Comparative Epidemiology and Resistance Trends of Proteae in Urinary Tract Infections of Inpatients and Outpatients: A 10-Year Retrospective Study



Abstract
:
1. Introduction
2. Results
2.1. Demographic Characteristics, Sample Types
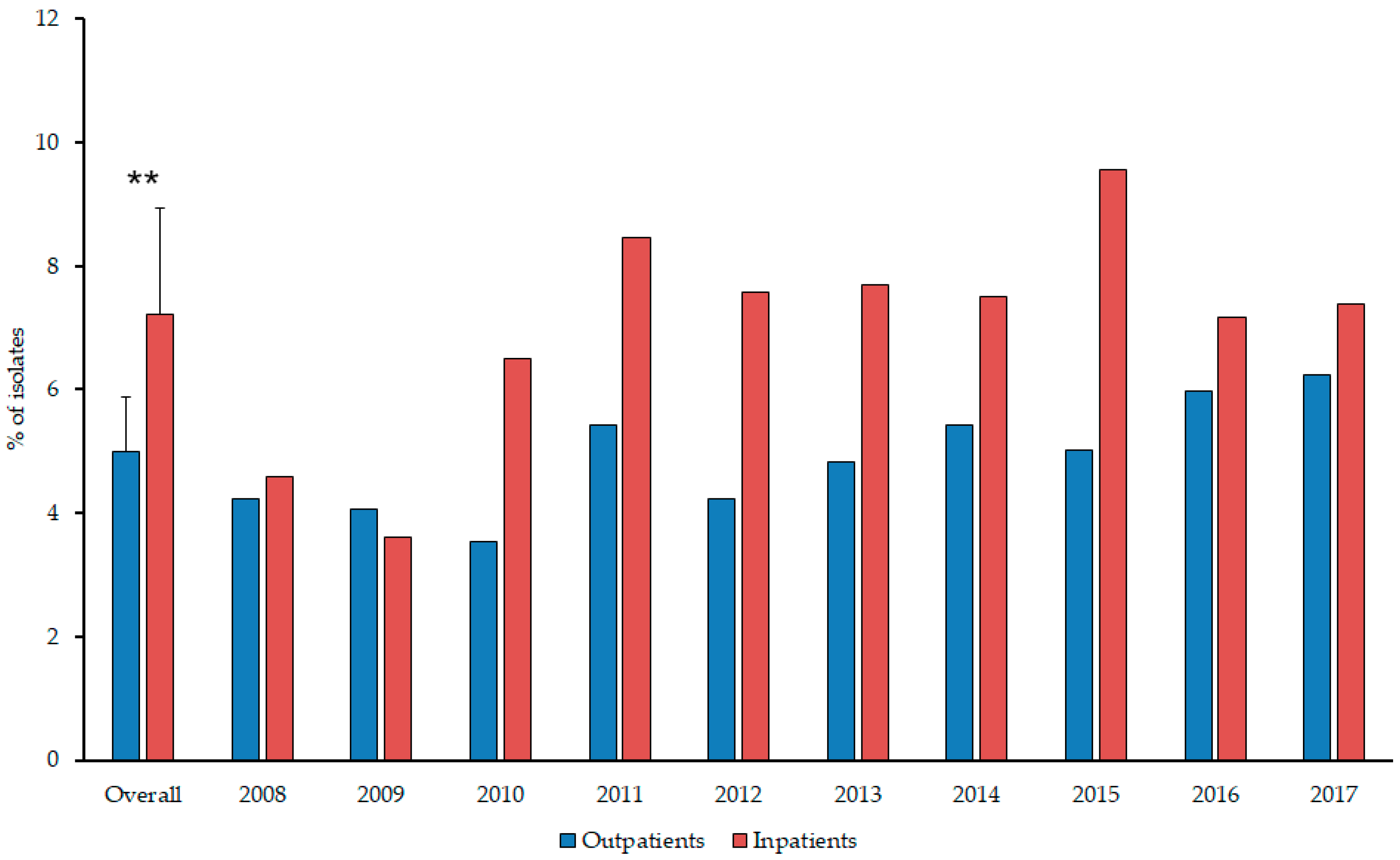
2.2. Distribution of Proteae among Inpatient and Outpatient Urine Samples
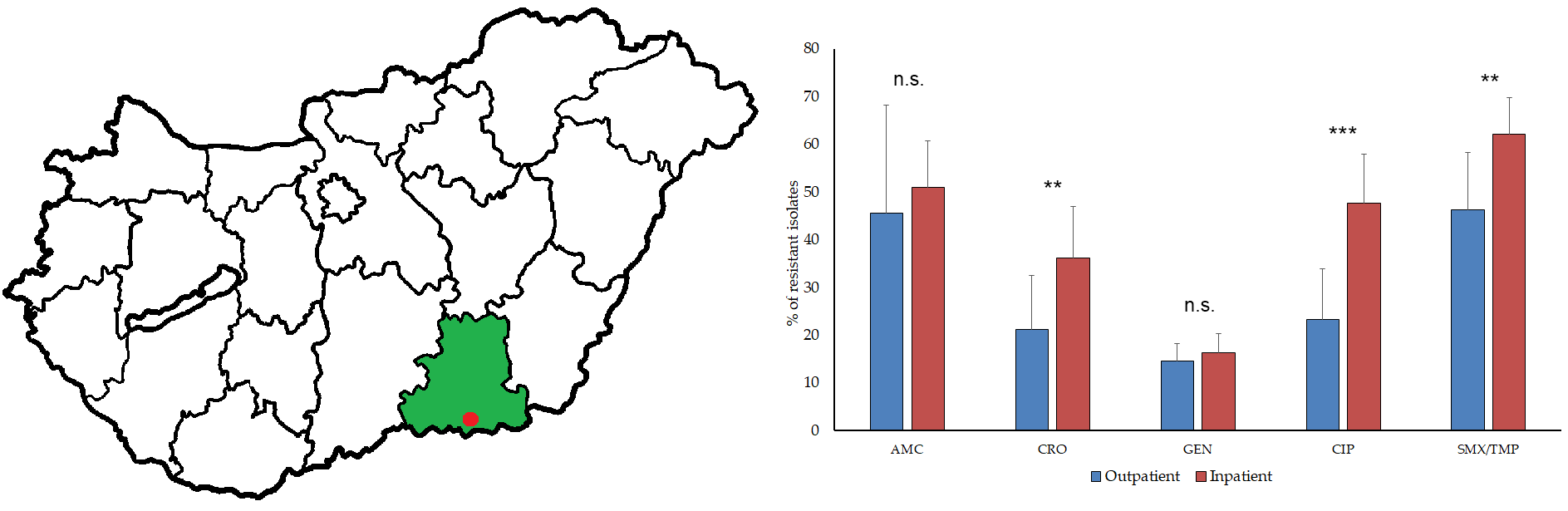
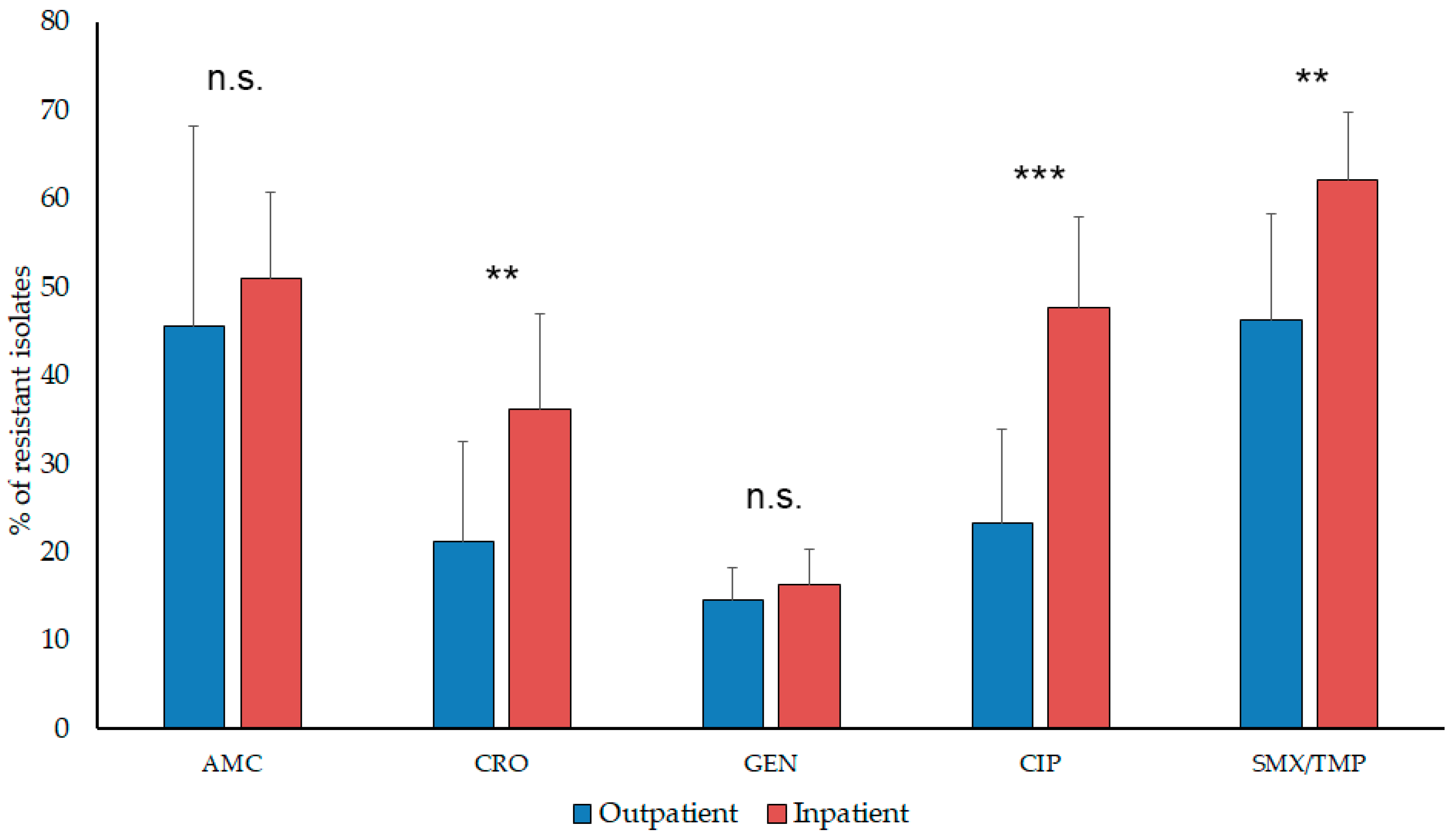
2.3. Antibiotic Susceptibility Trends among Proteae
3. Discussion
4. Materials and Methods
4.1. Study Design, Data Collection
4.2. Identification of Isolates
4.3. Antimicrobial Susceptibility Testing
4.4. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
List of abbreviations
References
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious diseases society of America and the European society for microbiology and infectious diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [PubMed]
- Wiedemann, B.; Heisig, A.; Heisig, P. Uncomplicated urinary tract infections and antibiotic resistance-epidemiological and mechanistic aspects. Antibiotics 2014, 3, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Hooton, T.M.; Bradley, S.F.; Cardenas, D.D.; Colgan, R.; Geerlings, S.E.; Rice, J.C.; Saint, S.; Schaeffer, A.J.; Tambayh, P.A.; Tenke, P.; et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 international clinical practice guidelines from the infectious diseases society of America. Clin. Infect. Dis. 2010, 50, 625–663. [Google Scholar] [CrossRef] [PubMed]
- Stefaniuk, E.; Suchocka, U.; Bosacka, K.; Hryniewicz, W. Etiology and antibiotic susceptibility of bacterial pathogens responsible for community-acquired urinary tract infections in Poland. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1363–1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achkar, J.M.; Fries, B.C. Candida infections of the genitourinary tract. Clin. Microbiol. Rev. 2010, 23, 253–273. [Google Scholar] [CrossRef] [PubMed]
- Calzi, A.; Grignolo, S.; Caviglia, I.; Calevo, M.G.; Losurdo, G.; Piaggio, G.; Bandettini, R.; Castagnola, E. Resistance to oral antibiotics in 4569 Gram-negative rods isolated from urinary tract infection in children. Eur. J. Pediatr. 2016, 175, 1219–1225. [Google Scholar] [CrossRef]
- Gajdács, M. The concept of an ideal antibiotic: Implications for drug design. Molecules 2019, 24, 892. [Google Scholar] [CrossRef]
