Predicting In-Hospital Antibiotic Use in the Medical Department: Derivation and Validation Study

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design, Participants, and Data Collection
2.2. Outcome
2.3. Candidate Predictor Variables
2.4. Model Development and Statistical Analysis
2.5. Test of Model Performance and External Validation
3. Results
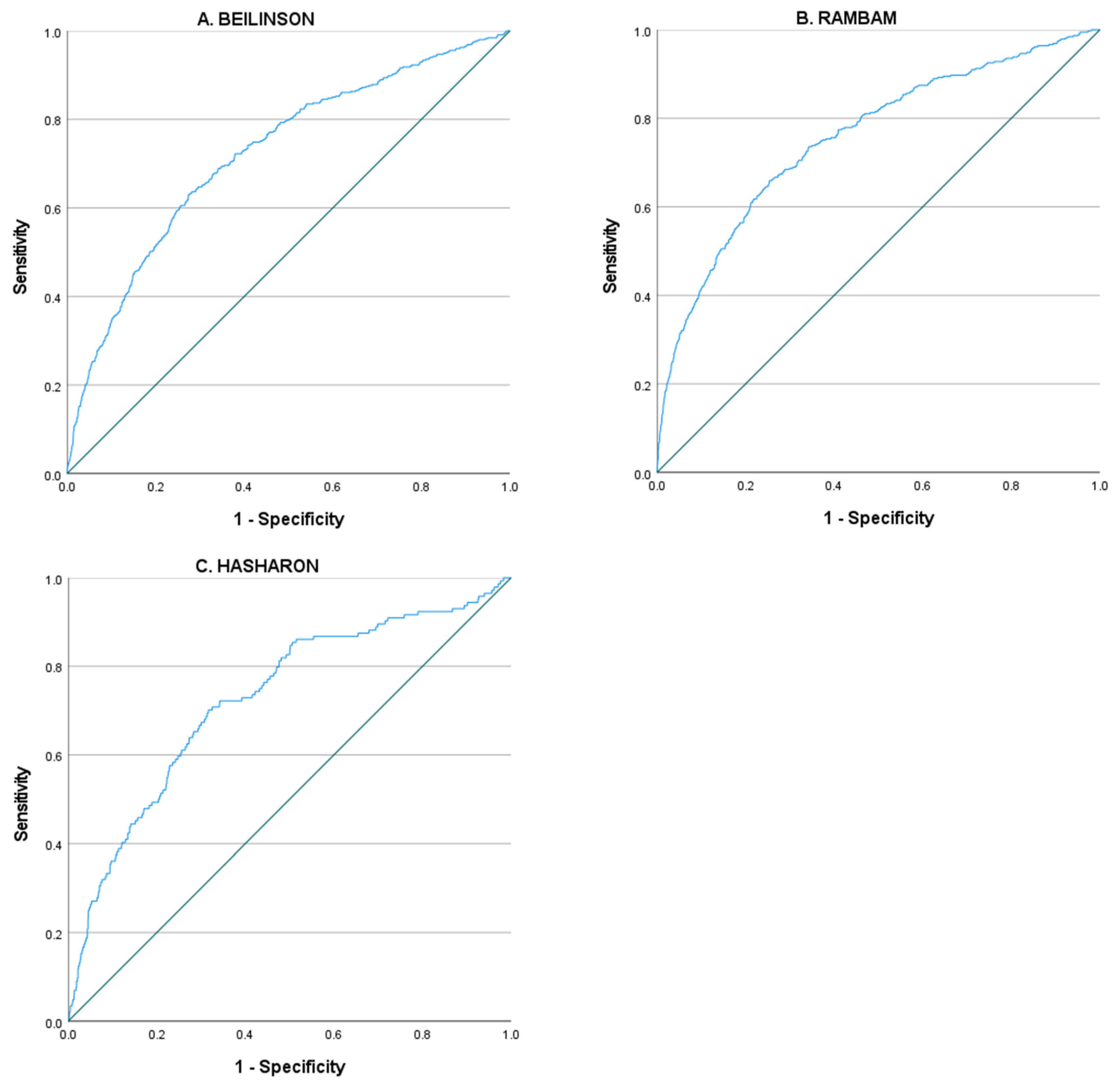
3.1. Derivation Cohort—Beilinson Hospital
3.2. Validation Cohort—Hasharon Hospital
3.3. Validation Cohort—Rambam Health Care Campus
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baggs, J.; Fridkin, S.K.; Pollack, L.A.; Srinivasan, A.; Jernigan, J.A. Estimating national trends in inpatient antibiotic use among US hospitals from 2006 to 2012. JAMA Intern. Med. 2016, 176, 1639–1648. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Jones, T.M.; Hamad, Y.; Pande, A.; Varon, J.; O’Brien, C.; Anderson, D.J.; Warren, D.K.; Dantes, R.B.; Epstein, L.; et al. Centers for Disease Control and Prevention (CDC) Prevention Epicenters Program Prevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care Hospitals. JAMA Netw. Open 2019, 2, e187571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, C.; Dantes, R.; Epstein, L.; Murphy, D.J.; Seymour, C.W.; Iwashyna, T.J.; Kadri, S.S.; Angus, D.C.; Danner, R.L.; Fiore, A.E.; et al. CDC Prevention Epicenter Program Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009–2014. JAMA 2017, 318, 1241–1249. