The Clinical and Economic Impact of Antibiotic Resistance in China: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Study Quality Assessment
2.5. Data Analysis
3. Results
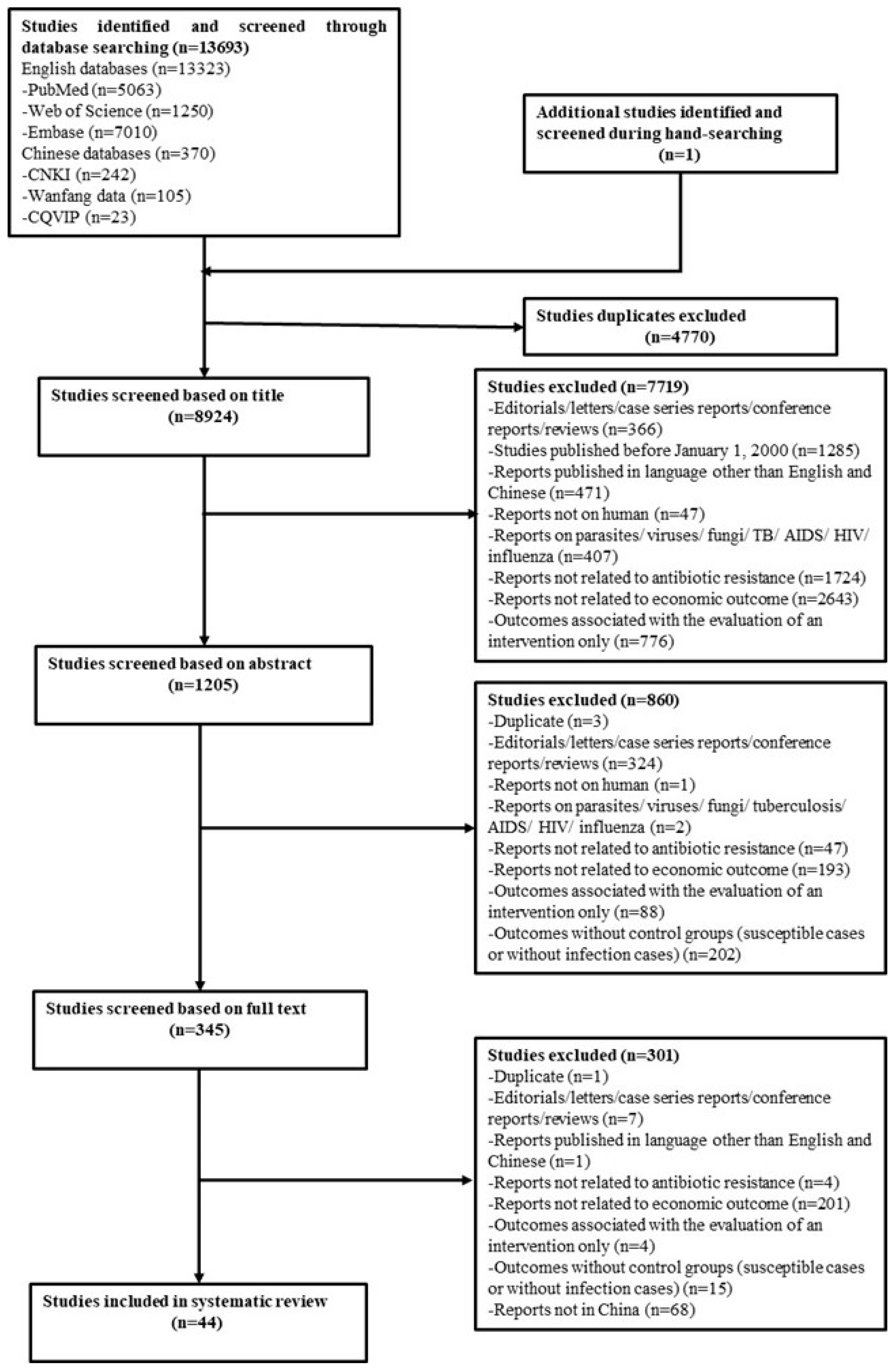
3.1. Study Identification
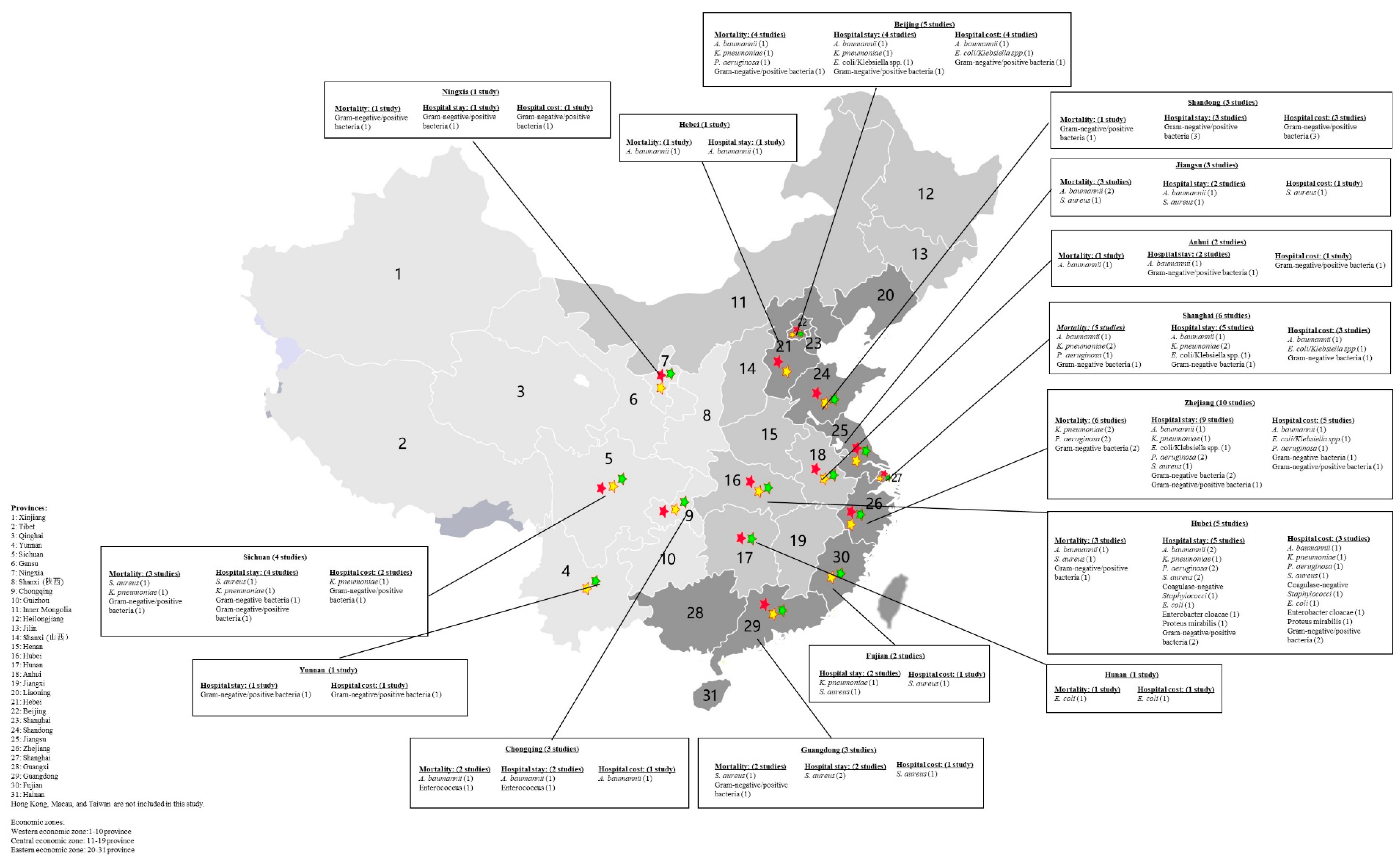
3.2. Study Characteristics and Quality
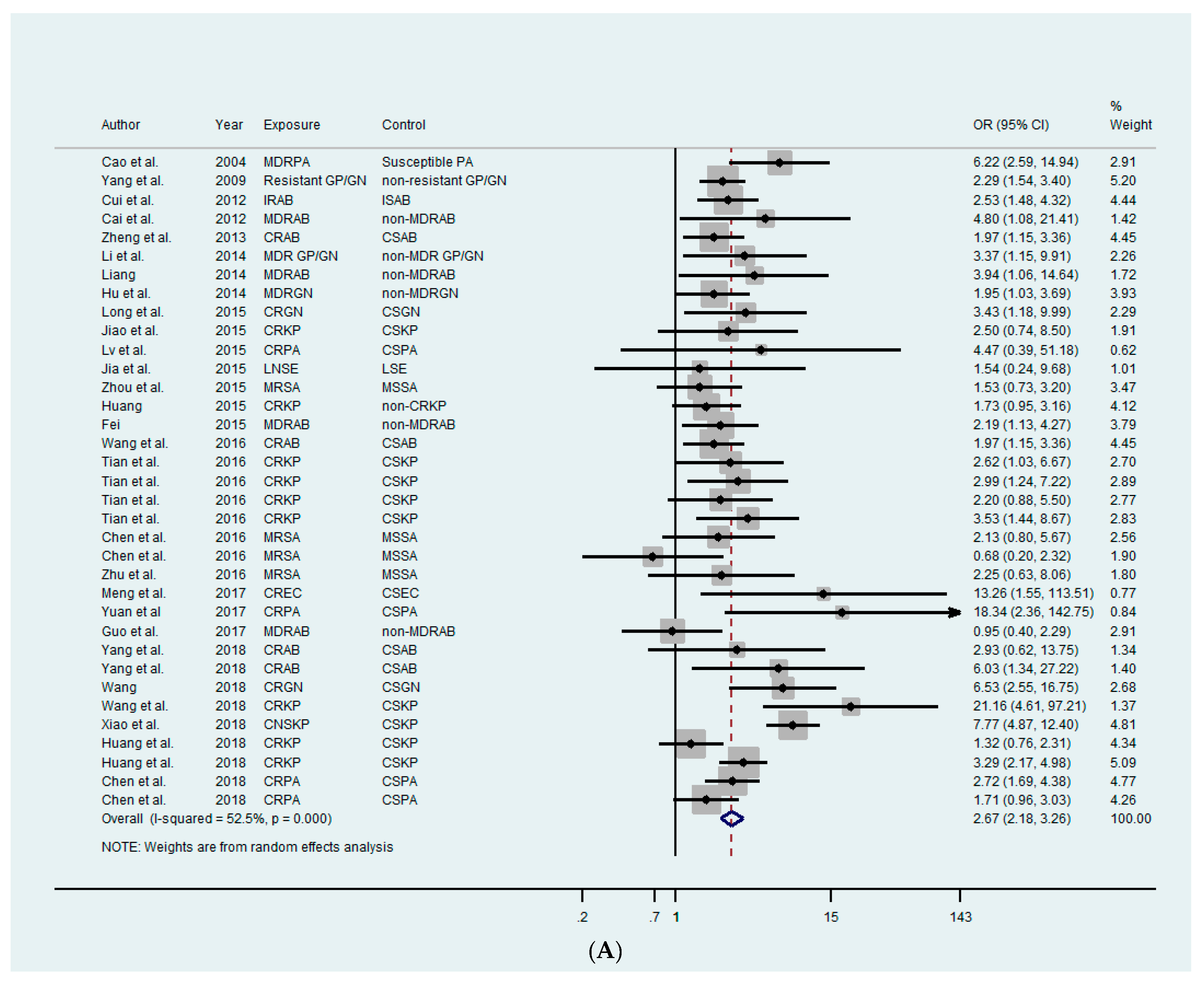
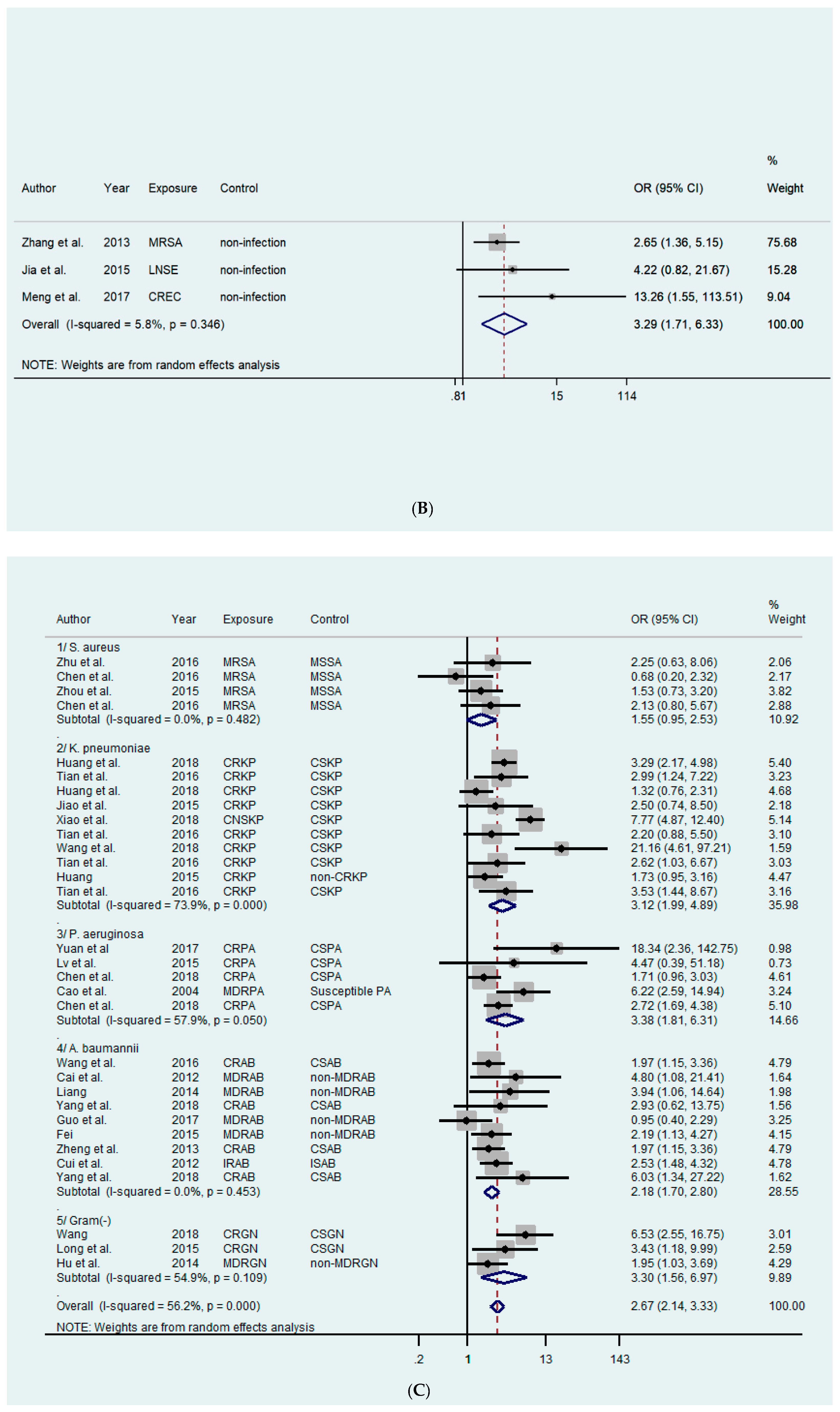
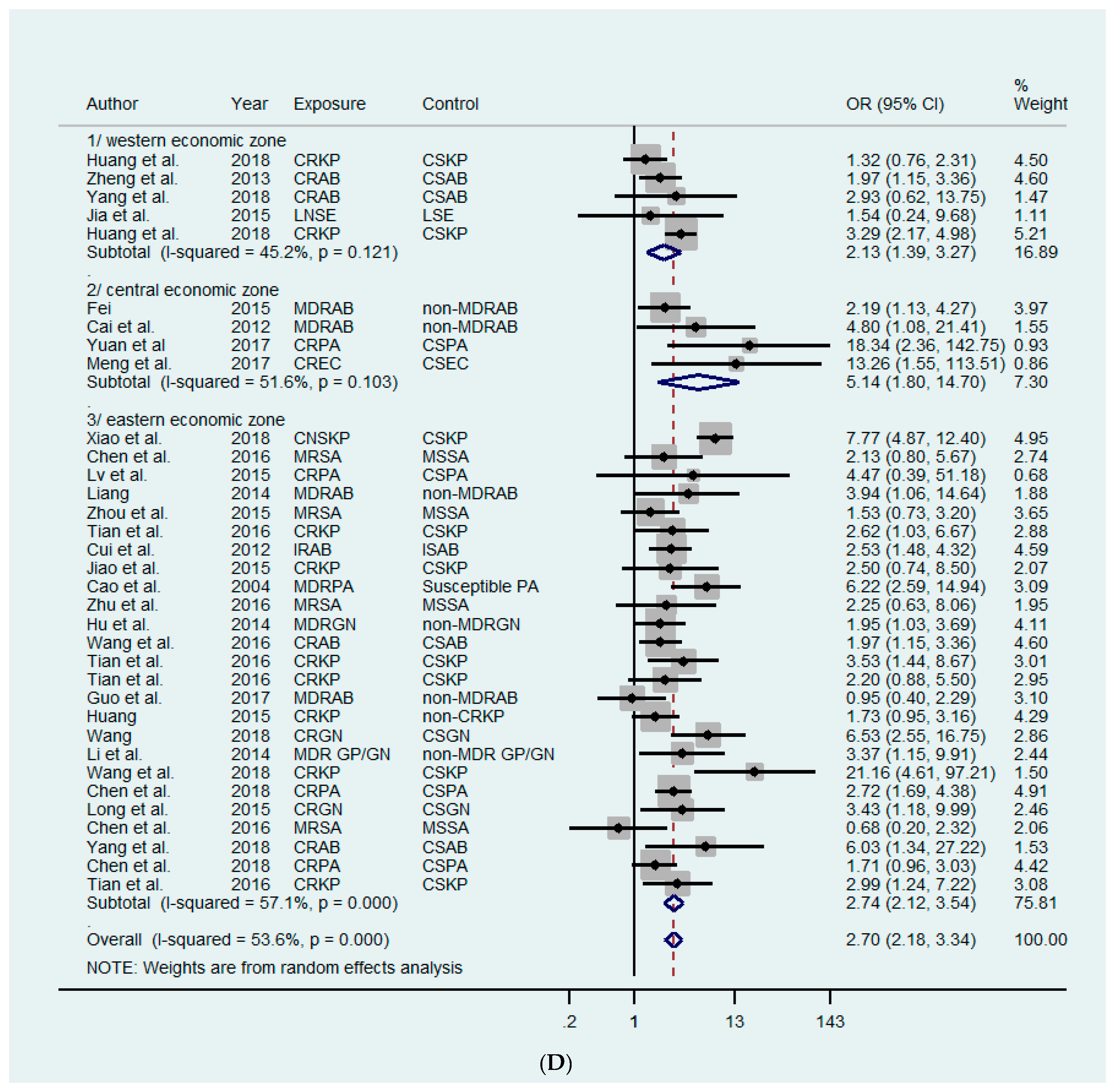
3.3. Mortality Outcome
3.4. Hospital Stay Outcome
3.5. Hospital Cost Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Yezli, S.; Li, H. Antibiotic resistance amongst healthcare-associated pathogens in China. Int. J. Antimicrob. Agents 2012, 40, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R. Antibiotic effectiveness: Balancing conservation against innovation. Science 2014, 345, 1299–1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect. Dis. 2017, 17, 897. [Google Scholar]
- Kan, Q.; Wen, J.; Liu, X.; Li, Z. Inappropriate use of antibiotics in children in China. Lancet 2016, 387, 1273–1274. [Google Scholar] [Green Version]
- Li, Y.; Xu, J.; Wang, F.; Wang, B.; Liu, L.; Hou, W.; Fan, H.; Tong, Y.; Zhang, J.; Lu, Z. Overprescribing in China, driven by financial incentives, results in very high use of antibiotics, injections, and corticosteroids. Health Aff. 2012, 31, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Eggleston, K.; Rotimi, V.; Zeckhauser, R.J. Antibiotic resistance as a global threat: Evidence from China, Kuwait and the United States. Glob. Health 2006, 2, 6. [Google Scholar] [CrossRef]
- Heddini, A.; Cars, O.; Qiang, S.; Tomson, G. Antibiotic resistance in China-a major future challenge. Lancet 2009, 373, 30. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Annual Report of the European Antimicrobial Resistance Surveillance Network. 2017. Available online: https://ecdc.europa.eu/sites/portal/files/documents/EARS-Net-report-2017-update-jan-2019.pdf (accessed on 14 February 2019).
