Er,Cr:YSGG Laser-Activation Enhances Antimicrobial and Antibiofilm Action of Low Concentrations of Sodium Hypochlorite in Root Canals

 , and
, and
Abstract
:1. Introduction
2. Results
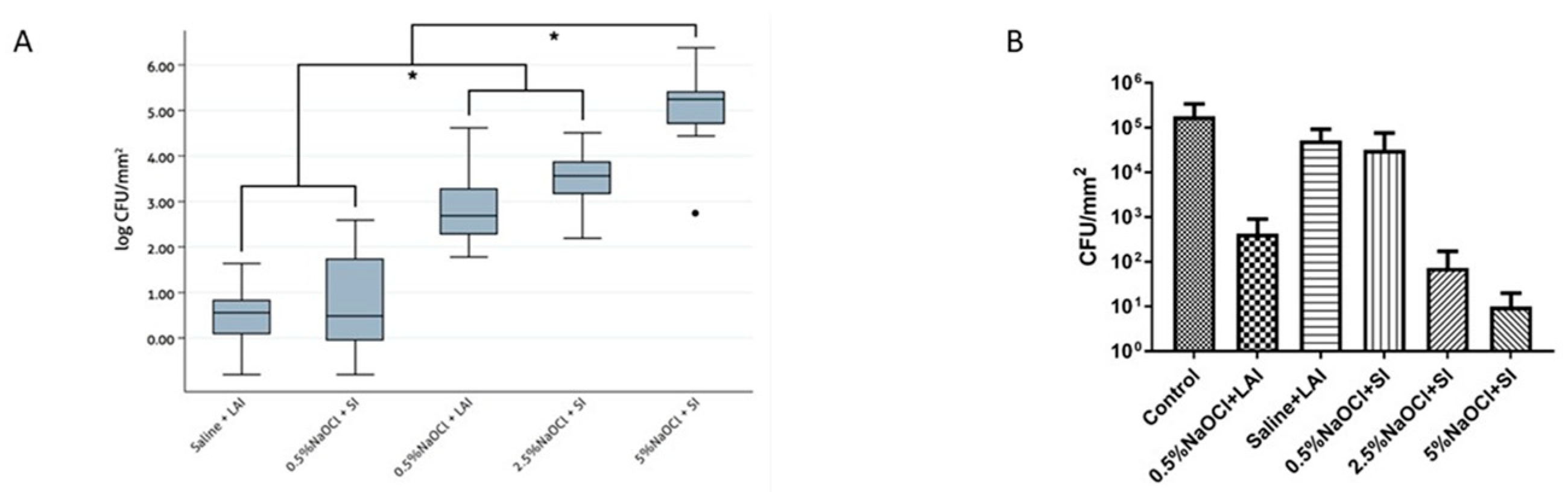
2.1. Bacterial Elimination
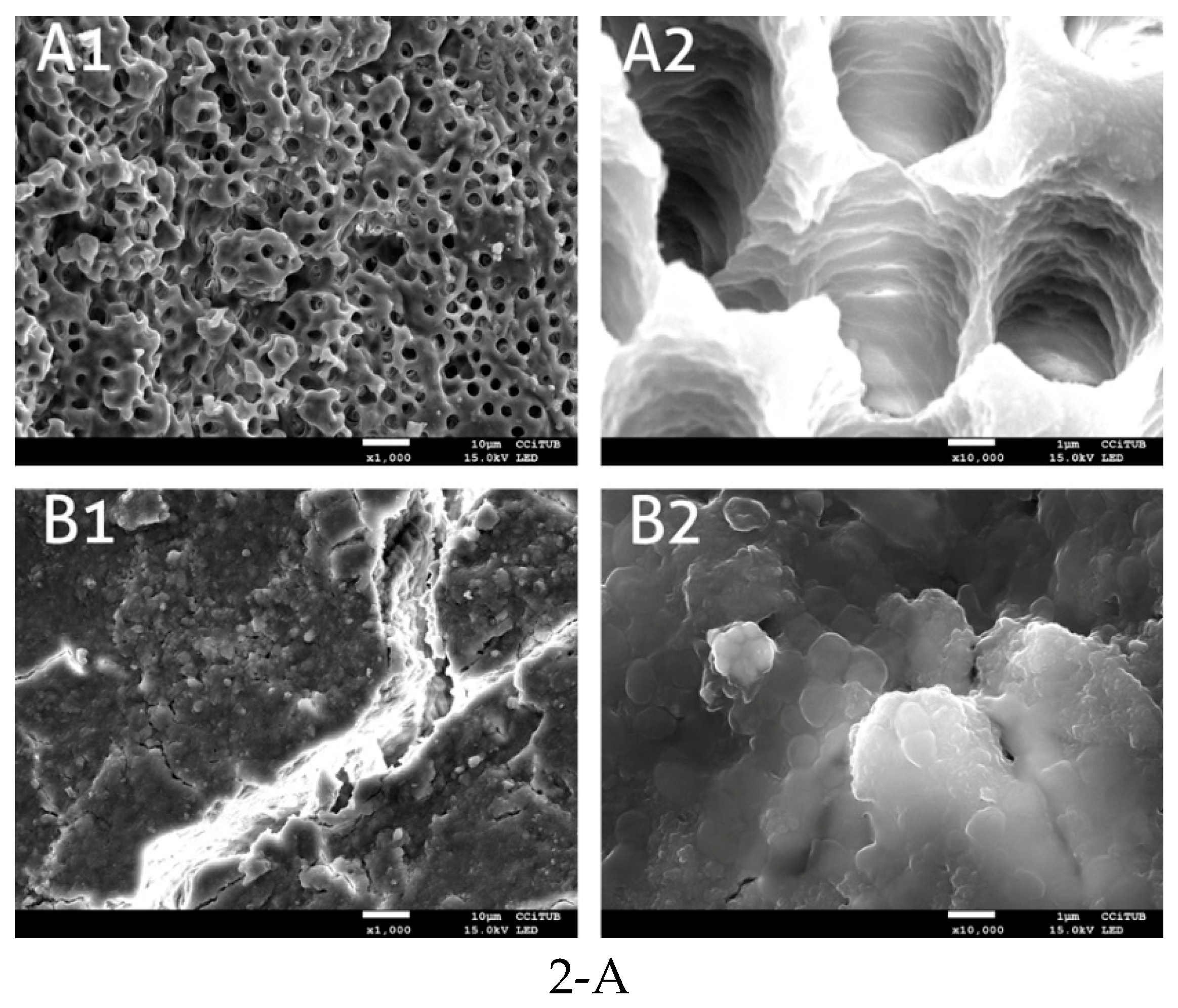
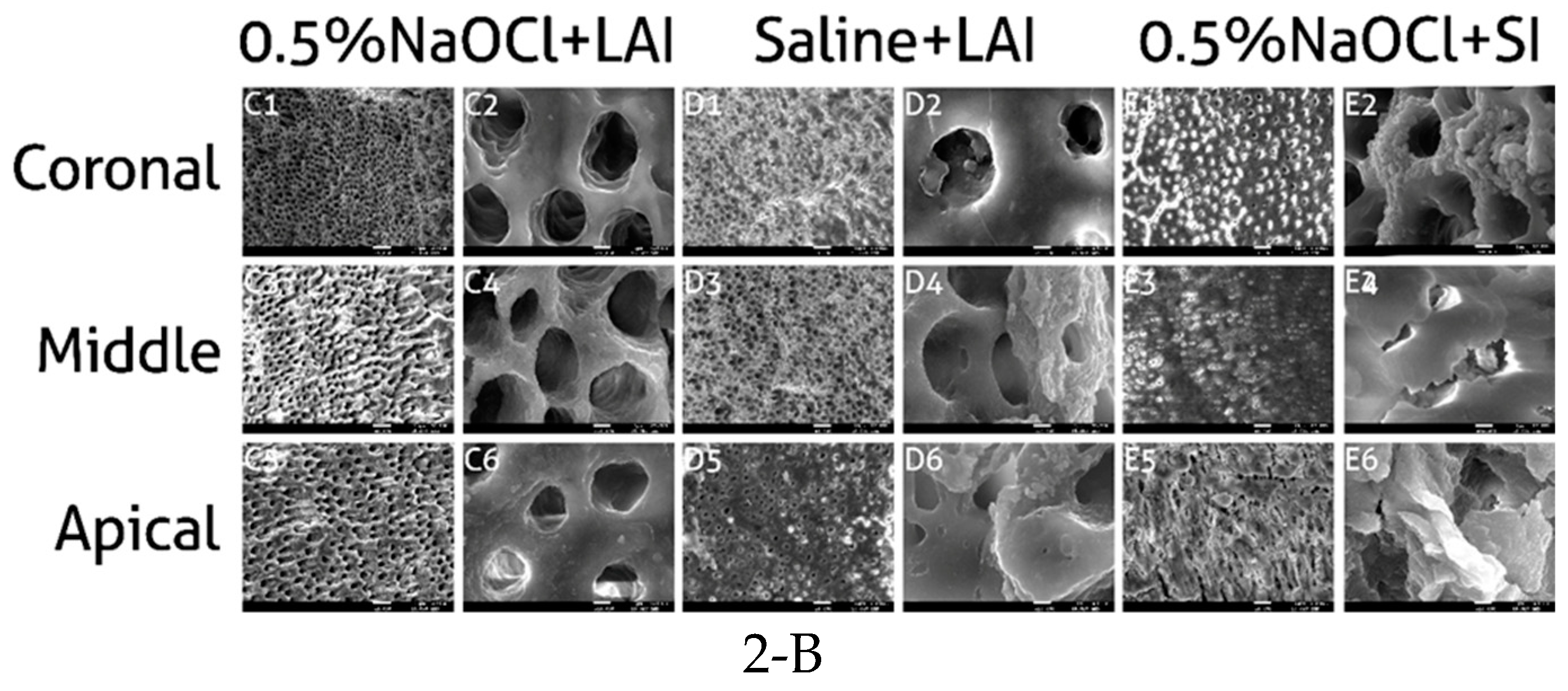
2.2. Scanning Electron Microscopy (SEM)
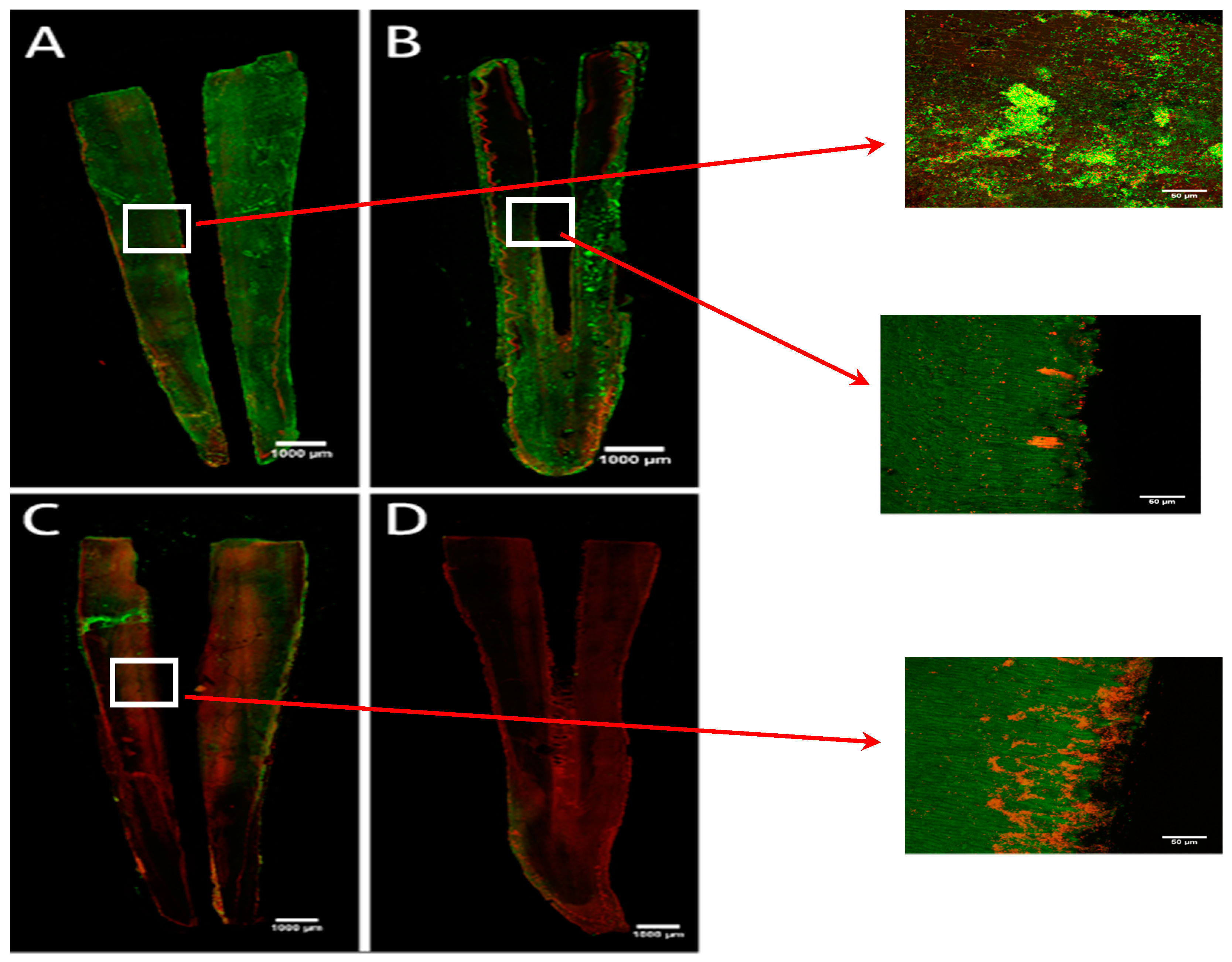
2.3. Confocal Laser Scaning Microscopy (CLSM)
3. Discussion
4. Materials and Methods
4.1. Specimens
4.2. Enterococcus Faecalis Biofilm Formation
4.3. Experimental Procedures
4.4. Bacterial Count
4.5. Scanning Electron Microscopy (SEM)
4.6. CLSM
4.7. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Ohsumi, T.; Takenaka, S.; Wakamatsu, R.; Sakaue, Y.; Narisawa, N.; Senpuku, H.; Ohshima, H.; Terao, Y.; Okiji, T. Residual structure of Streptococcus mutans biofilm following complete disinfection favors secondary bacterial adhesion and biofilm re-development. PLoS ONE 2015, 10, e0116647. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.; Tsesis, I.; Elbahary, S.; Storzi, N.; Kolodkin-Gal, I. Eradication of Enterococcus faecalis biofilms on human dentin. Front. Microbiol. 2016, 7, 2055. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.; Phillips, C. The ecology, epidemiology and virulence of Enterococcus. Microbiology 2009, 155, 1749–1757. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, L.; Shlezinger, M.; Beyth, S.; Houri-Haddad, Y.; Coppenhagen-Glazer, S.; Beyth, N.; Hazan, R. Phage therapy against Enterococcus faecalis in dental root canals. J. Oral Microbiol. 