
Management of Helicobacter Pylori Infection and Effectiveness Rates in Daily Clinical Practice in Spain: 2010–2019

 ,
,
Abstract
:1. Introduction

{kind=link}
{kind=link}
| IISCC2005[5] | IIISCC2013[6] | IVSCC2016[7] |
| PCA 7–10 days | PCAM 10 days | PCAM 10–14 days PBMT 10 days |
| Maastricht III2007[10] | Maastricht IV2012[11] | Maastricht V2016[12] |
| PC A/M >7 days | PCA 10–14 days PBMT | PCAM 10–14 days PBMT 10–14 days |
2. Results
2.1. Baseline Characteristics
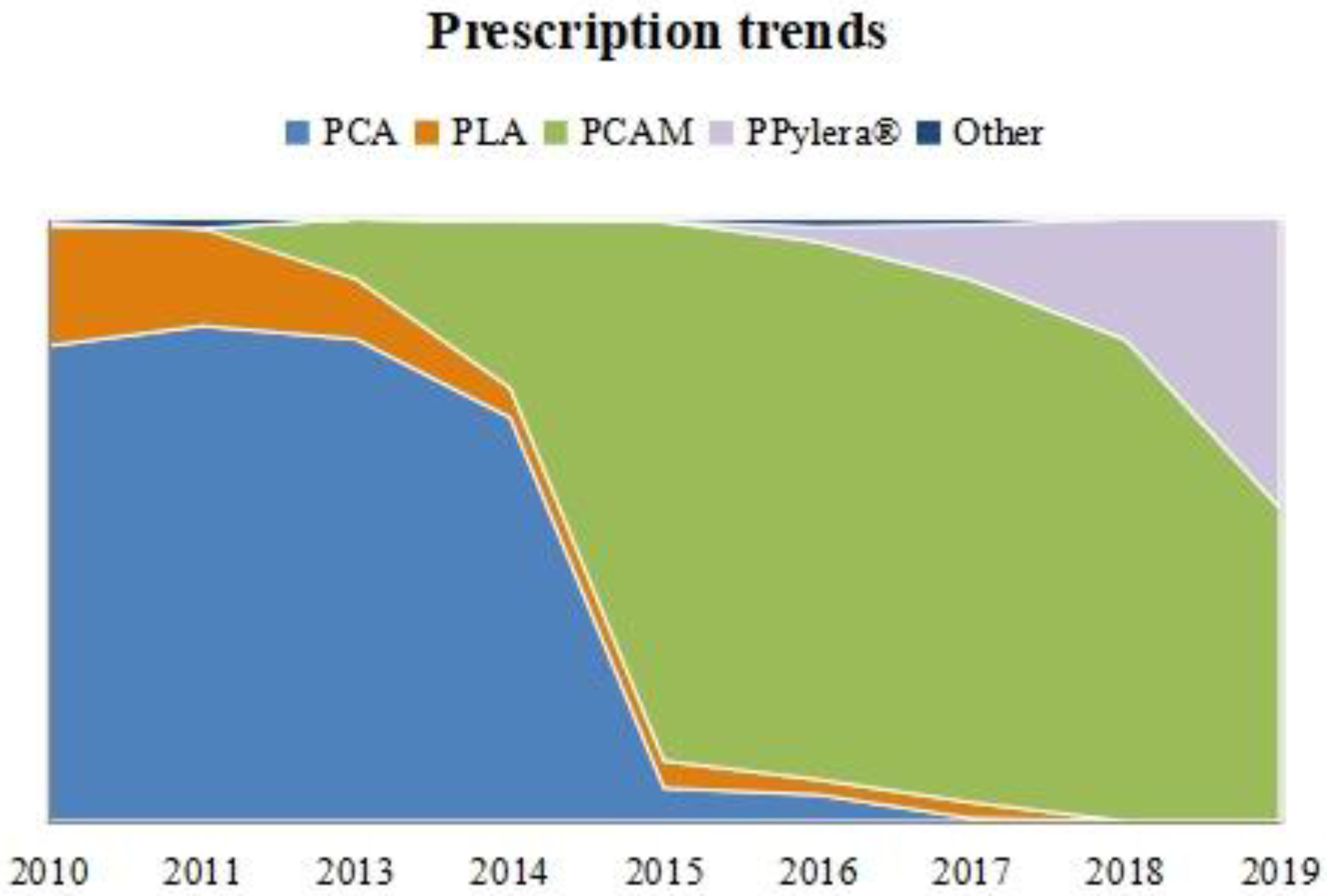
2.2. First-Line Prescription Trends
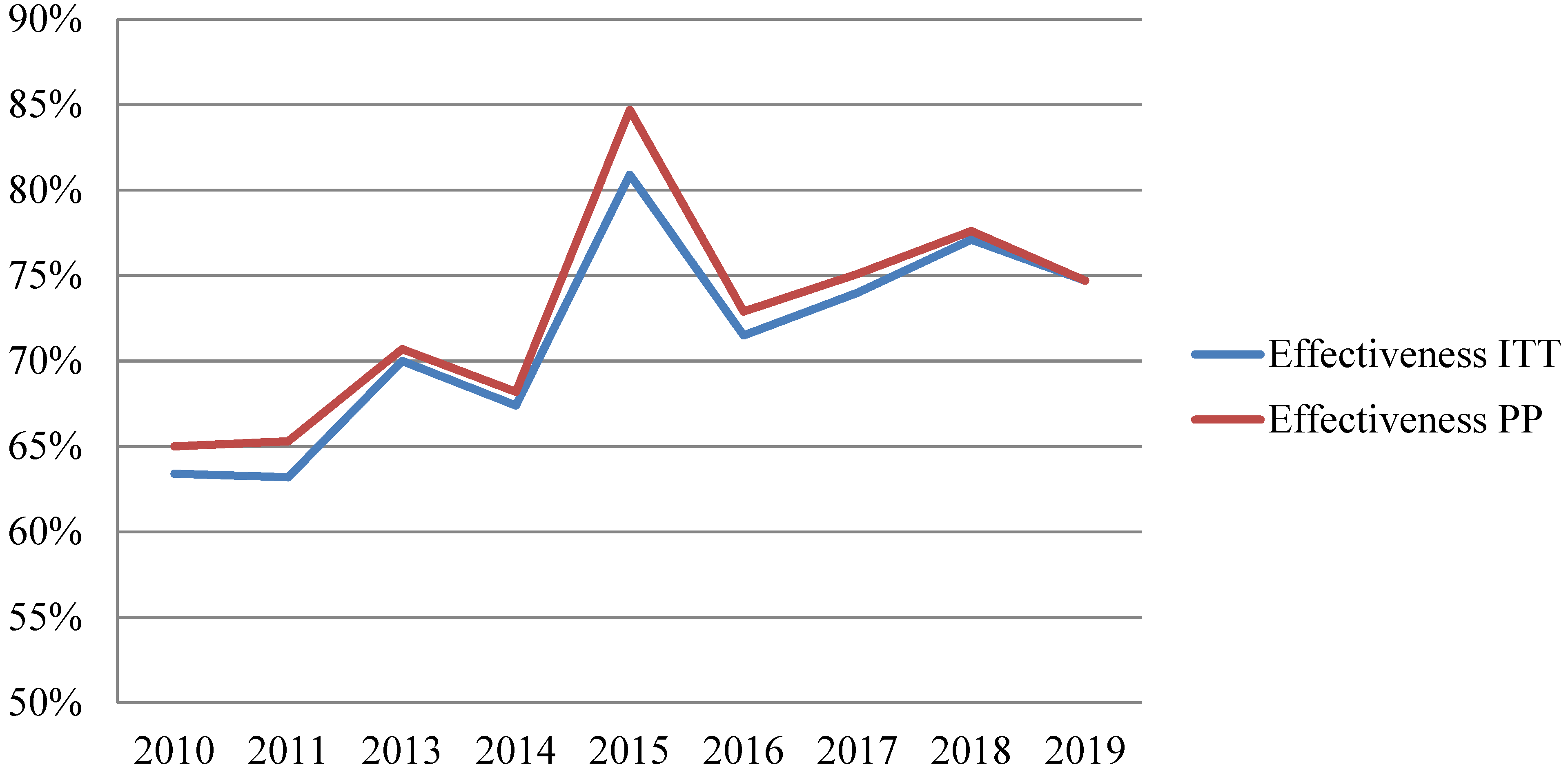
2.3. Effectiveness Analysis
2.3.1. First-Line Eradication Rates
2.3.2. Effectiveness Analysis Based on Other Variables
3. Discussion
3.1. PCA
3.2. PCAM
3.3. PBMT–PPYLERA®
3.4. PLA
3.5. Strengths and Weaknesses
4. Materials and Methods
4.1. Study Design
4.2. Variables
4.3. Definition of Agreement with Guidelines
- First triene (2010–August 2013, and 6 months after the III (third) Spanish Consensus Conference (SCC) publication): PCA (PPI + Clarithromycin + Amoxicillin);
- Second triene (February 2013–November 2016, and 6 months after the IV SCC publication): PCAM(PPI + Clarithromycin + Amoxicillin + Metronidazole);
- Third triene (May 2016–December 2019): PPylera ® (PPI + Pylera®, the three-in-one capsule containing Bismuth Subcitrate + Metronidazole + Tetracycline).
4.4. Statistical Analysis and Ethics Statement
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zamani, M.; Ebrahimtabar, F.; Zamani, V.; Miller, W.H.; Alizadeh-Navaei, R.; Shokri-Shirvani, J.; Derakhshan, M.H. Systematic Review with Meta-Analysis: The Worldwide Prevalence of Helicobacter Pylori Infection. Aliment. Pharmacol. Ther. 2018, 47, 868–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrara, P.; Agüero, F.; Masuet-Aumatell, C.; Ramon-Torrell, J.M. Burden of Cancer Mortality Attributable to Carcinogenic Infections in Spain. Med. Clin. 2020, 154, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Megraud, F.; Bruyndonckx, R.; Coenen, S.; Wittkop, L.; Huang, T.-D.; Hoebeke, M.; Bénéjat, L.; Lehours, P.; Goossens, H.; Glupczynski, Y.; et al. Helicobacter Pylori Resistance to Antibiotics in Europe in 2018 and Its Relationship to Antibiotic Consumption in the Community. Gut 2021, 70, 1815–1822. [Google Scholar] [CrossRef] [PubMed]