- China Antimicrobial Resistance Surveillance System. Annual Report of the China Antimicrobial Resistance Surveillance System, 2017. 2018. Available online: http://www.carss.cn/Report/Details?aId=552 (accessed on 14 February 2019).
- Hu, F.P.; Guo, Y.; Zhu, D.M.; Wang, F.; Jiang, X.F.; Xu, Y.C.; Zhang, X.J.; Zhang, C.X.; Ji, P.; Xie, Y.; et al. Resistance trends among clinical isolates in China reported from CHINET surveillance of bacterial resistance, 2005–2014. Clin. Microbiol. Infect. 2016, 22 (Suppl. 1), S9–S14. [Google Scholar] [CrossRef]
- National Health and Family Plan Commission. National Action Plan to Combat Antimicrobial Resistance. 2016. Available online: http://www.gov.cn/xinwen/2016–08/25/content_5102348.htm (accessed on 5 March 2019).
- World Health Organization. Global Action Plan on Antimicrobial Resistance. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/193736/9789241509763_eng.pdf?sequence=1 (accessed on 12 February 2019).
- Xiao, Y.; Li, L. China’s national plan to combat antimicrobial resistance. Lancet Infect. Dis. 2016, 16, 1216–1218. [Google Scholar] [CrossRef]
- Xiao, Y.; Zhang, J.; Zheng, B.; Zhao, L.; Li, S.; Li, L. Changes in Chinese policies to promote the rational use of antibiotics. PLoS Med. 2013, 10, e1001556. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Li, L. Legislation of clinical antibiotic use in China. Lancet Infect. Dis. 2013, 13, 189–191. [Google Scholar] [CrossRef]
- Sipahi, O.R. Economics of antibiotic resistance. Expert Rev. Anti-Infect. 2008, 6, 523–539. [Google Scholar] [CrossRef] [PubMed]