- Spengler, G.; Kincses, A.; Gajdacs, M.; Amaral, L. New roads leading to old destinations: Efflux pumps as targets to reverse multidrug resistance in bacteria. Molecules 2017, 22, 468. [Google Scholar] [CrossRef]
- Codjoe, F.S.; Donkor, E.S. Carbapenem resistance: A review. Med. Sci. 2018, 6, 1. [Google Scholar] [CrossRef]
- Dhillon, R.H.-P.; Clark, J. ESBLs: A clear and present danger? Crit. Care Res. Pract. 2012, 2012, 625170. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M. [Extra deaths due to pandrug resistant bacteria: A survey of the literature]. Egészségfejlesztés 2019, 60, 31–36. [Google Scholar]
- O’Hara, C.M.; Brenner, F.W.; Miller, J.M. Classification, identification, and clinical significance of Proteus, Providencia, and Morganella. Clin. Microbiol. Rev. 2000, 13, 534–546. [Google Scholar] [CrossRef] [PubMed]
- Manos, J.; Belas, R. The genera Proteus, Providencia, and Morganella. In The Prokaryotes: Volume 6: Proteobacteria: Gamma Subclass; Dworkin, M., Falkow, S., Rosenberg, E., Schleifer, K.-H., Stackebrandt, E., Eds.; Springer: New York, NY, USA, 2006; pp. 245–269. ISBN 978-0-387-30746-6. [Google Scholar]
- Taxonomy of the family Morganellaceae Adeolu et al. 2016. Available online: https://www.namesforlife.com/10.1601/tx.29308 (accessed on 14 May 2019). [CrossRef]
- Adeolu, M.; Alnajar, S.; Naushad, S.; Gupta, R.S. Genome-based phylogeny and taxonomy of the “Enterobacteriales”: Proposal for Enterobacterales ord. nov. divided into the families Enterobacteriaceae, Erwiniaceae fam. nov., Pectobacteriaceae fam. nov., Yersiniaceae fam. nov., Hafniaceae fam. nov., Morganellaceae fam. nov., and Budviciaceae fam. nov. Int. J. Syst. Evol. Microbiol. 2016, 66, 5575–5599. [Google Scholar] [PubMed]
- Braunstein, H.; Tomasulo, M. Identification of Proteus morganii and distinction from other Proteus species. Am. J. Clin. Pathol. 1978, 70, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Pignato, S.; Giammanco, G.M.; Grimont, F.; Grimont, P.A.D.; Giammanco, G. Molecular characterization of the Genera Proteus, Morganella, and Providencia by Ribotyping. J. Clin. Microbiol. 1999, 37, 2840–2847. [Google Scholar] [PubMed]
- Barnaud, G.; Arlet, G.; Danglot, C.; Philippon, A. Cloning and sequencing of the gene encoding the AmpC beta-lactamase of Morganella morganii. FEMS Microbiol. Lett. 1997, 148, 15–20. [Google Scholar] [CrossRef]