2016, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Donlan, R.M.; Costerton, J.W. Biofilms: Survival mechanisms of clinically relevant microorgansims. Clin. Microbiol. Rev. 2002, 15, 167–193. [Google Scholar] [CrossRef] [PubMed]
- Distel, J.W.; Hatton, J.F.; Gillespie, M.J. Biofilm formation in medicated root canals. J. Endod. 2002, 28, 689–693. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Lambrianidis, T.; Kastrinakis, E. Irrigant flow within a prepared root canal using various flow rates: A Computational Fluid Dynamics study. Int. Endod. J. 2009, 42, 144–155. [Google Scholar] [CrossRef]
- Falk, K.W.; Sedgley, C.M. The influence of preparation size on the mechanical efficacy of root canal irrigation in vitro. J. Endod. 2005, 31, 742–745. [Google Scholar] [CrossRef]
- Betancourt, P.; Merlos, A.; Sierra, J.M.; Arnabat-Dominguez, J.; Viñas, M. Er,Cr:YSGG Laser-Activated Irrigation and Passive Ultrasonic Irrigation: Comparison of Two Strategies for Root Canal Disinfection. Photobiomodul. Photomed. Laser Surg. 2019. [Google Scholar] [CrossRef]
- Blanken, J.; Verdaasdonk, R. Cavitation as a working mechanism of the Er, Cr: YSGG laser in endodontics: A visualization study. J. Oral Laser Appl. 2007, 7, 97–106. [Google Scholar]
- George, R.; Meyers, I.A.; Walsh, L.J. Laser Activation of Endodontic Irrigants with Improved Conical Laser Fiber Tips for Removing Smear Layer in the Apical Third of the Root Canal. J. Endod. 2008, 34, 1524–1527. [Google Scholar] [CrossRef] [PubMed]