- Naylor, N.R.; Atun, R.; Zhu, N.; Kulasabanathan, K.; Silva, S.; Chatterjee, A.; Knight, G.M.; Robotham, J.V. Estimating the burden of antimicrobial resistance: A systematic literature review. Antimicrob. Resist. Infect. Control 2018, 7, 58. [Google Scholar] [CrossRef] [PubMed]
- Giske, C.G.; Monnet, D.L.; Cars, O.; Carmeli, Y. Clinical and economic impact of common multidrug-resistant gram-negative bacilli. Antimicrob. Agents Chemother. 2008, 52, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE 2017, 12, e189621. [Google Scholar] [CrossRef] [PubMed]
- De Kraker, M.E.A.; Davey, P.G.; Grundmann, H. Mortality and hospital stay associated with resistant Staphylococcus aureus and Escherichia coli bacteremia: Estimating the burden of antibiotic resistance in Europe. PLoS Med. 2011, 8, e1001104. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Tacking Drug Resistant Infections Globally: Final Report and Recommendations: The Review on Antimicrobial Resistance. 2016. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 15 February 2019).
- Nathwani, D.; Raman, G.; Sulham, K.; Gavaghan, M.; Menon, V. Clinical and economic consequences of hospital-acquired resistant and multidrug-resistant Pseudomonas aeruginosa infections: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2014, 3, 32. [Google Scholar] [CrossRef] [PubMed]
- Maragakis, L.L.; Perencevich, E.N.; Cosgrove, S.E. Clinical and economic burden of antimicrobial resistance. Expert Rev. Anti-Infect. 2008, 6, 751–763. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Cooperation and Development. Consumer Price Indices. 2019. Available online: https://stats.oecd.org/index.aspx?queryid=221# (accessed on 15 February 2019).
- Organisation for Economic Cooperation and Development. Exchange Rates, End of Period. 2019. Available online: https://stats.oecd.org/index.aspx?queryid=221# (accessed on 15 February 2019).