- Penner, J.; Allerberger, F.; Dierich, M.P.; Pfaller, W.; Hager, J. In vitro experiments on catheter-related infections due to gram-negative rods. Chemotherapy 1993, 39, 336–354. [Google Scholar] [CrossRef] [PubMed]
- Maharjan, G.; Khadka, P.; Shilpakar, G.S.; Chapagain, G.; Dhungana, G.R. Catheter-associated urinary tract infection and obstinate biofilm producers. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 7624857. [Google Scholar] [CrossRef] [PubMed]
- Cortese, Y.J.; Wagner, V.E.; Tierney, M.; Devine, D.; Fogarty, A. Review of catheter-associated urinary tract infections and in vitro urinary tract models. J. Healthc. Eng. 2018, 2018, 2986742. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, S.M.; Stickler, D.J.; Mobley, H.L.T.; Shirtliff, M.E. Complicated catheter-associated urinary tract infections due to Escherichia coli and Proteus mirabilis. Clin. Microbiol. Rev. 2008, 21, 26–59. [Google Scholar] [CrossRef] [PubMed]
- Mazzariol, A.; Bazaj, A.; Cornaglia, G. Multi-drug-resistant Gram-negative bacteria causing urinary tract infections: A review. J. Chemother. 2017, 29, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Morrissey, I.; Hackel, M.; Badal, R.; Bouchillon, S.; Hawser, S.; Biedenbach, D. A review of ten years of the study for monitoring antimicrobial resistance trends (SMART) from 2002 to 2011. Pharmaceuticals 2013, 6, 1335–1346. [Google Scholar] [CrossRef] [PubMed]
- Sader, H.S.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Antimicrobial susceptibility of Gram-negative organisms isolated from patients hospitalised with pneumonia in US and European hospitals: Results from the SENTRY Antimicrobial Surveillance Program, 2009–2012. Int. J. Antimicrob. Agents 2014, 43, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Ponce-de-Leon, A.; Rodríguez-Noriega, E.; Morfín-Otero, R.; Cornejo-Juárez, D.P.; Tinoco, J.C.; Martínez-Gamboa, A.; Gaona-Tapia, C.J.; Guerrero-Almeida, M.L.; Martin-Onraët, A.; Vallejo Cervantes, J.L.; et al. Antimicrobial susceptibility of gram-negative bacilli isolated from intra-abdominal and urinary-tract infections in Mexico from 2009 to 2015: Results from the study for monitoring antimicrobial resistance trends (SMART). PLoS ONE 2018, 13, e0198621. [Google Scholar] [CrossRef] [PubMed]
