Antibiotic Susceptibility Patterns of Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis Strains from Different Decades

 , , and
, , and
Abstract
:1. Introduction
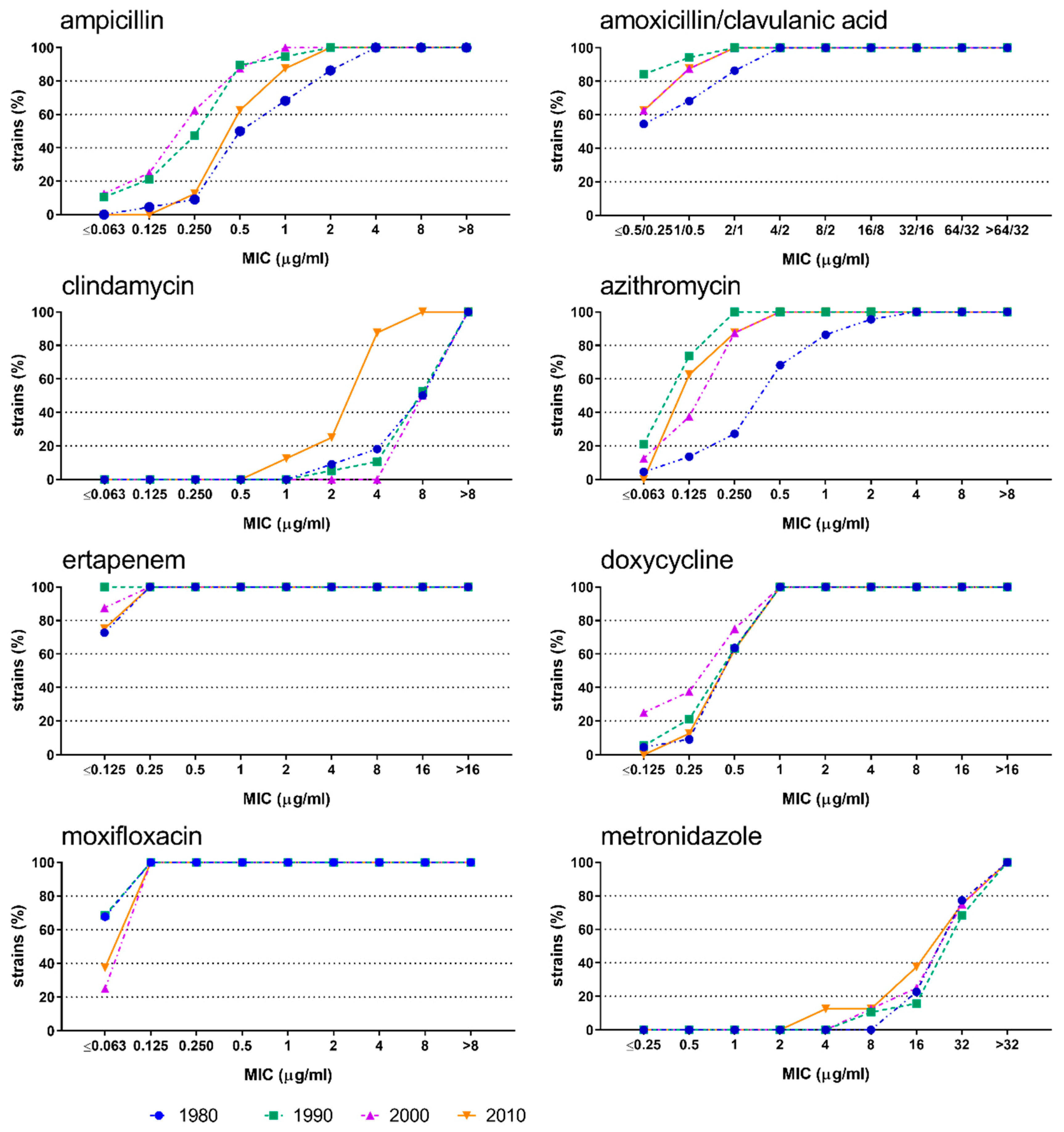
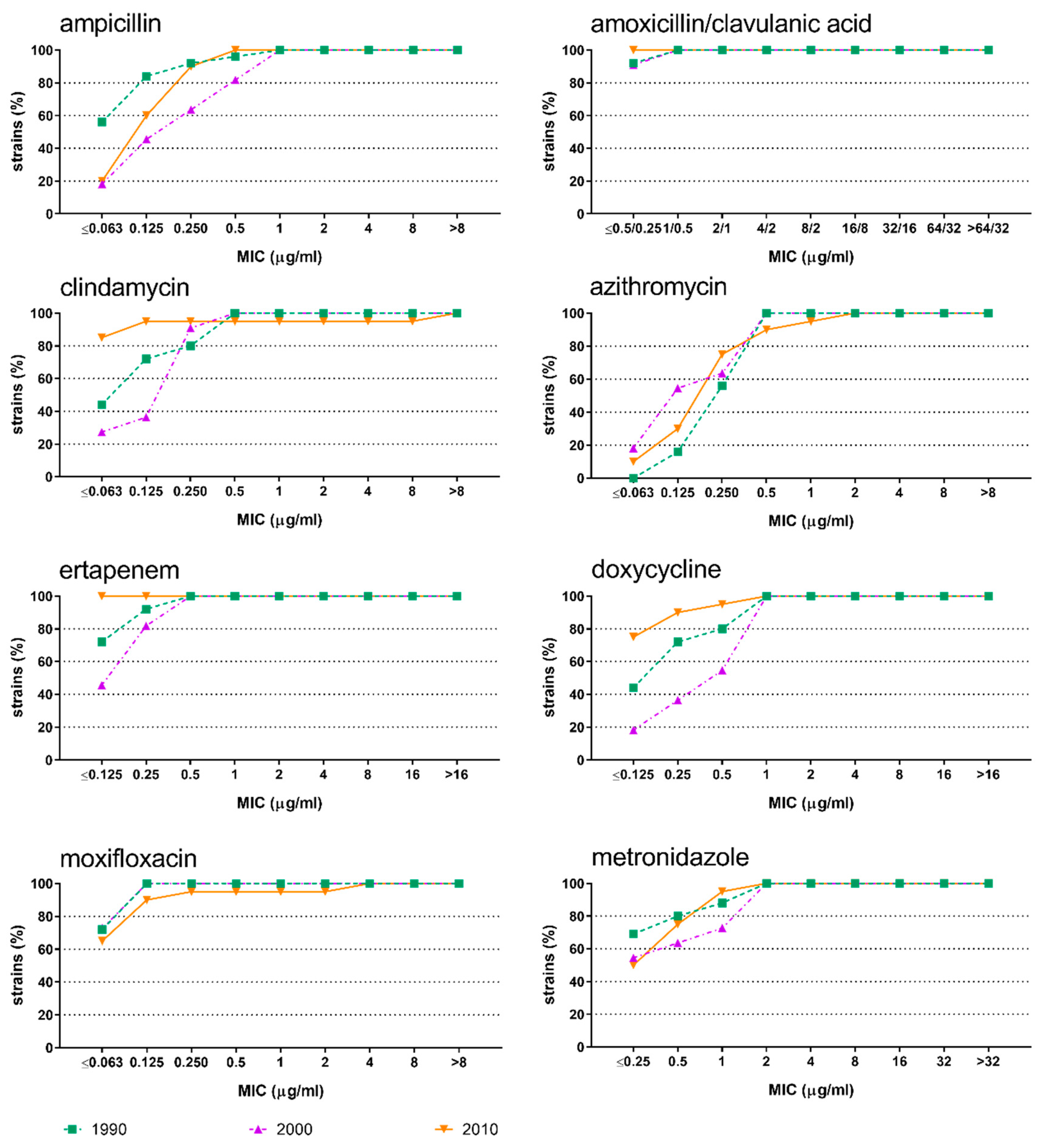
2. Results
3. Discussion
4. Materials and Methods
4.1. Isolation of Bacteria
4.2. Determination of the Minimal Inhibitory Concentration (MIC) and Resistance Testing
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Durand, G.A.; Raoult, D.; Dubourg, G. Antibiotic discovery: History, methods and perspectives. Int. J. Antimicrob. Agents 2019, 53, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Plüss-Suard, C.; Pannatier, A.; Kronenberg, A.; Muhlemann, K.; Zanetti, G. Hospital antibiotic consumption in Switzerland: Comparison of a multicultural country with Europe. J. Hosp. Infect. 2011, 79, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.A.; Laxminarayan, R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- Glinz, D.; Leon Reyes, S.; Saccilotto, R.; Widmer, A.F.; Zeller, A.; Bucher, H.C.; Hemkens, L.G. Quality of antibiotic prescribing of Swiss primary care physicians with high prescription rates: A nationwide survey. J. Antimicrob. Chemother. 2017, 72, 3205–3212. [Google Scholar] [CrossRef] [PubMed]
- Roope, L.S.J.; Smith, R.D.; Pouwels, K.B.; Buchanan, J.; Abel, L.; Eibich, P.; Butler, C.C.; Tan, P.S.; Walker, A.S.; Robotham, J.V.; et al. The challenge of antimicrobial resistance: What economics can contribute. Science 2019, 364, eaau4679. [Google Scholar] [CrossRef] [PubMed]
- Allcock, S.; Young, E.H.; Holmes, M.; Gurdasani, D.; Dougan, G.; Sandhu, M.S.; Solomon, L.; Torok, M.E. Antimicrobial resistance in human populations: Challenges and opportunities. Glob. Health Epidemiol. Genom. 2017, 2, e4. [Google Scholar] [CrossRef] [Green Version]
- Durkin, M.J.; Hsueh, K.; Sallah, Y.H.; Feng, Q.; Jafarzadeh, S.R.; Munshi, K.D.; Lockhart, P.B.; Thornhill, M.H.; Henderson, R.R.; Fraser, V.J. An evaluation of dental antibiotic prescribing practices in the United States. J. Am. Dent. Assoc. 2017, 148, 878–886.e871. [Google Scholar] [CrossRef] [Green Version]
