; Liu, R.; Li, B. Performance evaluation of three automated identification systems in detecting carbapenem-resistant Enterobacteriaceae. Ann. Clin. Microbiol. Antimicrob. 2016, 15, 40. [Google Scholar] [CrossRef] [Green Version]
- EUCAST. EUCAST Guidelines for Detection of Resistance Mechanisms and Specific Resistances of Clinical and/or Epidemiological Importance. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Resistance_mechanisms/EUCAST_detection_of_resistance_mechanisms_170711.pdf (accessed on 12 August 2021).
- Drieux, L.; Brossier, F.; Sougakoff, W.; Jarlier, V. Phenotypic detection of extended-spectrum beta-lactamase production in Enterobacteriaceae: Review and bench guide. Clin. Microbiol. Infect. 2008, 14 (Suppl. 1), 90–103. [Google Scholar] [CrossRef] [Green Version]
- Kaur, J.; Chopra, S.; Sheevani, G.M. Modified Double Disc Synergy Test to Detect ESBL Production in Urinary Isolates of Escherichia coli and Klebsiella pneumoniae. J. Clin. Diagn Res. 2013, 7, 229–233. [Google Scholar] [CrossRef]
- Doi, Y.; Potoski, B.A.; Adams-Haduch, J.M.; Sidjabat, H.E.; Pasculle, A.W.; Paterson, D.L. Simple disk-based method for detection of Klebsiella pneumoniae carbapenemase-type beta-lactamase by use of a boronic acid compound. J. Clin. Microbiol. 2008, 46, 4083–4086. [Google Scholar] [CrossRef] [Green Version]
- Giske, C.G.; Gezelius, L.; Samuelsen, O.; Warner, M.; Sundsfjord, A.; Woodford, N. A sensitive and specific phenotypic assay for detection of metallo-beta-lactamases and KPC in Klebsiella pneumoniae with the use of meropenem disks supplemented with aminophenylboronic acid, dipicolinic acid and cloxacillin. Clin. Microbiol. Infect. 2011, 17, 552–556. [Google Scholar] [CrossRef] [Green Version]
- Tsakris, A.; Poulou, A.; Bogaerts, P.; Dimitroulia, E.; Pournaras, S.; Glupczynski, Y. Evaluation of a new phenotypic OXA-48 disk test for differentiation of OXA-48 carbapenemase-producing Enterobacteriaceae clinical isolates. J. Clin. Microbiol. 2015, 53, 1245–1251. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.D.; Poirel, L.; Bogaerts, P.; Berhin, C.; Nordmann, P.; Glupczynski, Y. Temocillin and piperacillin/tazobactam resistance by disc diffusion as antimicrobial surrogate markers for the detection of carbapenemase-producing Enterobacteriaceae in geographical areas with a high prevalence of OXA-48 producers. J. Antimicrob. Chemother. 2014, 69, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, K.; Voets, G.M.; Scharringa, J.; Voskuil, S.; Fluit, A.C.; Rottier, W.C.; Leverstein-Van Hall, M.A.; Cohen Stuart, J.W. A disc diffusion assay for detection of class A, B and OXA-48 carbapenemases in Enterobacteriaceae using phenyl boronic acid, dipicolinic acid and temocillin. Clin. Microbiol. Infect. 2014, 20, 345–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, K.M.; Pike, R.; Winstanley, T.G.; Lanyon, C.; Cummings, S.P.; Raza, M.W.; Woodford, N.; Perry, J.D. Use of faropenem as an indicator of carbapenemase activity in the Enterobacteriaceae. J. Clin. Microbiol. 2013, 51, 1881–1886. [Google Scholar] [CrossRef] [Green Version]
- Koroska, F.; Gottig, S.; Kaase, M.; Steinmann, J.; Gatermann, S.; Sommer, J.; Wille, T.; Plum, G.; Hamprecht, A. Comparison of Phenotypic Tests and an Immunochromatographic Assay and Development of a New Algorithm for Detection of OXA-48-like Carbapenemases. J. Clin. Microbiol. 2017, 55, 877–883. [Google Scholar] [CrossRef] [Green Version]
- CLSI. The Modified Hodge Test for Suspected Carbapenemase Production in Enterobacteriaceae. Available online: https://clsi.org/media/1899/_m100_archived_methods_table.pdf (accessed on 12 August 2021).
- CLSI. M100 Performance Standards for Antimicrobial Susceptibility Testing. Available online: https://clsi.org/standards/products/microbiology/documents/m100/ (accessed on 12 August 2021).
- Bianco, G.; Boattini, M.; Iannaccone, M.; Fossati, L.; Cavallo, R.; Costa, C. Direct Beta-Lactam Inactivation Method: A New Low-Cost Assay for Rapid Detection of Carbapenemase- or Extended-Spectrum-beta-Lactamase-Producing Enterobacterales Directly from Positive Blood Culture Bottles. J. Clin. Microbiol. 2019, 58, e01178-19. [Google Scholar] [CrossRef]
- Camelena, F.; Cointe, A.; Mathy, V.; Hobson, C.; Doit, C.; Bercot, B.; Decre, D.; Podglajen, I.; Dortet, L.; Monjault, A.; et al. Within-a-Day Detection and Rapid Characterization of Carbapenemase by Use of a New Carbapenem Inactivation Method-Based Test, CIMplus. J. Clin. Microbiol. 2018, 56, e00137-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sfeir, M.M.; Hayden, J.A.; Fauntleroy, K.A.; Mazur, C.; Johnson, J.K.; Simner, P.J.; Das, S.; Satlin, M.J.; Jenkins, S.G.; Westblade, L.F. EDTA-Modified Carbapenem Inactivation Method: A Phenotypic Method for Detecting Metallo-beta-Lactamase-Producing Enterobacteriaceae. J. Clin. Microbiol. 2019, 57, e01757-18. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, P.; Dortet, L.; Poirel, L. Rapid detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceae. J. Clin. Microbiol. 2012, 50, 3016–3022. [Google Scholar] [CrossRef] [Green Version]
- Poirel, L.; Fernandez, J.; Nordmann, P. Comparison of Three Biochemical Tests for Rapid Detection of Extended-Spectrum-beta-Lactamase-Producing Enterobacteriaceae. J. Clin. Microbiol. 2016, 54, 423–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallah, S.; Decre, D.; Genel, N.; Arlet, G. The beta-Lacta test for direct detection of extended-spectrum-beta-lactamase-producing Enterobacteriaceae in urine. J. Clin. Microbiol. 2014, 52, 3792–3794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordmann, P.; Poirel, L.; Dortet, L. Rapid detection of carbapenemase-producing Enterobacteriaceae. Emerg Infect. Dis. 2012, 18, 1503–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dortet, L.; Poirel, L.; Nordmann, P. Rapid identification of carbapenemase types in Enterobacteriaceae and Pseudomonas spp. by using a biochemical test. Antimicrob. Agents Chemother. 2012, 56, 6437–6440. [Google Scholar] [CrossRef] [Green Version]