- Nyssen, O.P.; Bordin, D.; Tepes, B.; Pérez-Aisa, Á.; Vaira, D.; Caldas, M.; Bujanda, L.; Castro-Fernandez, M.; Lerang, F.; Leja, M.; et al. European Registry on Helicobacter Pylori Management (Hp-EuReg): Patterns and Trends in First-Line Empirical Eradication Prescription and Outcomes of 5 Years and 21 533 Patients. Gut 2021, 70, 40–54. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Calvet, X.; Gomollón, F.; Monés, J.; Grupo Conferencia Española de Consenso sobre Helicobacter Pylori. Tratamiento erradicador de Helicobacter pylori. Recommendations of the II Spanish Consensus Conference. Med. Clin. 2005, 125, 301–316. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Calvet, X.; Bermejo, F.; Boixeda, D.; Bory, F.; Bujanda, L.; Castro-Fernández, M.; Dominguez-Muñoz, E.; Elizalde, J.I.; Forné, M.; et al. III Spanish Consensus Conference on Helicobacter Pylori infection. Gastroenterol. Hepatol. 2013, 36, 340–374. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Molina-Infante, J.; Amador, J.; Bermejo, F.; Bujanda, L.; Calvet, X.; Castro-Fernández, M.; Cuadrado-Lavín, A.; Elizalde, J.I.; Gene, E.; et al. IV Conferencia Española de Consenso sobre el tratamiento de la infección por Helicobacter Pylori. Gastroenterol. Y Hepatol. 2016, 39, 697–721. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Alcedo, J.; Amador, J.; Bujanda, L.; Calvet, X.; Castro-Fernández, M.; Fernández-Salazar, L.; Gené, E.; Lanas, Á.; Lucendo, A.J.; et al. V Spanish Consensus Conference on Helicobacter Pylori Infection Treatment. Gastroenterol. Hepatol. 2022, 45, 392–417. [Google Scholar] [CrossRef]
- McNicholl, A.G.; O’Morain, C.A.; Megraud, F.; Gisbert, J.P. As Scientific Committee of the Hp-Eureg on Behalf of the National Coordinators Protocol of the European Registry on the Management of Helicobacter Pylori Infection (Hp-EuReg). Helicobacter 2019, 24, e12630. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.; Bazzoli, F.; El-Omar, E.; Graham, D.; Hunt, R.; Rokkas, T.; Vakil, N.; Kuipers, E.J. Current Concepts in the Management of Helicobacter Pylori Infection: The Maastricht III Consensus Report. Gut 2007, 56, 772–781. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Atherton, J.; Axon, A.T.R.; Bazzoli, F.; Gensini, G.F.; Gisbert, J.P.; Graham, D.Y.; Rokkas, T.; et al. Management of Helicobacter Pylori Infection—The Maastricht IV/ Florence Consensus Report. Gut 2012, 61, 646–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter Pylori Infection—The Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mentis, A.; Lehours, P.; Mégraud, F. Epidemiology and Diagnosis of Helicobacter Pylori Infection. Helicobacter 2015, 20, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, A.C.; Marwaha, A.; Sood, R.; Moayyedi, P. Global Prevalence of, and Risk Factors for, Uninvestigated Dyspepsia: A Meta-Analysis. Gut 2015, 64, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Moayyedi, P.; Lacy, B.E.; Andrews, C.N.; Enns, R.A.; Howden, C.W.; Vakil, N. ACG and CAG Clinical Guideline: Management of Dyspepsia. Am. J. Gastroenterol. 2017, 112, 988–1013. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Calvet, X. Review Article: The Effectiveness of Standard Triple Therapy for Helicobacter Pylori Has Not Changed over the Last Decade, but It Is Not Good Enough. Aliment. Pharmacol. Ther. 2011, 34, 1255–1268. [Google Scholar] [CrossRef]
- Calvet, X.; López-Lorente, M.-T.; Cubells, M.-J.; Barè, M.; Gálvez, E.; Molina, E. Two-Week Dual vs. One-Week Triple Therapy for Cure of Helicobacter Pylori Infection in Primary Care: A Multicentre, Randomized Trial. Aliment. Pharmacol. Ther. 1999, 13, 781–786. [Google Scholar] [CrossRef]
- Martos, M.; Bujanda, L.; Salicio, Y.; Sarasqueta, C.; Ibarra, B.; Mendarte, U.; Fernández-Reyes, M.; Cosme, A. Clarithromycin for First-Line Treatment of Helicobacter Pylori Infection after Culture in High-Resistance Regions. Eur. J. Gastroenterol. Hepatol. 2014, 26, 1380–1384. [Google Scholar] [CrossRef]
- Ducóns, J.A.; Santolaria, S.; Guirao, R.; Ferrero, M.; Montoro, M.; Gomollón, F. Impact of Clarithromycin Resistance on the Effectiveness of a Regimen for Helicobacter Pylori: A Prospective Study of 1-Week Lansoprazole, Amoxycillin and Clarithromycin in Active Peptic Ulcer. Aliment. Pharmacol. Ther. 1999, 13, 775–780. [Google Scholar] [CrossRef]