- Rescala, B.; Rosalem, W., Jr.; Teles, R.P.; Fischer, R.G.; Haffajee, A.D.; Socransky, S.S.; Gustafsson, A.; Figueredo, C.M. Immunologic and microbiologic profiles of chronic and aggressive periodontitis subjects. J. Periodontol. 2010, 81, 1308–1316. [Google Scholar] [CrossRef]
- Herbert, B.A.; Novince, C.M.; Kirkwood, K.L. Aggregatibacter actinomycetemcomitans, a potent immunoregulator of the periodontal host defense system and alveolar bone homeostasis. Mol. Oral. Microbiol. 2016, 31, 207–227. [Google Scholar] [CrossRef] [Green Version]
- Zenobia, C.; Hajishengallis, G. Porphyromonas gingivalis virulence factors involved in subversion of leukocytes and microbial dysbiosis. Virulence 2015, 6, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Keestra, J.A.; Grosjean, I.; Coucke, W.; Quirynen, M.; Teughels, W. Non-surgical periodontal therapy with systemic antibiotics in patients with untreated chronic periodontitis: A systematic review and meta-analysis. J. Periodontal. Res. 2015, 50, 294–314. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; Modarai, M.; Naylor, N.R.; Boyd, S.E.; Atun, R.; Barlow, J.; Holmes, A.H.; Johnson, A.; Robotham, J.V. Quantifying drivers of antibiotic resistance in humans: A systematic review. Lancet Infect. Dis. 2018, 18, e368–e378. [Google Scholar] [CrossRef] [Green Version]
- Eick, S.; Schmitt, A.; Sachse, S.; Schmidt, K.H.; Pfister, W. In vitro antibacterial activity of fluoroquinolones against Porphyromonas gingivalis strains. J. Antimicrob. Chemother. 2004, 54, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Kulik, E.M.; Lenkeit, K.; Chenaux, S.; Meyer, J. Antimicrobial susceptibility of periodontopathogenic bacteria. J. Antimicrob. Chemother. 2008, 61, 1087–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köhler, M.; Meyer, J.; Linder, M.; Lambrecht, J.T.; Filippi, A.; Kulik Kunz, E.M. Prescription of antibiotics in the dental practice: A survey of dentists in Switzerland. Schweiz. Monatsschr. Zahnmed. 2013, 123, 748–759. [Google Scholar]
- Johnson, T.M.; Hawkes, J. Awareness of antibiotic prescribing and resistance in primary dental care. Prim. Dent. J. 2014, 3, 44–47. [Google Scholar] [CrossRef]
- Veloo, A.C.; Seme, K.; Raangs, E.; Rurenga, P.; Singadji, Z.; Wekema-Mulder, G.; van Winkelhoff, A.J. Antibiotic susceptibility profiles of oral pathogens. Int. J. Antimicrob. Agents 2012, 40, 450–454. [Google Scholar] [CrossRef]