- Guo, Y.; Guo, W.; Qiu, P.; He, Q.; Pan, C.; Wu, P.; He, J. Study of attributive hospitalized cost and length of stay for hospital acquired infection due to multidrug resistance and non-resistance Acinetobacter baumannii. Chin. J. Health Stat. 2017, 34, 378–381. [Google Scholar]
- Hu, G.; Shen, L.; Jiang, S.; Chen, W.; Wang, Z. Impact of multi-drug gram-negative bacilli bloodstream infection on outcome of patients. Zhejiang Med. J. 2014, 36, 1942–1944. [Google Scholar]
- Huang, J. Risk Factors and Clinical Outcomes of Carbapenem-Resistant Klebsiella Pneumoniae Infections of Critically Ill Patients; Zhejiang University: Hangzhou, China, 2015; p. 44. [Google Scholar]
- Li, H.; Sun, S.; Zhou, H. Analysis of clinical features and outcomes of infections with multi-drug resistant organisms in certain intensive care unit in 2011. Chin. J. Nosocomiol. 2014, 24, 1643–1644. [Google Scholar]
- Liang, L. Mechanical Ventilation in Patients with Multi-Drug Resistant (MDR) Acinetobacter Infection Distribution Characteristics and Drug Resistance Affecting Factors; Hebei United University: Tangshan, Hebei, 2014; p. 48. [Google Scholar]
- Lv, Q.; Ruan, Z.; Wang, J.; Ma, Q.; Dai, Y. Clinical characteristics and prognosis of patients with carbapenem resistant Pseudomonas aeruginosa infection. Chin. J. Nosocomiol. 2015, 25, 5570–5571. [Google Scholar]
- Pei, H. Clinical Characteristics, Risk Factors for Occurrence and Prognosis Analysis for Multidrug-Resistant Acinetobacter Baumannii in a Tertiary Care Hospital from 2010 to 2012; Anhui Medical University: Hefei, China, 2015; p. 51. [Google Scholar]
- Wang, D. Clinical Characteristics and Risk Factors of Carbapenem Resistant Gram-Negative Bacteria Bloodstream Infection; Zhejiang University: Hangzhou, China, 2018; p. 45. [Google Scholar]
- Wang, Y.; Fu, R.; Zheng, Y.; Wan, Y.; Zhou, L. Risk factors and mortality of patients with nosocomial carbapenem-resistant Acinetobacter baumannii pneumonia. J. Clin. Pulm. Med. 2016, 21, 784–788. [Google Scholar]
- Zhang, Z.; Zhang, J.; Xie, F.; Lou, G.; Li, X. Analysis of drug resistance of Staphyloccus aureus isolated from bloodstream and risk factors of methicillin resistant strains. Lab. Med. Clin. 2013, 10, 2380–2382. [Google Scholar]
- Zhou, L.; Qiao, F.; Huang, W.; Zong, Z. Impact of methicillin resistant Staphylococcus aureus bloodstream infection on the prognosis of patients. Chin. J. Infect. Control 2015, 14, 27–30. [Google Scholar]
- Chen, W.; Li, S.; Li, H.; Zhang, S.; Liu, B.; Zhang, X.; Xu, P.; Zhang, W. Comparison in prognosis of hospital-acquired pneumonia due to methicillin resistant and methicillin sensitive Staphylococcus aureus: Analysis of propensity score matching. Chin. J. Infect. Control 2016, 15, 299–303. [Google Scholar]
- Cui, N.; Cao, B.; Liu, Y.; Liang, L.; Gu, L.; Song, S. The impact of imipenem resistant Acinetobacter baumannii infection on clinical outcomes and medical care costs. Chin. J. Infect. Dis. 2012, 30, 209–214. [Google Scholar]
- Long, Z. Clinical and Economic Impact of Carbapenem Resistance in Children’s Nonfermenters Sepsis; Shanghai Jiao Tong University: Shanghai, China, 2015; p. 72. [Google Scholar]
- Zhu, C.; Liu, C.; Wu, B.; Wu, Q.; Huang, D. Analysis of antibiotic resistance in the Staphylococcus aureus strains isolated from bloodstream infections and associated patient outcome. Chin. J. Infect. Chemother. 2016, 16, 1–4. [Google Scholar]
- Yang, S.; Sun, J.; Wu, X.; Zhang, L. Determinants of mortality in patients with nosocomial Acinetobacter baumannii bacteremia in southwest China: A five-year case-control study. Can. J. Infect. Dis. Med. 2018, 2018. [Google Scholar] [CrossRef]
- Chen, Z.; Xu, Z.; Wu, H.; Chen, L.; Gao, S.; Chen, Y. The impact of carbapenem-resistant Pseudomonas aeruginosa on clinical and economic outcomes in a Chinese tertiary care hospital: A propensity score-matched analysis. Am. J. Infect. Control 2019, 47, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Liu, S.; Duan, J.; Huang, X.; Zhou, P.; Xiong, X.; Gong, R.; Zhang, Y.; Liu, Y.; Fu, C.; et al. Risk factors and medical costs for healthcare-associated carbapenem-resistant Escherichia coli infection among hospitalized patients in a Chinese teaching hospital. BMC Infect. Dis. 2017, 17, 82. [Google Scholar] [CrossRef]
- Zheng, Y.; Wan, Y.; Zhou, L.; Ye, M.; Liu, S.; Xu, C.; He, Y.; Chen, J. Risk factors and mortality of patients with nosocomial carbapenem-resistant Acinetobacter baumannii pneumonia. Am. J. Infect. Control 2013, 41, E59–E63. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Ding, B.; Shen, Z.; Wu, H.; Xu, X.; Li, G. Clinical investigation of infections caused by carbapenem-resistant Pseudomonas aeruginosa in huashan hospital. Chin. J. Infect. Chemother. 2017, 17, 121–126. [Google Scholar]
- Xiao, T.; Yu, W.; Niu, T.; Huang, C.; Xiao, Y. A retrospective, comparative analysis of risk factors and outcomes in carbapenem-susceptible and carbapenem-nonsusceptible Klebsiella pneumoniae bloodstream infections: Tigecycline significantly increases the mortality. Infect. Drug Resist. 2018, 11, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Qin, R.; Huang, L.; Sun, L. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection and mortality of Klebsiella pneumoniae infection. Chin. Med. J. 2018, 131, 56–62. [Google Scholar] [CrossRef]
- Tian, L.; Tan, R.; Chen, Y.; Sun, J.; Liu, J.; Qu, H.; Wang, X. Epidemiology of Klebsiella pneumoniae bloodstream infections in a teaching hospital: Factors related to the carbapenem resistance and patient mortality. Antimicrob. Resist. Infect. Control 2016, 5, 48. [Google Scholar] [CrossRef]
- Jiao, Y.; Qin, Y.; Liu, J.; Li, Q.; Dong, Y.; Shang, Y.; Huang, Y.; Liu, R. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection/colonization and predictors of mortality: A retrospective study. Pathog. Glob. Health 2015, 109, 68–74. [Google Scholar] [CrossRef]
- Huang, W.; Qiao, F.; Zhang, Y.; Huang, J.; Deng, Y.; Li, J.; Zong, Z. In-hospital medical costs of infections caused by carbapenem-resistant Klebsiella pneumoniae. Clin. Infect. Dis. 2018, 672, S225–S230. [Google Scholar] [CrossRef]
- Yang, L.; Xiao, Y.; Wang, J.; Zheng, Y.; Yan, Q.; Hou, F.; Ma, Y.; Xu, S.; Sun, Z.; Lv, X. Analysis of the effect of antibiotic resistance on hospital costs. China J. Pharm. Econ. 2009, 13, 16–20. [Google Scholar]