- Martín Mir, M.L.; Val, J.; Fuentes, J.; García, S.; Yus, C.; Simón, M.A.; Gomollón, F. Effectiveness of the eradication of Helicobacter Pylori by treatment with omeprazol, amoxicillin, and clarithromycin according to dosage and administration schedule. Gastroenterol. Hepatol. 1998, 21, 432–436. [Google Scholar]
- Molina-Infante, J.; Lucendo, A.J.; Angueira, T.; Rodriguez-Tellez, M.; Perez-Aisa, A.; Balboa, A.; Barrio, J.; Martin-Noguerol, E.; Gomez-Rodriguez, B.J.; Botargues-Bote, J.M.; et al. Optimised Empiric Triple and Concomitant Therapy for Helicobacter Pylori Eradication in Clinical Practice: The OPTRICON Study. Aliment. Pharmacol. Ther. 2015, 41, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.W.; Ko, W.J.; Oh, C.H.; Park, Y.M.; Oh, S.J.; Moon, J.R.; Cho, J.-H.; Kim, J.-W.; Jang, J.-Y. Clarithromycin Resistance and Female Gender Affect Helicobacter Pylori Eradication Failure in Chronic Gastritis. Korean J. Intern. Med. 2019, 34, 1022–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, W.; Zhou, L.; Ren, W.; Deng, L.; Yu, M. Variables Influencing Outcome of Helicobacter Pylori Eradication Therapy in South China. Helicobacter 2009, 14, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Molina-Infante, J.; Pazos-Pacheco, C.; Vinagre-Rodriguez, G.; Perez-Gallardo, B.; Dueñas-Sadornil, C.; Hernandez-Alonso, M.; Gonzalez-Garcia, G.; Mateos-Rodriguez, J.M.; Fernandez-Bermejo, M.; Gisbert, J.P. Nonbismuth Quadruple (Concomitant) Therapy: Empirical and Tailored Efficacy versus Standard Triple Therapy for Clarithromycin-Susceptible Helicobacter Pylori and versus Sequential Therapy for Clarithromycin-Resistant Strains. Helicobacter 2012, 17, 269–276. [Google Scholar] [CrossRef]
- McNicholl, A.G.; Marin, A.C.; Molina-Infante, J.; Castro, M.; Barrio, J.; Ducons, J.; Calvet, X.; de la Coba, C.; Montoro, M.; Bory, F.; et al. Randomised Clinical Trial Comparing Sequential and Concomitant Therapies for Helicobacter Pylori Eradication in Routine Clinical Practice. Gut 2014, 63, 244–249. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Calvet, X. Review Article: Non-Bismuth Quadruple (Concomitant) Therapy for Eradication of Helicobater Pylori. Aliment. Pharmacol. Ther. 2011, 34, 604–617. [Google Scholar] [CrossRef]
- Toros, A.B.; İnce, A.T.; Kesici, B.; Saglam, M.; Polat, Z.; Uygun, A. A New Modified Concomitant Therapy for Helicobacter Pylori Eradication in Turkey. Helicobacter 2011, 16, 225–228. [Google Scholar] [CrossRef]