- Blanken, J.; De Moor, R.J.G.; Meire, M.; Verdaasdonk, R. Laser induced explosive vapor and cavitation resulting in effective irrigation of the root canal. Part 1: A visualization study. Lasers Surg. Med. 2009, 41, 514–519. [Google Scholar] [CrossRef] [PubMed]
- De Groot, S.D.; Verhaagen, B.; Versluis, M.; Wu, M.K.; Wesselink, P.R.; Van Der Sluis, L.W.M. Laser-activated irrigation within root canals: Cleaning efficacy and flow visualization. Int. Endod. J. 2009, 42, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Tian, T.; Tian, Y.; Xiang, D.; Qiu, J.; Liu, X.; Yu, Q. Erbium:Yttrium Aluminum Garnet Laser-Activated Sodium Hypochlorite Irrigation: A Promising Procedure for Minimally Invasive Endodontics. Photomed. Laser Surg. 2017, 35, 695–701. [Google Scholar] [CrossRef]
- DiVito, E.; Peters, O.A.; Olivi, G. Effectiveness of the erbium: YAG laser and new design radial and stripped tips in removing the smear layer after root canal instrumentation. Lasers Med. Sci. 2012, 27, 273–280. [Google Scholar] [CrossRef]
- Cullen, J.K.T.; Wealleans, J.A.; Kirkpatrick, T.C.; Yaccino, J.M. The effect of 8.25% sodium hypochlorite on dental pulp dissolution and dentin flexural strength and modulus. J. Endod. 2015, 41, 920–924. [Google Scholar] [CrossRef]
- Zhang, W.; Torabinejad, M.; Li, Y. Evaluation of cytotoxicity of MTAD using the MTT- tetrazolium method. J. Endod. 2003, 29, 654–657. [Google Scholar] [CrossRef]
- Zhu, W.C.; Gyamfi, J.; Niu, L.N.; Schieffel, G.J.; Liu, S.Y.; Santarcangelo, F.; Khan, S.; Tay, K.C.; Pashley, D.H.; Tay, F.R. Anatomy of sodium hypochlorite accidents involving facial ecchymosis—A review. J. Dent. 2013, 41, 935–948. [Google Scholar] [CrossRef]