- Cao, B.; Wang, H.; Sun, H.; Zhu, Y.; Chen, M. Risk factors and clinical outcomes of nosocomial multi-drug resistant Pseudomonas aeruginosa infections. J. Hosp. Infect. 2004, 57, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Ma, W.; Xu, X.; Yang, S.; Zhang, L. Retrospective analysis of hospital-acquired linezolid-nonsusceptible enterococci infection in Chongqing, China, 2011–2014. Am. J. Infect. Control 2015, 43, E101–E106. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Sun, J.; Bao, L.; Li, W. Risk factors and antibiotic resistance of pneumonia caused by multidrug resistant Acinetobacter baumannii in pediatric intensive care unit. World J. Emerg. Med. 2012, 3, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Baoqin, C.; Wang, X.; Ye, Q.; Lu, Z.; Su, C.; Niu, J. Case-control study of influence of methicillin-resistant Staphylococcus aureus infection on economic losses and length of hospital stay. Chin. J. Nosocomiol. 2014, 24, 2363–2365. [Google Scholar]
- Jiang, X.; Sun, J.; Xing, M.; Wang, L.; Zhang, X.; Qiu, H. Characteristics and the direct economic loss of multi-drug resistant organisms nosocomial infection in a general hospital. Chin. J. Nosocomiol. 2016, 26, 5727–5729. [Google Scholar]
- Li, C.; Han, M.; Zhou, X.; Huang, J. Study on the distribution of pathogenic bacteria and the direct economic burden caused by drug resistance in patients with bronchiectasis and infection. J. Clin. Pulm. Med. 2018, 23, 1680–1683. [Google Scholar]
- Li, H.; Lin, X.; Hua, Z.; Tu, X.; Yu, M.; Hu, X.; Yao, X.; Chen, Y. Risk factors for infection with Klebsiella pneumoniae producing drug-resistant enzymes in respiratory department. Chin. J. Clin. Res. 2016, 29, 185–188. [Google Scholar]
- Liu, X. Estimating the Direct Economic Disease Burden of Healthcare Associated Infections with Antimicrobial Resistance (AMR) of Tertiary Hospital in Hubei Province; Wuhan University: Wuhan, China, 2018; p. 69. [Google Scholar]
- Pan, H.; Chen, Q.; Chu, C.; Chen, L.; Yang, B.; Liang, C. Risk factors of multi-drug resistant infection in surgical sites. Pract. Prev. Med. 2018, 25, 367–369. [Google Scholar]
- Jiang, D.; Zuo, S.; Liang, Y.; Li, H. Risk factor for multi-drug resistant organism infection in department of respiratory medicine. J. North Sichuan Med Coll. 2016, 31, 730–733. [Google Scholar]
- Wu, X.; Ding, L.; Wu, X. Direct economic loss due to healthcare-associated infection with multi-drug resistant Acinetobacter baumannii. Chin. J. Infect. Control 2018, 17, 735–738. [Google Scholar]
- Xing, M.; Qiu, H.; Wang, L.; Sun, J. Targeted monitoring and economic burden evaluation on nosocomial infection of multi-drug resistant bacteria from 2013 to 2015. Chin. J. Disinfect. 2017, 34, 1045–1047. [Google Scholar]
- Xu, B.; Yuan, H.; Yang, P. Evaluation of economic burden induced by multi-drug resistant bacteria related infections in a tertiary general hospital. Chin. J. Exp. Clin. Infect. Dis. 2017, 11, 455–459. [Google Scholar]
- Yu, Y. Risk Factors of Nosocomial MRSA Infection and Molecular Characteristics of Staphylococcus Aureus Isolated from Blood; Suzhou University: Suzhou, China, 2016; p. 134. [Google Scholar]
- Hu, B.; Ye, H.; Xu, Y.; Ni, Y.; Hu, Y.; Yu, Y.; Huang, Z.; Ma, L. Clinical and economic outcomes associated with community-acquired intra-abdominal infections caused by extended spectrum beta-lactamase (ESBL) producing bacteria in China. Curr. Med. Res. Opin. 2010, 26, 1443–1449. [Google Scholar] [CrossRef] [PubMed]
- Zhen, X.; Chen, Y.; Hu, X.; Dong, P.; Gu, S.; Sheng, Y.Y.; Dong, H. The difference in medical costs between carbapenem-resistant Acinetobacter baumannii and non-resistant groups: A case study from a hospital in Zhejiang province, China. Eur. J. Clin. Microbiol. 2017, 36, 1989–1994. [Google Scholar] [CrossRef] [PubMed]
- Zhen, X.; Li, Y.; Chen, Y.; Dong, P.; Liu, S.; Dong, H. Effect of multiple drug resistance on total medical costs among patients with intra-abdominal infections in China. PLoS ONE 2018, 13, e0193977. [Google Scholar] [CrossRef]
- Li, X.; Chen, Y.; Gao, W.; Ouyang, W.; Wei, J.; Wen, Z. Epidemiology and outcomes of complicated skin and soft tissue infections among inpatients in southern China from 2008 to 2013. PLoS ONE 2016, 11, e0149960. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, X.L.; Huang, A.W.; Liu, S.L.; Liu, W.J.; Zhang, N.; Lu, X.Z. Mortality attributable to carbapenem-resistant Pseudomonas aeruginosa bacteremia: A meta-analysis of cohort studies. Emerg. Microbes Infect. 2016, 5, e27. [Google Scholar] [CrossRef]
- Xu, L.; Sun, X.; Ma, X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 18. [Google Scholar] [CrossRef]
- Schwaber, M.J.; Carmeli, Y. Mortality and delay in effective therapy associated with extended-spectrum beta-lactamase production in Enterobacteriaceae bacteraemia: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2007, 60, 913–920. [Google Scholar] [CrossRef]
- Ramos-Castaneda, J.A.; Ruano-Ravina, A.; Barbosa-Lorenzo, R.; Paillier-Gonzalez, J.E.; Saldana-Campos, J.C.; Salinas, D.F.; Lemos-Luengas, E.V. Mortality due to KPC carbapenemase-producing Klebsiella pneumoniae infections: Systematic review and meta-analysis: Mortality due to KPC Klebsiella pneumoniae infections. J. Infect. 2018, 76, 438–448. [Google Scholar] [CrossRef]
- Lemos, E.V.; de la Hoz, F.P.; Einarson, T.R.; McGhan, W.F.; Quevedo, E.; Castaneda, C.; Kawai, K. Carbapenem resistance and mortality in patients with Acinetobacter baumannii infection: Systematic review and meta-analysis. Clin. Microbiol. Infect. 2014, 20, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, S.E.; Sakoulas, G.; Perencevich, E.N.; Schwaber, M.J.; Karchmer, A.W.; Carmeli, Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: A meta-analysis. Clin. Infect. Dis. 2003, 36, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.; Yin, C.; Sun, X.; Huang, S.; Li, C.; Dong, P.; Lu, X.; Zhang, Z.; Yin, A. Consumption of antibiotics in Chinese public general tertiary hospitals (2011–2014): Trends, pattern changes and regional differences. PLoS ONE 2018, 13, e196668. [Google Scholar] [CrossRef] [PubMed]
- RAND Corporation. Estimating the Economic Costs of Antimicrobial Resistance. 2014. Available online: https://www.rand.org/randeurope/research/projects/antimicrobial-resistance-costs.html (accessed on 2 December 2018).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Bacteria | Comparison Group | Sample Size | Description of Mortality | Mortality Rate | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Case | Control | Case | Control | |||||||
