
An Overview of Antimicrobial Stewardship Optimization: The Use of Antibiotics in Humans and Animals to Prevent Resistance

 ,
,  , , , ,
, , , ,  ,
,  , and
, and 
Abstract
:1. Introduction
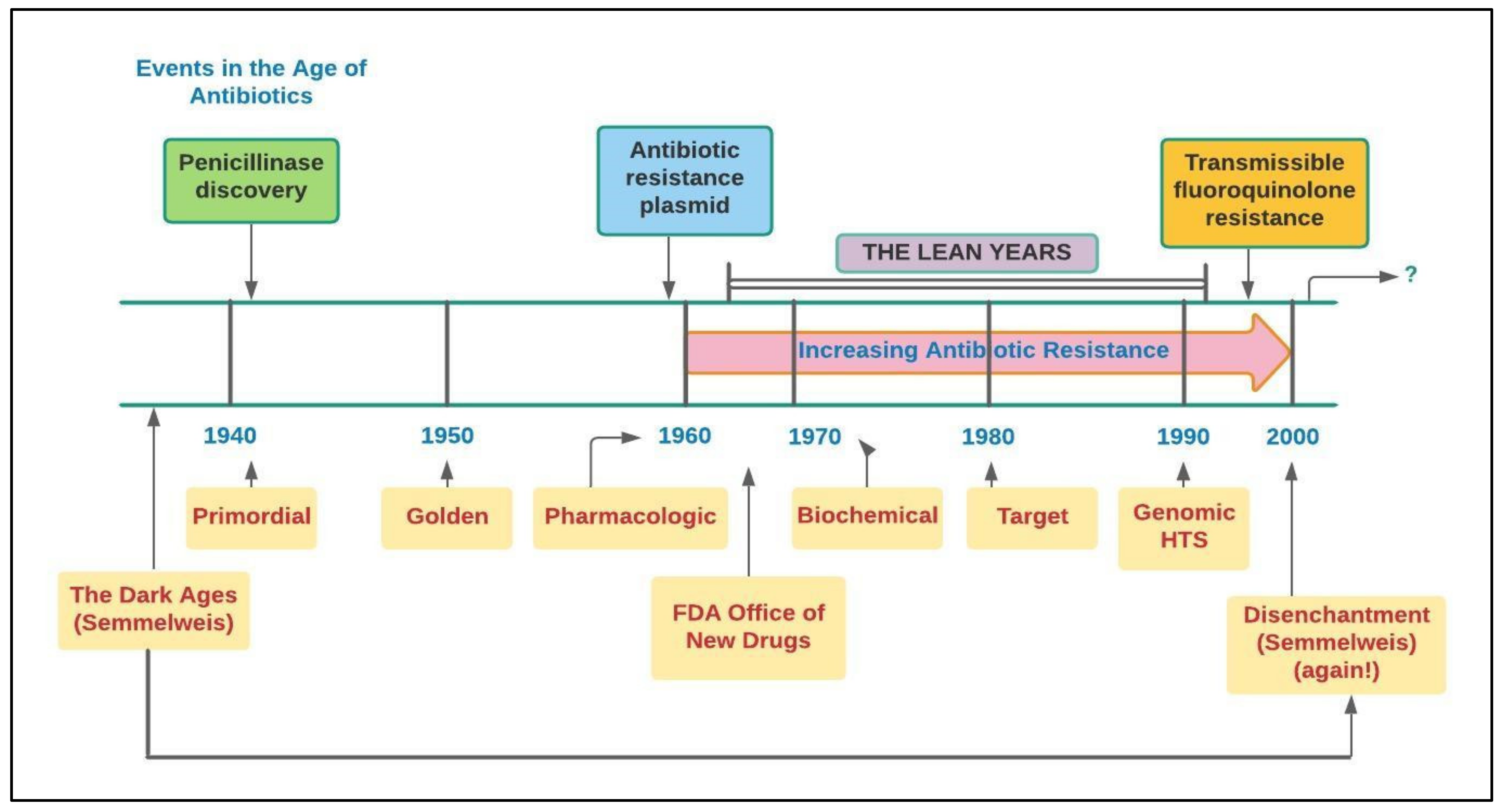
2. The Natural History of Antibiotics
3. Methodologies for Detecting the Human Gut Resistome
4. The Antibiotic Resistome
5. Resistance to Antibiotics
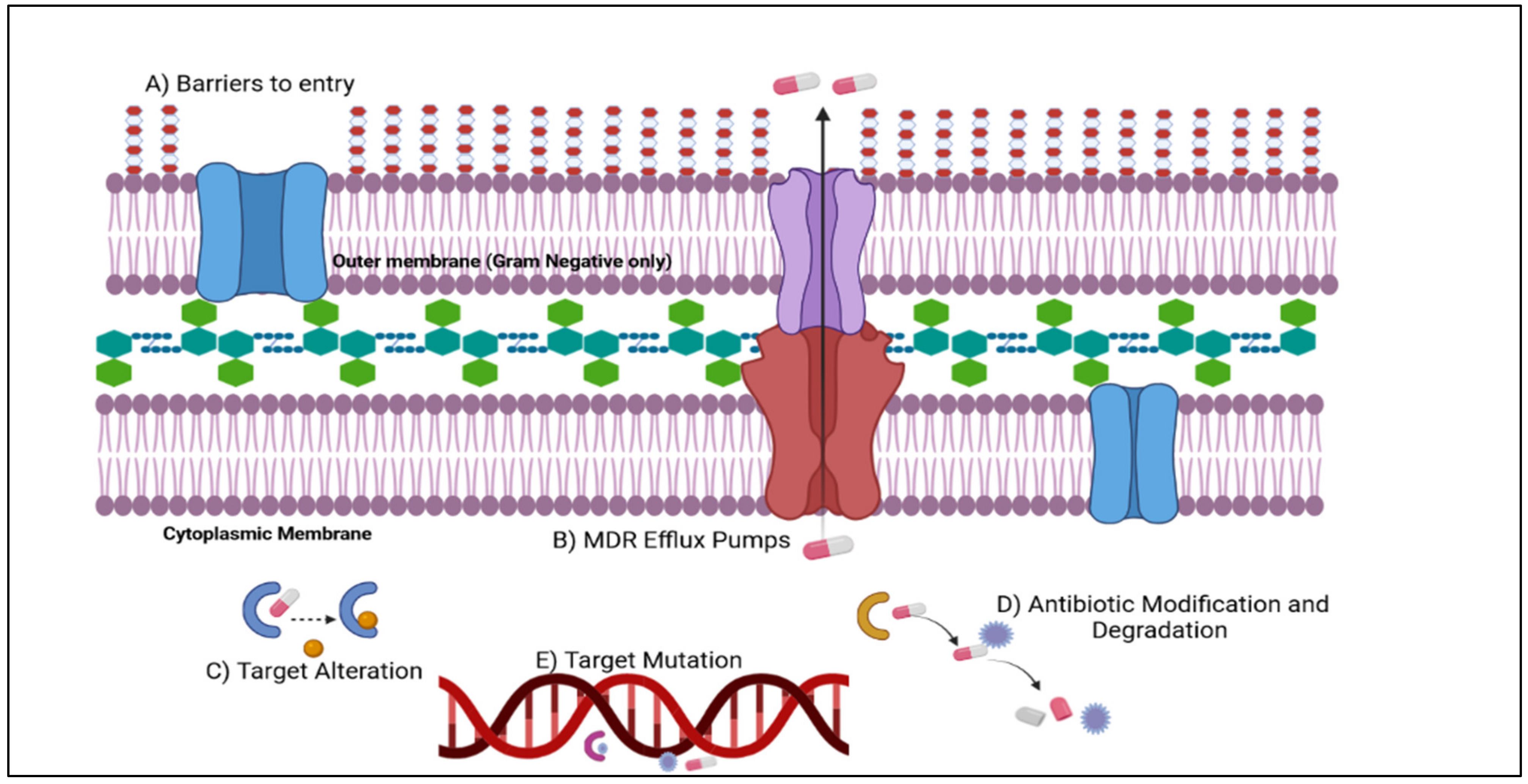
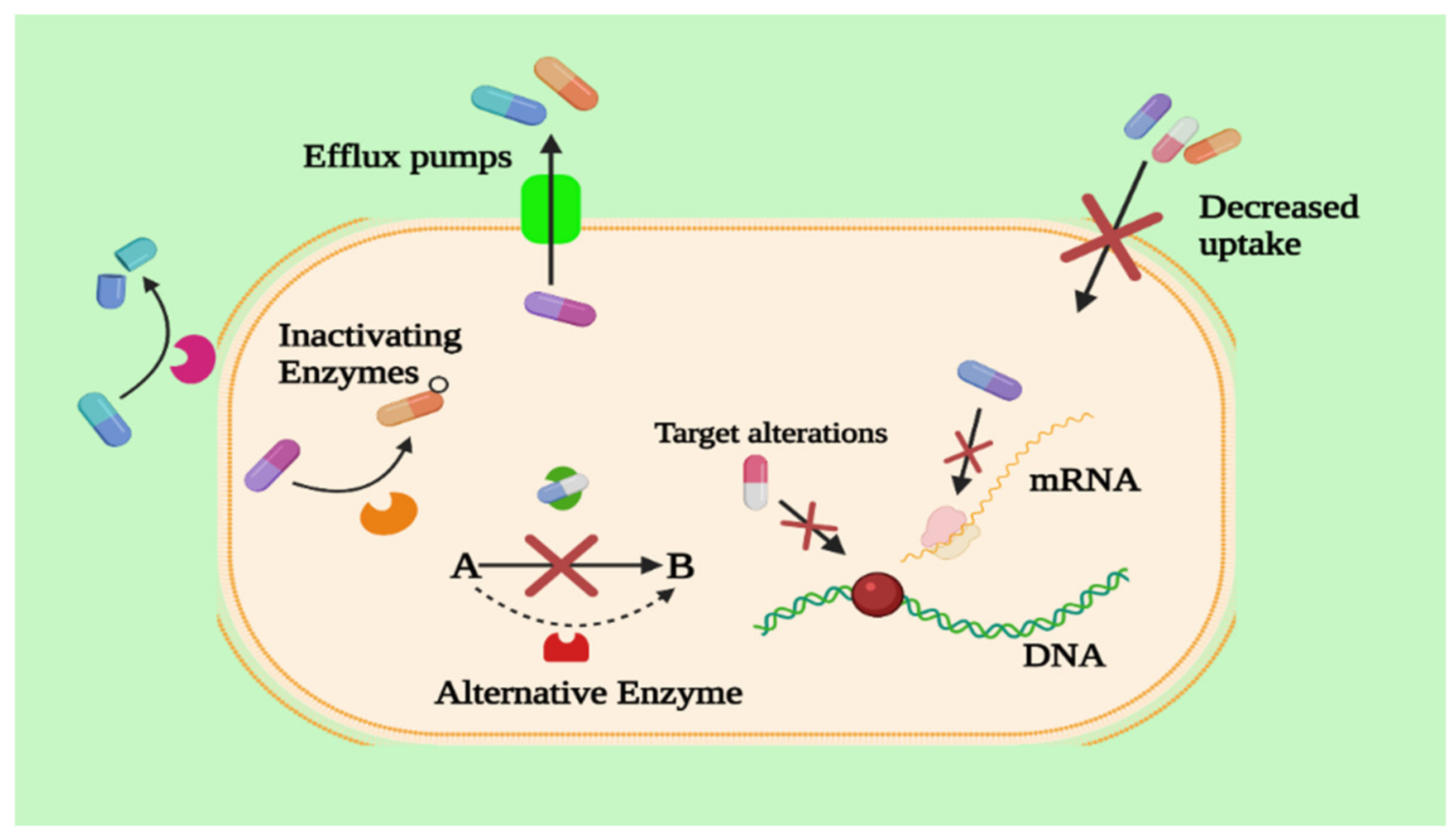
6. Mechanisms of Antimicrobial Resistance
7. Relationship between Antibiotic Use in Animals and Antibiotic Use in Humans
8. Development of Antimicrobial Resistance in Human and Animal Healthcare
8.1. New Antibiotics
8.2. Beta-Lactam/Beta-Lactamase Inhibitor
9. Alternatives to Antibiotics
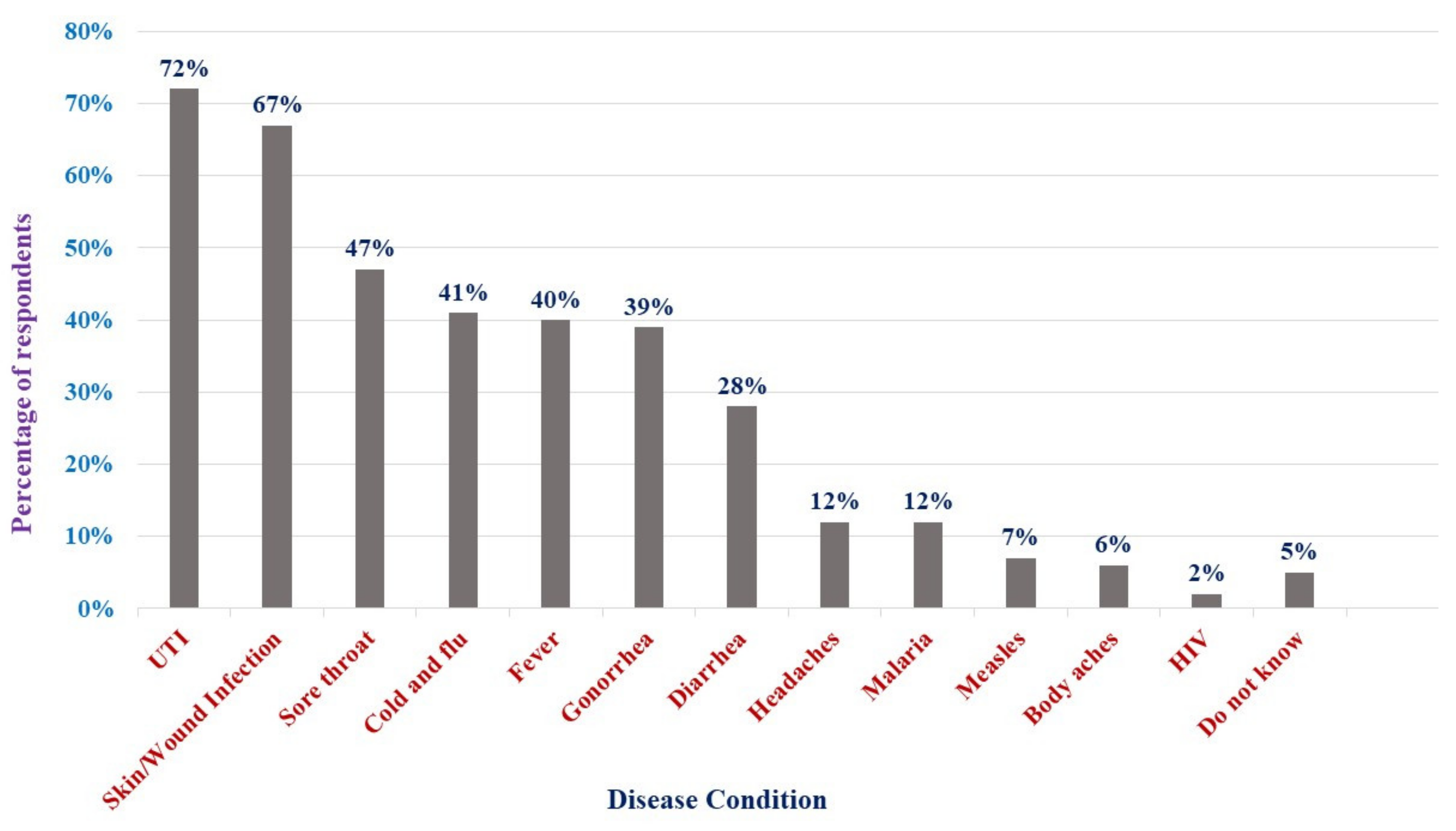
10. Lack of Awareness
11. Prevention of Antimicrobial Resistance in Human and Animal Healthcare
12. Poor Provider Knowledge and Lack of Guidelines
13. Awareness in the Community
14. Regulate the Sale and Use of Antibiotics through Prescription
15. Global Action Plan on Antimicrobial Resistance
16. Role of Pharmacists in Combating Resistance to Antimicrobials
17. Types of Intervention
18. Prescribing and Intervention Context
19. Knowledge of Antimicrobial Resistance and Appropriate Antibiotics Use
20. Practical Concerns and Diverse Influences on Antibiotic Prescribing
21. The Most Current Antimicrobial Stewardship Programs
21.1. The Southeast Asia Region Antimicrobial Stewardship 2022 Webinar Series (24 March–7 December 2022)
21.2. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) AMS Certificate (2022–2024)
22. Current Situation of Antibiotic Resistance in Bangladesh and Treatment Difficulty and Rising Costs
22.1. Treatment Pattern, Use
22.2. Self-Treatment and Non-Compliance
22.3. Antimicrobial Resistance and Sensitivity
22.4. Food Production and Food Animals, Fisheries, and the Environment, and the Spread of AMR
22.5. Bangladesh’s Current Antimicrobial Resistance Policies and Initiatives
22.6. Treatment Cost
23. Antimicrobial Stewardship in Bangladesh
24. Concluding Remarks and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aminov, R.I. A Brief History of the Antibiotic Era: Lessons Learned and Challenges for the Future. Front. Microbiol. 2010, 1, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Evolving Threat of Antimicrobial Resistance Options for Action; World Health Organization: Geneva, Switzerland, 2012; ISBN 9789241503181. [Google Scholar]
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- O’Neill, J. Securing New Drugs for Future Generations: The Pipeline of Antibiotics. Review on Antimicrobial Resistance. 2015. Available online: https://amr-review.org/sites/default/files/SECURING%20NEW%20DRUGS%20FOR%20FUTURE%20GENERATIONS%20FINAL%20WEB_0.pdf (accessed on 29 March 2022).
- Doma, A.O.; Popescu, R.; Mituleţu, M.; Muntean, D.; Dégi, J.; Boldea, M.V.; Radulov, I.; Dumitrescu, E.; Muselin, F.; Puvača, N.; et al. Comparative Evaluation of QnrA, QnrB, and QnrS Genes in Enterobacteriaceae Ciprofloxacin-Resistant Cases, in Swine Units and a Hospital from Western Romania. Antibiotics 2020, 9, 698. [Google Scholar] [CrossRef] [PubMed]
- Moruzi, R.F.; Tîrziu, E.; Muselin, F.; Tulcan, C.; Doma, A.; Degi, J.; Bărăităreanu, S.; Cristina, R. The importance of databases to manage the phenomenon of resistance to antimicrobials for veterinary use. Environment 2019, 9, 33. [Google Scholar]