- Laupland, K.B.; Parkins, M.D.; Ross, T.; Pitout, J.D.D. Population-based laboratory surveillance for tribe Proteeae isolates in a large Canadian health region. Clin. Microbiol. Infect. 2007, 13, 683–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, S.; Weber, R.; Zbinden, R.; Ruef, C.; Hasse, B. Extended-spectrum β-lactamase-producing Gram-negative pathogens in community-acquired urinary tract infections: An increasing challenge for antimicrobial therapy. Infection 2011, 39, 333–340. [Google Scholar] [CrossRef]
- Luzzaro, F.; Perilli, M.; Amicosante, G.; Lombardi, G.; Belloni, R.; Zollo, A.; Bianchi, C.; Toniolo, A. Properties of multidrug-resistant, ESBL-producing Proteus mirabilis isolates and possible role of beta-lactam/beta-lactamase inhibitor combinations. Int. J. Antimicrob. Agents 2001, 17, 131–135. [Google Scholar] [CrossRef]
- Magyar, A.; Köves, B.; Nagy, K.; Dobák, A.; Arthanareeswaran, V.K.A.; Bálint, P.; Wagenlehner, F.; Tenke, P. Spectrum and antibiotic resistance of uropathogens between 2004 and 2015 in a tertiary care hospital in Hungary. J. Med. Microbiol. 2017, 66, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Takhar, S.S.; Moran, G.J. Diagnosis and management of urinary tract infection in the emergency department and outpatient settings. Infect. Dis. Clin. N. Am. 2014, 28, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Yang, F.; Wang, S.; Wang, Q.; Liu, Z.; Feng, W.; Sun, F.; Xia, P. Analysis of the spectrum and antibiotic resistance of uropathogens in outpatients a. tertiary hospital. J. Chemother. 2018, 30, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M.; Paulik, E.; Szabó, A. [The opinions of community pharmacists related to antibiotic use and resistance] (article in Hungarian). Acta Pharm. Hung. 2018, 88, 249–252. [Google Scholar]
- Kim, B.-N.; Kim, N.J.; Kim, M.-N.; Kim, Y.S.; Woo, J.-H.; Ryu, J. Bacteraemia due to tribe Proteeae: A review of 132 cases during a decade (1991–2000). Scand. J. Infect. Dis. 2003, 35, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Abbo, L.M.; Hooton, T.M. Antimicrobial stewardship and urinary tract infections. Antibiotics 2014, 3, 174–192. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Davila, M.J. Role of old antibiotics in the era of antibiotic resistance. Highlighted nitrofurantoin for the treatment of lower urinary tract infections. Antibiotics 2014, 3, 39–48. [Google Scholar] [CrossRef]
- Cohen-Nahum, K.; Saidel-Odes, L.; Riesenberg, K.; Schlaeffer, F.; Borer, A. Urinary tract infections caused by multi-drug resistant Proteus mirabilis: Risk factors and clinical outcomes. Infection 2010, 38, 41–46. [Google Scholar] [CrossRef]