- Tijet, N.; Boyd, D.; Patel, S.N.; Mulvey, M.R.; Melano, R.G. Evaluation of the Carba NP test for rapid detection of carbapenemase-producing Enterobacteriaceae and Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2013, 57, 4578–4580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazin, M.; Paasch, F.; Goossens, H.; Malhotra-Kumar, S.; Mosar, W.P.; Teams, S.W.S. Current trends in culture-based and molecular detection of extended-spectrum-beta-lactamase-harboring and carbapenem-resistant Enterobacteriaceae. J. Clin. Microbiol. 2012, 50, 1140–1146. [Google Scholar] [CrossRef] [Green Version]
- Dallenne, C.; Da Costa, A.; Decre, D.; Favier, C.; Arlet, G. Development of a set of multiplex PCR assays for the detection of genes encoding important beta-lactamases in Enterobacteriaceae. J. Antimicrob. Chemother. 2010, 65, 490–495. [Google Scholar] [CrossRef] [Green Version]
- Roschanski, N.; Fischer, J.; Guerra, B.; Roesler, U. Development of a multiplex real-time PCR for the rapid detection of the predominant beta-lactamase genes CTX-M, SHV, TEM and CIT-type AmpCs in Enterobacteriaceae. PLoS ONE 2014, 9, e100956. [Google Scholar] [CrossRef]
- Chavda, K.D.; Satlin, M.J.; Chen, L.; Manca, C.; Jenkins, S.G.; Walsh, T.J.; Kreiswirth, B.N. Evaluation of a Multiplex PCR Assay to Rapidly Detect Enterobacteriaceae with a Broad Range of beta-Lactamases Directly from Perianal Swabs. Antimicrob. Agents Chemother. 2016, 60, 6957–6961. [Google Scholar] [CrossRef] [Green Version]
- Ogutu, J.O.; Zhang, Q.; Huang, Y.; Yan, H.; Su, L.; Gao, B.; Zhang, W.; Zhao, J.; Cai, W.; Li, W.; et al. Development of a multiplex PCR system and its application in detection of blaSHV, blaTEM, blaCTX-M-1, blaCTX-M-9 and blaOXA-1 group genes in clinical Klebsiella pneumoniae and Escherichia coli strains. J. Antibiot. 2015, 68, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Souverein, D.; Euser, S.M.; van der Reijden, W.A.; Herpers, B.L.; Kluytmans, J.; Rossen, J.W.A.; Den Boer, J.W. Clinical sensitivity and specificity of the Check-Points Check-Direct ESBL Screen for BD MAX, a real-time PCR for direct ESBL detection from rectal swabs. J. Antimicrob. Chemother. 2017, 72, 2512–2518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, H.-S.; Lee, M. Verification of the performance of the BD MAX Check-Points CPO Assay on clinical isolates. J. Lab. Med. 2020, 44, 165–168. [Google Scholar] [CrossRef]
- Cunningham, S.A.; Vasoo, S.; Patel, R. Evaluation of the Check-Points Check MDR CT103 and CT103 XL Microarray Kits by Use of Preparatory Rapid Cell Lysis. J. Clin. Microbiol. 2016, 54, 1368–1371. [Google Scholar] [CrossRef] [Green Version]
- Ko, Y.J.; Kim, J.; Kim, H.N.; Yoon, S.Y.; Lim, C.S.; Lee, C.K. Diagnostic performance of the Xpert Carba-R assay for active surveillance of rectal carbapenemase-producing organisms in intensive care unit patients. Antimicrob. Resist. Infect. Control 2019, 8, 127. [Google Scholar] [CrossRef] [PubMed]
- Traczewski, M.M.; Carretto, E.; Canton, R.; Moore, N.M.; Carba, R.S.T. Multicenter Evaluation of the Xpert Carba-R Assay for Detection of Carbapenemase Genes in Gram-Negative Isolates. J. Clin. Microbiol. 2018, 56, e00272-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, N.M.; Canton, R.; Carretto, E.; Peterson, L.R.; Sautter, R.L.; Traczewski, M.M.; Carba, R.S.T. Rapid Identification of Five Classes of Carbapenem Resistance Genes Directly from Rectal Swabs by Use of the Xpert Carba-R Assay. J. Clin. Microbiol. 2017, 55, 2268–2275. [Google Scholar] [CrossRef] [Green Version]
- Zalas-Wiecek, P.; Gospodarek-Komkowska, E.; Smalczewska, A. Rapid Detection of Genes Encoding Extended-Spectrum Beta-Lactamase and Carbapenemase in Clinical Escherichia coli Isolates with eazyplex SuperBug CRE System. Microb. Drug Resist. 2020, 26, 1245–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekowska, A.; Bogiel, T.; Gospodarek-Komkowska, E. Evaluation of eazyplex((R)) SuperBug CRE Test for Beta-Lactamase Genes Detection in Klebsiella spp. and P. aeruginosa Strains. Curr. Microbiol. 2020, 77, 99–103. [Google Scholar] [CrossRef] [Green Version]
- Findlay, J.; Hopkins, K.L.; Meunier, D.; Woodford, N. Evaluation of three commercial assays for rapid detection of genes encoding clinically relevant carbapenemases in cultured bacteria. J. Antimicrob. Chemother. 2015, 70, 1338–1342. [Google Scholar] [CrossRef] [Green Version]
- Hinic, V.; Ziegler, J.; Straub, C.; Goldenberger, D.; Frei, R. Extended-spectrum beta-lactamase (ESBL) detection directly from urine samples with the rapid isothermal amplification-based eazyplex(R) SuperBug CRE assay: Proof of concept. J. Microbiol. Methods 2015, 119, 203–205. [Google Scholar] [CrossRef]
- Bernabeu, S.; Ratnam, K.C.; Boutal, H.; Gonzalez, C.; Vogel, A.; Devilliers, K.; Plaisance, M.; Oueslati, S.; Malhotra-Kumar, S.; Dortet, L.; et al. A Lateral Flow Immunoassay for the Rapid Identification of CTX-M-Producing Enterobacterales from Culture Plates and Positive Blood Cultures. Diagnostics 2020, 10, 764. [Google Scholar] [CrossRef]
- Cointe, A.; Bonacorsi, S.; Truong, J.; Hobson, C.; Doit, C.; Monjault, A.; Bidet, P.; Birgy, A. Detection of Carbapenemase-Producing Enterobacteriaceae in Positive Blood Culture Using an Immunochromatographic RESIST-4 O.K.N.V. Assay. Antimicrob. Agents Chemother. 2018, 62, e01828-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianco, G.; Boattini, M.; Iannaccone, M.; Bondi, A.; Ghibaudo, D.; Zanotto, E.; Peradotto, M.; Cavallo, R.; Costa, C. Carbapenemase detection testing in the era of ceftazidime/avibactam-resistant KPC-producing Enterobacterales: A 2-year experience. J. Glob. Antimicrob. Resist. 2021, 24, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Saleh, A.; Gottig, S.; Hamprecht, A.G. Multiplex Immunochromatographic Detection of OXA-48, KPC, and NDM Carbapenemases: Impact of Inoculum, Antibiotics, and Agar. J. Clin. Microbiol. 2018, 56, e00050-18. [Google Scholar] [CrossRef] [Green Version]