| n | % | n | % | |||||||||
| Guo et al. [27] | 2017 | A. baumannii | MDR | non-MDR | 122 | 366 | in hospital mortality | 7 | 5.74 | 22 | 6.01 | 0.912 |
| Hu et al. [28] | 2014 | gram-negative | MDR | non-MDR | 89 | 165 | 30-day hospital mortality | 23 | 25.8 | 25 | 15.2 | <0.05 |
| Huang [29] | 2015 | K. pneumoniae | CRKP | non-CRKP | 113 | 77 | in hospital mortality | 53 | 46.9 | 26 | 33.77 | 0.07 |
| Li et al. [30] | 2014 | gram-negative/gram positive | MDR | non-MDR | 62 | 473 | in hospital mortality | 5 | 8.07 | 12 | 2.54 | <0.05 |
| Liang [31] | 2014 | A. baumannii | MDR | non-MDR | 68 | 53 | in hospital mortality | 13 | 19.12 | 3 | 5.66 | 0.03 |
| Lv et al. [32] | 2015 | P. aeruginosa | CRPA | CSPA | 32 | 68 | in hospital mortality | 2 | 13.33 | 1 | 1.79 | <0.05 |
| Pei [33] | 2015 | A. baumannii | MDR | non-MDR | 226 | 65 | in hospital mortality | 80 | 35.4 | 13 | 20 | 0.019 |
| Wang [34] | 2018 | gram-negative | carbapenem resistance | carbapenem susceptibility | 26 | 113 | 28-day hospital mortality | 13 | 50 | 15 | 13.3 | <0.001 |
| Wang et al. [35] | 2016 | A. baumannii | CRAB | CSAB | 97 | 145 | in hospital mortality | 44 | 45.6 | 43 | 29.9 | 0.02 |
| Zhang et al. [36] | 2013 | S. aureus | MRSA | without infection | 192 | 384 | in hospital mortality | 21 | 10.94 | 17 | 4.43 | 0.03 |
| Zhou et al. [37] | 2015 | S. aureus | MRSA | MSSA | 91 | 266 | in hospital mortality | 12 | 13.19 | 24 | 9.02 | 0.26 |
| Chen et al. [38] | 2016 | S. aureus | MRSA | MSSA | 75 | 78 | in hospital mortality | 13 | 17.33 | 7 | 8.97 | 0.131 |
| 46 | 46 | in hospital mortality | 5 | 10.87 | 7 | 15.22 | 0.385 | |||||
| Cui et al. [39] | 2012 | A. baumannii | IRAB | ISAB | 138 | 138 | in hospital mortality | 54 | 39.1 | 28 | 20.3 | <0.01 |
| Long et al. [40] | 2015 | Gram-negative | carbapenem resistance | carbapenem susceptibility | 34 | 34 | in hospital mortality | 16 | 47.1 | 7 | 20.6 | 0.021 |
| Zhu et al. [41] | 2016 | S. aureus | MRSA | MSSA | 22 | 42 | in hospital mortality | 6 | 27.3 | 6 | 14.3 | 0.312 |
| Yang et al. [42] | 2018 | A. baumannii | CRAB | CSAB | 84 | 34 | in hospital mortality | 23 | 27.4 | 2 | 5.9 | 0.011 |
| 84 | 34 | 30-day hospital mortality | 13 | 15.5 | 2 | 5.9 | 0.025 | |||||
| Chen et al. [43] | 2018 | P. aeruginosa | CRPA | CSPA | 327 | 472 | in hospital mortality | 51 | 15.6 | 30 | 6.4 | <0.001 |
| 270 | 270 | in hospital mortality | 34 | 12.6 | 21 | 7.8 | 0.044 | |||||
| Meng et al. [44] | 2017 | E. coli | CREC | CSEC | 49 | 96 | in hospital mortality | 6 | 12 | 1 | 1 | 0.01 |
| CREC | without infection | 49 | 96 | in hospital mortality | 6 | 12 | 1 | 1 | 0.01 | |||
| Zheng et al. [45] | 2013 | A. baumannii | CRAB | CSAB | 97 | 145 | 28-day hospital mortality | 44 | 45.6 | 43 | 29.9 | 0.02 |
| Yuan et al. [46] | 2017 | P. aeruginosa | CRPA | CSPA | 85 | 94 | in hospital mortality | 14 | 16.5 | 1 | 1.1 | <0.001 |
| Xiao et al. [47] | 2018 | K. pneumoniae | CNSKP | CSKP | 135 | 293 | 30-day hospital mortality | 79 | 58.5 | 45 | 15.4 | <0.001 |
| Wang et al. [48] | 2018 | K. pneumoniae | CRKP | CSKP | 48 | 48 | in hospital mortality | 23 | 47.9 | 2 | 4.2 | 0.03 |
| Tian et al. [49] | 2016 | K. pneumoniae | CRKP | CSKP | 33 | 81 | in hospital mortality | 14 | 42.4 | 16 | 19.8 | 0.013 |
| 33 | 81 | 28-day hospital mortality | 11 | 33.3 | 15 | 18.5 | 0.087 | |||||
| 33 | 81 | attributable 28-day hospital mortality | 11 | 33.3 | 13 | 16 | 0.04 | |||||
| 33 | 81 | attributable in hospital mortality | 14 | 42.4 | 14 | 24.6 | 0.005 | |||||
| Jiao et al. [50] | 2015 | K. pneumoniae | CRKP | CSKP | 30 | 30 | in hospital mortality | 10 | 33.3 | 5 | 16.7 | >0.05 |
| Huang et al. [51] | 2018 | K. pneumoniae | CRKP | CSKP | 237 | 237 | in hospital mortality | 32 | 13.5 | 25 | 10.55 | 0.324 |
| 237 | 1328 | in hospital mortality | 39 | 14.61 | 75 | 5.65 | <0.001 | |||||
| Yang et al. [52] | 2009 | gram-positive/gram-negative | resistance | non-resistance | 676 | 732 | in hospital mortality | 79 | 11.7 | 40 | 5.4 | <0.001 |
| Cao et al. [53] | 2004 | P. aeruginosa | MDR P. aeruginosa | susceptibility | 44 | 68 | in hospital mortality | 24 | 54.5 | 11 | 16.2 | <0.05 |
| Jia et al. [54] | 2015 | Enterococcus | linezolid non-susceptibility | linezolid susceptibility | 44 | 44 | in hospital mortality | 3 | 6.8 | 2 | 4.5 | >0.05 |
| linezolid non-susceptibility | Inpatients during the same time | 44 | 176 | in hospital mortality | 3 | 6.8 | 3 | 1.7 | >0.05 | |||
| Cai et al. [55] | 2012 | A. baumannii | MDR | non-MDR | 115 | 45 | in hospital mortality | 21 | 18.26 | 2 | 4.44 | <0.05 |
| Author | Year | Bacteria | Comparison Group | Sample Size | Description of LOS | LOS | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Case | Control | Case | Control | ||||||||
| Fu et al. [56] | 2014 | S. aureus | MRSA | without infection | 456 | 706 | total LOS | median (Q) | 31 | 42 | 16 | 14 | 0.001 |
| Guo et al. [27] | 2017 | A. baumannii | MDR | non-MDR | 122 | 366 | total LOS | mean (SD) | 24 | 17 | 11 | 9 | <0.001 |
| median (Q1-Q3) | 19 | (13–29) | 9 | (5–15) | <0.001 | ||||||||
| Hu et al. [28] | 2014 | gram-negative | MDR | non-MDR | 89 | 165 | total LOS | median (IQR) | 24 | (18–39) | 25 | (17–52) | >0.05 |
| Huang [29] | 2015 | K. pneumoniae | CRKP | non-CRKP | 113 | 77 | total LOS | mean (SD) | 70 | 69 | 32 | 34 | <0.000 |
| ICU LOS | mean (SD) | 59 | 70 | 22 | 33 | <0.001 | |||||||
| Jiang et al. [57] | 2016 | gram-negative/gram-positive | MDR | non-MDR | 41 | 41 | total LOS | median (Q) | 24 | 25 | 19 | 14 | 0.01 |
| Li et al. [58] | 2018 | gram-negative/gram-positive | MDR | susceptibility | 78 | 78 | total LOS | mean (SD) | 14 | 6 | 11 | 3 | <0.001 |
| Li et al. [59] | 2016 | K. pneumoniae | resistant enzymes producing | non-resistant enzymes producing | 41 | 80 | total LOS | mean (SD) | 22 | 17 | 14 | 9 | 0.003 |
| LOS before infection | mean (SD) | 8 | 8 | 5 | 5 | 0.017 | |||||||
| Liang [31] | 2014 | A. baumannii | MDR | non-MDR | 68 | 53 | total LOS | mean (SD) | 24 | 10 | 14 | 5 | 0.002 |
| Liu [60] | 2018 | gram-negative/gram-positive | antibiotic resistance | without nosocomial infection | 133 | 133 | total LOS | mean | 68 | 28 | <0.05 | ||