- Grau, S.; Echeverria-Esnal, D.; Gómez-Zorrilla, S.; Navarrete-Rouco, M.E.; Masclans, J.R.; Espona, M.; Gracia-Arnillas, M.P.; Duran, X.; Comas, M.; Horcajada, J.P.; et al. Evolution of Antimicrobial Consumption During the First Wave of COVID-19 Pandemic. Antibiotics 2021, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Dégi, J.; Imre, K.; Herman, V.; Bucur, I.; Radulov, I.; Petrec, O.C.; Cristina, R.T. Antimicrobial Drug-Resistant Salmonella in Urban Cats: Is There an Actual Risk to Public Health? Antibiotics 2021, 10, 1404. [Google Scholar] [CrossRef] [PubMed]
- Béahdy, J. Recent Developments of Antibiotic Research and Classification of Antibiotics According to Chemical Structure. Adv. Appl. Microbiol. 1974, 18, 309–406. [Google Scholar] [CrossRef]
- Sengupta, S.; Chattopadhyay, M.K.; Grossart, H.P. The Multifaceted Roles of Antibiotics and Antibiotic Resistance in Nature. Front. Microbiol. 2013, 4, 47. [Google Scholar] [CrossRef] [Green Version]
- Tamma, P.D.; Cosgrove, S.E. Antimicrobial Stewardship. Infect. Dis. Clin. N. Am. 2011, 25, 245–260. [Google Scholar] [CrossRef]
- Dyar, O.J.; Pagani, L.; Pulcini, C. Strategies and Challenges of Antimicrobial Stewardship in Long-Term Care Facilities. Clin. Microbiol. Infect. 2015, 21, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Guardabassi, L.; Prescott, J.F. Antimicrobial Stewardship in Small Animal Veterinary Practice: From Theory to Practice Introduction: Nature of the Problem. Vet. Clin. NA Small Anim. Pract. 2015, 45, 361–376. [Google Scholar] [CrossRef]
- Bengtsson, B.; Greko, C. Antibiotic Resistance-Consequences for Animal Health, Welfare, and Food Production. Ups. J. Med. Sci. 2014, 119, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Powell, N.; Davidson, I.; Yelling, P.; Collinson, A.; Pollard, A.; Johnson, L.; Gibson, N.; Taylor, J.; Wisner, K.; Gaze, W.; et al. Developing a Local Antimicrobial Resistance Action Plan: The Cornwall One Health Antimicrobial Resistance Group. J. Antimicrob. Chemother. 2017, 72, 2661–2665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C. What Is Antimicrobial Stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beyer, P. Options for a Global Development and Stewardship Framework to Combat AMR Consultation of Member States and Relevant Partners. 2016. Available online: https://cdn.who.int/media/docs/default-source/antimicrobial-resistance/amr-gcp-irc-website/presentations-firstconsultation-stewardshipdevelopmentframework-2017-11-9-10.pdf?sfvrsn=e5aec720_2 (accessed on 29 March 2022).
- Eden, C.; Ackermann, F. Making Strategy: The Journey of Strategic Management; SAGE Publications Ltd.: London, UK, 2013. [Google Scholar]
- Cavalu, S.; Banica, F.; Gruian, C.; Vanea, E.; Goller, G.; Simon, V. Microscopic and Spectroscopic Investigation of Bioactive Glasses for Antibiotic Controlled Release. J. Mol. Struct. 2013, 1040, 47–52. [Google Scholar] [CrossRef]
- Tamma, P.D.; Holmes, A.; Ashley, E.D. Antimicrobial Stewardship: Another Focus for Patient Safety? Curr. Opin. Infect. Dis. 2014, 27, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Waksman, S.A. What Is an Antibiotic or an Antibiotic Substance? Mycologia 1947, 39, 565–569. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. The History of Antibiotics—HealthyChildren.Org. Available online: https://www.healthychildren.org/ (accessed on 29 March 2022).