- Dahlen, G.; Preus, H.R. Low antibiotic resistance among anaerobic Gram-negative bacteria in periodontitis 5 years following metronidazole therapy. Anaerobe 2017, 43, 94–98. [Google Scholar] [CrossRef]
- Rams, T.E.; Degener, J.E.; van Winkelhoff, A.J. Antibiotic resistance in human chronic periodontitis microbiota. J. Periodontol. 2014, 85, 160–169. [Google Scholar] [CrossRef]
- Xie, Y.; Chen, J.; He, J.; Miao, X.; Xu, M.; Wu, X.; Xu, B.; Yu, L.; Zhang, W. Antimicrobial resistance and prevalence of resistance genes of obligate anaerobes isolated from periodontal abscesses. J. Periodontol. 2014, 85, 327–334. [Google Scholar] [CrossRef]
- Al-Ahmad, A.; Ameen, H.; Pelz, K.; Karygianni, L.; Wittmer, A.; Anderson, A.C.; Spitzmuller, B.; Hellwig, E. Antibiotic resistance and capacity for biofilm formation of different bacteria isolated from endodontic infections associated with root-filled teeth. J. Endod. 2014, 40, 223–230. [Google Scholar] [CrossRef]
- Eick, S.; Seltmann, T.; Pfister, W. Efficacy of antibiotics to strains of periodontopathogenic bacteria within a single species biofilm—An in vitro study. J. Clin. Periodontol. 2004, 31, 376–383. [Google Scholar] [CrossRef]
- Kulik Kunz, E.M.; Lenkeit, K.; Waltimo, T.; Weiger, R.; Walter, C. Combinatorial effects of amoxicillin and metronidazole on selected periodontal bacteria and whole plaque samples. Arch. Oral. Biol. 2014, 59, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.L.; Johnston, W.; Delaney, C.; Short, B.; Butcher, M.C.; Young, T.; Butcher, J.; Riggio, M.; Culshaw, S.; Ramage, G. Polymicrobial oral biofilm models: Simplifying the complex. J. Med. Microbiol. 2019, 68, 1573–1584. [Google Scholar] [CrossRef] [PubMed]
- Eick, S.; Pfister, W. Efficacy of antibiotics against periodontopathogenic bacteria within epithelial cells: An in vitro study. J. Periodontol. 2004, 75, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Pitiriga, V.; Vrioni, G.; Saroglou, G.; Tsakris, A. The impact of antibiotic stewardship programs in combating quinolone resistance: A systematic review and recommendations for more efficient interventions. Adv. Ther. 2017, 34, 854–865. [Google Scholar] [CrossRef]