| Lv et al. [32] | 2015 | P. aeruginosa | CRPA | CSPA | 32 | 68 | LOS after admitting ICU | mean (SD) | 11 | 1 | 3 | 1 | 0.01 |
| Pan et al. [61] | 2018 | gram-negative/gram-positive | MDR | susceptibility | 102 | 79 | total LOS | mean (SD) | 36 | 22 | 29 | 18 | 0.026 |
| Pei [33] | 2015 | A. baumannii | MDR | non-MDR | 226 | 65 | total LOS | mean (SD) | 35 | 25 | 27 | 17 | 0.002 |
| Wang [34] | 2018 | gram-negative | carbapenem resistance | carbapenem susceptibility | 26 | 113 | LOS before infection | median (IQR) | 19 | (3–42) | 3 | (0–13) | <0.001 |
| Jiang [62] | 2018 | gram-negative | MDR | non-MDR | 79 | 79 | total LOS | mean (SD) | 19 | 15 | 13 | 7 | <0.05 |
| LOS before infection | mean (SD) | 10 | 5 | 9 | 7 | <0.05 | |||||||
| Wang et al. [35] | 2016 | A. baumannii | CRAB | CSAB | 97 | 145 | LOS before pneumonia | mean (SD) | 18 | 6 | 18 | 7 | 0.38 |
| Wu et al. [63] | 2018 | A. baumannii | MDR | non-MDR | 65 | 65 | total LOS | median (Q) | 52 | 42 | 27 | 21 | <0.01 |
| Xing et al. [64] | 2017 | gram-negative/gram-positive | MDR | without infection | 178 | 178 | total LOS | median (IQR) | 32 | (23–47) | 12 | (9–27) | <0.001 |
| Xu et al. [65] | 2017 | E. coli | MDR | non-MDR | 969 | 1940 | total LOS | mean (SD) | 19 | 23 | 13 | 12 | <0.001 |
| K. pneumoniae | MDR | non-MDR | 186 | 529 | total LOS | mean (SD) | 19 | 16 | 15 | 14 | 0.03 | ||
| Proteus mirabilis | MDR | non-MDR | 38 | 60 | total LOS | mean (SD) | 25 | 22 | 14 | 9 | 0.002 | ||
| A. baumannii | MDR | non-MDR | 53 | 45 | total LOS | mean (SD) | 22 | 21 | 16 | 11 | 0.045 | ||
| P. aeruginosa | MDR | non-MDR | 13 | 490 | total LOS | mean (SD) | 64 | 43 | 18 | 17 | <0.001 | ||
| Enterobacter cloacae | MDR | non-MDR | 94 | 166 | total LOS | mean (SD) | 29 | 31 | 18 | 19 | 0.001 | ||
| S. aureus | MDR | non-MDR | 41 | 237 | total LOS | mean (SD) | 21 | 18 | 14 | 15 | 0.008 | ||
| coagulase-negative Staphylococci | MDR | non-MDR | 76 | 184 | total LOS | mean (SD) | 26 | 26 | 18 | 16 | 0.002 | ||
| Yu [66] | 2016 | S. aureus | MRSA | MSSA | 118 | 116 | total LOS | median | 33 | 14 | <0.05 | ||
| Zhang et al. [36] | 2013 | S. aureus | MRSA | without infection | 192 | 384 | total LOS | mean (SD) | 27 | 9 | 18 | 9 | <0.01 |
| Zhou et al. [37] | 2015 | S. aureus | MRSA | MSSA | 91 | 266 | total LOS | median (IQR) | 29 | (21–60) | 23 | (15–42) | <0.01 |
| LOS before infection | median (IQR) | 11 | (4–23) | 3.5 | (0–13) | <0.01 | |||||||
| LOS after infection | median (IQR) | 17 | (7–31) | 16.5 | (8–29) | 0.92 | |||||||
| Chen et al. [38] | 2016 | S. aureus | MRSA | MSSA | 75 | 78 | total LOS | median (IQR) | 40 | (20–94) | 28 | (21–53) | 0.003 |
| 46 | 46 | total LOS | median (IQR) | 28 | (21–52) | 28 | (21–53) | 0.899 | |||||
| 75 | 78 | LOS after infection | median (IQR) | 19 | (10–46) | 17 | (8–29) | 0.011 | |||||
| 46 | 46 | LOS after infection | median (IQR) | 15 | (9–25) | 17 | (8–29) | 0.676 | |||||
| Cui et al. [39] | 2012 | A. baumannii | IRAB | ISAB | 138 | 138 | total LOS | median (IQR) | 29 | (19–57) | 23 | (15–39) | <0.01 |
| ICU LOS | median (IQR) | 15 | (8–28) | 0 | (0–10) | <0.01 | |||||||
| LOS before infection | median (IQR) | 10 | (4–20) | 13 | (7–20) | >0.05 | |||||||
| Long et al. [40] | 2015 | gram-negative | carbapenem resistance | carbapenem susceptibility | 34 | 34 | total LOS | mean (SD) | 28 | 3 | 22 | 2 | >0.05 |
| ICU LOS | mean (SD) | 17 | 3 | 13 | 3 | >0.05 | |||||||
| Zhu et al. [41] | 2016 | S. aureus | MRSA | MSSA | 22 | 42 | total LOS | mean (SD) | 26 | 23 | 15 | 11 | 0.062 |
| Hu et al. [67] | 2010 | E. coli/Klebsiella spp. | ESBL-positive | ESBL-negative | 32 | 53 | total LOS | mean | 24 | 15 | 0.001 | ||
| Zhen et al. [68] | 2017 | A. baumannii | CRAB | CSAB | 2126 | 854 | LOS before infection | mean (SD) | 10 | 16 | 11 | 28 | 0.057 |
| Zhen et al. [69] | 2018 | gram-negative/gram-positive | MDR | non-MDR | 64 | 37 | total LOS | mean (SD) | 31 | 29 | 16 | 13 | <0.000 |
| Chen et al. [43] | 2018 | P. aeruginosa | CRPA | CSPA | 327 | 472 | total LOS | median (IQR) | 29 | (17–44) | 21 | (11–34) | <0.001 |
| 270 | 270 | total LOS | median (IQR) | 29 | (17–42) | 26 | (14–41) | 0.026 | |||||
| 327 | 472 | LOS after infection | median (IQR) | 17 | (8–32) | 13 | (7–25) | 0.005 | |||||
| 270 | 270 | LOS after infection | median (IQR) | 19 | (8–30) | 14 | (7–28) | 0.029 | |||||
| Wang et al. [48] | 2018 | K. pneumoniae | CRKP | CSKP | 48 | 48 | total LOS | median (IQR) | 84 | (41–188) | 33 | (21–60) | 0.097 |
| Tian et al. [49] | 2016 | K. pneumoniae | CRKP | CSKP | 33 | 81 | total LOS | median (IQR) | 50 | (28–83) | 24 | (16.5–51) | 0.001 |
| LOS after infection | median (IQR) | 24 | (10–51) | 15 | (9–28) | 0.066 | |||||||
| Jiao et al. [50] | 2015 | K. pneumoniae | CRKP | CSKP | 30 | 30 | total LOS | mean (SD) | 34 | 31 | 18 | 23 | 0.054 |
| LOS before infection | mean (SD) | 34 | 31 | 13 | 27 | 0.02 | |||||||
| Huang et al. [51] | 2018 | K. pneumoniae | CRKP | CSKP | 237 | 237 | total LOS | median (range) | 31 | (22–55) | 24 | (14–46) | <0.001 |
| 237 | 1328 | total LOS | median (range) | 31 | (22–56) | 19 | (11–35) | <0.001 | |||||
| 237 | 1328 | LOS before infection | median (range) | 13 | (2–25) | 3 | (0–11) | <0.001 | |||||
| 237 | 1328 | LOS after infection | median (range) | 21 | (10–44) | 18 | (9–46) | 0.612 | |||||
| Yang et al. [52] | 2009 | gram-negative/gram-positive | resistance | non-resistance | 676 | 732 | total LOS | mean (SD) | 34 | 39 | 18 | 24 | <0.001 |
| total LOS | median | 21 | 12 | <0.001 | |||||||||
| infection related LOS | mean (SD) | 22 | 21 | 12 | 13 | <0.001 | |||||||
| infection related LOS | median | 15 | 9 | <0.001 | |||||||||
| Li et al. [70] | 2016 | S. aureus | MRSA | MSSA | 14 | 61 | total LOS | mean (SD) | 38 | 47 | 19 | 14 | 0.12 |
| total LOS | median | 19 | 15 | 0.12 | |||||||||
| Jia et al. [54] | 2015 | Enterococcus | linezolid nonsusceptibility | linezolid susceptibility | 44 | 44 | total LOS | median (IQR) | 37 | (15–57) | 22 | (9–43) | <0.05 |
| linezolid nonsusceptibility | inpatients during the same time | 44 | 176 | total LOS | median (IQR) | 37 | (15–57) | 17 | (11–28) | <0.05 | |||
| linezolid nonsusceptibility | linezolid susceptibility | 44 | 44 | LOS after infection | median (IQR) | 8 | (3–15) | 5 | (3–20) | <0.05 | |||