- Yeika, E.V.; Foryoung, J.B.; Efie, D.T.; Nkwetateba, E.A.; Tolefac, P.N.; Ngowe, M.N. Multidrug resistant Proteus mirabilis and Escherichia coli causing fulminant necrotising fasciitis: A case report. BMC Res. Notes 2018, 11, 322. [Google Scholar] [CrossRef]
- Wagenlehner, F.; Tandogdu, Z.; Bartoletti, R.; Cai, T.; Cek, M.; Kulchavenya, E.; Köves, B.; Naber, K.; Perepanova, T.; Tenke, P.; et al. The global prevalence of infections in urology study: A long-term, worldwide surveillance study on urological infections. Pathogens 2016, 5, 10. [Google Scholar] [CrossRef]
- Gajdács, M.; Dóczi, I.; Ábrók, M.; Lázár, A.; Burián, K. Epidemiology of candiduria and Candida urinary tract infections in inpatients and outpatients: Results from a 10-year retrospective survey. Cent. Eur. J. Urol. 2019, 72, 209–214. [Google Scholar]
- Gajdács, M.; Urbán, E. Resistance trends and epidemiology of citrobacter-enterobacter-serratia in urinary tract infections of inpatients and outpatients (RECESUTI): A 10-year survey. Medicina 2019, 55, 285. [Google Scholar] [CrossRef]
- Rank, E.L.; Lodise, T.; Avery, L.; Bankert, E.; Dobson, E.; Dumyati, G.; Hassett, S.; Keller, M.; Pearsall, M.; Lubowski, T.; et al. Antimicrobial susceptibility trends observed in urinary pathogens obtained from New York State. Open Forum Infect. Dis. 2018, 5, ofy297. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M.; Spengler, G.; Urbán, E. Identification and antimicrobial susceptibility testing of anaerobic bacteria: Rubik’s cube of clinical microbiology? Antibiotics 2017, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.I.; Kim, J.; Park, D.W.; Kim, B.N.; Ha, U.S.; Lee, S.J.; Yeo, J.K.; Min, S.K.; Lee, H.; Wie, S.H. Clinical practice guidelines for the antibiotic treatment of community-acquired urinary tract infections. Infect. Chemother. 2018, 50, 67–100. [Google Scholar] [CrossRef] [PubMed]
- Moehring, R.W.; Hazen, K.C.; Hawkins, M.R.; Drew, R.H.; Sexton, D.J.; Anderson, D.J. Challenges in preparation of cumulative antibiogram reports for community hospitals. J. Clin. Microbiol. 2015, 53, 2977–2982. [Google Scholar] [CrossRef] [PubMed]
- Abbott, I.J.; Meletiadis, J.; Belghanch, I.; Wijma, R.A.; Kanioura, L.; Roberts, J.A.; Peleg, A.Y.; Mouton, J.W. Fosfomycin efficacy and emergence of resistance among Enterobacteriaceae in an in vitro dynamic bladder infection model. J. Antimicrob. Chemother. 2018, 73, 709–719. [Google Scholar] [CrossRef]