- Heo, J.; Jeon, S.W.; Jung, J.T.; Kwon, J.G.; Lee, D.W.; Kim, H.S.; Yang, C.H.; Park, J.B.; Park, K.S.; Cho, K.B.; et al. Concomitant and Hybrid Therapy for Helicobacter Pylori Infection: A Randomized Clinical Trial. J. Gastroenterol. Hepatol. 2015, 30, 1361–1366. [Google Scholar] [CrossRef]
- Macías-García, F.; Bastón-Rey, I.; de la Iglesia-García, D.; Calviño-Suárez, C.; Nieto-García, L.; Domínguez-Muñoz, J.E. Bismuth-Containing Quadruple Therapy versus Concomitant Quadruple Therapy as First-Line Treatment for Helicobacter Pylori Infection in an Area of High Resistance to Clarithromycin: A Prospective, Cross-Sectional, Comparative, Open Trial. Helicobacter 2019, 24, e12546. [Google Scholar] [CrossRef] [Green Version]
- Alcedo, J.; Gracia, M.; García-Cámara, P.; Palacín, C.; Gallego, S.; Jimeno-Ayllon, C.; Frago, S.; Aured, I.; Luzón, L. Prospective comparative study between two first-line regimens for Helicobacter Pylori eradication: Non-bismuth quadruple versus bismuth quadruple therapy. Gastroenterol. Hepatol. 2020, 43, 301–309. [Google Scholar] [CrossRef]
- Molina–Infante, J.; Romano, M.; Fernandez–Bermejo, M.; Federico, A.; Gravina, A.G.; Pozzati, L.; Garcia–Abadia, E.; Vinagre–Rodriguez, G.; Martinez–Alcala, C.; Hernandez–Alonso, M.; et al. Optimized Nonbismuth Quadruple Therapies Cure Most Patients With Helicobacter Pylori Infection in Populations With High Rates of Antibiotic Resistance. Gastroenterology 2013, 145, 121–128.e1. [Google Scholar] [CrossRef] [PubMed]
- Nyssen, O.P.; Vaira, D.; Tepes, B.; Kupcinskas, L.; Bordin, D.; Pérez-Aisa, Á.; Gasbarrini, A.; Castro-Fernández, M.; Bujanda, L.; Garre, A.; et al. Room for Improvement in the Treatment of Helicobacter Pylori Infection: Lessons from the European Registry on: H. Pylori: Management (Hp-EuReg). J. Clin. Gastroenterol. 2021. In Press. [Google Scholar] [CrossRef] [PubMed]
- Shakya Shrestha, S.; Bhandari, M.; Thapa, S.R.; Shrestha, R.; Poudyal, R.; Purbey, B.; Gurung, R.B. Medication Adherence Pattern and Factors Affecting Adherence in Helicobacter Pylori Eradication Therapy. Kathmandu Univ. Med. J. 2016, 14, 58–64. [Google Scholar]
