
Patterns and Determinants of Antibiotic Use Behaviors among Rural Community Residents in Eastern China

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Study Participants
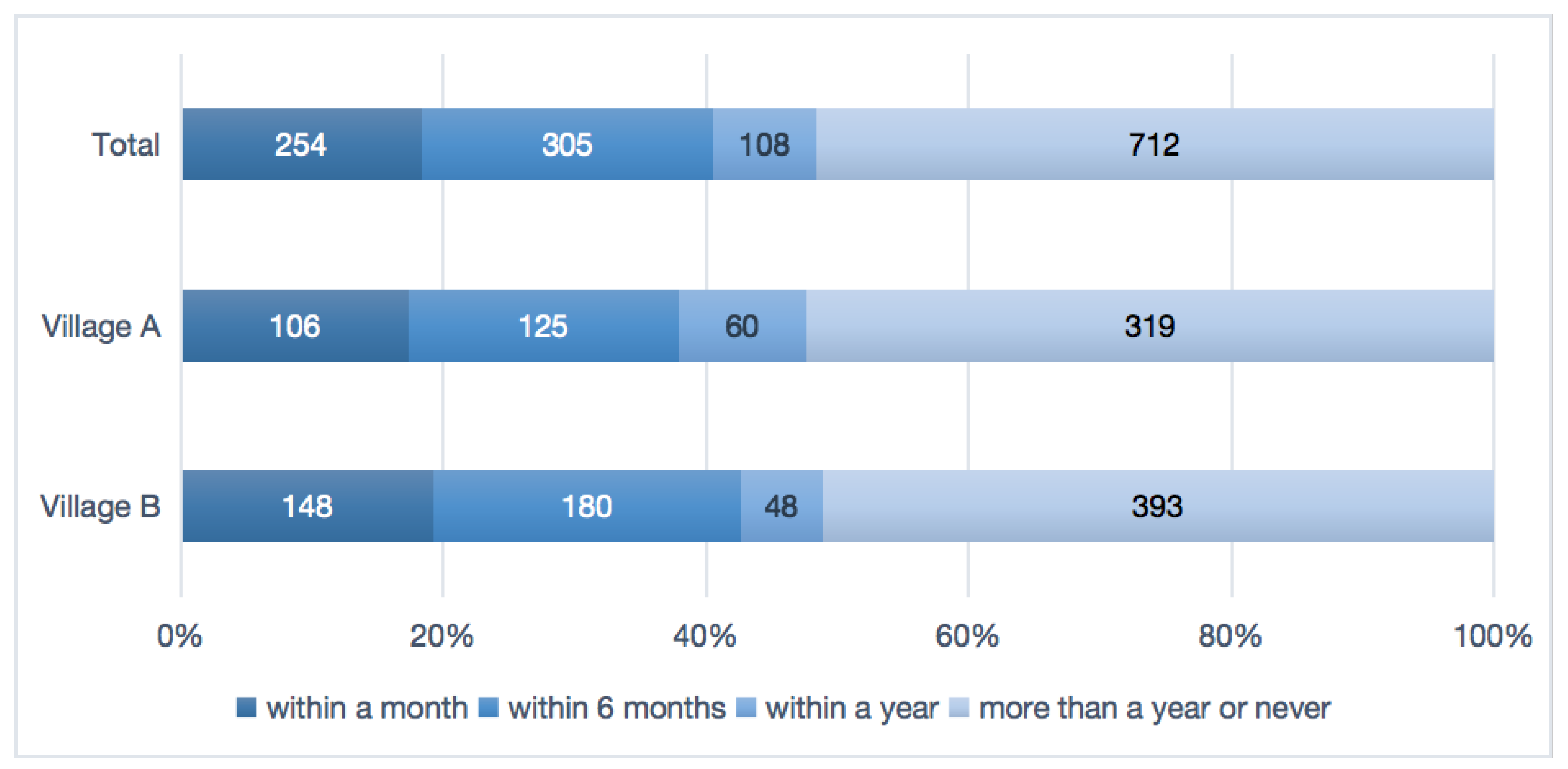
2.2. Distribution and Determinants of Most Recent Antibiotic Use
2.3. Antibiotic Access and Its Determinants
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
4.2. The Questionnaire and Data Collection
4.3. Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, S.; Yuan, S.; Kabba, J.A.; Chen, C.; Liu, W.; Chang, J.; Fang, Y. Analysis of Antibiotic Use Patterns and Trends Based on Procurement Data of Healthcare Institutions in Shaanxi Province, Western China, 2015–2018. Int. J. Environ. Res. Public Health 2020, 17, 7536. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Ying, G.-G.; He, L.-Y.; Ying, A.J.; Zhang, Q.-Q.; Liu, Y.-S.; Zhao, J.-L. China Must Reduce Its Antibiotic Use. Environ. Sci. Technol. 2017, 51, 1072–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofer, U. The cost of antimicrobial resistance. Nat. Rev. Microbiol. 2019, 17, 3. [Google Scholar] [CrossRef]
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. 2014. Available online: https://amr-review.org/ (accessed on 23 April 2022).