- Stewardson, A.J.; Vervoort, J.; Adriaenssens, N.; Coenen, S.; Godycki-Cwirko, M.; Kowalczyk, A.; Huttner, B.D.; Lammens, C.; Malhotra-Kumar, S.; Goossens, H.; et al. Effect of outpatient antibiotics for urinary tract infections on antimicrobial resistance among commensal Enterobacteriaceae: A multinational prospective cohort study. Clin. Microbiol. Infect. 2018, 24, 972–979. [Google Scholar] [CrossRef]
- Trautner, B.W. Fluoroquinolones for urinary tract infection and within-household spread of resistant Enterobacteriaceae: The smoking gun. Clin. Microbiol. Infect. 2018, 24, 929–930. [Google Scholar] [CrossRef]
- Catry, B.; Latour, K.; Bruyndonckx, R.; Diba, C.; Geerdens, C.; Coenen, S. Characteristics of the antibiotic regimen that affect antimicrobial resistance in urinary pathogens. Antimicrob. Resist. Infect. Control 2018, 7, 76. [Google Scholar] [CrossRef]
- Latour, K.; Jans, B.; Coenen, S.; Preal, R.; Catry, B. Antibiograms of consecutive urinary tract samples in elderly. Antimicrob. Resist. Infect. Control 2013, 2, P22. [Google Scholar] [CrossRef]
- Owumi, W.; Banaei, N.; Shortliffe, L.D. Adult and pediatric intra-institutional trends of ciprofloxacin susceptibility in E. coli positive urinary cultures. Antibiotics 2014, 3, 163–173. [Google Scholar] [CrossRef]
- Adriaenssens, N.; Coenen, S.; Versporten, A.; Muller, A.; Vankerckhoven, V.; Goossens, H.; ESAC Project Group. European surveillance of antimicrobial consumption (ESAC): Quality appraisal of antibiotic use in Europe. J. Antimicrob. Chemother. 2011, 66 (Suppl. 6), vi71–vi77. [Google Scholar] [CrossRef] [PubMed]
- Elseviers, M.M.; Ferech, M.; Vander Stichele, R.H.; Goossens, H.; ESAC Project Group. Antibiotic use in ambulatory care in Europe (ESAC data 1997–2002): Trends, regional differences and seasonal fluctuations. Pharmacoepidemiol. Drug Saf. 2007, 16, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Kong, K.-F.; Schneper, L.; Mathee, K. Beta-lactam antibiotics: From antibiosis to resistance and bacteriology. APMIS 2010, 118, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Rupp, M.E.; Fey, P.D. Extended spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae: Considerations for diagnosis, prevention and drug treatment. Drugs 2003, 63, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Cantón, R.; González-Alba, J.M.; Galán, J.C. CTX-M enzymes: Origin and diffusion. Front. Microbiol. 2012, 3, 110. [Google Scholar] [CrossRef] [PubMed]