- Abbasinazari, M.; Sahraee, Z.; Mirahmadi, M. The Patients’ Adherence and Adverse Drug Reactions (ADRs) Which Are Caused by Helicobacter Pylori Eradication Regimens. J. Clin. Diagn Res. 2013, 7, 462–466. [Google Scholar] [CrossRef]
- Agudo-Fernández, S.; González Blanco, A. Retrospective Analysis of the Use of Quadruple Therapy with Bismuth (Pylera®) in Real-Life Clinical Practice in Spain. Gastroenterol. Hepatol. 2018, 41, 483–489. [Google Scholar] [CrossRef]
- Pérez-Arellano, E.; Rodriguez-Garcia, M.I.; Galera Rodenas, A.B.; de la Morena-Madrigal, E. Eradication of Helicobacter Pylori Infection with a New Bismuth-Based Quadruple Therapy in Clinical Practice. Gastroenterol. Hepatol. 2018, 41, 145–152. [Google Scholar] [CrossRef]
- Tursi, A.; Franceschi, M.; Allegretta, L.; Savarino, E.; De Bastiani, R.; Elisei, W.; Baldassarre, G.; Ferronato, A.; Scida, S.; Miraglia, C.; et al. Effectiveness and Safety of Pylera® in Patients Infected by Helicobacter Pylori: A Multicenter, Retrospective, Real Life Study. Dig Dis. 2018, 36, 264–268. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Fernández-Bermejo, M.; Molina-Infante, J.; Pérez-Gallardo, B.; Prieto-Bermejo, A.-B.; Mateos-Rodríguez, J.-M.; Robledo-Andrés, P.; González-García, G. First-Line Triple Therapy with Levofloxacin for Helicobacter Pylori Eradication. Alimentary Pharmacol. Ther. 2007, 26, 495–500. [Google Scholar] [CrossRef]
- Antos, D.; Schneider-Brachert, W.; Bästlein, E.; Hänel, C.; Haferland, C.; Buchner, M.; Meier, E.; Trump, F.; Stolte, M.; Lehn, N.; et al. 7-Day Triple Therapy of Helicobacter Pylori Infection with Levofloxacin, Amoxicillin, and High-Dose Esomeprazole in Patients with Known Antimicrobial Sensitivity. Helicobacter 2006, 11, 39–45. [Google Scholar] [CrossRef]
- Cammarota, G.; Cianci, R.; Cannizzaro, O.; Cuoco, L.; Pirozzi, G.; Gasbarrini, A.; Armuzzi, A.; Zocco, M.A.; Santarelli, L.; Arancio, F.; et al. Efficacy of Two One-Week Rabeprazole/Levofloxacin-Based Triple Therapies for Helicobacter Pylori Infection. Aliment. Pharmacol. Ther. 2000, 14, 1339–1343. [Google Scholar] [CrossRef]