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef] [PubMed]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.A.; Laxminarayan, R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- Klein, E.Y.; Milkowska-Shibata, M.; Tseng, K.K.; Sharland, M.; Gandra, S.; Pulcini, C.; Laxminarayan, R. Assessment of WHO antibiotic consumption and access targets in 76 countries, 2000–2015: An analysis of pharmaceutical sales data. Lancet Infect. Dis. 2021, 21, 107–115. [Google Scholar] [CrossRef]
- Magill, S.S.; Edwards, J.R.; Beldavs, Z.G.; Dumyati, G.; Janelle, S.J.; Kainer, M.A.; Lynfield, R.; Nadle, J.; Neuhauser, M.M.; Ray, S.M.; et al. Emerging Infections Program Healthcare-Associated Infections and Antimicrobial Use Prevalence Survey Team Prevalence of antimicrobial use in US acute care hospitals, May-September 2011. JAMA 2014, 312, 1438–1446. [Google Scholar] [CrossRef] [Green Version]
- Tamma, P.D.; Avdic, E.; Li, D.X.; Dzintars, K.; Cosgrove, S.E. Association of adverse events with antibiotic use in hospitalized patients. JAMA Intern. Med. 2017, 177, 1308–1315. [Google Scholar] [CrossRef] [Green Version]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, 987–994. [Google Scholar] [CrossRef]
- Hensgens, M.P.M.; Goorhuis, A.; Dekkers, O.M.; Kuijper, E.J. Time interval of increased risk for Clostridium difficile infection after exposure to antibiotics. J. Antimicrob. Chemother. 2012, 67, 742–748. [Google Scholar] [CrossRef]
- WHO Global Action Plan on Antimicrobial Resistance. Available online: http://www.wpro.who.int/entity/drug_resistance/resources/global_action_plan_eng.pdf (accessed on 8 June 2021).