- Boattini, M.; Bianco, G.; Iannaccone, M.; Ghibaudo, D.; Almeida, A.; Cavallo, R.; Costa, C. Fast-track identification of CTX-M-extended-spectrum-beta-lactamase- and carbapenemase-producing Enterobacterales in bloodstream infections: Implications on the likelihood of deduction of antibiotic susceptibility in emergency and internal medicine departments. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1495–1501. [Google Scholar] [CrossRef]
- Bogaerts, P.; Oueslati, S.; Meunier, D.; Nonhoff, C.; Yunus, S.; Massart, M.; Denis, O.; Woodford, N.; Hopkins, K.L.; Naas, T.; et al. Multicentre evaluation of the BYG Carba v2.0 test, a simplified electrochemical assay for the rapid laboratory detection of carbapenemase-producing Enterobacteriaceae. Sci. Rep. 2017, 7, 9937. [Google Scholar] [CrossRef] [Green Version]
- Rochelet, M.; Solanas, S.; Betelli, L.; Neuwirth, C.; Vienney, F.; Hartmann, A. Amperometric detection of extended-spectrum beta-lactamase activity: Application to the characterization of resistant E. coli strains. Analyst 2015, 140, 3551–3556. [Google Scholar] [CrossRef] [PubMed]
- Feucherolles, M.; Cauchie, H.M.; Penny, C. MALDI-TOF Mass Spectrometry and Specific Biomarkers: Potential New Key for Swift Identification of Antimicrobial Resistance in Foodborne Pathogens. Microorganisms 2019, 7, 593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florio, W.; Baldeschi, L.; Rizzato, C.; Tavanti, A.; Ghelardi, E.; Lupetti, A. Detection of Antibiotic-Resistance by MALDI-TOF Mass Spectrometry: An Expanding Area. Front. Cell Infect. Microbiol. 2020, 10, 572909. [Google Scholar] [CrossRef] [PubMed]
- Burckhardt, I.; Zimmermann, S. Using matrix-assisted laser desorption ionization-time of flight mass spectrometry to detect carbapenem resistance within 1 to 2.5 hours. J. Clin. Microbiol. 2011, 49, 3321–3324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hrabak, J.; Walkova, R.; Studentova, V.; Chudackova, E.; Bergerova, T. Carbapenemase activity detection by matrix-assisted laser desorption ionization-time of flight mass spectrometry. J. Clin. Microbiol. 2011, 49, 3222–3227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa-Martinez, C.L.; Idelevich, E.A.; Sparbier, K.; Kostrzewa, M.; Becker, K. Rapid Detection of Extended-Spectrum Beta-Lactamases (ESBL) and AmpC beta-Lactamases in Enterobacterales: Development of a Screening Panel Using the MALDI-TOF MS-Based Direct-on-Target Microdroplet Growth Assay. Front. Microbiol. 2019, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Huang, Y.; Lizou, Y.; Li, J.; Zhang, R. Evaluation of Staphylococcus aureus Subtyping Module for Methicillin-Resistant Staphylococcus aureus Detection Based on Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry. Front. Microbiol. 2019, 10, 2504. [Google Scholar] [CrossRef]
- Cordovana, M.; Kostrzewa, M.; Soki, J.; Witt, E.; Ambretti, S.; Pranada, A.B. Bacteroides fragilis: A whole MALDI-based workflow from identification to confirmation of carbapenemase production for routine laboratories. Anaerobe 2018, 54, 246–253. [Google Scholar] [CrossRef]
- Camara, J.E.; Hays, F.A. Discrimination between wild-type and ampicillin-resistant Escherichia coli by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Anal. Bioanal. Chem. 2007, 389, 1633–1638. [Google Scholar] [CrossRef]
- Figueroa-Espinosa, R.; Costa, A.; Cejas, D.; Barrios, R.; Vay, C.; Radice, M.; Gutkind, G.; Di Conza, J. MALDI-TOF MS based procedure to detect KPC-2 directly from positive blood culture bottles and colonies. J. Microbiol. Methods 2019, 159, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Yoon, E.J.; Lee, E.H.; Hwang, D.H.; Lee, H.; Baek, J.H.; Jeong, S.H. Direct detection of intact Klebsiella pneumoniae carbapenemases produced by Enterobacterales using MALDI-TOF MS. J. Antimicrob. Chemother. 2020, 75, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Cordovana, M.; Kostrzewa, M.; Glandorf, J.; Bienia, M.; Ambretti, S.; Pranada, A.B. A Full MALDI-Based Approach to Detect Plasmid-Encoded KPC-Producing Klebsiella pneumoniae. Front. Microbiol. 2018, 9, 2854. [Google Scholar] [CrossRef]
- Knight, G.M.; Dyakova, E.; Mookerjee, S.; Davies, F.; Brannigan, E.T.; Otter, J.A.; Holmes, A.H. Fast and expensive (PCR) or cheap and slow (culture)? A mathematical modelling study to explore screening for carbapenem resistance in UK hospitals. BMC Med. 2018, 16, 141. [Google Scholar] [CrossRef] [Green Version]
- Doern, C.D. The Confounding Role of Antimicrobial Stewardship Programs in Understanding the Impact of Technology on Patient Care. J. Clin. Microbiol. 2016, 54, 2420–2423. [Google Scholar] [CrossRef] [Green Version]
- Deurenberg, R.H.; Bathoorn, E.; Chlebowicz, M.A.; Couto, N.; Ferdous, M.; Garcia-Cobos, S.; Kooistra-Smid, A.M.; Raangs, E.C.; Rosema, S.; Veloo, A.C.; et al. Application of next generation sequencing in clinical microbiology and infection prevention. J. Biotechnol 2017, 243, 16–24. [Google Scholar] [CrossRef]
- Berglund, F.; Osterlund, T.; Boulund, F.; Marathe, N.P.; Larsson, D.G.J.; Kristiansson, E. Identification and reconstruction of novel antibiotic resistance genes from metagenomes. Microbiome 2019, 7, 52. [Google Scholar] [CrossRef] [PubMed]
- Ellington, M.J.; Ekelund, O.; Aarestrup, F.M.; Canton, R.; Doumith, M.; Giske, C.; Grundman, H.; Hasman, H.; Holden, M.T.G.; Hopkins, K.L.; et al. The role of whole genome sequencing in antimicrobial susceptibility testing of bacteria: Report from the EUCAST Subcommittee. Clin. Microbiol. Infect. 2017, 23, 2–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossen, J.W.A.; Friedrich, A.W.; Moran-Gilad, J.; on behalf ofthe ESCMID Study Group for Genomic and Molecular Diagnostics (ESGMD). Practical issues in implementing whole-genome-sequencing in routine diagnostic microbiology. Clin. Microbiol. Infect. 2018, 24, 355–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Ambler’s classification with examples of main β-lactamases in Enterobacterales.