- Laskin, A.I.; Bennett, J.W.; Gadd, G.M. Advances in Applied Microbiology; Elsevier: Amsterdam, Netherlands, 2003; Volume 52. [Google Scholar]
- History of Antibiotic Development. Available online: https://www.reactgroup.org/toolbox/understand/antibiotics/development-of-antibiotics-as-medicines/ (accessed on 29 March 2022).
- Sneader, W. History of Sulfonamides. Encycl. Life Sci. 2001, 1. [Google Scholar] [CrossRef]
- Reygaert, W.C. An Overview of the Antimicrobial Resistance Mechanisms of Bacteria. AIMS Microbiol. 2018, 4, 482. [Google Scholar] [CrossRef]
- Davies, J. Origins and Evolution of Antibiotic Resistance. Microbiologia 1996, 12, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.-W.; Cha, C.-J. Antibiotic Resistome from the One-Health Perspective: Understanding and Controlling Antimicrobial Resistance Transmission. Exp. Mol. Med. 2021, 53, 301–309. [Google Scholar] [CrossRef]
- Wright, G.D. The Antibiotic Resistome: The Nexus of Chemical and Genetic Diversity. Nat. Rev. Microbiol. 2007, 5, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Yong, D.; Toleman, M.A.; Giske, C.G.; Cho, H.S.; Sundman, K.; Lee, K.; Walsh, T.R. Characterization of a New Metallo-β-Lactamase Gene, Bla NDM-1, and a Novel Erythromycin Esterase Gene Carried on a Unique Genetic Structure in Klebsiella pneumoniae Sequence Type 14 from India. Antimicrob. Agents Chemother. 2009, 53, 5046–5054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, G.; Wright, G.D. Intrinsic Antibiotic Resistance: Mechanisms, Origins, Challenges and Solutions. Int. J. Med. Microbiol. 2013, 303, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Miere, F.; Vicas, S.I.; Timar, A.V.; Ganea, M.; Zdrinca, M.; Cavalu, S.; Fritea, L.; Vicas, L.; Muresan, M.; Pallag, A.; et al. Preparation and Characterization of Two Different Liposomal Formulations with Bioactive Natural Extract for Multiple Applications. Processes 2021, 9, 432. [Google Scholar] [CrossRef]
- Blair, J.M.A.; Webber, M.A.; Baylay, A.J.; Ogbolu, D.O.; Piddock, L.J. Molecular Mechanisms of Antibiotic Resistance. Nat. Rev. Microbiol. 2015, 13, 42–51. [Google Scholar] [CrossRef]
- Perry, J.; Waglechner, N.; Wright, G. The Prehistory of Antibiotic Resistance. Cold Spring Harb. Perspect. Med. 2016, 6, a025197. [Google Scholar] [CrossRef]
- Hall, B.G.; Barlow, M. Evolution of the Serine β-Lactamases: Past, Present and Future. Drug Resist. Updates 2004, 7, 111–123. [Google Scholar] [CrossRef]
- Bush, K. Past and Present Perspectives on β-Lactamases. Antimicrob. Agents Chemother. 2018, 62, e01076-18. [Google Scholar] [CrossRef] [Green Version]
- Waglechner, N.; McArthur, A.G.; Wright, G.D. Phylogenetic Reconciliation Reveals the Natural History of Glycopeptide Antibiotic Biosynthesis and Resistance. Nat. Microbiol. 2019, 4, 1862–1871. [Google Scholar] [CrossRef]
- Bhullar, K.; Waglechner, N.; Pawlowski, A.; Koteva, K.; Banks, E.D.; Johnston, M.D.; Barton, H.A.; Wright, G.D. Antibiotic Resistance Is Prevalent in an Isolated Cave Microbiome. PLoS ONE 2012, 7, e34953. [Google Scholar] [CrossRef]
- Allen, H.K.; Moe, L.A.; Rodbumrer, J.; Gaarder, A.; Handelsman, J. Functional Metagenomics Reveals Diverse β-Lactamases in a Remote Alaskan Soil. ISME J. 2009, 3, 243–251. [Google Scholar] [CrossRef] [PubMed]
- McMillan, E.A.; Gupta, S.K.; Williams, L.E.; Jové, T.; Hiott, L.M.; Woodley, T.A.; Barrett, J.B.; Jackson, C.R.; Wasilenko, J.L.; Simmons, M.; et al. Antimicrobial Resistance Genes, Cassettes, and Plasmids Present in Salmonella Enterica Associated with United States Food Animals. Front. Microbiol. 2019, 10, 832. [Google Scholar] [CrossRef] [PubMed]
- About Antibiotic Resistance|Antibiotic/Antimicrobial Resistance. Available online: https://www.cdc.gov/drugresistance/about.html (accessed on 29 March 2022).
- World Health Organization Antibiotic Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 29 March 2022).
- Li, G.; Zhang, J.; Guo, Q.; Wei, J.; Jiang, Y.; Zhao, X.; Zhao, L.L.; Liu, Z.; Lu, J.; Wan, K. Study of Efflux Pump Gene Expression in Rifampicin-Monoresistant Mycobacterium tuberculosis Clinical Isolates. J. Antibiot. 2015, 68, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.C.; Xi, H.; Liang, L.; Liu, J.D.; Liu, C.H.; Xue, Y.R.; Yu, X.Y. Rifampicin-Resistance Mutations in the RpoB Gene in Bacillus Velezensis CC09 Have Pleiotropic Effects. Front. Microbiol. 2017, 8, 178. [Google Scholar] [CrossRef] [Green Version]
- Makarov, V.; Manina, G.; Mikusova, K.; Möllmann, U.; Ryabova, O.; Saint-Joanis, B.; Dhar, N.; Pasca, M.R.; Buroni, S.; Lucarelli, A.P.; et al. Benzothiazinones Kill Mycobacterium tuberculosis by Blocking Arabinan Synthesis. Science 2009, 324, 801–804. [Google Scholar] [CrossRef] [Green Version]
- Safi, H.; Lingaraju, S.; Amin, A.; Kim, S.; Jones, M.; Holmes, M.; McNeil, M.; Peterson, S.N.; Chatterjee, D.; Fleischmann, R.; et al. Evolution of High-Level Ethambutol-Resistant Tuberculosis through Interacting Mutations in Decaprenylphosphoryl-β-D-Arabinose Biosynthetic and Utilization Pathway Genes. Nat. Genet. 2013, 45, 1190–1197. [Google Scholar] [CrossRef]
- Sreevatsan, S.; Stockbauer, K.E.; Pan, X.; Kreiswirth, B.N.; Moghazeh, S.L.; Jacobs, W.R.; Telenti, A.; Musser, J.M. Ethambutol Resistance in Mycobacterium tuberculosis: Critical Role of EmbB Mutations. Antimicrob. Agents Chemother. 1997, 41, 1677–1681. [Google Scholar] [CrossRef] [Green Version]
- Zheng, J.; Rubin, E.J.; Bifani, P.; Mathys, V.; Lim, V.; Au, M.; Jang, J.; Nam, J.; Dick, T.; Walker, J.R.; et al. Para-Aminosalicylic Acid Is a Prodrug Targeting Dihydrofolate Reductase in Mycobacterium tuberculosis. J. Biol. Chem. 2013, 288, 23447–23456. [Google Scholar] [CrossRef] [Green Version]
- Desjardins, C.A.; Cohen, K.A.; Munsamy, V.; Abeel, T.; Maharaj, K.; Walker, B.J.; Shea, T.P.; Almeida, D.V.; Manson, A.L.; Salazar, A.; et al. Genomic and Functional Analyses of Mycobacterium tuberculosis Strains Implicate Ald in D-Cycloserine Resistance. Nat. Genet. 2016, 48, 544–551. [Google Scholar] [CrossRef] [Green Version]
- Neuhaus, F.C.; Lynch, J.L. The Enzymatic Synthesis of D-Alanyl-d-Alanine. III. On the Inhibition of d-Alanyl-d-Alanine Synthetase by the Antibiotic d-Cycloserine. Biochemistry 1964, 3, 471–480. [Google Scholar] [CrossRef]
- Cáceres, N.E.; Harris, N.B.; Wellehan, J.F.; Feng, Z.; Kapur, V.; Barletta, R.G. Overexpression of the D-Alanine Racemase Gene Confers Resistance to D-Cycloserine in Mycobacterium Smegmatis. J. Bacteriol. 1997, 179, 5046–5055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, G.; Monecke, S.; Brus, O.; Ehricht, R.; Söderquist, B. Long Term Molecular Epidemiology of Methicillin-Susceptible Staphylococcus Aureus Bacteremia Isolates in Sweden. PLoS ONE 2014, 9, e114276. [Google Scholar] [CrossRef] [PubMed]
- Vilchèze, C.; Av-Gay, Y.; Attarian, R.; Liu, Z.; Hazbón, M.H.; Colangeli, R.; Chen, B.; Liu, W.; Alland, D.; Sacchettini, J.C.; et al. Mycothiol Biosynthesis Is Essential for Ethionamide Susceptibility in Mycobacterium tuberculosis. Mol. Microbiol. 2008, 69, 1316–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scorpio, A.; Zhang, Y. Mutations in PncA, a Gene Encoding Pyrazinamidase/Nicotinamidase, Cause Resistance to the Antituberculous Drug Pyrazinamide in Tubercle Bacillus. Nat. Med. 1996, 2, 662–667. [Google Scholar] [CrossRef]
- Randall, L.P.; Cooles, S.W.; Osborn, M.K.; Piddock, L.J.V.; Woodward, M.J. Antibiotic Resistance Genes, Integrons and Multiple Antibiotic Resistance in Thirty-Five Serotypes of Salmonella Enterica Isolated from Humans and Animals in the UK. J. Antimicrob. Chemother. 2004, 53, 208–216. [Google Scholar] [CrossRef] [Green Version]
- Musser, J.M.; Kapur, V.; Williams, D.L.; Kreiswirth, B.N.; Van Soolingen, D.; Van Embden, J.D.A. Characterization of the Catalase-Peroxidase Gene (KatG) and InhA Locus in Isoniazid-Resistant and -Susceptible Strains of Mycobacterium tuberculosis by Automated DNA Sequencing: Restricted Array of Mutations Associated with Drug Resistance. J. Infect. Dis. 1996, 173, 196–202. [Google Scholar] [CrossRef]
- Rozwarski, D.A.; Grant, G.A.; Barton, D.H.R.; Jacobs, W.R.; Sacchettini, J.C. Modification of the NADH of the Isoniazid Target (InhA) from Mycobacterium tuberculosis. Science 1998, 279, 98–102. [Google Scholar] [CrossRef]
- Torres, J.N.; Paul, L.V.; Rodwell, T.C.; Victor, T.C.; Amallraja, A.M.; Elghraoui, A.; Goodmanson, A.P.; Ramirez-Busby, S.M.; Chawla, A.; Zadorozhny, V.; et al. Novel KatG Mutations Causing Isoniazid Resistance in Clinical M. Tuberculosis Isolates. Emerg. Microbes Infect. 2015, 4, e42. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Røttingen, J.A.; Klugman, K.; Davies, S. Access to Effective Antimicrobials: A Worldwide Challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef]
- Holmes, A.H.; Moore, L.S.P.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J.V. Understanding the Mechanisms and Drivers of Antimicrobial Resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Sefton, A.M. Mechanisms of Antimicrobial Resistance: Their Clinical Relevance in the New Millennium. Drugs 2002, 62, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Resistance Mechanisms–Antibiotic Resistance–ReAct. Available online: https://www.reactgroup.org/toolbox/understand/antibiotic-resistance/resistance-mechanisms-in-bacteria/ (accessed on 24 August 2021).