- Eick, S.; Straube, A.; Guentsch, A.; Pfister, W.; Jentsch, H. Comparison of real-time polymerase chain reaction and DNA-strip technology in microbiological evaluation of periodontitis treatment. Diagn. Microbiol. Infect. Dis. 2011, 69, 12–20. [Google Scholar] [CrossRef]
- Tran, C.M.; Tanaka, K.; Watanabe, K. PCR-based detection of resistance genes in anaerobic bacteria isolated from intra-abdominal infections. J. Infect. Chemother. 2013, 19, 279–290. [Google Scholar] [CrossRef]
- EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters. v 9.0.1, 01.01.2019. Available online: http://www.eucast.org/clinical_breakpoints (accessed on 25 October 2019).



{kind=link}
{kind=link}
| Years | A. actinomycetemcomitans | P. gingivalis |
|---|---|---|
| 1980–1989 | 22 | na |
| 1990–1999 | 19 | 25 |
| 2000–2009 | 8 | 11 |
| 2010–2017 | 8 | 20 |
| Antibiotic | A. actinomycetemcomitans | P. gingivalis | ||
|---|---|---|---|---|
| MIC50 | MIC90 | MIC50 | MIC90 | |
| Ampicillin | 0.5 | 2 | 0.125 | 0.5 |
| Amoxicillin/Clavulanic Acid | 0.5/0.25 | 2/1 | 0.5/0.25 | 0.5/0.25 |
| Clindamycin | 8 | >8 | 0.0625 | 0.25 |
| Azithromycin | 0.25 | 1 | 0.250 | 0.5 |
| Ertapenem | 0.125 | 0.25 | 0.125 | 0.25 |
| Doxycycline | 0.5 | 1 | 0.25 | 1 |
| Moxifloxacin | 0.0625 | 0.125 | 0.0625 | 0.125 |
| Metronidazole | 32 | >32 | 0.25 | 2 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kulik, E.M.; Thurnheer, T.; Karygianni, L.; Walter, C.; Sculean, A.; Eick, S. Antibiotic Susceptibility Patterns of Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis Strains from Different Decades. Antibiotics 2019, 8, 253. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8040253
Kulik EM, Thurnheer T, Karygianni L, Walter C, Sculean A, Eick S. Antibiotic Susceptibility Patterns of Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis Strains from Different Decades. Antibiotics. 2019; 8(4):253. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8040253
Chicago/Turabian StyleKulik, Eva M., Thomas Thurnheer, Lamprini Karygianni, Clemens Walter, Anton Sculean, and Sigrun Eick. 2019. "Antibiotic Susceptibility Patterns of Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis Strains from Different Decades" Antibiotics 8, no. 4: 253. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8040253