Antibiotic Prescribing for Uncomplicated Acute Bronchitis Is Highest in Younger Adults


Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Ethics
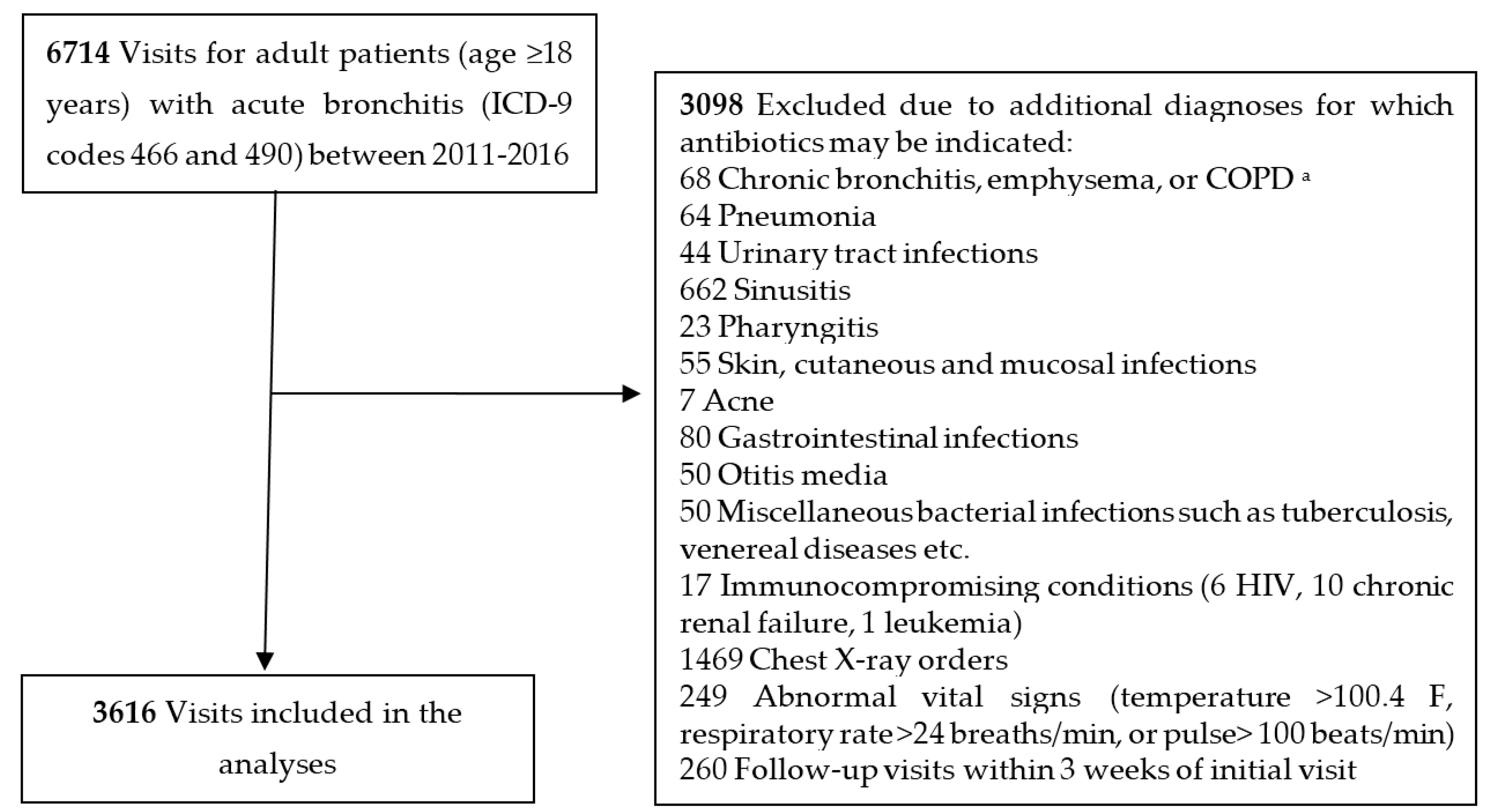
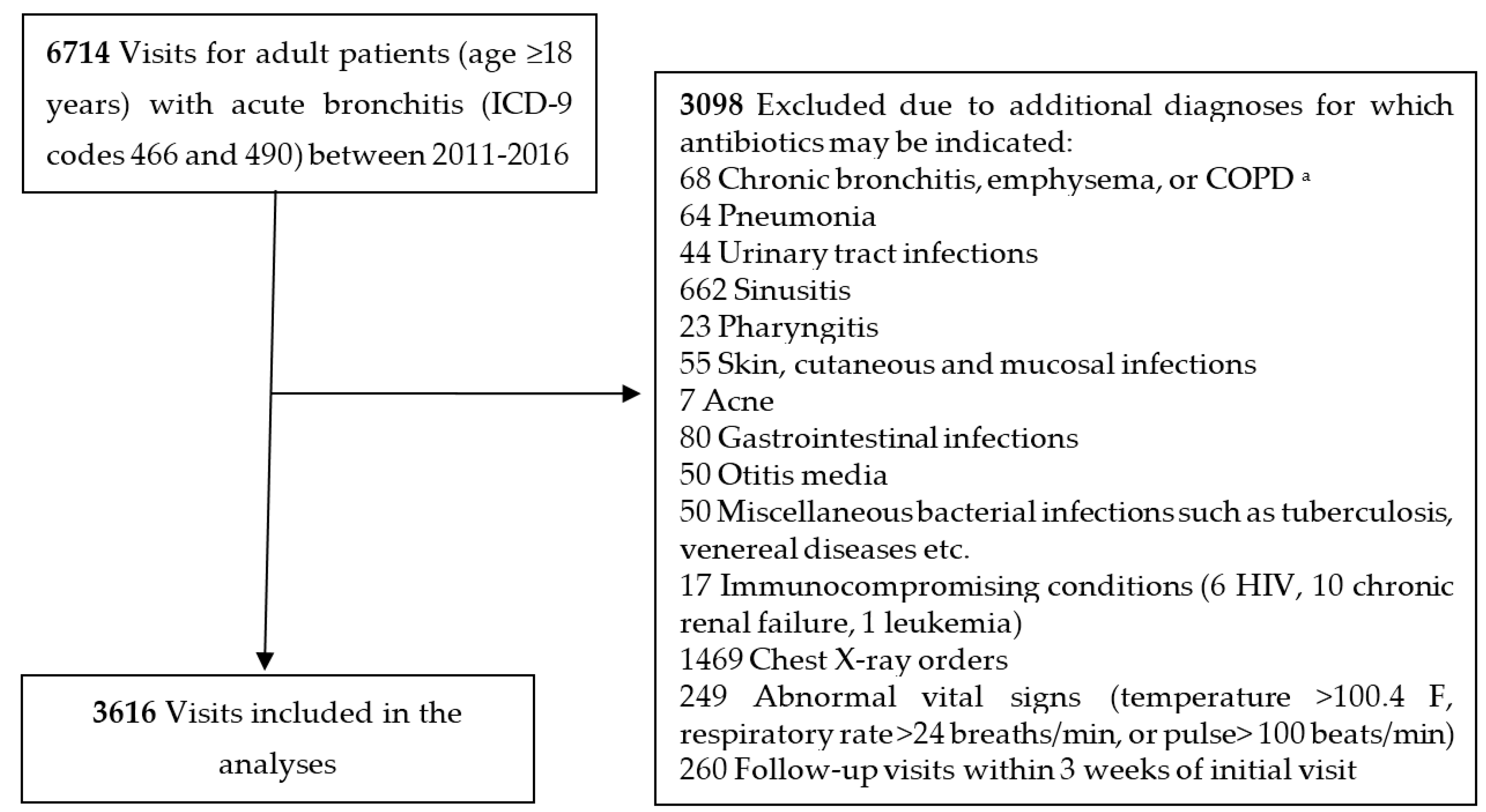
4.2. Setting and Study Population
4.3. Statistical Analysis
Acknowledgments
Author Contributions
Conflicts of Interest
References
- The White House. National Action Plan for Combating Antibiotic-Resistant Bacteria. Available online: https://obamawhitehouse.archives.gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf (accessed on 26 October 2017).