- Kattupalli, S.; Chatla, S. Antibiotic Resistance-Reasons and Control Measures. Int. J. Pharm. Biol. Sci. 2019, 9, 503–508. [Google Scholar] [CrossRef]
- Van Den Bogaard, A.E.; Stobberingh, E.E. Antibiotic Usage in Animals. Impact on Bacterial Resistance and Public Health. Drugs 1999, 58, 589–607. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Rahaman, M.S.; Islam, M.R.; Hossain, M.E.; Mithi, F.M.; Ahmed, M.; Saldías, M.; Akkol, E.K.; Sobarzo-Sánchez, E. Multifunctional Therapeutic Potential of Phytocomplexes and Natural Extracts for Antimicrobial Properties. Antibiotics 2021, 10, 1076. [Google Scholar] [CrossRef]
- Rousham, E.K.; Unicomb, L.; Islam, M.A. Human, Animal and Environmental Contributors to Antibiotic Resistance in Low-Resource Settings: Integrating Behavioural, Epidemiological and One Health Approaches. Proc. R. Soc. B Biol. Sci. 2018, 285, 20180332. [Google Scholar] [CrossRef]
- Eagar, H.; Swan, G.; Van Vuuren, M. A Survey of Antimicrobial Usage in Animals in South Africa with Specific Reference to Food Animals. J. S. Afr. Vet. Assoc. 2012, 83, 8. [Google Scholar] [CrossRef] [Green Version]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial Resistance: A Global Multifaceted Phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [Green Version]
- Cavalu, S.; Simon, V. Microstructure and bioactivity of acrylic bone cements for prosthetic surgery. J. Optoelectron. Adv. Mater. 2006, 8, 1520–1523. [Google Scholar]
- South African National Aids Council. National Strategic Plan on HIV, STIs and TB 2012–2016; South African National Aids Council: Pretoria, South Africa, 2011. [Google Scholar]
- Shaeer, K.M.; Zmarlicka, M.T.; Chahine, E.B.; Piccicacco, N.; Cho, J.C. Plazomicin: A Next-Generation Aminoglycoside. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2019, 39, 77–93. [Google Scholar] [CrossRef] [Green Version]
- Eljaaly, K.; Alharbi, A.; Alshehri, S.; Ortwine, J.K.; Pogue, J.M. Plazomicin: A Novel Aminoglycoside for the Treatment of Resistant Gram-Negative Bacterial Infections. Drugs 2019, 79, 243–269. [Google Scholar] [CrossRef]
- Denervaud-Tendon, V.; Poirel, L.; Connolly, L.E.; Krause, K.M.; Nordmann, P. Plazomicin Activity against Polymyxin-Resistant Enterobacteriaceae, Including MCR-1-Producing Isolates. J. Antimicrob. Chemother. 2017, 72, 2787–2791. [Google Scholar] [CrossRef] [PubMed]
- Wagenlehner, F.M.E.; Cloutier, D.J.; Komirenko, A.S.; Cebrik, D.S.; Krause, K.M.; Keepers, T.R.; Connolly, L.E.; Miller, L.G.; Friedland, I.; Dwyer, J.P. Once-Daily Plazomicin for Complicated Urinary Tract Infections. J. Urol. 2019, 202, 641–642. [Google Scholar] [CrossRef] [PubMed]
- Connolly, L.E.; Riddle, V.; Cebrik, D.; Armstrong, E.S.; Miller, L.G. A Multicenter, Randomized, Double-Blind, Phase 2 Study of the Efficacy and Safety of Plazomicin Compared with Levofloxacin in the Treatment of Complicated Urinary Tract Infection and Acute Pyelonephritis. Antimicrob. Agents Chemother. 2018, 62, e01989-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portsmouth, S.; van Veenhuyzen, D.; Echols, R.; Machida, M.; Ferreira, J.C.A.; Ariyasu, M.; Tenke, P.; Nagata, T. Den Cefiderocol versus Imipenem-Cilastatin for the Treatment of Complicated Urinary Tract Infections Caused by Gram-Negative Uropathogens: A Phase 2, Randomised, Double-Blind, Non-Inferiority Trial. Lancet Infect. Dis. 2018, 18, 1319–1328. [Google Scholar] [CrossRef]
- Carmeli, Y.; Armstrong, J.; Laud, P.J.; Newell, P.; Stone, G.; Wardman, A.; Gasink, L.B. Ceftazidime-Avibactam or Best Available Therapy in Patients with Ceftazidime-Resistant Enterobacteriaceae and Pseudomonas aeruginosa Complicated Urinary Tract Infections or Complicated Intra-Abdominal Infections (REPRISE): A Randomised, Pathogen-Directed, Phase 3 Study. Lancet Infect. Dis. 2016, 16, 661–673. [Google Scholar] [CrossRef]
- Wagenlehner, F.M.; Sobel, J.D.; Newell, P.; Armstrong, J.; Huang, X.; Stone, G.G.; Yates, K.; Gasink, L.B. Ceftazidime-Avibactam Versus Doripenem for the Treatment of Complicated Urinary Tract Infections, Including Acute Pyelonephritis: RECAPTURE, a Phase 3 Randomized Trial Program. Clin. Infect. Dis. 2016, 63, 754–762. [Google Scholar] [CrossRef] [Green Version]
- Popejoy, M.W.; Paterson, D.L.; Cloutier, D.; Huntington, J.A.; Miller, B.; Bliss, C.A.; Steenbergen, J.N.; Hershberger, E.; Umeh, O.; Kaye, K.S. Efficacy of Ceftolozane/Tazobactam against Urinary Tract and Intra-Abdominal Infections Caused by ESBL-Producing Escherichia coli and Klebsiella pneumoniae: A Pooled Analysis of Phase 3 Clinical Trials. J. Antimicrob. Chemother. 2017, 72, 268–272. [Google Scholar] [CrossRef] [Green Version]
- Wagenlehner, F.M.; Umeh, O.; Steenbergen, J.; Yuan, G.; Darouiche, R.O. Ceftolozane-Tazobactam Compared with Levofloxacin in the Treatment of Complicated Urinary-Tract Infections, Including Pyelonephritis: A Randomised, Double-Blind, Phase 3 Trial (ASPECT-CUTI). Lancet 2015, 385, 1949–1956. [Google Scholar] [CrossRef]
- Kaye, K.S.; Bhowmick, T.; Metallidis, S.; Bleasdale, S.C.; Sagan, O.S.; Stus, V.; Vazquez, J.; Zaitsev, V.; Bidair, M.; Chorvat, E.; et al. Effect of Meropenem-Vaborbactam vs Piperacillin-Tazobactam on Clinical Cure or Improvement and Microbial Eradication in Complicated Urinary Tract Infection: The TANGO I Randomized Clinical Trial. JAMA 2018, 319, 788–799. [Google Scholar] [CrossRef]
- Wunderink, R.G.; Giamarellos-Bourboulis, E.J.; Rahav, G.; Mathers, A.J.; Bassetti, M.; Vazquez, J.; Cornely, O.A.; Solomkin, J.; Bhowmick, T.; Bishara, J.; et al. Effect and Safety of Meropenem–Vaborbactam versus Best-Available Therapy in Patients with Carbapenem-Resistant Enterobacteriaceae Infections: The TANGO II Randomized Clinical Trial. Infect. Dis. Ther. 2018, 7, 439–455. [Google Scholar] [CrossRef] [Green Version]
- Motsch, J.; De Oliveira, C.U.M.; Stus, V.; Kö Ksal, I.; Lyulko, O.; Boucher, H.W.; Kaye, K.S.; File, T.M.; Brown, M.L.; Khan, I.; et al. RESTORE-IMI 1: A Multicenter, Randomized, Double-Blind Trial Comparing Efficacy and Safety of Imipenem/Relebactam vs Colistin Plus Imipenem in Patients With Imipenem-Nonsusceptible Bacterial Infections. Clin. Infect. Dis. 2020, 70, 1799–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhanel, G.G.; Baxter, M.R.; Adam, H.J.; Sutcliffe, J.; Karlowsky, J.A. In Vitro Activity of Eravacycline against 2213 Gram-Negative and 2424 Gram-Positive Bacterial Pathogens Isolated in Canadian Hospital Laboratories: CANWARD Surveillance Study 2014–2015. Diagn. Microbiol. Infect. Dis. 2018, 91, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Livermore, D.M.; Tulkens, P.M. Temocillin Revived. J. Antimicrob. Chemother. 2009, 63, 243–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balakrishnan, I.; Awad-El-Kariem, F.M.; Aali, A.; Kumari, P.; Mulla, R.; Tan, B.; Brudney, D.; Ladenheim, D.; Ghazy, A.; Khan, I.; et al. Temocillin Use in England: Clinical and Microbiological Efficacies in Infections Caused by Extended-Spectrum and/or Derepressed AmpC β-Lactamase-Producing Enterobacteriaceae. J. Antimicrob. Chemother. 2011, 66, 2628–2631. [Google Scholar] [CrossRef] [Green Version]
- Adams-Haduch, J.M.; Potoski, B.A.; Sidjabat, H.E.; Paterson, D.L.; Doi, Y. Activity of Temocillin against KPC-Producing Klebsiella pneumoniae and Escherichia coli. Antimicrob. Agents Chemother. 2009, 53, 2700–2701. [Google Scholar] [CrossRef] [Green Version]
- Tsakris, A.; Koumaki, V.; Politi, L.; Balakrishnan, I. Activity of Temocillin against KPC-Producing Enterobacteriaceae Clinical Isolates. Int. J. Antimicrob. Agents 2019, 55, 105843. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Golden, A.R.; Zelenitsky, S.; Wiebe, K.; Lawrence, C.K.; Adam, H.J.; Idowu, T.; Domalaon, R.; Schweizer, F.; Zhanel, M.A.; et al. Cefiderocol: A Siderophore Cephalosporin with Activity Against Carbapenem-Resistant and Multidrug-Resistant Gram-Negative Bacilli. Drugs 2019, 79, 271–289. [Google Scholar] [CrossRef]
- Jacobs, M.R.; Abdelhamed, A.M.; Good, C.E.; Rhoads, D.D.; Hujer, K.M.; Hujer, A.M.; Domitrovic, T.N.; Rudin, S.D.; Richter, S.S.; van Duin, D.; et al. ARGONAUT-I: Activity of Cefiderocol (s-649266), a Siderophore Cephalosporin, against Gram-Negative Bacteria, Including Carbapenem-Resistant Nonfermenters and Enterobacteriaceae with Defined Extended-Spectrum β-Lactamases and Carbapenemases. Antimicrob. Agents Chemother. 2019, 63, e01801-18. [Google Scholar] [CrossRef] [Green Version]