- Betancourt, P.; Merlos, A.; Sierra, J.M.; Camps-Font, O.; Arnabat-Dominguez, J.; Viñas, M. Effectiveness of low concentration of sodium hypochlorite activated by Er,Cr:YSGG laser against Enterococcus faecalis biofilm. Lasers Med. Sci. 2019, 34, 247–254. [Google Scholar] [CrossRef]
- Licata, M.E.; Albanese, A.; Campisi, G.; Geraci, D.M.; Russo, R.; Gallina, G. Effectiveness of a new method of disinfecting the root canal, using Er, Cr:YSGG laser to kill Enterococcus faecalis in an infected tooth model. Lasers Med. Sci. 2015, 30, 707–712. [Google Scholar] [CrossRef]
- Yavari, H.R.; Rahimi, S.; Shahi, S.; Lotfi, M.; Barhaghi, M.H.; Fatemi, A.; Abdolrahimi, M. Effect of Er, Cr: YSGG Laser Irradiation on Enterococcus faecalis in Infected Root Canals. Photomed. Laser Surg. 2010, 28, S91–S96. [Google Scholar] [CrossRef] [PubMed]
- Bago Jurič, I.; Plečko, V.; Anić, I. Antimicrobial Efficacy of Er,Cr:YSGG Laser-Activated Irrigation Compared with Passive Ultrasonic Irrigation and RinsEndo ® Against Intracanal Enterococcus faecalis. Photomed. Laser Surg. 2014, 32, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Mohmmed, S.A.; Vianna, M.E.; Penny, M.R.; Hilton, S.T.; Mordan, N.; Knowles, J.C. Confocal laser scanning, scanning electron, and transmission electron microscopy investigation of Enterococcus faecalis biofilm degradation using passive and active sodium hypochlorite irrigation within a simulated root canal model. Microbiologyopen 