- You, J.H.S.; Yau, B.; Choi, K.C.; Chau, C.T.S.; Huang, Q.R.; Lee, S.S. Public knowledge, attitudes and behavior on antibiotic use: A telephone survey in Hong Kong. Infection 2008, 36, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Song, X.; Yang, T.; Chen, Y.; Gong, Y.; Yin, X.; Lu, Z. A Systematic Review of Antibiotic Prescription Associated with Upper Respiratory Tract Infections in China. Medicine 2016, 95, e3587. [Google Scholar] [CrossRef]
- Hu, Y.; Wang, X.; Tucker, J.D.; Little, P.; Moore, M.; Fukuda, K.; Zhou, X. Knowledge, Attitude, and Practice with Respect to Antibiotic Use among Chinese Medical Students: A Multicentre Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 1165. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Antimicrobial Resistance. 2021. Available online: https://www.who.int/health-topics/antimicrobial-resistance (accessed on 14 June 2021).
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan on Antimicrobial Resistance. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/193736/9789241509763_eng.pdf?sequence=1&isAllowed=y (accessed on 23 May 2022).
- World Health Organization. Antimicrobial Resistance: No Action Today, No Cure Tomorrow. 2011. Available online: https://www.who.int/dg/speeches/detail/antimicrobial-resistance-no-action-today-no-cure-tomorrow (accessed on 23 April 2022).
- G20 Summits. Communiqué of the G20 Leaders, Hangzhou, China. 2016. Available online: http://www.g20chn.org/hywj/dncgwj/201609/t20160906_3392.html (accessed on 23 April 2022).
- Li, H.; Yan, S.; Li, D.; Gong, Y.; Lu, Z.; Yin, X. Trends and patterns of outpatient and inpatient antibiotic use in China’s hospitals: Data from the Center for Antibacterial Surveillance, 2012–2016. J. Antimicrob. Chemother. 2019, 74, 1731–1740. [Google Scholar] [CrossRef]
- Xiao, Y.; Li, L. Legislation of clinical antibiotic use in China. Lancet Infect. Dis. 2013, 13, 189–191. [Google Scholar] [CrossRef]
- National Health and Family Planning Commission of the People’s Republic of China. China’s National Action Plan to Contain Antimicrobial Resistance. 2016. Available online: http://www.nhc.gov.cn/yzygj/s3593/201608/f1ed26a0c8774e1c8fc89dd481ec84d7.shtml (accessed on 23 April 2022).