- Neuwirth, C.; Siébor, E.; Duez, J.M.; Péchinot, A.; Kazmierczak, A. Imipenem resistance in clinical isolates of Proteus mirabilis associated with alterations in penicillin-binding proteins. J. Antimicrob. Chemother. 1995, 36, 335–342. [Google Scholar] [CrossRef]
- National Health Insurance Fund of Hungary. Hospital Bed Count and Patient Turnover Report 2017; National Health Insurance Fund of Hungary: Budapest, Hungary, 2017. [Google Scholar]
- Gajdács, M.; Urbán, E. Epidemiological trends and resistance associated with Stenotrophomonas maltophilia bacteremia: A 10-year retrospective cohort study in a tertiary-care hospital in Hungary. Diseases 2019, 7, 41. [Google Scholar] [CrossRef]
- Ábrók, M.; Lázár, A.; Szécsényi, M.; Deák, J.; Urbán, E. Combination of MALDI-TOF MS and PBP2’ latex agglutination assay for rapid MRSA detection. J. Microbiol. Methods 2018, 144, 122–124. [Google Scholar] [CrossRef]
- Benkő, R.; Matuz, M.; Hajdú, E.; Bor, A.; Doró, P.; Viola, R.; Soós, G. [Antibiotic use in the Hungarian hospitals in the last two decades (1996–2015)]. ORVOSI HETILAP 2016, 157, 1839–1846. [Google Scholar] [CrossRef]
- Juhász, Z.; Benkő, R.; Matuz, M.; Viola, R.; Soós, G.; Hajdú, E. [Treatment practice of acute cystitis on the basis of national prescription data]. ORVOSI HETILAP 2014, 155, 590–596. [Google Scholar] [CrossRef]
- Matuz, M.; Benkő, R.; Hajdú, E.; Viola, R.; Soós, G. [Evaluation of ambulatory antibiotic use in Hungary using drug-specific quality indicators]. ORVOSI HETILAP 2013, 154, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M.; Paulik, E.; Szabó, A. [The attitude of community pharmacists towards their widening roles in the prevention and treatment of infectious diseases in the southeast region of Hungary] (article in Hungarian). Gyógyszerészet 2019, 63, 26–30. [Google Scholar]
- Gajdács, M.; Ábrók, M.; Lázár, A.; Burián, K. [Susceptibility patterns of extended-spectrum beta-lactamase-producing (ESBL) urinary pathogens: Single-center experience.] (article in Hungarian). Gyógyszerészet 2019, in press. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Isolated co-pathogen | Setting | Proteus spp. | Morganella spp. |
|---|---|---|---|
| Escherichia coli | Inpatient | 41 | 5 |
| Outpatient | 29 | 3 | |
| Enterococcus faecalis | Inpatient | 31 | 3 |
| Outpatient | 22 | 2 | |