2017, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Radcliffe, C.E.; Potouridou, L.; Qureshi, R.; Habahbeh, N.; Qualtrough, A.; Worthington, H.; Drucker, D.B. Antimicrobial activity of varying concentrations of sodium hypochlorite on the endodontic microorganisms Actinomyces israelii, A. naeslundii, Candida albicans and Enterococcus faecalis. Int. Endod. J. 2004, 37, 438–446. [Google Scholar] [CrossRef]
- Patini, R.; Cattani, P.; Marchetti, S.; Isola, G.; Quaranta, G.; Gallenzi, P. Evaluation of Predation Capability of Periodontopathogens Bacteria by Bdellovibrio Bacteriovorus HD100. An in Vitro Study. Materials 2019, 12, 2008. [Google Scholar] [CrossRef]
- Eneide, C.; Castagnola, R.; Martini, C.; Grande, N.M.; Bugli, F.; Patini, R.; Cordaro, M.; Sanguinetti, M.; Olivi, G.; Isola, G.; et al. Antibiofilm Activity of Three Different Irrigation Techniques: An in Vitro Study. Antibiotics 2019, 8, 112. [Google Scholar] [CrossRef]
- Cheng, X.; Xiang, D.; He, W.; Qiu, J.; Han, B.; Yu, Q.; Tian, Y. Bactericidal Effect of Er:YAG Laser-Activated Sodium Hypochlorite Irrigation Against Biofilms of Enterococcus faecalis Isolate from Canal of Root-Filled Teeth with Periapical Lesions. Photomed. Laser Surg. 2017, 35, 386–392. [Google Scholar] [CrossRef]
- Macedo, R.G.; Wesselink, P.R.; Zaccheo, F.; Fanali, D.; Van Der Sluis, L.W.M. Reaction rate of NaOCl in contact with bovine dentine: Effect of activation, exposure time, concentration and pH. Int. Endod. J. 2010, 43, 1108–1115. [Google Scholar] [CrossRef]