- Zanichelli, V.; Monnier, A.A.; Gyssens, I.C.; Adriaenssens, N.; Versporten, A.; Pulcini, C.; Le Maréchal, M.; Tebano, G.; Vlahovic-Palcevski, V.; Stanic Benic, M.; et al. Variation in antibiotic use among and within different settings: A systematic review. J. Antimicrob. Chemother. 2018, 73, vi17–vi29. [Google Scholar] [CrossRef] [Green Version]
- Kallen, M.C.; Natsch, S.; Opmeer, B.C.; Hulscher, M.E.J.L.; Schouten, J.A.; Prins, J.M.; van der Linden, P. How to measure quantitative antibiotic use in order to support antimicrobial stewardship in acute care hospitals: A retrospective observational study. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 347–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, C.; Vermeulen, M.; Wang, X.; Zvonar, R.; Garber, G.; Daneman, N. Variability in antibiotic use across Ontario acute care hospitals. J. Antimicrob. Chemother. 2017, 72, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.C.; Jacob, J.T.; Varkey, J.B.; Gaynes, R.P. Antibiotic use in US hospitals: Quantification, quality measures and stewardship. Expert Rev. Anti. Infect. Ther. 2015, 13, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. the index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Dent, E.; Martin, F.C.; Bergman, H.; Woo, J.; Romero-Ortuno, R.; Walston, J.D. Management of frailty: Opportunities, challenges, and future directions. Lancet 2019, 394, 1376–1386. [Google Scholar] [CrossRef]
- Van Werkhoven, C.H.; van der Tempel, J.; Jajou, R.; Thijsen, S.F.T.; Diepersloot, R.J.A.; Bonten, M.J.M.; Postma, D.F.; Oosterheert, J.J. Identification of patients at high risk for Clostridium difficile infection: Development and validation of a risk prediction model in hospitalized patients treated with antibiotics. Clin. Microbiol. Infect. 2015, 21, 786.e1–786.e8. [Google Scholar] [CrossRef] [Green Version]
- Czepiel, J.; Dróżdż, M.; Pituch, H.; Kuijper, E.J.; Perucki, W.; Mielimonka, A.; Goldman, S.; Wultańska, D.; Garlicki, A.; Biesiada, G. Clostridium difficile infection: Review. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1211–1221. [Google Scholar] [CrossRef] [Green Version]
- Datta, P.; Chander, J.; Gupta, V.; Mohi, G.K.; Attri, A.K. Evaluation of various risk factors associated with multidrug-resistant organisms isolated from diabetic foot ulcer patients. J. Lab. Physicians 2019, 11, 58–62. [Google Scholar] [CrossRef]
- Li, J.; Li, Y.; Song, N.; Chen, Y. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection: A meta-analysis. J. Glob. Antimicrob. Resist. 2020, 21, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Dryden, M.; Baguneid, M.; Eckmann, C.; Corman, S.; Stephens, J.; Solem, C.; Li, J.; Charbonneau, C.; Baillon-Plot, N.; Haider, S. Pathophysiology and burden of infection in patients with diabetes mellitus and peripheral vascular disease: Focus on skin and soft-tissue infections. Clin. Microbiol. Infect. 2015, 21 (Suppl 2), S27–S32. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | Antibiotic Treatment (NO) N = 5138 | Antibiotic Treatment (YES) N = 454 | p-Value |
|---|---|---|---|
| Gender, female | 2461 (47.9%) | 199 (43.8%) | 0.096 |
| Age, years | 71 (60–80) | 73 (64–82) | <0.001 |
| Hospitalization, days | 3 (2–6) | 12 (8–20) | <0.001 |