- Kresken, M.; Korte-Berwanger, M.; Gatermann, S.G.; Pfeifer, Y.; Pfennigwerth, N.; Seifert, H.; Werner, G. In Vitro Activity of Cefiderocol against Aerobic Gram-Negative Bacterial Pathogens from Germany. Int. J. Antimicrob. Agents 2020, 56, 106128. [Google Scholar] [CrossRef]
- Kresken, M.; Körber-Irrgang, B.; Pfeifer, Y.; Werner, G. Activity of Temocillin against CTX-M-Producing Escherichia coli and Klebsiella pneumoniae from Germany. Int. J. Antimicrob. Agents 2018, 51, 159–160. [Google Scholar] [CrossRef]
- Wunderink, R.G.; Matsunaga, Y.; Ariyasu, M.; Clevenbergh, P.; Echols, R.; Kaye, K.S.; Kollef, M.; Menon, A.; Pogue, J.M.; Shorr, A.F.; et al. Cefiderocol versus High-Dose, Extended-Infusion Meropenem for the Treatment of Gram-Negative Nosocomial Pneumonia (APEKS-NP): A Randomised, Double-Blind, Phase 3, Non-Inferiority Trial. Lancet Infect. Dis. 2021, 21, 213–225. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Lawrence, C.K.; Adam, H.; Schweizer, F.; Zelenitsky, S.; Zhanel, M.; Lagacé-Wiens, P.R.S.; Walkty, A.; Denisuik, A.; Golden, A.; et al. Imipenem–Relebactam and Meropenem–Vaborbactam: Two Novel Carbapenem-β-Lactamase Inhibitor Combinations. Drugs 2017, 78, 65–98. [Google Scholar] [CrossRef] [PubMed]
- Shortridge, D.; Castanheira, M.; Pfaller, M.A.; Flamm, R.K. Ceftolozane-Tazobactam Activity against Pseudomonas aeruginosa Clinical Isolates from U.S. Hospitals: Report from the PACTS Antimicrobial Surveillance Program, 2012 to 2015. Antimicrob. Agents Chemother. 2017, 61, e00465-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, S.C.; Liu, C.E.; Lu, P.L.; Chen, Y.S.; Lu, M.C.; Ko, W.C.; Hsueh, P.R.; Chuang, Y.C.; Wang, F. Der Activity of Ceftolozane-Tazobactam against Gram-Negative Pathogens Isolated from Lower Respiratory Tract Infections in the Asia-Pacific Region: SMART 2015–2016. Int. J. Antimicrob. Agents 2020, 55, 105883. [Google Scholar] [CrossRef] [PubMed]
- Karlowsky, J.A.; Hackel, M.A.; Bouchillon, S.K.; Sahm, D.F. In Vitro Activity of WCK 5222 (Cefepime-Zidebactam) against Worldwide Collected Gram-Negative Bacilli Not Susceptible to Carbapenems. Antimicrob. Agents Chemother. 2020, 64, e01432-20. [Google Scholar] [CrossRef]
- Lapuebla, A.; Abdallah, M.; Olafisoye, O.; Cortes, C.; Urban, C.; Landman, D.; Quale, J. Activity of Imipenem with Relebactam against Gram-Negative Pathogens from New York City. Antimicrob. Agents Chemother. 2015, 59, 5029–5031. [Google Scholar] [CrossRef] [Green Version]
- Roca, I.; Akova, M.; Baquero, F.; Carlet, J.; Cavaleri, M.; Coenen, S.; Cohen, J.; Findlay, D.; Gyssens, I.; Heure, O.E.; et al. The Global Threat of Antimicrobial Resistance: Science for Intervention. N. Microbes N. Infect. 2015, 6, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Sheard, D.E.; O’Brien-Simpson, N.M.; Wade, J.D.; Separovic, F. Combating Bacterial Resistance by Combination of Antibiotics with Antimicrobial Peptides. Pure Appl. Chem. 2019, 91, 199–209. [Google Scholar] [CrossRef]
- Qiao, Y.; Ma, X.; Zhang, M.; Zhong, S. Cerocin, a Novel Piscidin-like Antimicrobial Peptide from Black Seabass, Centropristis Striata. Fish Shellfish Immunol. 2021, 110, 86–90. [Google Scholar] [CrossRef]
- Jia, F.; Wang, J.; Zhang, L.; Zhou, J.; He, Y.; Lu, Y.; Liu, K.; Yan, W.; Wang, K. Multiple Action Mechanism and in Vivo Antimicrobial Efficacy of Antimicrobial Peptide Jelleine-I. J. Pept. Sci. 2021, 27, e3294. [Google Scholar] [CrossRef]
- Li, F.; Gao, Z.; Wang, K.; Zhao, Y.; Wang, H.; Zhao, M.; Zhao, Y.; Bai, L.; Yu, Z.; Yang, X. A Novel Defensin-like Peptide Contributing to Antimicrobial and Antioxidant Capacity of the Tick Dermacentor silvarum (Acari: Ixodidae). Exp. Appl. Acarol. 2021, 83, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Huang, J.; Hao, H.; Wei, H.; Zhou, Y.; Peng, J. Applications of New Functions for Inducing Host Defense Peptides and Synergy Sterilization of Medium Chain Fatty Acids in Substituting In-Feed Antibiotics. J. Funct. Foods 2019, 52, 348–359. [Google Scholar] [CrossRef]
- Qamar, F.; Kauser, H.; Fatima, K. Open Access Bioequivalence & Bioavailability Prevalence and Consequences of Misuse of Antibiotics, Survey Based Study in Karachi. Karachi Artic. J. Bioequiv. Bioavailab. 2015, 7, 5. [Google Scholar] [CrossRef]
- Naveed, S.; Hameed, A.; Sharif, N.; Urooj, A.; Mehak, R. Nat Ional Treat Ment Guidelines for Ant Imicrobial Use in Infect Ious Diseases NAT IONAL CENT RE FOR DI… Correspondence: Use of 3rd Generation Cephalosporins in Different Age Groups in Tertiary Health Care Centers of Karachi. J. Sci. Innov. Res. 2014, 3, 1–4. [Google Scholar] [CrossRef]
- Hameed, A.; Naveed, S. Analysis of Parts of Precription in Common Practice. Int. J. Pharm. Pract. Pharm. Sci. 2016, 2, 1–4. [Google Scholar]
- Hameed, A.; Naveed, S.; Qamar, F.; Alam, M.T. Irrational Use of Antibiotics, in Different Age Groups of Karachi: A Wakeup Call for Antibiotic Resistance and Future Infections Formulation and Evaluation of Fast Dissolving Tablets (ODTs) of Etoricoxib by DC View Project Cyberchondria, A Peril in Our Soc. Artic. J. Bioequiv. Bioavailab. 2016, 8, 5. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan on Antimicrobial Resistance. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 29 March 2022).
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic Resistance-the Need for Global Solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [Green Version]
- Borg, M.A. National Cultural Dimensions as Drivers of Inappropriate Ambulatory Care Consumption of Antibiotics in Europe and Their Relevance to Awareness Campaigns. J. Antimicrob. Chemother. 2012, 67, 763–767. [Google Scholar] [CrossRef] [Green Version]
- Dar, O.A.; Hasan, R.; Schlundt, J.; Harbarth, S.; Caleo, G.; Dar, F.K.; Littmann, J.; Rweyemamu, M.; Buckley, E.J.; Shahid, M.; et al. Exploring the Evidence Base for National and Regional Policy Interventions to Combat Resistance. Lancet 2016, 387, 285–295. [Google Scholar] [CrossRef] [Green Version]
- ReAct Rational Use of Antibiotics–Implement the Plan. Available online: https://www.reactgroup.org/toolbox/policy/implement-the-national-action-plan/rational-use-of-antibiotics/ (accessed on 29 March 2022).
- BioMérieux Public Awareness of Antibiotic Resistance. Available online: https://amr.biomerieux.com/en/education/awareness-initiatives/ (accessed on 29 March 2022).
- Davey, P.G.; Bax, R.P.; Newey, J.; Reeves, D.; Rutherford, D.; Slack, R.; Warren, R.E.; Watt, B.; Wilson, J. Growth in the Use of Antibiotics in the Community in England and Scotland in 1980–1993. Br. Med. J. 1996, 312, 613. [Google Scholar] [CrossRef] [Green Version]
- Guillemot, D.; Carbon, C.; Vauzelle-Kervroëdan, F.; Balkau, B.; Maison, P.; Bouvenot, G.; Eschwège, E. Inappropriateness and Variability of Antibiotic Prescription among French Office-Based Physicians. J. Clin. Epidemiol. 1998, 51, 61–68. [Google Scholar] [CrossRef]
- Carbon, C.; Bax, R.P. Regulating the Use of Antibiotics in the Community. Br. Med. J. 1998, 317, 663–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillemot, D.; Maison, P.; Carbon, C.; Balkau, B.; Vauzelle-Kervroëdan, F.; Sermet, C.; Bouvenot, G.; Eschwège, E. Trends in Antimicrobial Drug Use in the Community-France, 1981-1992. J. Infect. Dis. 1998, 177, 492–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillemot, D.; Carbon, C.; Balkau, B.; Geslin, P.; Lecoeur, H.; Vauzelle-Kervroedan, F.; Bouvenot, G.; Eschwege, E. Low Dosage and Long Treatment Duration of β-Lactam: Risk Factors for Carriage of Penicillin-Resistant Streptococcus Pneumoniae. J. Am. Med. Assoc. 1998, 279, 365–370. [Google Scholar] [CrossRef]
- Pichichero, M.E. Group A Streptococcal Tonsillopharyngitis: Cost-Effective Diagnosis and Treatment. Ann. Emerg. Med. 1995, 25, 390–403. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Top, F.H.; Dudding, B.A.; Wannamaker, L.W. Diagnosis of Streptococcal Pharyngitis: Differentiation of Active Infection from the Carrier State in the Symptomatic Child. J. Infect. Dis. 1971, 123, 490–501. [Google Scholar] [CrossRef]
- Kaplan, W.; Laing, R. Priority Medicines for Europe and the World. 2004. Available online: https://apps.who.int/iris/handle/10665/68769 (accessed on 29 March 2022).
- Tomson, G.; Vlad, I. The Need to Look at Antibiotic Resistance from a Health Systems Perspective. Upsala J. Med. Sci. 2014, 119, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Western Pacific. Available online: https://www.who.int/westernpacific (accessed on 29 March 2022).