- Krishnasamy, V.; Otte, J.; Silbergeld, E. Antimicrobial use in Chinese swine and broiler poultry production. Antimicrob. Resist. Infect. Control 2015, 4, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Wang, P.; Wang, X.; Zheng, Y.; Xiao, Y. Use and prescription of antibiotics in primary health care settings in China. JAMA Intern. Med. 2014, 174, 1914–1920. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.-Q.; Ying, G.-G.; Pan, C.-G.; Liu, Y.-S.; Zhao, J.-L. Comprehensive evaluation of antibiotics emission and fate in the river basins of China: Source analysis, multimedia modeling, and linkage to bacterial resistance. Environ. Sci. Technol. 2015, 49, 6772–6782. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Zhang, J.; Zheng, B.; Zhao, L.; Li, S.; Li, L. Changes in Chinese policies to promote the rational use of antibiotics. PLoS Med. 2013, 10, e1001556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do, N.T.T.; Vu, H.T.L.; Nguyen, C.T.K.; Punpuing, S.; Khan, W.A.; Gyapong, M.; Asante, K.P.; Munguambe, K.; Gómez-Olivé, F.X.; John-Langba, J.; et al. Community-based antibiotic access and use in six low-income and middle-income countries: A mixed-method approach. Lancet Glob. Health 2021, 9, e610–e619. [Google Scholar] [CrossRef]
- Chowdhury, M.; Williams, J.S.; Wertheim, H.; Khan, W.A.; Matin, A.; Kinsman, J. Rural community perceptions of antibiotic access and understanding of antimicrobial resistance: Qualitative evidence from the Health and Demographic Surveillance System site in Matlab, Bangladesh. Glob. Health Action 2019, 12 (Suppl. 1), 1824383. [Google Scholar] [CrossRef]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey. 2015. Available online: http://apps.who.int/iris/bitstream/10665/194460/1/9789241509817_eng.pdf (accessed on 23 April 2022).
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Eurosurveillance 2020, 25, 2001886. [Google Scholar] [CrossRef]
- Founou, R.C.; Blocker, A.J.; Noubom, M.; Tsayem, C.; Choukem, S.P.; Van Dongen, M.; Founou, L.L. The COVID-19 pandemic: A threat to antimicrobial resistance containment. Future Sci. OA 2021, 7, Fso736. [Google Scholar] [CrossRef]
- Cheng, J.; Coope, C.; Chai, J.; Oliver, I.; Kessel, A.; Wang, D.; Sun, Y. Knowledge and behaviors in relation to antibiotic use among rural residents in Anhui, China. Pharmacoepidemiol. Drug Saf. 2018, 27, 652–659. [Google Scholar] [CrossRef]
- Dong, L.; Yan, H.; Wang, D. Antibiotic prescribing patterns in village health clinics across 10 provinces of Western China. J. Antimicrob. Chemother. 2008, 62, 410–415. [Google Scholar] [CrossRef] [Green Version]
- Deng, P.; Yu, J.; Zhou, N.; Hu, M. Access to medicines for acute illness and antibiotic use in residents: A medicines household survey in Sichuan Province, western China. PLoS ONE 2018, 13, e0201349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Using Indicators to Measure Country Pharmaceutical Situations: Fact Book on WHO Level I and Level II Monitoring Indicators. 2006. Available online: http://apps.who.int/medicinedocs/index/assoc/s14101e/s14101e.pdf (accessed on 23 April 2022).
- Ding, L.; Sun, Q.; Sun, W.; Du, Y.; Li, Y.; Bian, X.; He, G.; Bai, H.; Dyar, O.J. Antibiotic use in rural China: A cross-sectional survey of knowledge, attitudes and self-reported practices among caregivers in Shandong province. BMC Infect. Dis. 2015, 15, 576. [Google Scholar] [CrossRef] [Green Version]