- Souza, M.A.; Tumelero Dias, C.; Zandoná, J.; Paim Hoffmann, I.; Sanches Menchik, V.H.; Palhano, H.S.; Bertol, C.D.; Rossato-Grando, L.G.; Cecchin, D.; de Figueiredo, J.A.P. Antimicrobial activity of hypochlorite solutions and reciprocating instrumentation associated with photodynamic therapy on root canals infected with Enterococcus faecalis – An in vitro study. Photodiagn. Photodyn. 2018, 23, 347–352. [Google Scholar] [CrossRef]
- Jaramillo, D.E.; Aguilar, E.; Arias, A.; Ordinola-Zapata, R.; Aprecio, R.M.; Ibarrola, J.L. Root canal disinfection comparing conventional irrigation vs photon-induced photoacoustic streaming (PIPS) using a buffered 0.5 % sodium hypochlorite solution. Evid.-Based Endod. 2016. [Google Scholar] [CrossRef]
- Christo, J.E.; Zilm, P.S.; Sullivan, T.; Cathro, P.R. Efficacy of low concentrations of sodium hypochlorite and low-powered Er,Cr: YSGG laser activated irrigation against an Enterococcus faecalis biofilm. Int. Endod. J. 2016, 49, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Peeters, H.H.; De Moor, R.J.G. Measurement of pressure changes during laser-activated irrigant by an erbium, chromium: Yttrium, scandium, gallium, garnet laser. Lasers Med. Sci. 2015, 30, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Peeters, H.H.; Suardita, K.; Mooduto, L.; Gutknecht, N. Extrusion of irrigant in open apex teeth with periapical lesions following laser-activated irrigation and passive ultrasonic irrigation. Iran. Endod. J. 2018, 13, 169–175. [Google Scholar]