| linezolid nonsusceptibility | inpatients in the same time | 44 | 176 | LOS after infection | median (IQR) | 8 | (3–15) | 4 | (1–12) | <0.05 | |||
| Cai et al. [55] | 2012 | A. baumannii | MDR | non-MDR | 115 | 45 | total LOS | mean (SD) | 19 | 9 | 14 | 4 | 0.001 |
| ICU LOS | mean (SD) | 17 | 7 | 14 | 4 | 0.009 | |||||||
| Author | Year | Bacteria | Comparison Group | Sample Size | Description of Cost | Mean (Median) Costs in 2015 USD | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Case | Control | Case | Control | |||||
| Fu et al. [56] | 2014 | S. aureus | MRSA | without infection | 456 | 706 | total hospital cost | (15,763) | (2185) | 0.001 |
| Li et al. [70] | 2016 | S. aureus | MRSA | MSSA | 14 | 61 | total hospital cost | 5305(319) | 2658(352) | 0.39 |
| Chen et al. [38] | 2016 | S. aureus | MRSA | MSSA | 75 | 78 | treatment cost | (23,933) | (19,905) | 0.395 |
| 46 | 46 | treatment cost | (19,718) | (19,538) | 0.935 | |||||
| Hu et al. [28] | 2014 | gram-negative | MDR | non-MDR | 89 | 165 | total hospital cost | (12,360) | (11,591) | >0.05 |
| 89 | 165 | antibiotic cost | (1946) | (1397) | <0.01 | |||||
| Long et al. [40] | 2015 | gram-negative | carbapenem resistance | carbapenem susceptibility | 34 | 34 | total treatment cost | 11,206 | 6686 | 0.034 |
| Jiang et al. [57] | 2016 | gram-positive/gram-negative | MDR | non-MDR | 41 | 41 | total hospital cost | (10,832) | (6607) | <0.00 |
| Li et al. [58] | 2018 | gram-positive/gram-negative | MDR | susceptibility | 78 | 78 | total hospital cost | 1660 | 1093 | <0.001 |
| 78 | 78 | antibiotic cost | 485 | 322 | <0.001 | |||||
| Liu [60] | 2018 | gram-positive/gram-negative | antibiotic resistance | without nosocomial infection | 133 | 133 | total hospital cost | 20,222 | 3726 | <0.05 |
| Pan et al. [61] | 2018 | gram-positive/gram-negative | MDR | susceptibility | 102 | 79 | total hospital cost | 12,602 | 9793 | <0.001 |
| 102 | 79 | antibiotic cost | 952 | 740 | <0.001 | |||||
| Yang et al. [52] | 2009 | gram-positive/gram-negative | resistance | non-resistance | 676 | 732 | total hospital cost | 11,035(4303) | 2940(1103) | <0.001 |
| 676 | 732 | antibiotic cost | 812(418) | 274(119) | <0.000 | |||||
| Xing et al. [64] | 2017 | gram-positive/gram-negative | MDR | without infection | 178 | 178 | total hospital cost | (16,138) | (1714) | <0.001 |
| Zhen et al. [69] | 2018 | gram-positive/gram-negative | MDR | non-MDR | 64 | 37 | total hospital cost | 21,164 | 6680 | <0.000 |
| 64 | 37 | antibiotic cost | 4001 | 760 | <0.000 | |||||
| Guo et al. [27] | 2017 | A. baumannii | MDR | non-MDR | 122 | 366 | total hospital cost | 14,159(10,452) | 7487(3759) | <0.001 |
| Wu et al. [63] | 2018 | A. baumannii | MDR | non-MDR | 65 | 65 | total hospital cost | (24,897) | (8823) | <0.01 |
| 65 | 65 | daily hospital cost | (581) | (688) | 0.14 | |||||
| Cui et al. [39] | 2012 | A. baumannii | IRAB | ISAB | 138 | 138 | daily total hospital cost | (591) | (338) | <0.01 |
| 138 | 138 | daily antibiotic cost | (90) | (55) | <0.01 | |||||
| Zhen et al. [68] | 2017 | A. baumannii | CRAB | CSAB | 2126 | 854 | total hospital cost | 30,575 | 19,783 | <0.000 |
| 2126 | 854 | antibiotic cost | 3047 | 1692 | <0.000 | |||||
| Chen et al. [43] | 2018 | P. aeruginosa | CRPA | CSPA | 327 | 472 | total hospital cost | (925) | (482) | <0.001 |
| 270 | 270 | total hospital cost | (868) | (707) | 0.015 | |||||
| 327 | 472 | daily hospital cost | (36) | (27) | <0.001 | |||||
| 270 | 270 | daily hospital cost | (34) | (32) | 0.045 | |||||
| Xu et al. [65] | 2017 | E. coli | MDR | non-MDR | 969 | 1940 | total hospital cost | 3645 | 2071 | <0.001 |
| 969 | 1940 | antibiotic cost | 234 | 154 | <0.001 | |||||
| K. pneumoniae | MDR | non-MDR | 186 | 529 | total hospital cost | 5132 | 3178 | 0.001 | ||
| 186 | 529 | antibiotic cost | 263 | 246 | 0.59 | |||||
| Proteus mirabilis | MDR | non-MDR | 38 | 60 | total hospital cost | 6383 | 2700 | <0.001 | ||
| 38 | 60 | antibiotic cost | 271 | 114 | 0.001 | |||||
| A. baumannii | MDR | non-MDR | 53 | 45 | total hospital cost | 5446 | 3100 | 0.025 | ||
| 53 | 45 | antibiotic cost | 222 | 136 | 0.054 | |||||
| P. aeruginosa | MDR | non-MDR | 13 | 490 | total hospital cost | 13,820 | 3847 | <0.001 | ||
| 13 | 490 | antibiotic cost | 884 | 325 | <0.001 | |||||
| Enterobacter cloacae | MDR | non-MDR | 94 | 166 | total hospital cost | 7788 | 3812 | <0.001 | ||
| 94 | 166 | antibiotic cost | 386 | 255 | 0.01 | |||||
| S. aureus | MDR | non-MDR | 41 | 237 | total hospital cost | 4139 | 2355 | 0.006 | ||
| 41 | 237 | antibiotic cost | 223 | 141 | 0.007 | |||||
| coagulase-negative Staphylococci | MDR | non-MDR | 76 | 184 | total hospital cost | 9028 | 3215 | <0.001 | ||
| 76 | 184 | antibiotic cost | 362 | 212 | <0.001 | |||||
| Hu et al. [67] | 2010 | E. coli/Klebsiella spp. | ESBL-positive | ESBL-negative | 32 | 53 | total hospital cost | 541 | 303 | <0.001 |
| 32 | 53 | cost of intravenous antibiotics | 98 | 40 | 0.001 | |||||
| Meng et al. [44] | 2017 | E. coli | CREC | CSEC | 49 | 96 | total hospital cost | (12,670) | (10,290) | 0.05 |
| without infection | 49 | 96 | total hospital cost | (12,670) | (2818) | <0.00 | ||||
| Huang et al. [51] | 2018 | K. pneumoniae | CRKP | CSKP | 237 | 237 | total hospital cost | (21,170) | (11,313) | <0.001 |
| 237 | 237 | total antibiotic cost | (2253) | (1251) | <0.01 | |||||
| 237 | 237 | hospital cost after infection | (8912) | (6677) | 0.003 | |||||
| 237 | 237 | antibiotic cost after infection | (973) | (573) | <0.001 | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhen, X.; Stålsby Lundborg, C.; Sun, X.; Hu, X.; Dong, H. The Clinical and Economic Impact of Antibiotic Resistance in China: A Systematic Review and Meta-Analysis. Antibiotics 2019, 8, 115. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8030115
Zhen X, Stålsby Lundborg C, Sun X, Hu X, Dong H. The Clinical and Economic Impact of Antibiotic Resistance in China: A Systematic Review and Meta-Analysis. Antibiotics. 2019; 8(3):115. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8030115
Chicago/Turabian StyleZhen, Xuemei, Cecilia Stålsby Lundborg, Xueshan Sun, Xiaoqian Hu, and Hengjin Dong. 2019. "The Clinical and Economic Impact of Antibiotic Resistance in China: A Systematic Review and Meta-Analysis" Antibiotics 8, no. 3: 115. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8030115