- Bagger, K.; Nielsen, A.B.S.; Siersma, V.; Bjerrum, L. Inappropriate antibiotic prescribing and demand for antibiotics in patients with upper respiratory tract infections is hardly different in female versus male patients as seen in primary care. Eur. J. Gen. Pract. 2015, 21, 118–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.; Ye, D.; Lv, B.; Jiang, M.; Zhu, S.; Yan, K.; Tian, Y.; Fang, Y. Sale of antibiotics without a prescription at community pharmacies in urban China: A multicentre cross-sectional survey. J. Antimicrob. Chemother. 2017, 72, 1235–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, D.J.; Okeke, I.N.; Laxminarayan, R.; Perencevich, E.N.; Weisenberg, S. Non-prescription antimicrobial use worldwide: A systematic review. Lancet Infect. Dis. 2011, 11, 692–701. [Google Scholar] [CrossRef] [Green Version]
- Ferech, M.; Coenen, S.; Malhotra-Kumar, S.; Dvorakova, K.; Hendrickx, E.; Suetens, C.; Goossens, H. European Surveillance of Antimicrobial Consumption (ESAC): Outpatient antibiotic use in Europe. J. Antimicrob. Chemother. 2006, 58, 401–407. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Husin, S.A.; Ali, Z.B.; Sim, B.; Ponnampalavanar, S.S.L.S. Factors influencing inappropriate use of antibiotics: Findings from a nationwide survey of the general public in Malaysia. PLoS ONE 2021, 16, e0258698. [Google Scholar] [CrossRef]
- Pan, H.; Cui, B.; Zhang, D.; Farrar, J.; Law, F.; Ba-Thein, W. Prior knowledge, older age, and higher allowance are risk factors for self-medication with antibiotics among university students in southern China. PLoS ONE 2012, 7, e41314. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Rao, K.; Ren, X. Use of and factors associated with self-treatment in China. BMC Public Health 2012, 12, 995. [Google Scholar] [CrossRef] [Green Version]
- Watkins, W.C.; Ford, J.A. Prescription drug misuse among Asian-American adults: Results from a national survey. Subst. Use Misuse 2011, 46, 1700–1708. [Google Scholar] [CrossRef]
- Chang, J.; Xu, S.; Zhu, S.; Li, Z.; Yu, J.; Zhang, Y.; Zu, J.; Fang, Y.; Ross-Degnan, D. Assessment of non-prescription antibiotic dispensing at community pharmacies in China with simulated clients: A mixed cross-sectional and longitudinal study. Lancet Infect. Dis. 2019, 19, 1345–1354. [Google Scholar] [CrossRef]
- Vialle-Valentin, C.E.; LeCates, R.F.; Zhang, F.; Desta, A.T.; Ross-Degnan, D. Predictors of antibiotic use in African communities: Evidence from medicines household surveys in five countries. Trop. Med. Int. Health 2012, 17, 211–222. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Manual for the Household Survey to Measure Access and Use of Medicines. 2015. Available online: https://www.scirp.org/reference/ReferencesPapers.aspx?ReferenceID=1608696 (accessed on 23 April 2022).
- Shahpawee, N.S.; Chaw, L.L.; Muharram, S.H.; Goh, H.P.; Hussain, Z.; Ming, L.C. University Students’ Antibiotic Use and Knowledge of Antimicrobial Resistance: What Are the Common Myths? Antibiotics 2020, 9, 349. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | n (%) | χ2 | p-Value | ||
|---|---|---|---|---|---|
| Total | Village A | Village B | |||
| Total | 1379 | 610 (44.2) | 769 (55.8) | ||
| Sex | 5.456 | 0.023 | |||
| Female | 774 (56.1) | 321 (52.6) | 453 (58.9) | ||