- Yamada, M.K.; Uo, M.; Ohkawa, S.; Akasaka, T.; Watari, F. Three-dimensional topographic scanning electron microscope and Raman spectroscopic analyses of the irradiation effect on teeth by Nd:YAG, Er:YAG, and CO2 lasers. J. Biomed. Mater. Res.- Part B Appl. Biomater. 2004, 71, 7–15. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Treatment | 0.5% NaOCl + LAI | Saline + LAI | 0.5% NaOCl + SI | 2.5% NaOCl + SI |
|---|---|---|---|---|---|
| 1 | 0.5% NaOCl + LAI | ||||
| 2 | Saline + LAI | <0.001 | |||
| 3 | 0.5% NaOCl + SI | <0.001 | 0.999 | ||
| 4 | 2.5% NaOCl + SI | 0.3167 | <0.001 | <0.001 | |
| 5 | 5.0% NaOCl + SI | <0.001 | <0.001 | <0.001 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Betancourt, P.; Sierra, J.M.; Camps-Font, O.; Arnabat-Domínguez, J.; Viñas, M. Er,Cr:YSGG Laser-Activation Enhances Antimicrobial and Antibiofilm Action of Low Concentrations of Sodium Hypochlorite in Root Canals. Antibiotics 2019, 8, 232. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8040232
Betancourt P, Sierra JM, Camps-Font O, Arnabat-Domínguez J, Viñas M. Er,Cr:YSGG Laser-Activation Enhances Antimicrobial and Antibiofilm Action of Low Concentrations of Sodium Hypochlorite in Root Canals. Antibiotics. 2019; 8(4):232. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8040232
Chicago/Turabian StyleBetancourt, Pablo, Josep María Sierra, Octavi Camps-Font, Josep Arnabat-Domínguez, and Miguel Viñas. 2019. "Er,Cr:YSGG Laser-Activation Enhances Antimicrobial and Antibiofilm Action of Low Concentrations of Sodium Hypochlorite in Root Canals" Antibiotics 8, no. 4: 232. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8040232