| Klebsiella pneumoniae | Inpatient | 23 | 1 |
| Outpatient | 7 | 2 | |
| Pseudomonas aeruginosa | Inpatient | 8 | 0 |
| Outpatient | 9 | 0 | |
| Enterobacter aerogenes | Inpatient | 2 | 0 |
| Outpatient | 2 | 0 | |
| Candida albicans | Inpatient | 0 | 0 |
| Outpatient | 2 | 0 | |
| Acinetobacter baumannii | Inpatient | 0 | 0 |
| Outpatient | 0 | 1 |
| Study Period | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | Statistics | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AMC R (%) b | Outpatient | 12.16 | 17.57 | 31.08 | 60.81 | 28.38 | 37.84 | 63.51 | 66.22 | 75.68 | 62.16 | n.s. (p = 0.499) |
| Inpatient | 32.35 | 37.50 | 47.17 | 59.74 | 56.08 | 63.23 | 54.44 | 56.56 | 53.13 | 49.03 | ||
| CRO R (%) | Outpatient | 4.05 | 4.11 | 11.94 | 27.72 | 31.58 | 38.14 | 25.41 | 26.15 | 17.76 | 24.10 | P = 0.0071 |
| Inpatient | 16.18 | 23.21 | 33.02 | 48.70 | 47.30 | 47.10 | 41.42 | 40.27 | 33.75 | 30.97 | ||
| GEN R (%) | Outpatient | 10.81 | 13.70 | 20.90 | 10.89 | 10.53 | 11.34 | 15.57 | 18.46 | 15.79 | 17.47 | n.s. (p = 0.32) |
| Inpatient | 16.18 | 14.29 | 16.04 | 11.69 | 20.27 | 14.19 | 10.06 | 23.53 | 18.75 | 18.06 | ||
| CIP R (%) | Outpatient | 8.11 | 10.96 | 11.94 | 23.76 | 30.26 | 18.56 | 27.05 | 37.69 | 26.97 | 37.35 | P < 0.0001 |
| Inpatient | 35.29 | 26.79 | 45.28 | 62.34 | 56.76 | 50.97 | 52.07 | 43.89 | 44.38 | 40.00 | ||
| SXT R (%) | Outpatient | 28.38 | 35.62 | 32.84 | 45.54 | 50.00 | 38.14 | 59.02 | 59.23 | 57.24 | 57.23 | P = 0.0025 |
| Inpatient | 55.88 | 50.00 | 50.94 | 74.68 | 68.24 | 61.94 | 66.27 | 64.71 | 62.50 | 65.16 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gajdács, M.; Urbán, E. Comparative Epidemiology and Resistance Trends of Proteae in Urinary Tract Infections of Inpatients and Outpatients: A 10-Year Retrospective Study. Antibiotics 2019, 8, 91. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8030091
Gajdács M, Urbán E. Comparative Epidemiology and Resistance Trends of Proteae in Urinary Tract Infections of Inpatients and Outpatients: A 10-Year Retrospective Study. Antibiotics. 2019; 8(3):91. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8030091
Chicago/Turabian StyleGajdács, Márió, and Edit Urbán. 2019. "Comparative Epidemiology and Resistance Trends of Proteae in Urinary Tract Infections of Inpatients and Outpatients: A 10-Year Retrospective Study" Antibiotics 8, no. 3: 91. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8030091