Commercial Local Pharmacotherapeutics and Adjunctive Agents for Nonsurgical Treatment of Periodontitis: A Contemporary Review of Clinical Efficacies and Challenges




Abstract
:1. Introduction
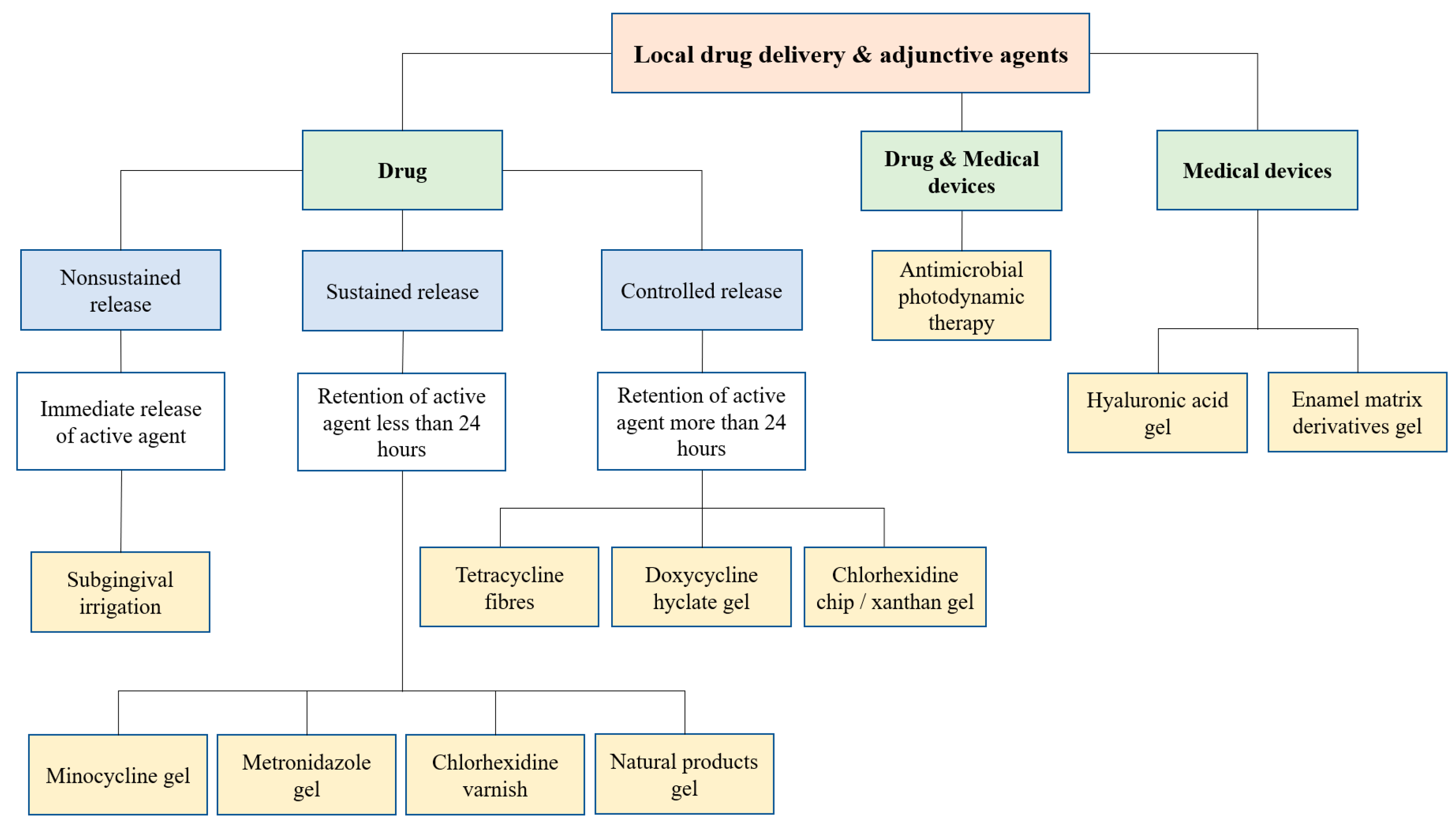
2. Classification of LDA for Nonsurgical Periodontal Therapy
3. Indications for the Use of LDA in Periodontal Treatment
4. Pharmacotherapeutic Agents Used as Local Adjuncts
4.1. Tetracycline
4.2. Doxycycline
4.3. Minocycline
4.4. Chlorhexidine
4.5. Metronidazole
4.6. Povidone–Iodine
4.7. Sodium Hypochlorite
4.8. Natural Products
4.9. EMD
4.10. Hyaluronic Acid
4.11. Antimicrobial Photodynamic Therapy (aPDT)
5. Occurrence of Adverse Effects with Use of LDA
6. Comparison of Clinical Efficacy between Different LDA
7. Use of LDA in Nonsurgical Treatment of Aggressive Periodontitis
8. Challenges of LDA
9. Cost Effectiveness and Patient-Centered Outcomes
10. Limitations
11. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Marsh, P.D.; Bradshaw, D.J. Dental plaque as a biofilm. J. Ind. Microbiol. 1995, 15, 169–175. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Lambris, J.D. Complement and dysbiosis in periodontal disease. Immunobiology 2012, 217, 1111–1116. [Google Scholar] [CrossRef] [Green Version]
- Razali, M.; Palmer, R.M.; Coward, P.; Wilson, R.F. A retrospective study of periodontal disease severity in smokers and non-smokers. Br. Dent. J. 2005, 198, 495–498. [Google Scholar] [CrossRef] [Green Version]
- Baharin, B.; Palmer, R.M.; Coward, P.; Wilson, R.F. Investigation of periodontal destruction patterns in smokers and non-smokers. J. Clin. Periodontol. 2006, 33, 485–490. [Google Scholar] [CrossRef]
- Michalowicz, B.S.; Aeppli, D.; Virag, J.G.; Klump, D.G.; Hinrichs, E.; Segal, N.L.; Bouchard, T.J.; Pihlstrom, B.L. Periodontal Findings in Adult Twins. J. Periodontol. 1991, 62, 293–299. [Google Scholar] [CrossRef]
- Hart, T.C.; Kornman, K.S. Genetic factors in the pathogenesis of periodontitis. Periodontology 2000 1997, 14, 202–215. [Google Scholar] [CrossRef]