| Male | 605 (43.9) | 289 (47.4) | 316 (41.1) | ||
| Age (years) | 14.679 | 0.001 | |||
| 15–44 | 97 (7.0) | 49 (8.0) | 48 (6.2) | ||
| 45–64 | 658 (47.7) | 320 (52.5) | 338 (44.0) | ||
| >65 | 624 (45.3) | 241 (39.5) | 383 (49.8) | ||
| Married | 1.111 | 0.292 | |||
| Yes | 1198 (86.9) | 537 (88.0) | 661 (86.0) | ||
| No | 181 (13.1) | 73 (12.0) | 108 (14.0) | ||
| Education years | 31.631 | <0.001 | |||
| 0–9 | 829 (60.1) | 418 (68.5) | 411 (53.4) | ||
| >9 | 550 (39.9) | 192 (31.5) | 358 (46.6) | ||
| Occupation | 143.158 | <0.001 | |||
| Unemployed | 279 (20.2) | 195 (32.0) | 84 (10.9) | ||
| Blue-collar | 951 (69.0) | 319 (52.3) | 632 (82.2) | ||
| White-collar | 149 (10.8) | 96 (15.7) | 53 (6.9) | ||
| Annual household income per capita, RMB | 179.390 | <0.001 | |||
| ≤10,000 | 312 (22.6) | 67 (11.0) | 245 (31.9) | ||
| 10,001–30,000 | 210 (15.2) | 56 (9.2) | 154 (20.0) | ||
| 30,001–50,000 | 232 (16.8) | 95 (15.6) | 137 (17.8) | ||
| >50,000 | 625 (45.3) | 392 (64.3) | 233 (30.3) | ||
| Chronic disease history | 3.007 | 0.074 | |||
| Yes | 756 (54.8) | 318 (52.1) | 438 (57.0) | ||
| No | 623 (45.2) | 292 (47.9) | 331 (43.0) | ||
| Antibiotic knowledge level | 16.547 | <0.001 | |||
| Low | 263 (28.6) | 197 (32.3) | 66 (21.2) | ||
| Medium | 299 (32.5) | 200 (32.8) | 99 (31.8) | ||
| High | 359 (39.0) | 213 (34.9) | 146 (46.9) | ||
| Variables | Antibiotic Use [n (%)] | χ2 | p-Value | |
|---|---|---|---|---|
| Yes | No | |||
| Total | 667 (48.4) | 712 (51.6) | ||
| Sex | 0.443 | 0.506 | ||
| Female | 381 (49.2) | 393 (50.8) | ||
| Male | 286 (47.3) | 319 (52.7) | ||
| Age (years) | 8.612 | 0.013 | ||
| 15–44 | 38 (39.2) | 59 (60.8) | ||
| 45–64 | 343 (52.1) | 315 (47.9) | ||
| ≧65 | 286 (45.8) | 338 (54.2) | ||
| Married | 5.766 | 0.016 | ||
| Yes | 595 (49.7) | 603 (50.3) | ||
| No | 72 (39.8) | 109 (60.2) | ||
| Education years | 0.146 | 0.702 | ||
| 0–9 | 397 (47.9) | 432 (52.1) | ||
| >9 | 270 (49.1) | 280 (50.9) | ||
| Occupation | 0.155 | 0.926 | ||
| Unemployed | 133 (47.7) | 146 (52.3) | ||
| Blue-collar | 460 (48.4) | 491 (51.6) | ||
| White-collar | 74 (49.7) | 75 (50.3) | ||
| Annual household income per capita, RMB | 3.377 | 0.337 | ||
| ≤10,000 | 139 (44.6) | 173 (55.4) | ||
| 10,001–30,000 | 105 (50.0) | 105 (50.0) | ||
| 30,001–50,000 | 121 (52.2) | 111 (47.8) | ||
| >50,000 | 302 (48.3) | 323 (51.7) | ||
| Chronic disease history | 2.244 | 0.134 | ||
| Yes | 380 (50.3) | 376 (49.7) | ||
| No | 287 (46.1) | 336 (53.9) | ||
| Antibiotic knowledge level | 1.913 | 0.384 | ||
| Low | 122 (46.4) | 141 (53.6) | ||
| Medium | 155 (51.8) | 144 (48.2) | ||
| High | 183 (51.0) | 176 (49.0) | ||
| Area | 0.148 | 0.700 | ||
| Village A | 291 (47.7) | 319 (52.3) | ||
| Village B | 376 (48.9) | 393 (51.1) | ||
| Variables | Antibiotic Access [n (%)] | χ2 | p-Value | ||
|---|---|---|---|---|---|
| Medical Facilities (with Prescription) | Medical Stores or Pharmacies | Others | |||
| Total | 826 (59.9) | 244 (17.7) | 309 (22.4) | ||
| Sex | 2.021 | 0.364 | |||
| Female | 453 (58.5) | 137 (17.7) | 184 (23.8) | ||
| Male | 373 (61.7) | 107 (17.7) | 125 (20.7) | ||
| Age (years) | 4.493 | 0.343 | |||
| 15–44 | 57 (58.8) | 23 (23.7) | 17 (17.5) | ||
| 45–64 | 403 (61.2) | 113 (17.2) | 142 (21.6) | ||
| ≧65 | 366 (58.7) | 108 (17.3) | 150 (24.0) | ||
| Married | 6.788 | 0.034 | |||
| Yes | 726 (60.6) | 217 (18.1) | 255 (21.3) | ||