- Jinks, T.; Lee, N.; Sharland, M.; Rex, J.; Gertler, N.; Diver, M.; Jones, I.; Jones, K.; Mathewson, S.; Chiara, F.; et al. A Time for Action: Antimicrobial Resistance Needs Global Response. Bull. World Health Organ. 2016, 94, 558. [Google Scholar] [CrossRef]
- Williford, S.L.; Johnson, D.F. Impact of Pharmacist Counseling on Medication Knowledge and Compliance. Mil. Med. 1995, 160, 561–564. [Google Scholar] [CrossRef]
- Booth, J.L.; Mullen, A.B.; Thomson, D.A.M.; Johnstone, C.; Galbraith, S.J.; Bryson, S.M.; McGovern, E.M. Antibiotic Treatment of Urinary Tract Infection by Community Pharmacists: A Cross-Sectional Study. Br. J. Gen. Pract. 2013, 63, e244–e249. [Google Scholar] [CrossRef] [PubMed]
- Farley, T.M.; Shelsky, C.; Powell, S.; Farris, K.B.; Carter, B.L. Effect of Clinical Pharmacist Intervention on Medication Discrepancies Following Hospital Discharge. Int. J. Clin. Pharm. 2014, 36, 430–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakeena, M.H.F.; Bennett, A.A.; McLachlan, A.J. Enhancing Pharmacists’ Role in Developing Countries to Overcome the Challenge of Antimicrobial Resistance: A Narrative Review. Antimicrob. Resist. Infect. Control 2018, 7, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roiu, G.; Cavalu, S.; Teusdea, A.; Petricas-Heredea, D.A.; Fratila, O. Assessment of Antibiotic Influence on Structural Modifications of Amniotic Membrane by FTIR Spectroscopy. Mater. Plast. 2020, 57, 191–198. [Google Scholar] [CrossRef]
- Schellack, N.; Pretorius, R.; Messina, A.P. ‘Esprit de Corps’: Towards Collaborative Integration of Pharmacists and Nurses into Antimicrobial Stewardship Programmes in South Africa. S. Afr. Med. J. 2016, 106, 973–974. [Google Scholar] [CrossRef] [Green Version]
- Burger, M.; Fourie, J.; Loots, D.; Mnisi, T.; Schellack, N.; Bezuidenhout, S.; Meyer, J.C. Knowledge and Perceptions of Antimicrobial Stewardship Concepts among Final Year Pharmacy Students in Pharmacy Schools across South Africa. S. Afr. J. Infect. Dis. 2016, 31, 84–90. [Google Scholar] [CrossRef] [Green Version]
- FIDSSA South African Antibiotic Stewardship Programme (SAASP). Available online: https://www.fidssa.co.za/federation-members/saasp-mission (accessed on 29 March 2022).
- Wilkinson, A.; Ebata, A.; MacGregor, H. Interventions to Reduce Antibiotic Prescribing in LMICs: A Scoping Review of Evidence from Human and Animal Health Systems. Antibiotics 2018, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Using Indicators to Measure Country Pharmaceutical Situations Fact Book on WHO Level I and Level II Monitoring Indicators. 2006. Available online: https://apps.who.int/iris/bitstream/handle/10665/69927/WHO_TCM_2007.2_eng.pdf (accessed on 29 March 2022).
- Dellit, T.H.; Owens, R.C.; McGowan, J.E.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef]
- Pulcini, C.; Gyssens, I.C. How to Educate Prescribers in Antimicrobial Stewardship Practices. Virulence 2013, 4, 192–202. [Google Scholar] [CrossRef] [Green Version]
- Rahal, J.J.; Urban, C.; Horn, D.; Freeman, K.; Segal-Maurer, S.; Maurer, J.; Mariano, N.; Marks, S.; Burns, J.M.; Dominick, D.; et al. Class Restriction of Cephalosporin Use to Control Total Cephalosporin Resistance in Nosocomial Klebsiella. JAMA 1998, 280, 1233–1237. [Google Scholar] [CrossRef] [Green Version]
- Lautenbach, E.; LaRosa, L.A.; Marr, A.M.; Nachamkin, I.; Bilker, W.B.; Fishman, N.O. Changes in the Prevalence of Vancomycin-Resistant Enterococci in Response to Antimicrobial Formulary Interventions: Impact of Progressive Restrictions on Use of Vancomycin and Third-Generation Cephalosporins. Clin. Infect. Dis. 2003, 36, 440–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, S.J.; Wilson, A.L.T.; Allen, M.C.; Sher, H.A.; Goldstone, A.H.; Scott, G.M. The Control of Hyperendemic Glycopeptide-Resistant Enterococcus Spp. on ahaematology Unit by Changing Antibiotic Usage. J. Antimicrob. Chemother. 1999, 43, 261–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zara, C.; Torralba, M.; Sotoca, J.M.; Prat, A.; Faixedas, M.-T.; Gilabert, A. The Impact of New Drug Introduction on Drug Expenditure in Primary Health Care in Catalunya, Spain. Ann. Pharmacother. 2005, 39, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Ostini, R.; Hegney, D.; Jackson, C.; Williamson, M.; Mackson, J.M.; Gurman, K.; Hall, W.; Tett, S.E. Systematic Review of Interventions to Improve Prescribing. Ann. Pharmacother. 2009, 43, 502–513. [Google Scholar] [CrossRef]
- Organisation mondiale de la Santé. Plan D’ Action Mondial Pour Combattre la Résistance aux Antimicrobiens. 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/249548/9789242509762-fre.pdf (accessed on 29 March 2022).
- Vadivoo, N.S.; Usha, B.; Padmavathi, B.K. Assessment of Clinicians Knowledge and Perception on Antimicrobial Resistance a Primary Strategy for Antimicrobial Resistance Control. Glob. J. Med. Res. 2015, 15, 9–14. [Google Scholar]
- Eccles, M.P.; Grimshaw, J.M.; Johnston, M.; Steen, N.; Pitts, N.B.; Thomas, R.; Glidewell, E.; Maclennan, G.; Bonetti, D.; Walker, A. Applying Psychological Theories to Evidence-Based Clinical Practice: Identifying Factors Predictive of Managing Upper Respiratory Tract Infections without Antibiotics. Implement. Sci. 2007, 2, 26. [Google Scholar] [CrossRef] [Green Version]
- Shehadeh, M.; Suaifan, G.; Darwish, R.M.; Wazaify, M.; Zaru, L.; Alja’fari, S. Knowledge, Attitudes and Behavior Regarding Antibiotics Use and Misuse among Adults in the Community of Jordan. A Pilot Study. Saudi Pharm. J. 2012, 20, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Gitzinger, M. Antibiotic Resistance Response—GARDP. Available online: https://gardp.org/what-we-do/antibiotic-resistance/ (accessed on 29 March 2022).
- De Sosa, A.J.; Byarugaba, D.K.; Amabile-Cuevas, C.F.; Hsueh, P.R.; Kariuki, S.; Okeke, I.N. Antimicrobial Resistance in Developing Countries. In Antimicrobial Resistance in Developing Countries; Springer: New York, NY, USA, 2010; pp. 1–554. [Google Scholar] [CrossRef]
- Jairoun, A.; Hassan, N.; Ali, A.; Jairoun, O.; Shahwan, M. Knowledge, Attitude and Practice of Antibiotic Use among University Students: A Cross Sectional Study in UAE. BMC Public Health 2019, 19, 518. [Google Scholar] [CrossRef]
- Shahpawee, N.S.; Chaw, L.L.; Muharram, S.H.; Goh, H.P.; Hussain, Z.; Ming, L.C. University Students’ Antibiotic Use and Knowledge of Antimicrobial Resistance: What Are the Common Myths? Antibiotics 2020, 9, 349. [Google Scholar] [CrossRef]
- Chandy, S.J.; Mathai, E.; Thomas, K.; Faruqui, A.; Holloway, K.; Lundborg, C.S. Antibiotic use and resistance: Perceptions and ethical challenges among doctors, pharmacists and the public in Vellore, South India. Indian J. Med. Ethic 2013, 10, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, L.; McKee, M. Factors Influencing Antibiotic Prescribing in China: An Exploratory Analysis. Health Policy 2009, 90, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Kotwani, A.; Wattal, C.; Joshi, P.C.; Holloway, K. Irrational Use of Antibiotics and Role of the Pharmacist: An Insight from a Qualitative Study in New Delhi, India. J. Clin. Pharm. Ther. 2012, 37, 308–312. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Organizations Says Being Trans Is Not A Mental Disorder|OutRight Action International. 2018. Available online: https://outrightinternational.org/content/world-health-organizations-says-being-trans-not-mental-disorder (accessed on 29 March 2022).
- ESCMID. ESCMID AMS Certificate 2022–2024. Available online: https://www.escmid.org/research_projects/study_groups/study_groups_a_f/antimicrobial_stewardship/escmid_ams_certificate_2022_2024/ (accessed on 29 March 2022).