- Telaku, S.; Manxhuka-Kerliu, S.; Kraja, B.; Qirjako, G.; Prifti, S.; Fejza, H. The Efficacy of Levofloxacin-Based Triple Therapy for First-Line Helicobacter Pylori Eradication. Med. Arch. 2013, 67, 348–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.-Y.; Wu, M.-S.; Chen, C.-Y.; Bair, M.-J.; Chou, C.-K.; Lin, J.-T.; Liou, J.-M. Systematic Review with Meta-Analysis: The Efficacy of Levofloxacin Triple Therapy as the First- or Second-Line Treatments of Helicobacter Pylori Infection. Aliment. Pharmacol. Ther. 2016, 44, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.-P.; Gu, M.; Zhang, G.-X. Is Levofloxacin-Based Triple Therapy an Alternative for First-Line Eradication of Helicobacter Pylori? A Systematic Review and Meta-Analysis. Scand. J. Gastroenterol. 2014, 49, 528–538. [Google Scholar] [CrossRef] [PubMed]


| Variables | Categories | ITT | PP | ||||
|---|---|---|---|---|---|---|---|
| N | % | 95% CI | N | % | 95% CI | ||
| Treatment | PCAM | 737 | 76.9% | 73.8–79.8 | 719 | 78,9% | 75.7–81.7 |
| PCA | 686 | 63.4% | 59.7–66.9 | 676 | 64.3% | 60.7–67.9 | |
| PLA | 123 | 69.1% | 60.5–76.6 | 120 | 70.8% | 62.2–78.2 | |
| PPylera® | 87 | 81.6% | 72.2–88.4 | 87 | 81.6% | 72.2–88.4 | |
| Other treatments | 11 | 36.4% | 15.2–64.6 | 9 | 44.4% | 18.9–73.3 | |
| p-value | <0.001 | <0.001 | |||||
| Duration | 7 days | 67 | 56.7% | 44.8–67.9 | 66 | 57.6% | 45.6–68.8 |
| 10 days | 612 | 72.9% | 69.2–76.2 | 598 | 74.6% | 70.9–77.9 | |
| 14 days | 333 | 82.3% | 77.8–86.0 | 329 | 83.3% | 78.9–86.9 | |
| p-value | <0.001 | <0.001 | |||||
| PPI | Omeprazole | 284 | 73.6% | 68.2–78.4 | 282 | 74.1% | 68.7–78.9 |
| Esomeprazole | 101 | 82.2% | 73.6–88.4 | 101 | 82.2% | 73.6–88.4 | |
| Other PPI | 61 | 70.5% | 58.1–80.4 | 61 | 70.5% | 58.1–80.4 | |
| p-value | 0.154 | 0.169 | |||||
| Sex | Female | 971 | 68.5% | 65.6–71.3 | 955 | 69.6% | 66.6–72.5 |
| Male | 673 | 73.8% | 70.4–77.0 | 656 | 75.8% | 72.3–78.9 | |
| p-value | 0.019 | 0.007 | |||||
| Center | Center 1 (Z) | 766 | 70.5% | 67.2–73.6 | 744 | 72.6% | 69.3–75.7 |
| Center 2 (T) | 878 | 70.8% | 67.8–73.8 | 867 | 71.7% | 68.7–74.6 | |
| p-value | 0.878 | 0.708 | |||||
| Age | <55 years | 962 | 69.6% | 66.7–72.5 | 938 | 71.4% | 68.5–74.2 |
| ≥55 years | 682 | 72.1% | 68.7–75.4 | 673 | 73.1% | 69.6–76.3 | |
| p-value | 0.274 | 0.459 | |||||
| Appropriateness | No | 388 | 65.7% | 60.9–70.3 | 381 | 66.9% | 62.1–71.5 |
| Yes | 1256 | 72.2% | 69.7–74.6 | 1230 | 73.7% | 71.2–76.1 | |