- The Pew Charitable Trusts. Antibiotic Use in Outpatient Settings. Available online: http://www.pewtrusts.org/~/media/assets/2016/05/antibioticuseinoutpatientsettings.pdf (accessed on 26 October 2017).
- The National Committee for Quality Assurance (NCAA). The Healthcare Effectiveness Data and Information Set (HEDIS). Available online: http://www.ncqa.org/report-cards/health-plans/state-of-health-care-quality/2016-table-of-contents/acute-bronchitis (accessed on 26 October 2017).
- Suda, K.J.; Hicks, L.A.; Roberts, R.M.; Hunkler, R.J.; Danziger, L.H. A national evaluation of antibiotic expenditures by healthcare setting in the United States, 2009. J. Antimicrob. Chemother. 2013, 68, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.M.; Hicks, L.A.; Qaseem, A. Appropriate antibiotic use for acute respiratory tract infection in adults. Ann. Intern. Med. 2016, 165, 674. [Google Scholar] [CrossRef] [PubMed]
- Albert, R.H. Diagnosis and treatment of acute bronchitis. Am. Fam. Physician 2010, 82, 1345–1350. [Google Scholar] [PubMed]
- Smith, S.M.; Fahey, T.; Smucny, J.; Becker, L.A. Antibiotics for acute bronchitis. Cochrane Database Syst. Rev. 2014, CD000245. [Google Scholar] [CrossRef]
- Barnett, M.L.; Linder, J.A. Antibiotic prescribing for adults with acute bronchitis in the United States, 1996–2010. JAMA 2014, 311, 2020–2022. [Google Scholar] [CrossRef] [PubMed]
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J.; Bartoces, M.; Enns, E.A.; File, T.M., Jr.; Finkelstein, J.A.; Gerber, J.S.; Hyun, D.Y.; Linder, J.A.; et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016, 315, 1864–1873. [Google Scholar] [CrossRef] [PubMed]
- Arabyat, R.M.; Raisch, D.W.; McKoy, J.M.; Bennett, C.L. Fluoroquinolone-associated tendon-rupture: A summary of reports in the Food and Drug Administration's adverse event reporting system. Expert Opin. Drug Saf. 2015, 14, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.W. Antimicrobials and QT prolongation. J. Antimicrob. Chemother. 2017, 72, 1272–1274. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Baddley, J.W.; Wang, H.E. Antibiotic utilization for acute respiratory tract infections in U.S. emergency departments. Antimicrob. Agents Chemother. 2014, 58, 1451–1457. [Google Scholar] [CrossRef] [PubMed]
- Malo, S.; Bjerrum, L.; Feja, C.; Lallana, M.J.; Moliner, J.; Rabanaque, M.J. Compliance with recommendations on outpatient antibiotic prescribing for respiratory tract infections: The case of Spain. Basic Clin. Pharmacol. Toxicol. 2015, 116, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.; Bradley, C.P.; Byrne, S. Antibiotic prescribing in primary care, adherence to guidelines and unnecessary prescribing—An Irish perspective. BMC Fam. Pract. 