- Monwar, M.; Rafiqul Islam, M.; Ashraf Ali, M.; Kumar Barman, R.; Sumon Kumar, D.; Rani Paul, T.; Khatun, A.; Rafiqul Islam, M.; Ashraf Ali, M.; Mokaddesur Rahman, B.; et al. Patterns of Prescription and Antibiotic Use among Outpatients in a Tertiary Care Teaching Hospital of Bangladesh Pharmacokinetic Evaluation of Drug Loaded Nanoparticle in Animal Models View Project Management Strategies of ACS Syndrome in Tertiary Care Ho. Artic. Int. J. Pharm. Pharm. Sci. 2016, 8, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Fahad, B. Antibiotic usage at a primary health care unit in Bangladesh. Australas. Med. J. 2010, 3, 414–421. [Google Scholar] [CrossRef]
- Rahman, M.S.; Begum, T.; Begum, R.; Islam, A. Antimicrobial and Analgesic Activity of Leaf Extracts of Phyllanthus Reticulatus Poir. (Family-Euphorbiaceae) View Project Evaluation of Gastroprotective and Wound Healing Potential of Phyllanthus niruri L. (Euphorbiaceae) Leaves in Experimental Rats View. Biol. Sci. 2016, 5, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Sayeed, M.A.; Iqbal, N.; Ali, M.S.; Rahman, M.M.; Islam, M.R.; Jakaria, M. Survey on Antibiotic Practices in Chittagong City of Bangladesh. Bangladesh Pharm. J. 2015, 18, 174–178. [Google Scholar] [CrossRef]
- Chowdhury, F.; Sturm-Ramirez, K.; Al Mamun, A.; Iuliano, A.D.; Chisti, M.J.; Ahmed, M.; Bhuiyan, M.U.; Hossain, K.; Haider, M.S.; Aziz, S.A.; et al. Effectiveness of an Educational Intervention to Improve Antibiotic Dispensing Practices for Acute Respiratory Illness among Drug Sellers in Pharmacies, a Pilot Study in Bangladesh. BMC Health Serv. Res. 2018, 18, 676. [Google Scholar] [CrossRef] [Green Version]
- Haque, M. Antimicrobial use, prescribing, and resistance in selected ten selected developing countries: A brief overview. Asian J. Pharm. Clin. Res. 2017, 10, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Biswas, M.; Roy, D.N.; Rahman, M.M.; Islam, M.; Parvez, G.M.; Haque, M.U.; Shahriar, A.A.E.; Ahmed, M.S.; Niloy, S.I. Doctor’s prescribing trends of antibiotics for out patients in Bangladesh: A cross-sectional health survey conducted in three districts. Int. J. Pharm. Sci. Res. 2014, 6, 669–675. [Google Scholar]
- Ahmed, S.; Korpe, P.; Ahmed, T.; Chisti, M.J.; Faruque, A.S.G. Burden and Risk Factors of Antimicrobial Use in Children Less Than 5 Years of Age with Diarrheal Illness in Rural Bangladesh. Am. J. Trop. Med. Hyg. 2018, 98, 1571. [Google Scholar] [CrossRef]
- Ata, M.; Hoque, R.; Biswas, R.S.R.; Mostafa, A.; Hasan, F.U.; Barua, H.R. Antibiotics Prescribing Pattern at Outpatient Department of A Tertiary Medical College Hospital. Chattagram Maa-O-Shishu Hosp. Med. Coll. J. 2018, 17, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Paul, T.; Imam Ibne Wahed, M.; Rani Paul, T.; Rana Hamid, M.; Shah Alam, M.; Lovely Nishuty, N.; Monjur Hossain, M.; Sarker, T.; Hosan, Z. Prescription pattern and use of antibiotics among pediatric out patients in rajshahi city of bangladesh. Int. J. Pharm. Sci. Res. 2018, 9, 3964. [Google Scholar] [CrossRef]
- Shamsuddin, A.K. Current Trend of Antibiotic Practice in Paediatric Surgery, Banladesh. IOSR J. Dent. Med. Sci. 2019, 18, 28–32. [Google Scholar]
- Hossain, M.; Mehdi Hasan, M.; Rasel Bin Mahabub Zaman, A.; Ar Rashid, H.; Al Rasel Bin Mahabub Zaman, C. Indication-based use of antibiotic in the treatment of patients attending at the primary health care facility. Pharma Innov. J. 2018, 7, 405–410. [Google Scholar]
- Rashid, M.M.; Chisti, M.J.; Akter, D.; Sarkar, M.; Chowdhury, F. Antibiotic Use for Pneumonia among Children Under-Five at a Pediatric Hospital in Dhaka City, Bangladesh. Patient Prefer. Adherence 2017, 11, 1335. [Google Scholar] [CrossRef] [Green Version]
- Hoque, R.; Mostafa, A.; Haque, M. Intern Doctors’ Views on the Current and Future Antibiotic Resistance Situation of Chattagram Maa O Shishu Hospital Medical College, Bangladesh. Ther. Clin. Risk Manag. 2015, 11, 1177. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S. Irrational Use of Drugs, Healthcare Level and Healthcare Expenditure in Bangladesh. Int. J. Health Econ. Policy 2017, 2, 152–158. [Google Scholar] [CrossRef]
- Afreen, S.; Rahman, M.S. Adherence to Treatment Guidelines in a University Hospital: Exploration of Facts and Factors. Bangladesh J. Pharmacol. 2014, 9, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.M.; Islam, Q.S. Availability and Rational Use of Drugs in Primary Healthcare Facilities Following the National Drug Policy of 1982: Is Bangladesh on Right Track? J. Health Popul. Nutr. 2012, 30, 99. [Google Scholar] [CrossRef] [Green Version]
- Basher, A.; Faiz, M.A. Antimicrobial Resistance: Bangladesh Experience. Reg. Health Forum 2011, 15, 1–8. [Google Scholar]
- Chouduri, A.U.; Biswas, M.; Haque, M.U.; Arman, M.S.I.; Uddin, N.; Kona, N.; Akter, R.; Haque, A. Cephalosporin-3G, Highly Prescribed Antibiotic to Outpatients in Rajshahi, Bangladesh: Prescription Errors, Carelessness, Irrational Uses Are the Triggering Causes of Antibiotic Resistance. J. Appl. Pharm. Sci. 2018, 8, 105–112. [Google Scholar] [CrossRef]
- Bishwajit Sutradhar, K.; Saha, A.; Hasan Huda, N.; Uddin, R. Irrational Use of Antibiotics and Antibiotic Resistance in Southern Rural Bangladesh: Perspectives from Both the Physicians and Patients. Orig. Res. Artic. Annu. Res. Rev. Biol. 2014, 4, 1421–1430. [Google Scholar] [CrossRef]
- Saha, M.R.; Sarwar, S.; Shill, M.C.; Shahriar, M. Patients’ Knowledge and Awareness towards Use of Antibiotics in Bangladesh: A Cross-Sectional Study Conducted in Three Tertiary Healthcare Centers in Bangladesh. Stamford J. Pharm. Sci. 2010, 3, 54–58. [Google Scholar] [CrossRef]
- Biswas, M.; Roy, M.N.; Manik, M.I.N.; Hossain, M.S.; Tapu, S.T.A.; Moniruzzaman, M.; Sultana, S. Self Medicated Antibiotics in Bangladesh: A Cross-Sectional Health Survey Conducted in the Rajshahi City. BMC Public Health 2014, 14, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishat, C.; Rashedul, M.I. Prevalence of Self-Medication of Antibiotics among People in Bangladesh. Indian J. Pharm. Pract. 2013, 4, 504–510. [Google Scholar]
- Anwar, M.; Islam, U. Prevalence, Practice and Irrationality of Self-Medicated Antibiotics among People in Northern and Southern Region of Bangladesh. Int. J. Res. Pharm. Biosci. 2017, 4, 17–24. [Google Scholar]
- Rana, M.M.; Karim, M.R.; Islam, M.R.; I Mondal, M.N.; Wadood, M.A.; A Bakar, S.M.; Hossain, M.G.; Chakrabarty, S.; Masud Rana, M.; Rafiqul Islam, M.; et al. Human Biology Review Original Scientific Paper. Hum. Biol. Rev. 2018, 7, 259–271. [Google Scholar]
- Saha, T.; Saha, T. Awareness Level of Patients Regarding Usage of Antibiotics in a Slum Area of Dhaka City, Bangladesh Formulation Development View Project Hospital Pharmacy Management and Futuristic Approach with Newer Ideas View Project Awareness Level of Patients Regardi. SSRG Int. J. Med. Sci. 2018, 5, 10–16. [Google Scholar]
- Begum, N.; Shamsuzzaman, S.M. Emergence of Carbapenemase-Producing Urinary Isolates at a Tertiary Care Hospital in Dhaka, Bangladesh. Tzu Chi Med. J. 2016, 28, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Mannan, A.; Shohel, M.; Rajia, S.; Mahmud, N.U.; Kabir, S.; Hasan, I. A Cross Sectional Study on Antibiotic Resistance Pattern of Salmonella Typhi Clinical Isolates from Bangladesh. Asian Pac. J. Trop. Biomed. 2014, 4, 306–311. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.S.; Huda, S. Antimicrobial Resistance and Related Issues: An Overview of Bangladesh Situation. Bangladesh J. Pharmacol. 2014, 9, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, B.; Akhter, M.; Hasan, M.; Khorshed Alam, M.; Professor, A. Sensitivity Pattern of Urinary Tract Pathogens to Anti-Microbial Drugs at a Tertiary Level Hospital in Bangladesh. J. Dhaka Natl. Med. Coll. Hosp. 2011, 17, 18–21. [Google Scholar] [CrossRef] [Green Version]
- Shahriar, M.; Hossain, M.; Kabir, S. A Survey on Antimicrobial Sensitivity Pattern of Different Antibiotics on Clinical Isolates of Escherichia coli Collected from Dhaka City, Bangladesh. J. Appl. Sci. Environ. Manag. 2010, 14, 19–20. [Google Scholar] [CrossRef] [Green Version]
- Tarana, M.N.; Shumu, S.J.; Khanam, R.A.; Jahan, H.; Sarker, S.; Bhowmic, D.; Sarwar, S. Antimicrobial Susceptibility Pattern for Salmonella Typhi Isolated from Blood in Shaheed Suhrawardy Medical College, Dhaka. J. Shaheed Suhrawardy Med. Coll. 2018, 10, 96–98. [Google Scholar] [CrossRef]
- Nahar, A.; Hasnat, S.; Akhter, H.; Begum, N.; Professor, A. Evaluation of Antimicrobial Resistance Pattern of Uropathogens in a Tertiary Care Hospital in Dhaka City, Bangladesh. South East Asia J. Public Health 2017, 7, 12–18. [Google Scholar] [CrossRef]
- Cardos, I.A.; Zaha, D.C.; Sindhu, R.K.; Cavalu, S. Revisiting Therapeutic Strategies for H. pylori Treatment in the Context of Antibiotic Resistance: Focus on Alternative and Complementary Therapies. Molecules 2021, 26, 6078. [Google Scholar] [CrossRef]
- Hosen, M.S.; Bachar, S.C. The Resistance Growing Trend of Common Gram-Negative Bacteria to the Potential Antibiotics over Three Consecutive Years: A Single Center Experience in Bangladesh. Pharm. Pharmacol. Int. J. 2019, 7, 114–119. [Google Scholar] [CrossRef] [Green Version]
- Jyoti Joshi. Antibiotic Use and Resistance in Bangladesh: Situation Analysis and Recommendations-Center for Disease Dynamics, Economics & Policy (CDDEP). 2018. Available online: https://cddep.org/publications/bangladesh-situation-analysis-amr/ (accessed on 29 March 2022).