Figure 2.
ESBL and carbapenemase detection by disc diffusion tests. Schematic overview of disc diffusion assay variations for detection of ESBL and carbapenemase-producing strains. (A) Principle of susceptibility testing by disc diffusion assay. (B) Modified Hodge test. (C) Combined disc test. (D) Double-disc synergy test. (E) β-lactam inactivation assay (e.g., CIM).
Figure 2.
ESBL and carbapenemase detection by disc diffusion tests. Schematic overview of disc diffusion assay variations for detection of ESBL and carbapenemase-producing strains. (A) Principle of susceptibility testing by disc diffusion assay. (B) Modified Hodge test. (C) Combined disc test. (D) Double-disc synergy test. (E) β-lactam inactivation assay (e.g., CIM).

Figure 3.
Principle of colorimetric assays for detection of ESBLs and carbapenemases. The test isolate is lysed and incubated in phenol red solution with an antibiotic. (a) If the test isolate is positive for ESBL/carbapenemase production, the enzyme hydrolyzes the antibiotic, resulting in a pH shift and a color change from magenta to yellow. (b) ESBL/carbapenemase-negative isolates do not induce a change in color. (c) Addition of enzyme-specific inhibitors prevents hydrolysis of the antibiotic, and no color change is visible.
Figure 3.