2012, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, R.; Anderer, T.; McCulloch, C.E.; Maselli, J.H.; Bloom, F.J., Jr.; Graf, T.R.; Stahl, M.; Yefko, M.; Molecavage, J.; Metlay, J.P. A cluster randomized trial of decision support strategies for reducing antibiotic use in acute bronchitis. JAMA Intern. Med. 2013, 173, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Drekonja, D.M.; Filice, G.A.; Greer, N.; Olson, A.; MacDonald, R.; Rutks, I.; Wilt, T.J. Antimicrobial stewardship in outpatient settings: A systematic review. Infect. Control Hosp. Epidemiol. 2015, 36, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Meeker, D.; Knight, T.K.; Friedberg, M.W.; Linder, J.A.; Goldstein, N.J.; Fox, C.R.; Rothfeld, A.; Diaz, G.; Doctor, J.N. Nudging guideline-concordant antibiotic prescribing: A randomized clinical trial. JAMA Intern. Med. 2014, 174, 425–431. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Visit Characteristics Number of Visits (%), n = 3616 | Number of Visits with Antibiotics Prescribed (% of All Visits; (95% CIs)), n = 2244 | p Value d | |
|---|---|---|---|
| Age | <0.001 | ||
| 18–39 years, n (%) | 1451 (40.1) | 971 (66.9; (64.5–69.3)) | |
| 40–64 years, n (%) | 1662 (46.0) | 976 (58.7; (56.3–61.1)) | |
| ≥65 years, n (%) | 503 (13.9) | 297 (59.0; (54.6–63.4)) | |
| Female | 2313 (64.0) | 1443 (62.4; (60.4–64.4)) | 0.59 |
| Race a | 0.64 | ||
| White | 2288 (74.1) | 1408 (61.5; (59.5–63.5)) | |
| Black | 515 (16.7) | 328 (63.7; (59.4–67.9)) | |
| Other b | 286 (9.2) | 508 (62.5; (59.1–65.8)) | |
| Year of visit c | 0.07 e | ||
| 2011 | 673 (18.6) | 484 (71.9; (68.4–75.3)) | |
| 2012 | 749 (20.7) | 506 (67.6; (64.1–70.9)) | |
| 2013 | 687 (19.0) | 348 (50.7; (46.8–54.5)) | |
| 2014 | 559 (15.5) | 320 (57.2; (53.0–61.4)) | |
| 2015 | 564 (15.6) | 311 (55.1; (50.9–59.3)) | |
| 2016 c | 384 (10.6) | 275 (71.6; (66.8–76.1)) | |
| Visit Characteristics | |||||
|---|---|---|---|---|---|
| Total (All Ages) n = 3616 | 18–39 Years n = 1451 | 40–64 Years n = 1662 | ≥65 Years n = 503 | p Value a | |
| No. visits with antibiotics prescribed (%) | 2244 (62.1) | 971 (66.9) | 976 (58.7) | 297 (59.0) | |
| Macrolides | 1953 (87.0) | 864 (89.0) | 841 (86.2) | 248 (83.5) | 0.03 |
| Fluoroquinolones | 74 (3.3) | 14 (1.4) | 44 (4.5) | 16 (5.4) | <0.001 |
| Other antibiotics | 217 (9.7) | 93 (9.6) | 91 (9.3) | 33 (11.1) | 0.65 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grigoryan, L.; Zoorob, R.; Shah, J.; Wang, H.; Arya, M.; Trautner, B.W. Antibiotic Prescribing for Uncomplicated Acute Bronchitis Is Highest in Younger Adults. Antibiotics 2017, 6, 22. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics6040022
Grigoryan L, Zoorob R, Shah J, Wang H, Arya M, Trautner BW. Antibiotic Prescribing for Uncomplicated Acute Bronchitis Is Highest in Younger Adults. Antibiotics. 2017; 6(4):22. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics6040022
Chicago/Turabian StyleGrigoryan, Larissa, Roger Zoorob, Jesal Shah, Haijun Wang, Monisha Arya, and Barbara W. Trautner. 2017. "Antibiotic Prescribing for Uncomplicated Acute Bronchitis Is Highest in Younger Adults" Antibiotics 6, no. 4: 22. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics6040022