- Islam, A.; Saifuddin, A.K.M.; Al Faruq, A.; Islam, S.; Shano, S.; Alam, M.; Hassan, M.M. Antimicrobial Residues in Tissues and Eggs of Laying Hens at Chittagong, Bangladesh. Int. J. One Health 2016, 2, 75–80. [Google Scholar] [CrossRef]
- Sattar, S.; Mahmudul Hassan, M.; Azizul Islam, S.K.M.; Alam, M.; Shohel Al Faruk, M.; Chowdhury, S.; Saifuddin, A.K.M. Antibiotic Residues in Broiler and Layer Meat in Chittagong District of Bangladesh. Vet. World 2014, 7, 738–743. [Google Scholar] [CrossRef] [Green Version]
- Hossen, M.S.; Hoque, Z.; Nahar, B.S. Assessment of Poultry Waste Management in Trishal Upazila, Mymensingh. Res. Agric. Livest. Fish. 2015, 2, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Motaher Hossain, M.; Apurbo Barman, A.K.; Matiur Rahim, M.; Tariqul Hassan, M.; Begum, M.; Bhattacharjee, D. Oxytetracycline Residues in Thai Pangas Pangasianodon Hypophthalmus Sampled from Sylhet Sadar Upazila, Bangladesh. Bangladesh J. Zool. 2018, 46, 81–90. [Google Scholar] [CrossRef]
- Ahmed, T.; Kanta Das, K.; Acharjee, M.; Jahan Urmi, N.; Sakil Munna, M.; Majibur Rahman, M.; Noor, R. Assessment of Microbiological Proliferation and in Vitro Demonstration of the Antimicrobial Activity of the Commonly Available Salad Vegetables within Dhaka Metropolis. Bangladesh. Am. J. Agric. For. 2014, 2, 55–60. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.A.; Islam, M.; Hasan, R.; Hossain, M.I.; Nabi, A.; Rahman, M.; Goessens, W.H.F.; Endtz, H.P.; Boehm, A.B.; Faruque, S.M. Environmental Spread of New Delhi Metallo-β- Lactamase-1-Producing Multidrug-Resistant Bacteria in Dhaka, Bangladesh. Appl. Environ. Microbiol. 2017, 83, e00793-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashid, M.; Rakib, M.M.; Hasan, B. Antimicrobial-Resistant and ESBL-Producing Escherichia coli in Different Ecological Niches in Bangladesh. Infect. Ecol. Epidemiol. 2015, 5, 26712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neela, F.A.; Banu, N.A.; Rahman, A.; Rahman, M.H.; Alam, M.F. Occurrence of Antibiotic Resistant Bacteria in Pond Water Associated with Integrated Poultry-Fish Farming in Bangladesh. Sains. Malays. 2015, 44, 371–377. [Google Scholar] [CrossRef]
- Haque, A.; Yoshizumi, A.; Saga, T.; Ishii, Y.; Tateda, K. ESBL-Producing Enterobacteriaceae in Environmental Water in Dhaka, Bangladesh. J. Infect. Chemother. 2014, 20, 735–737. [Google Scholar] [CrossRef]
- Hoque, R.; Ahmed, S.M.; Naher, N.; Islam, M.A.; Rousham, E.K.; Islam, B.Z.; Hassan, S. Tackling Antimicrobial Resistance in Bangladesh: A Scoping Review of Policy and Practice in Human, Animal and Environment Sectors. PLoS ONE 2020, 15, e0227947. [Google Scholar] [CrossRef] [Green Version]
- Bhowmik, P.; Ahaduzzaman, M.; Hasan, R.B. A cross sectional anthropo-clinical study on antimicrobials prescription pattern in goat patients at chittagong, bangladesh. Bangladesh J. Vet. Med. 2017, 15, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Hassan, M.M.; Al Faruq, A.; Alam, M.; Begum, S.; Mahmud, T.; Islam, A.; Coelho, A.C. Fatima Mukhtar. Bangladesh Artic. Microbiol. Res. J. Int. March 2019, 26, 1–8. [Google Scholar] [CrossRef]
- Huda, T.; Khan, J.A.M.; Ahsan, K.Z.; Jamil, K.; Arifeen, S. El Monitoring and Evaluating Progress towards Universal Health Coverage in Bangladesh. PLoS Med. 2014, 11, e1001722. [Google Scholar] [CrossRef]
- Report of the Household Income and Expenditure Survey. 2010. Available online: http://203.112.218.65:8008/WebTestApplication/userfiles/Image/LatestReports/HIES-10.pdf (accessed on 29 March 2022).
- Haque, M.; Godman, B. Potential Strategies to Improve Antimicrobial Utilisation in Hospitals in Bangladesh Building on Experiences Across Developing Countries. Bangladesh J. Med. Sci. 2021, 20, 469–477. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Mode of Action | Antimicrobial Groups |
|---|---|---|
| 1 | Cell wall synthesis inhibitor | -lactams: Penicillin, Cephalosporins, monobactams, carbapenemsGlycopeptides: Vancomycin |
| 2 | Depolarization of cell membrane | Lipopeptide |
| 3 | Protein synthesis inhibitors |
Bind to 30 s ribosomal subunit:
|
| 4 | Nucleic acid synthesis inhibitor | Quinolones, Fluoroquinolones |
| 5 | Inhibitors of metabolic pathways | Sulfonamides, Trimethoprim |
| No. | Name of Antimicrobials | Structure | Genes | Reference |
|---|---|---|---|---|
| 1 | Rifampicin |  | drrABC | [43] |
| rpoB | [44] | |||
| 2 | Benzothiazinones |  | dprE1 | [45] |
| 3 | Ethambutol | aftA | [46] | |
 | embABC | [47] | ||
| ubiA | [46] | |||
| 4 | Para-aminosalicylic acid (PASA) | thyA | [48] | |
 | ribD | |||
| folC | ||||
| 5 | D-cycloserine |  | ald | [49] |
| ddl | [50] | |||
| alr | [51] | |||
| 6 | Fucidic acid |  | far1/fusB | [52] |
| 7 | Glycylcycline |  | tetK | [52] |
| 8 | Ethionamide |  | mshC | [53] |
| 9 | Tetracycline |  | tetM | [52] |
| 10 | Pyrazinamide |  | pncA | [54] |
| 11 | Penicillin |  | blaZ | [52] |
| 12 | Streptomycin |  | aadA1 | [55] |
| 13 | Chloramphenicol |  | cat | [52] |
| 14 | Methicillin |  | mecA | [52] |
| 15 | Isoniazid |  | katG | [56] |
| inhA | [57] | |||
| fabG1 | [58] |
| Antimicrobial Groups | Examples | Mechanism of Resistance |
|---|---|---|
| Penicillins, Cephalosporins, Carbapenems, Monobactams | Hydrolysis, efflux, altered target | |
| Aminoglycosides | Streptomycin, Gentamycin | Altered target, acetylation, efflux |
| Tetracyclines | Minocycline, Tigecycline | Efflux, altered target, hydrolysis |
| Lincosamides | Clindamycin | Efflux, altered target |
| Macrolides | Erythromycin, azithromycin | Hydrolysis, efflux, altered target |
| Phenols | Chloramphenicol | Acetylation, efflux, altered target |
| Quinolones | Ciprofloxacin | Acetylation, efflux, altered target |
| Pyrimidines | Trimethroprim | Efflux, altered target |
| Sulfonamides | Sulfamethoxazole | Efflux, altered target |
| First Author (Ref) | Resistant Microorganisms | Dose New Antibiotic (n Patient) | Comparator, Dose (n Patient) | Definition Outcome | Timing Assessment of Outcomes | Outcomes (New Antibiotics vs. Comparator) |
|---|---|---|---|---|---|---|
| A comparative study with Plazomicin | ||||||
| Wagenlehner [74] | ESBL 26.5% CRE 4.8% | 15 mg/kg IV, QD (n = 306) | Meropenem 1 g IV, TID (n = 303) | Clinical cure and microbiological response | 15 to 19 days after the start of therapy | 81.7% vs. 70.1% |
| Conolly [75] | Ceftazidime non-susceptible 17.6% | 15 mg/kg IV, QD (n = 51) | Levofloxacin 750 mg IV, QD (n = 29) | Microbiological eradication rate | 12 days after the last dose | 60.8% vs. 58.6% |
| A comparative study with Eravacycline | ||||||
| Clinical trial identifier NCT03032510 | No information | 1.5 mg/kg IV, QD + levofloxacin PO (n = 603). | Ertapenem 1 g IV, QD + levofloxacin PO (n = 602). | Clinical cure and microbiological response | 14 to 17 days post randomization | 84.8% vs. 94.8% |
| Clinical trial identifier NCT01978938 | No information | 1.5 mg/kg IV, QD (n = 455). | Levofloxacin 750 mg IV, QD (n = 453). | Clinical cure and microbiological response | Post-treatment visit | 60.4% vs. 66.9% |
| A comparative study with Cefiderocol | ||||||
| Portsmouth [76] | No information | 2 g IV, TID (n = 252) | Imipenem-cilastatin 1 g IV, TID (n = 119) | Clinical cure and microbiological response | 7 ± 2 days after the end of antibiotic treatment | 73% vs. 55% |
| A comparative study with Ceftazidime/avibactam | ||||||
| Carmeli [77] a | Ceftazidime non-susceptible Enterobacterales or P. aeruginosa 100% | 2 g/500 mg IV, TD (n = 165) | Best available therapy (97% carbapenems) (n = 168) | Clinical response | 7 to 10 days after the last infusion | 91% vs. 91% |
| Wagenlehner [78] | Ceftazidime non-susceptible 19.6% | 2 g/500 mg IV, TD (n = 393) | Doripenem 500 mg IV, TD (n = 417) | Clinical cure and microbiological response | 21 to 25 days post-randomization | 71.2% vs. 64.5% |
| Comparative study with Ceftolozane/tazobactam | ||||||
| Popejoy [79] | ESBL 11.1% | 1 g/500 mg IV, TD (n = 54) | Levofloxacin 750 mg IV, QD (n = 46) Meropenem 1 g, IV, TD (n = 26) | Clinical cure | 5 to 9 days post therapy | 95.8% vs. 82.6% (p = 0.01) |
| Wagenlehner [80] | ESBL 14.8% | 1 g/500 mg IV, TD (n = 398) | Levofloxacin 750 mg IV, QD (n = 402) | Clinical cure and microbiological response | 5 to 9 days post-therapy | 76.9% vs. 68.4% |
| A comparative study with Meropenem/tazobactam | ||||||
| Kaye [81] | Piperacillin/tazobactam-resistant E. coli and K. pneumoniae 15% | 2 g/2 g IV, TD (n = 274) | Piperacillin/tazobactam 4 g/500 mg IV, TD (n = 276) | Clinical cure and microbiological response | End of intravenous treatment | 98.4% vs. 94.0% |
| Wunderink [82] b | Multicenter study (27 CRE 78.7% | 2 g/2 g IV, TD (n = 32) | Best available therapy (n = 15) (46.7% dual therapy) | Cure rates | At day 28 | 65.6% vs. 33.3% (95% CI: 3.3. to 61.3) |
| Comparative study with Imipenem+ cilastatin/relebactam | ||||||
| Motsch [83] c | Imipenem-nonsusceptible microorganisms 100% | 500 mg/250 mg IV, QD (n = 31) | Colistimethate Sodium + imipenem + cilastatin loading dose 300 mg colistin base activity, followed by maintenance doses up to 150 mg colistin base activity, IV, BD (n = 16) | Clinical and microbiological response Survival (HAP/VAP) Clinical response (cIAI) | On therapy visit (cUTI) On day 28 (HAP/VAP and cIAI) | 71.4% vs. 70.0% Favorable overall response against P. aeruginosa: 81% vs. 63% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, M.M.; Alam Tumpa, M.A.; Zehravi, M.; Sarker, M.T.; Yamin, M.; Islam, M.R.; Harun-Or-Rashid, M.; Ahmed, M.; Ramproshad, S.; Mondal, B.; et al. An Overview of Antimicrobial Stewardship Optimization: The Use of Antibiotics in Humans and Animals to Prevent Resistance. Antibiotics 2022, 11, 667. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11050667
Rahman MM, Alam Tumpa MA, Zehravi M, Sarker MT, Yamin M, Islam MR, Harun-Or-Rashid M, Ahmed M, Ramproshad S, Mondal B, et al. An Overview of Antimicrobial Stewardship Optimization: The Use of Antibiotics in Humans and Animals to Prevent Resistance. Antibiotics. 2022; 11(5):667. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11050667
Chicago/Turabian StyleRahman, Md. Mominur, Mst. Afroza Alam Tumpa, Mehrukh Zehravi, Md. Taslim Sarker, Md. Yamin, Md. Rezaul Islam, Md. Harun-Or-Rashid, Muniruddin Ahmed, Sarker Ramproshad, Banani Mondal, and et al. 2022. "An Overview of Antimicrobial Stewardship Optimization: The Use of Antibiotics in Humans and Animals to Prevent Resistance" Antibiotics 11, no. 5: 667. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11050667