Principle of colorimetric assays for detection of ESBLs and carbapenemases. The test isolate is lysed and incubated in phenol red solution with an antibiotic. (a) If the test isolate is positive for ESBL/carbapenemase production, the enzyme hydrolyzes the antibiotic, resulting in a pH shift and a color change from magenta to yellow. (b) ESBL/carbapenemase-negative isolates do not induce a change in color. (c) Addition of enzyme-specific inhibitors prevents hydrolysis of the antibiotic, and no color change is visible.

Figure 4.
Basic principle of lateral flow assays. Schematic illustration of different zones of commercially available lateral flow assays for detection of, i.e., β-lactamases. Antigens within the sample migrate along the nitrocellulose membrane by capillary flow. Antigens (e.g., β-lactamase) conjugate with specific dye-labeled antibodies and are captured by immobilized antigen-specific antibodies, resulting in the visualization of the test line. Non-conjugated and unbound antibodies migrate further to the control line and are captured by immobilized anti-IgG antibodies, resulting in the visibility of a control line.
Figure 4.
Basic principle of lateral flow assays. Schematic illustration of different zones of commercially available lateral flow assays for detection of, i.e., β-lactamases. Antigens within the sample migrate along the nitrocellulose membrane by capillary flow. Antigens (e.g., β-lactamase) conjugate with specific dye-labeled antibodies and are captured by immobilized antigen-specific antibodies, resulting in the visualization of the test line. Non-conjugated and unbound antibodies migrate further to the control line and are captured by immobilized anti-IgG antibodies, resulting in the visibility of a control line.

Figure 5.
Algorithm for the detection of carbapenemases in routine laboratory as proposed by Baeza et al. * OXA-48-like KPC, VIM, NDM, (IMP). ** Multiplex PCR targeting rare carba-penemases (e.g., IMI, GES, etc.), whole genome sequencing, other tests [61].
Figure 5.
Algorithm for the detection of carbapenemases in routine laboratory as proposed by Baeza et al. * OXA-48-like KPC, VIM, NDM, (IMP). ** Multiplex PCR targeting rare carba-penemases (e.g., IMI, GES, etc.), whole genome sequencing, other tests [61].


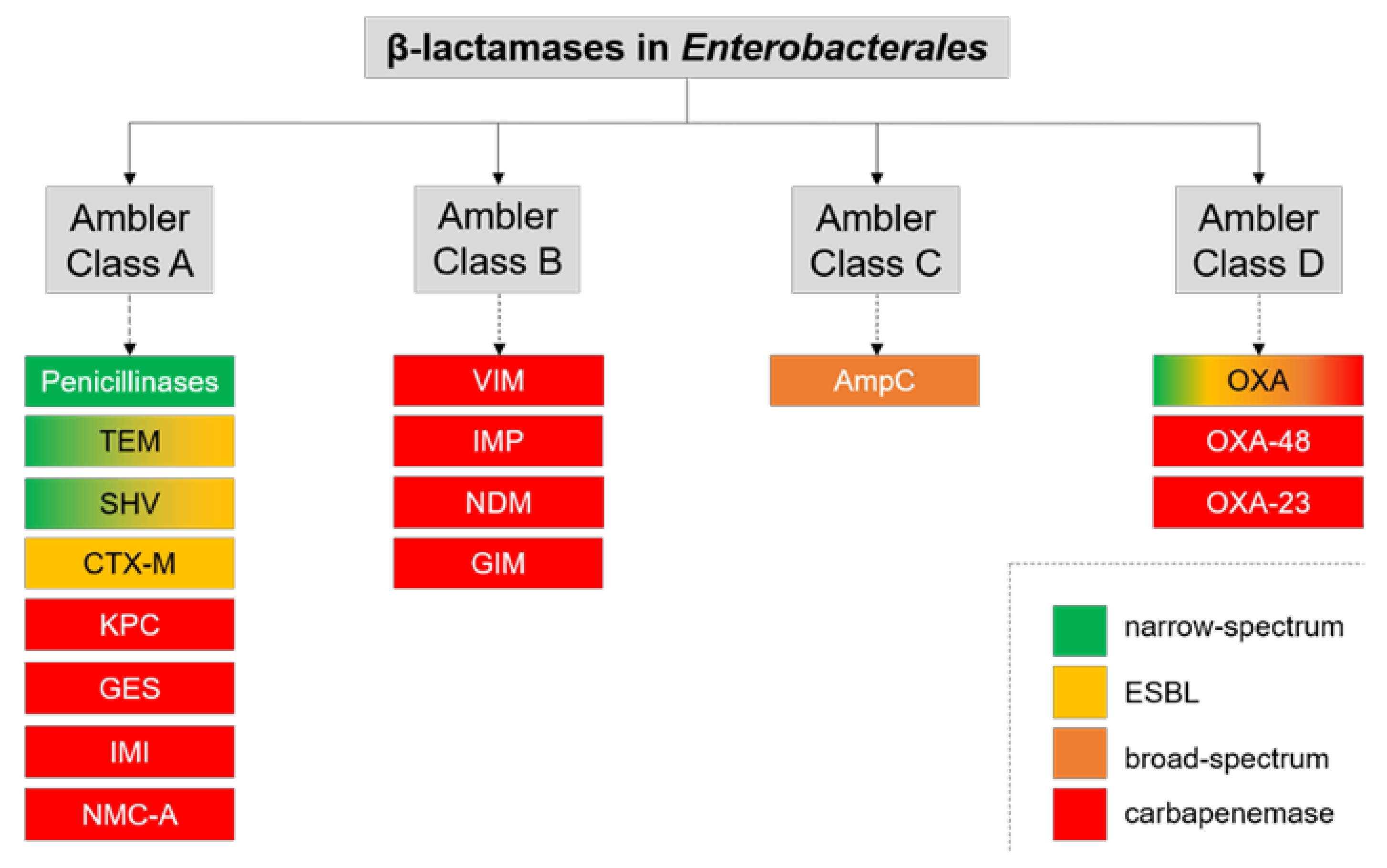{kind=link}
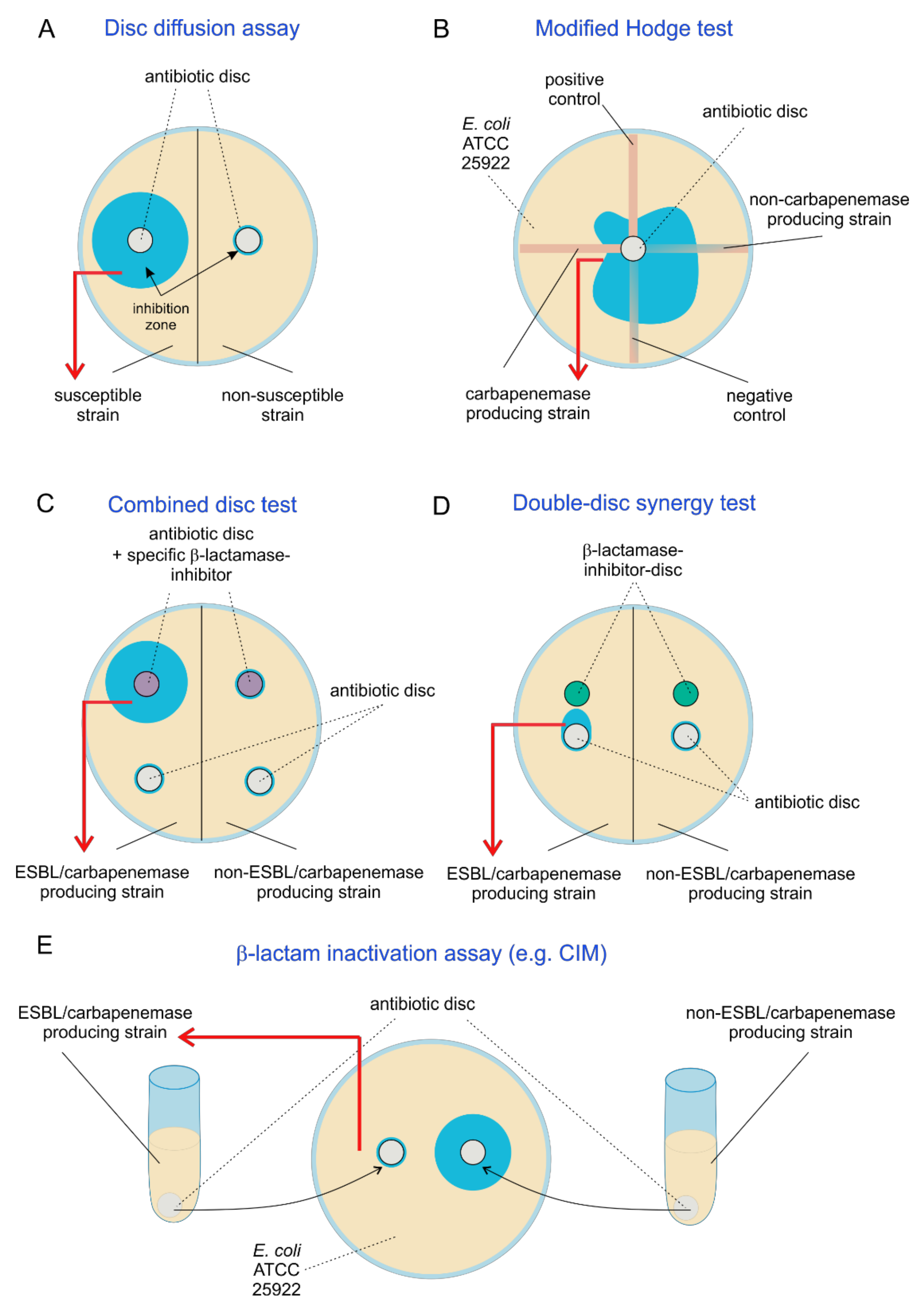{kind=link}
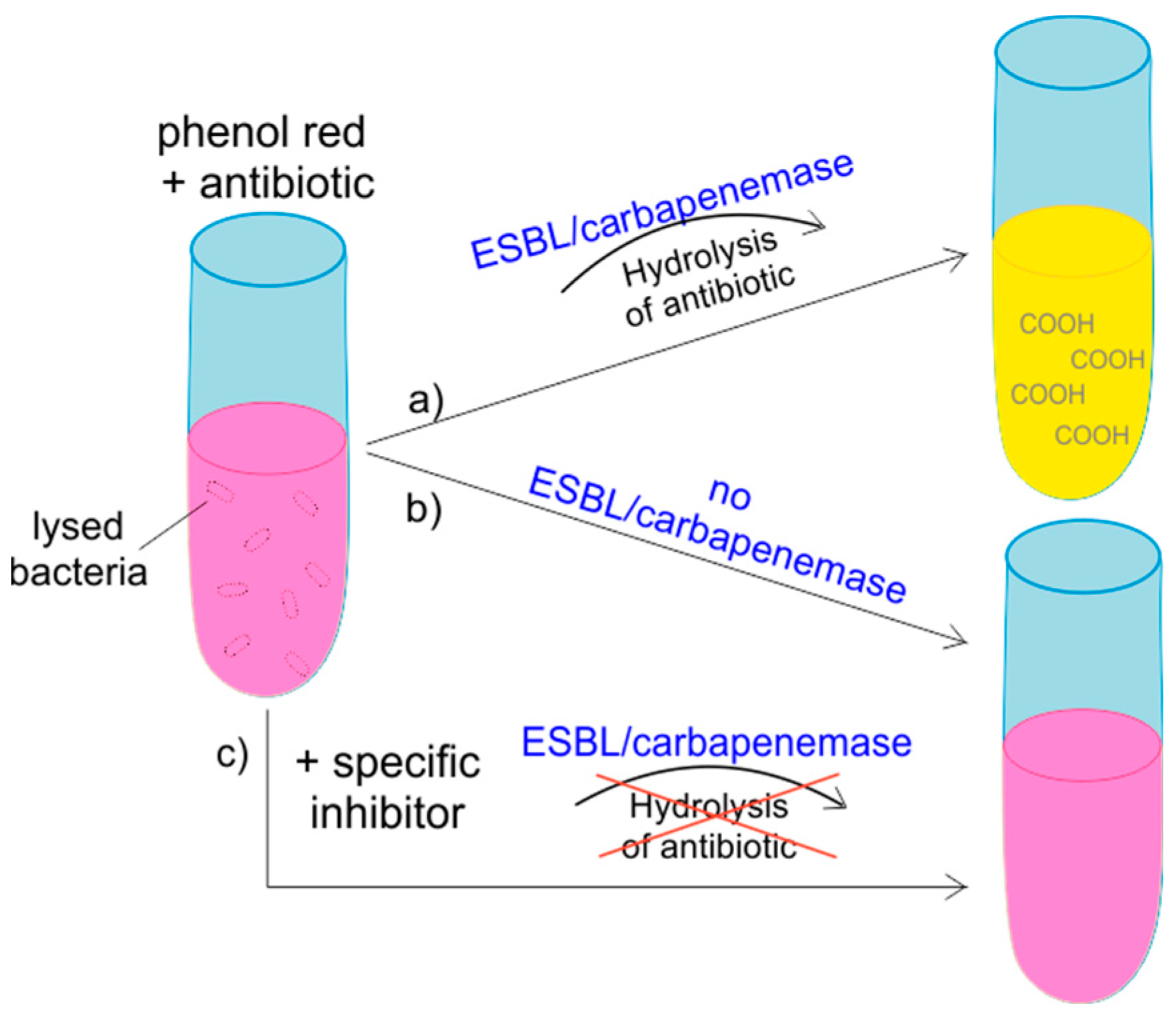{kind=link}
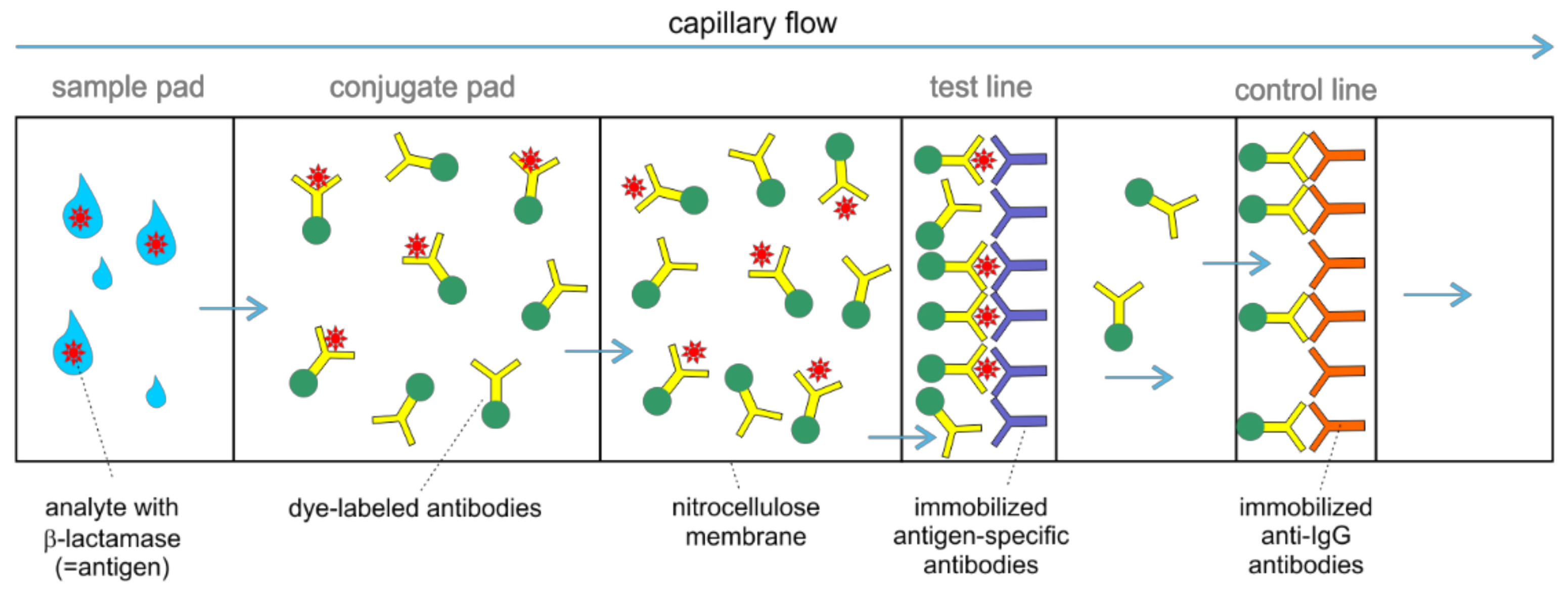{kind=link}
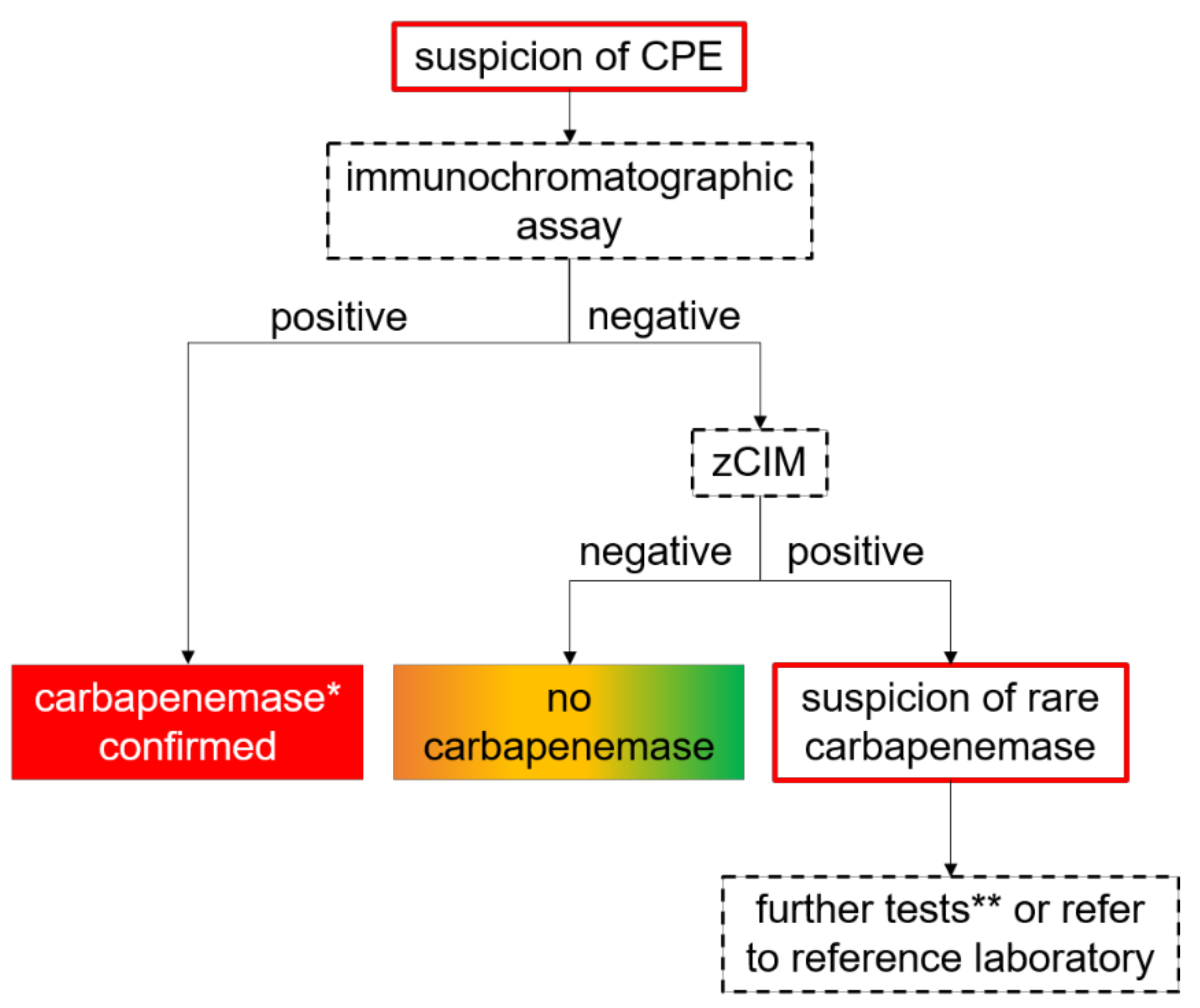{kind=link}
Table 1.