| Amount of chronic medication | 6 (3–9) | 7 (4–9) | 0.001 |
| Prophylactic antibiotic treatment | 181 (3.5%) | 35 (7.7%) | <0.001 |
| Body temp (°C) | 36.7 (36.5–36.9) | 36.8 (36.6–37.1) | <0.001 |
| Heart rate | 80 (69–94) | 85 (74–96) | <0.001 |
| Systolic blood pressure (mmHg) | 136 (120–152) | 133 (113–153) | 0.003 |
| Diastolic blood pressure (mmHg) | 73 (62–83) | 70 (59–81) | <0.001 |
| O2 saturation (%) | 98 (97–100) | 98 (96–100) | <0.001 |
| White blood cell count (cells/µL) | 8.15 (6.44–10.38) | 8.87 (6.61–11.98) | <0.001 |
| Hemoglobin (mg/dL) | 12.6 (10.9–14.0) | 11.9 (10.0–13.3) | <0.001 |
| Platelet count (cells/µL) | 236 (186–301) | 244 (181–309) | 0.669 |
| Albumin (mg/dL) | 4.2 (3.8–4.5) | 3.8 (3.4–4.2) | <0.001 |
| Neutrophils (cells/µL) | 5.6 (4.2–7.6) | 6.5 (4.3–9.3) | <0.001 |
| Creatinine (mg/dL) | 0.95 (0.76–1.32) | 1.04 (0.76–1.57) | 0.012 |
| Urea (mg/dL) | 40 (29–59) | 47 (33–78) | <0.001 |
| Full functional capacity | 3063 (59.6%) | 163 (35.9%) | <0.001 |
| Full mental status | 4660 (90.7%) | 339 (74.7%) | <0.001 |
| Steroidal treatment at admission | 474 (9.2%) | 58 (12.8%) | 0.013 |
| Solid-organ transplantation | 156 (3.0%) | 22 (4.8%) | 0.035 |
| Diabetes mellitus | 1521 (29.6%) | 148 (32.6%) | 0.181 |
| Insulin treatment | 668 (13%) | 72 (15.9%) | 0.085 |
| Chemotherapy 6 months before hospitalization | 319 (6.2%) | 45 (9.9%) | 0.002 |
| Hypertension | 2435 (47.4%) | 231 (50.9%) | 0.154 |
| Ischemic heart disease | 1115 (21.7%) | 100 (22.0%) | 0.872 |
| Congestive heart failure | 788 (15.3%) | 77 (17.0%) | 0.359 |
| Chronic obstructive lung disease | 299 (5.8%) | 33 (7.3%) | 0.21 |
| Peripheral vascular disease | 185 (3.6%) | 29 (6.4%) | 0.003 |
| Cerebrovascular disease | 931 (18.1%) | 87 (19.2%) | 0.581 |
| Atrial fibrillation | 787 (15.3%) | 94 (20.7%) | 0.003 |
| Bronchiectasis | 54 (1.1%) | 11 (2.4%) | 0.009 |
| Diverticulosis | 75 (1.5%) | 5 (1.1%) | 0.538 |
| Liver cirrhosis | 94 (1.8%) | 18 (4.0%) | 0.002 |
| End-stage renal disease | 105 (2.0%) | 14 (3.1%) | 0.141 |
| Nasogastric tube | 97 (1.9%) | 46 (10.1%) | <0.001 |
| Surgery 30 days before hospitalization | 109 (2.1%) | 17 (3.7%) | 0.026 |
| Pressure wounds | 305 (5.9%) | 73 (16.1%) | <0.001 |
| Central venous catheter | 78 (1.5%) | 19 (4.2%) | <0.001 |
| Urinary catheter | 476 (9.3%) | 112 (24.7%) | <0.001 |
| Variable | B | Odds–Ratio | 95% CI | p-Value |
|---|---|---|---|---|
| Constant | 1.777 | |||
| Gender, female | −0.293 | 0.746 | 0.608–0.916 | 0.005 |
| Prophylactic antibiotic treatment | 0.627 | 1.872 | 1.248–2.809 | 0.002 |
| Heart rate * | 0.006 | 1.006 | 1.001–1.011 | 0.014 |
| Diastolic blood pressure (mmHg) * | −0.006 | 0.994 | 0.987–1.001 | 0.091 |
| O2 saturation (%) * | −0.026 | 0.974 | 0.946–1.003 | 0.075 |
| Albumin (mg/dL) * | −0.550 | 0.577 | 0.487–0.684 | <0.001 |
| Full functional capacity | 0.379 | 1.460 | 1.148–1.857 | 0.002 |
| Full mental status | 0.629 | 1.876 | 1.416–2.485 | <0.001 |
| Solid–organ transplantation | 0.601 | 1.823 | 1.114–2.983 | 0.017 |
| Peripheral vascular disease | 0.538 | 1.713 | 1.124–2.613 | 0.012 |
| Atrial fibrillation | 0.233 | 1.262 | 0.981–1.623 | 0.071 |
| Nasogastric tube | 0.810 | 2.249 | 1.464–3.454 | 0.000 |
| Central venous catheter | 0.771 | 2.161 | 1.251–3.734 | 0.006 |