| No | 100 (55.2) | 27 (14.9) | 54 (29.8) | ||
| Education years | 6.383 | 0.041 | |||
| 0–9 | 503 (60.7) | 130 (15.7) | 196 (23.6) | ||
| >9 | 323 (58.7) | 114 (20.7) | 113 (20.6) | ||
| Occupation | 18.953 | 0.001 | |||
| Unemployed | 181 (64.9) | 34 (12.2) | 64 (22.9) | ||
| Blue-collar | 539 (56.7) | 188 (19.8) | 224 (23.5) | ||
| White-collar | 106 (71.1) | 22 (14.8) | 21 (14.1) | ||
| Annual household income per capita, RMB | 12.966 | 0.044 | |||
| ≤10,000 | 164 (52.6) | 72 (23.1) | 76 (24.3) | ||
| 10,001–30,000 | 129 (61.4) | 35 (16.7) | 46 (21.9) | ||
| 30,001–50,000 | 136 (58.6) | 43 (18.5) | 53 (22.9) | ||
| >50,000 | 397 (63.5) | 94 (15.1) | 134 (21.4) | ||
| Chronic disease history | 9.574 | 0.008 | |||
| Yes | 483 (56.7) | 162 (19.0) | 207 (24.3) | ||
| No | 343 (65.1) | 82 (15.6) | 102 (19.3) | ||
| Antibiotic knowledge level | 13.699 | 0.008 | |||
| Low | 146 (55.5) | 43 (16.3) | 74 (28.2) | ||
| Medium | 198 (66.2) | 33 (11.0) | 68 (22.8) | ||
| High | 248 (69.1) | 43 (12.0) | 68 (18.9) | ||
| Area | 115.560 | <0.001 | |||
| Village A | 431 (70.7) | 33 (5.4) | 146 (23.9) | ||
| Village B | 395 (51.4) | 211 (27.4) | 163 (21.2) | ||
| Variables | Pharmacies | Others | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Sex (Ref: Female) | ||||
| Male | 0.95 (0.75~1.21) | 0.688 | 0.85 (0.70~1.03) | 0.100 |
| Age (Ref: ≧65 years) | ||||
| 15–44 | 2.21 (1.28~3.81) | 0.004 | 0.70 (0.43~1.14) | 0.151 |
| 45–64 | 1.17 (0.87~1.59) | 0.298 | 0.91 (0.72~1.17) | 0.472 |
| Married (Ref: Yes) | ||||
| Other | 0.70 (0.48~1.02) | 0.065 | 1.42 (1.06~1.89) | 0.018 |
| Occupation (Ref: White-collar) | ||||
| Unemployed | 0.94 (0.59~1.49) | 0.776 | 1.74 (1.19~2.54) | 0.005 |
| Blue-collar | 1.51 (1.01~2.26) | 0.044 | 1.96 (1.38~2.77) | <0.001 |
| Education (Ref: >9 years) | ||||
| 0–9 | 0.64 (0.49~0.83) | 0.001 | 0.96 (0.77~1.20) | 0.725 |
| Annual household income per capita (Ref: >50,000 RMB) | ||||
| ≤10,000 | 1.91 (1.34~2.73) | 0.001 | 1.10 (0.82~1.48) | 0.533 |
| 10,001–30,000 | 1.10 (0.76~1.61) | 0.615 | 0.92 (0.68~1.25) | 0.587 |
| 30,001–50,000 | 1.25 (0.89~1.76) | 0.201 | 1.05 (0.79~1.38) | 0.753 |
| Antibiotic knowledge level (Ref: High) | ||||
| Low | 2.74 (2.01~3.72) | <0.001 | 1.50 (1.18~1.92) | 0.001 |
| Medium | 1.07 (0.74~1.57) | 0.713 | 1.23 (0.93~1.62) | 0.143 |
| Chronic disease history (Ref: Yes) | ||||
| No | 1.23 (0.97~1.58) | 0.093 | 1.76 (1.44~2.16) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Zhao, X.; Li, Y.; Wang, N.; Jiang, F.; Lambert, H.; Yan, F.; Fu, C.; Jiang, Q. Patterns and Determinants of Antibiotic Use Behaviors among Rural Community Residents in Eastern China. Antibiotics 2022, 11, 823. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11060823
Wang Y, Zhao X, Li Y, Wang N, Jiang F, Lambert H, Yan F, Fu C, Jiang Q. Patterns and Determinants of Antibiotic Use Behaviors among Rural Community Residents in Eastern China. Antibiotics. 2022; 11(6):823. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11060823
Chicago/Turabian StyleWang, Yanhuan, Xinping Zhao, Yurong Li, Na Wang, Feng Jiang, Helen Lambert, Fei Yan, Chaowei Fu, and Qingwu Jiang. 2022. "Patterns and Determinants of Antibiotic Use Behaviors among Rural Community Residents in Eastern China" Antibiotics 11, no. 6: 823. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11060823