Overview of selected versions of carbapenemase detection methods available for Enterobacterales. Table modified from [46].
Table 1.
Overview of selected versions of carbapenemase detection methods available for Enterobacterales. Table modified from [46].
| Method | Test | Time to Result | Ease of Interpretation | Target Enzymes/ Genes | Sens. (%) | Spec. (%) | Tested on Clinical Specimens | Reference |
|---|---|---|---|---|---|---|---|---|
| Selective chromogenic/non-chromogenic agar | Brilliance CRE (Oxoid) | 18–48 h | easy | Classes A, B, D | 77.6–98.6 | 60–87.1 | bacterial colonies | [47,48] |
| Chromatic CRE (Liofilchem) | 18–48 h | easy | Classes A, B, D | 94.2 | 60 | bacterial colonies | [47] | |
| chromID CARBA (bioMérieux) | 18–48 h | easy | Classes A, B, D | 85.5–89.8 | 87.5–95 | bacterial colonies | [47,48] | |
| chromID OXA-48 (bioMérieux) | 18–48 h | easy | OXA-48 | 34.8 (all CPE) 100 (OXA-48) | 100 | bacterial colonies | [47] | |
| McConkey supplemented with ertapenem, cloxacillin, zinc-sulfate and ticarcillin | 24–48 h | easy | Classes A, B, D | 97.1 | 77.5 | bacterial colonies | [47] | |
| Disc diffusion and related assays | Mastdiscs TM Carbapenemase Detection Set (MAST GROUP) | 18–24 h | easy | Classes A, B | 78 | 93 | bacterial colonies | [49] |
| Combi Carba Plus Kit (MAST GROUP) | 18 h | easy | Classes A, B, D | 86 | 98 | bacterial colonies | [50] | |
| KPC/MBL & OXA-48 Confirm Kits (Rosco Diagnostica) | 18–24 h | subjective | Classes A, B, D | 86–98.8 | 93.1–98 | bacterial colonies | [50,51] | |
| KPC&MBL&OXA-48 disc kit (Liofilchem) | 18 h | Classes A, B, D | 96 | 87 | bacterial colonies | [50] | ||
| faropenem disc | 18 h | easy | Classes A, B, D | 99 | 81 | bacterial colonies | [50] | |
| Modified Hodge Test | 18–24 h | subjective | Classes A, B, D | 77.4 | 38.9 | bacterial colonies | [52] | |
| Carbapenem inactivation method (CIM) | 18–24 h | easy | Classes A, B, D | n.a. | n.a. | bacterial colonies | [53] | |
| mCIM | 18–24 h | subjective | Classes A, B, D | 97 | 99 | bacterial colonies | [54,55] | |
| zCIM | 18–24 | easy | Classes A, B, D | 97.4–98 | 97.7–100 | bacterial colonies | [50] | |
| bcCIM | 18–24 h | easy | Classes A, B, D | 100 | 100 | blood culture fluid | [56] | |
| rapid carbapenemase detection method (rCDM) | 5–6 h | easy | Classes A, B, D | 100 | 99.6 | bacterial colonies | [57] | |
| Colorimetric assays | Carba NP test | 5–120 min | subjective | Classes A, B, D | 97.9 | 100 | spiked blood cultures | [58] |
| bcCarba NP test | 5–120 min | subjective | Classes A, B, D | 99 | 95.1 | blood culture fluid | [56] | |
| Neo-Rapid CARB Screen (Rosco Diagnostica) | 15–120 min | subjective | Classes A, B, D | 89.5 | 70.9 | blood culture fluid, urine | [59] | |
| Neo-Rapid CARB from PBC | 90–120 min | subjective | Classes A, B, D | 99 | 91.4 | blood culture fluid | [56] | |
| Rapidec carba NP test (bioMérieux) | 5–120 min | subjective | Classes A, B, D | 99 | 100 | blood culture fluid | [59] | |
| β-CARBA test (Bio-Rad) | 30 min | subjective | Classes A, B, D | 64.9–84.9 | 90–95.6 | bacterial colonies | [60,61] | |
| β-CARBA test from PBC | 30 min | subjective | Classes A, B, D | 100 | 95.1 | blood culture fluid | [56] | |
| CARBA PAcE (MAST GROUP) | 10 min | subjective | Classes A, B, D | 72 | 91 | bacterial colonies | [62] | |
| Blue Carba test | 30–120 min | subjective | Classes A, B, D | 100 | 100 | bacterial cultures | [63] | |
| Rapid Carb Blue kit (Rosco Diagnostica) | 15-60 min | subjective | Classes A, B, D | 93.3 | 100 | blood culture fluid, urine | [64] | |
| CNPt-direct test | 2 h | subjective | Classes A, B, D | 98 | 100 | bacterial colonies | [65] | |
| Carba-H-assay | 2 h | subjective | Classes A, B, D | n.a. | n.a. | bacterial colonies, spiked urine samples | [66] | |
| Immunochromatographic assays | RESIST-3 O.K.N. assays (Coris BioConcept) | 20–45 min | easy | KPC, NDM, OXA-48-like | 100 | 100 | blood culture fluid | [67] |
| RESIST-4 O.K.N.V. assays (Coris BioConcept) | 15 min | easy | KPC, NDM, VIM, OXA-48-like | 84.2–99.2 | 100 | bacterial colonies | [55,68] | |
| RESIST-5 O.O.K.N.V. assays (Coris BioConcept) | 15 min | easy | KPC, NDM, VIM, OXA-48-like, OXA-163 | 99.4 | 100 | bacterial colonies | [69] | |
| NG-Test Carba 5 (NG Biotech) from PBC | 30 min | easy | KPC, NDM, VIM, OXA-48-like, IMP | 97.7 | 96.1 | blood culture fluid | [70] | |
| NG-Test Carba 5 (NG Biotech) | 15 min | easy | KPC, NDM, VIM, OXA-48-like, IMP | 88.2–100 | 95.3–100 | bacterial colonies | [55,69,71,72] | |
| Mass spectrometry | MALDI-TOF MS | 4.5 h | complex | Classes A, B, D | 100 | 90 | blood culture fluid | [73] |
| MBT STAR-Carba IVD Kit (Bruker DALTONICS) | 30–60 min | moderate | mass shift of hydrolyzed carbapenem | 98–100 | 97–100 | bacterial colonies | [74,75,76,77] | |
| MBT STAR-Carba IVD Kit (Bruker DALTONICS) from PBC | 1 h | moderate | mass shift of hydrolyzed carbapenem | 100 | 100 | blood culture fluid | [76] | |