| Urinary catheter | 0.439 | 1.551 | 1.158–2.078 | 0.003 |
| Cohort | p-Value * | No. of Patients Treated with Antibiotics/Total (%) |
|---|---|---|
| Beilinson | ≤0.04 | 50/1540 (3.2%) |
| 0.04–0.06 | 58/1390 (4.2%) | |
| 0.06–0.1 | 108/1355 (8.0%) | |
| ≥0.1 | 238/1307 (18.2%) | |
| Hasharon | ≤0.04 | 19/1115 (1.7%) |
| 0.04–0.06 | 21/830 (2.5%) | |
| 0.06–0.1 | 38/590 (6.4%) | |
| ≥0.1 | 66/526 (12.5%) | |
| Rambam | ≤0.04 | 14/549 (2.6%) |
| 0.04–0.06 | 48/1392 (3.4%) | |
| 0.06–0.1 | 84/1374 (6.1%) | |
| ≥0.1 | 244/1179 (20.7%) |
| Validation Cohort Hasharon (N = 3061) | Validation Cohort Rambam (N = 4494) | |||||
|---|---|---|---|---|---|---|
| Variable | Antibiotic Treatment (NO) N = 2917 | Antibiotic Treatment (YES) N = 144 | p-Value | Antibiotic Treatment (NO) N = 4104 | Antibiotic Treatment (YES) N = 390 | p-Value |
| Hospitalization, days | 3 (2–4) | 8 (5–15) | <0.001 | 4 (3–6) | 10 (6–16) | <0.001 |
| Gender, female | 1457 (49.9%) | 86 (59.7%) | 0.022 | 1859 (45.3%) | 191 (49%) | 0.164 |
| Prophylactic antibiotic treatment | 54 (1.9%) | 4 (2.8%) | 0.426 | 71 (1.7%) | 13 (3.3%) | 0.025 |
| Heart rate | 79 (68–92) | 85 (72–96) | 0.008 | 80 (70–94) | 85 (72–96) | 0.001 |
| Diastolic blood pressure (mmHg) | 73 (63–83) | 69 (58–80) | 0.001 | 77 (69–85) | 75 (66–81) | <0.001 |
| O2 saturation (%) | 98 (97–100) | 97 (95–100) | <0.001 | 97 (95–99) | 96 (93–98) | <0.001 |
| Albumin mg/dL | 4.2 (3.9–4.5) | 3.8 (3.4–4.2) | <0.001 | 3.7 (3.4–4.0) | 3.4 (3.1–3.8) | <0.001 |
| Full functional capacity | 1961 (67.2%) | 53 (36.8%) | <0.001 | 2748 (67%) | 154 (39.5%) | <0.001 |
| Full mental status | 2644 (90.6%) | 105 (72.9%) | <0.001 | 3924 (95.6%) | 319 (81.8%) | <0.001 |
| Solid organ transplantation | 29 (1%) | 2 (1.4%) | 0.644 | 45 (1.1%) | 6 (1.5%) | 0.431 |
| Peripheral vascular disease | 108 (3.7%) | 9 (6.3%) | 0.12 | 141 (3.4%) | 27 (6.9%) | 0.001 |
| Atrial fibrillation | 489 (16.8%) | 28 (19.4%) | 0.4 | 750 (18.3%) | 115 (29.5%) | <0.001 |
| Nasogastric tube | 30 (1%) | 10 (6.9%) | <0.001 | 24 (0.6%) | 14 (3.6%) | <0.001 |
| Central venous catheter | 9 (0.3%) | 4 (2.8%) | <0.001 | 31 (0.8%0 | 34 (8.7%) | <0.001 |
| Urinary catheter | 170 (5.8%) | 25 (17.4%) | <0.001 | 290 (7.1%) | 168 (43.1%) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poran, I.; Elbaz, M.; Turjeman, A.; Huberman Samuel, M.; Eliakim-Raz, N.; Nashashibi, J.; Paul, M.; Leibovici, L. Predicting In-Hospital Antibiotic Use in the Medical Department: Derivation and Validation Study. Antibiotics 2022, 11, 813. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11060813
Poran I, Elbaz M, Turjeman A, Huberman Samuel M, Eliakim-Raz N, Nashashibi J, Paul M, Leibovici L. Predicting In-Hospital Antibiotic Use in the Medical Department: Derivation and Validation Study. Antibiotics. 2022; 11(6):813. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11060813
Chicago/Turabian StylePoran, Itamar, Michal Elbaz, Adi Turjeman, Maayan Huberman Samuel, Noa Eliakim-Raz, Jeries Nashashibi, Mical Paul, and Leonard Leibovici. 2022. "Predicting In-Hospital Antibiotic Use in the Medical Department: Derivation and Validation Study" Antibiotics 11, no. 6: 813. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11060813