| p-value | 0.014 | 0.010 | |||||
| Total | 1644 | 70.7% | 68.4–72.8 | 1611 | 72.1% | 69.9–74.3 | |
| Univariate | Multivariate | ||||
|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| Treatment | [R: PCAM] | 1 | 1 | ||
| PCA | 0.520 (0.412–0.655) | <0.001 | 0.489 (0.376–0.636) | <0.001 | |
| PLA | 0.671 (0.441–1.020) | 0.062 | 0.595 (0.305–1.014) | 0.056 | |
| PPylera® | 1.330 (0.753–2.350) | 0.325 | 1.266 (0.714–2.243) | 0.420 | |
| Othertreatments | 0.171 (0.050–0.592) | 0.005 | 0.162 (0.05–0.587) | 0.006 | |
| Duration | [R: 7 days] | 1 | - | - | |
| 10 days | 2.050 (1.225–3.432) | 0.006 | |||
| 14 days | 3.544 (2.026–6.200) | <0.001 | - | - | |
| PPI | [R: Omeprazole] | 1 | |||
| Esomeprazole | 1.655 (0.932–2.937) | 0.085 | - | - | |
| Other PPI | 0.857 (0.466–1.578) | 0.621 | - | - | |
| Sex | [R: Female] | 1 | 1 | ||
| Male | 1.299 (1.044–1.617) | 0.021 | 1.270 (1.013–1.592) | 0.038 | |
| Center | [R: Center 1 (Z)] | 1 | 1 | ||
| Center 2 (T) | 1.017 (0.822–1.258) | 0.878 | 1.132 (0.902–1.419) | 0.284 | |
| Age | [R: <55 years] | ||||
| ≥55 years | 1.129 (0.090–1.401) | 0.274 | 1.106 (0.885–1.383 | 0.374 | |
| Appropriateness | [R: No] | 1 | 1 | ||
| Yes | 1.355 (1.063–1.729) | 0.014 | 0.893 (0.645–1.236) | 0.493 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ariño Pérez, I.; Martínez-Domínguez, S.J.; Alfaro Almajano, E.; Carrera-Lasfuentes, P.; Lanas, Á. Management of Helicobacter Pylori Infection and Effectiveness Rates in Daily Clinical Practice in Spain: 2010–2019. Antibiotics 2022, 11, 698. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11050698
Ariño Pérez I, Martínez-Domínguez SJ, Alfaro Almajano E, Carrera-Lasfuentes P, Lanas Á. Management of Helicobacter Pylori Infection and Effectiveness Rates in Daily Clinical Practice in Spain: 2010–2019. Antibiotics. 2022; 11(5):698. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11050698
Chicago/Turabian StyleAriño Pérez, Inés, Samuel J. Martínez-Domínguez, Enrique Alfaro Almajano, Patricia Carrera-Lasfuentes, and Ángel Lanas. 2022. "Management of Helicobacter Pylori Infection and Effectiveness Rates in Daily Clinical Practice in Spain: 2010–2019" Antibiotics 11, no. 5: 698. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11050698