| Direct-on-target microdroplet growth assay (DOT MGA), RUO | 4–6 h | moderate | bacterial growth in presence of defined carbapenem concentration | 100 | 100 | bacterial colonies | [78] | |
| Direct-on-target microdroplet growth assay (DOT MGA), RUO, from PBC | 4–6 h | moderate | bacterial growth in presence of defined carbapenem concentration | 91.7 | 100 | blood culture fluid | [79] | |
| Electrochemical assay | BYG Carba test (not yet commercially available) | 5–30 min | easy | Classes A, B, D | 95 | 100 | bacterial colonies | [80] |
| BL-RED test (Coris BioConcept) | 20 min | easy | 3GC resistance by hydrolysis | 46.7 (83.8 for detection of class A β-lactamases) | 100 | blood culture fluid | [81] | |
| Other molecular methods | Eazyplex Superbug CRE (Amplex Diagnostics) | 15 min | easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like | 100 | 100 | blood culture fluid, rectal swab, urine | [82] |
| Multiplex PCR-based assays | BD MAX TM Check-Points CPO assay (Check Points) | <180 min | easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP | 97.1 | 98.8 | rectal swab | [83] |
| Check-MDR CT103 (Check Points) | 6 h | relatively easy | among others blaKPC2,3, blaNDM1,2,3, blaOXA-48, blaOXA-181, blaVIM1,2,3,4,19, blaIMP1,4,8,13 | 95–100 | 100 | DNA extracted from bacterial colonies | [84] | |
| CRE ELITe MGB ® kit (ELITechGroup) | <180 | easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP | 100 | 100 | PBC, rectal swab, respiratory sample | [85] | |
| Amplidiag ® CarbaR + VRE (Mobidiag Ltd.) | <180 min | relatively easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP, ISAba1-OXA-51, blaOXA-23, blaOXA-24/40, blaOXA-58 | 100 | 99 | DNA extracted from stool samples, rectal swab, pure culture | [86] | |
| Amplidiag ® CarbaR + MCR (Mobidiag Ltd.) | <180 min | relatively easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP, ISAba1-OXA-51, blaOXA-23, blaOXA-24/40, blaOXA-58, blaGES-2, blaGES4 throughblaGES-6, blaGES-13 throughblaGES-16, blaGES-18, blaGES-20/21, blaGES-24 | 92–100 | 86–100 | DNA extracted from stool samples, rectal swab, pure culture | [87] | |
| Xpert-Carba-R assay ® (Cepheid) | 50 min | easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP | 97.8 | 95.3 | rectal swab | [88] | |
| GenePOC/Revogene Carba C assay ® (Meridian) | 70 min | easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP | 100 | 100 | bacterial colonies | [46] | |
| Verigene BC-GN (Nanosphere) | 2–2.5 h | relatively easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP, blaOXA-23, blaOXA-24/40, blaOXA-58 | 100 | 100 | blood culture fluid | [89] | |
| Biofire ® Filmarray ® Blood Culture Identification (BCID) Panel (bioMérieux) | 1 h | easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP | n.a. | n.a. | blood culture fluid | [90] | |
| Biofire ® Filmarray ® Pneumonia plus Panel (bioMérieux) | 1 h | easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP | n.a. | n.a. | Respiratory specimen | [91] | |
| ePlex ® Blood Culture Identification Gram Negative Panel (GenMark) | 90 min | easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaOXA-23, blaIMP | n.a. | n.a. | blood culture fluid | [92] | |
| Unyvero (Curetis) | 4–5 h | relatively easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaOXA-23, blaOXA-24/40, blaOXA-58, blaIMP | n.a. | n.a. | sputum, tissue, bone fragment, pus, blood culture fluid | [93] | |
| Hyplex SuperBug ID test system (Amplex Diagnostics) | relatively easy | blaKPC, blaVIM, blaNDM, blaOXA-48-like, blaIMP | 96.7 | ≥99 | sputum, urine, blood culture fluid, swab specimens | [94] | ||
| Luminex xTAG ® assay (Luminex Corporation) | 5 h | relatively easy | blaKPC, blaVIM, blaNDM, blaIMI, blaGES, blaOXA-23, blaOXA-51, blaSEM, blaVEM, blaOXA-48-like, blaIMP | 100 | 99.4 | DNA extracted from bacterial colonies | [95] | |
| VAPChip ® (EppendorfArray Technologies) | 4 h | relatively easy | blaKPC, blaVIM, blaOXA-23, blaOXA-48-like, blaIMP, blaOXA-24/40, blaOXA-58 | 100 | 100 | Respiratory sample | [96] | |
| Next generation sequencing | MinION (Oxford Nanopore Technologies) | >8 h | complex | Classes A, B, D | 100 | 100 | extracted DNA | [97] |
PBC, positive blood culture; sens, sensitivity; spec, specificity; n.a., not available.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Noster, J.; Thelen, P.; Hamprecht, A. Detection of Multidrug-Resistant Enterobacterales—From ESBLs to Carbapenemases. Antibiotics 2021, 10, 1140. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091140
AMA Style
Noster J, Thelen P, Hamprecht A. Detection of Multidrug-Resistant Enterobacterales—From ESBLs to Carbapenemases. Antibiotics. 2021; 10(9):1140. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091140
Chicago/Turabian StyleNoster, Janina, Philipp Thelen, and Axel Hamprecht. 2021. "Detection of Multidrug-Resistant Enterobacterales—From ESBLs to Carbapenemases" Antibiotics 10, no. 9: 1140. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091140
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.