- Albandar, J.M.; Susin, C.; Hughes, F.J. Manifestations of systemic diseases and conditions that affect the periodontal attachment apparatus: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45, S171–S189. [Google Scholar] [CrossRef] [Green Version]
- Leong, X.; Ng, C.; Badiah, B.; Das, S. Association between hypertension and periodontitis: Possible mechanisms. Sci. World J. 2014. [Google Scholar] [CrossRef] [Green Version]
- Kornman, K.S. Mapping the Pathogenesis of Periodontitis: A New Look. J. Periodontol. 2008, 79, 1560–1568. [Google Scholar] [CrossRef]
- Durham, J.; Fraser, H.M.; McCracken, G.I.; Stone, K.M.; John, M.T.; Preshaw, P.M. Impact of periodontitis on oral health-related quality of life. J. Dent. 2013, 41, 370–376. [Google Scholar] [CrossRef]
- Petersen, P.E.; Ogawa, H. The global burden of periodontal disease: Towards integration with chronic disease prevention and control. Periodontology 2000 2012, 60, 15–39. [Google Scholar] [CrossRef]
- Collaborators, G. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar]
- Jepsen, K.; Jepsen, S. Antibiotics/antimicrobials: Systemic and local administration in the therapy of mild to moderately advanced periodontitis. Periodontology 2000 2016, 71, 82–112. [Google Scholar] [CrossRef]
- Gatej, S.; Gully, N.; Gibson, R.; Bartold, P.M. Probiotics and Periodontitis—A Literature Review. J. Int. Acad. Periodontol. 2017, 19, 42–50. [Google Scholar]
- Fauzi, A.; Shafiei, Z.; Baharin, B.; Mohd, N. Isolation of lactobacillus from periodontally healthy subjects and its antimicrobial activity against periodontal pathogens. Sains Malays. 2013, 42, 19–24. [Google Scholar]
- Moro, M.G.; Silveira Souto, M.L.; Franco, G.C.N.; Holzhausen, M.; Pannuti, C.M. Efficacy of local phytotherapy in the nonsurgical treatment of periodontal disease: A systematic review. J. Periodontal Res. 2018, 53, 288–297. [Google Scholar] [CrossRef]
- Hamzah, N.; Aziz, S.; Fauzi, A.; Yusof, Y.; Razali, M.; Ibrahim, N.; Baharin, B. Effects of gelam honey (Melaleuca cajuputi) on alveolar bone loss in experimental periodontitis. J. Dent. Surg. 2014. [Google Scholar] [CrossRef]
- Preshaw, P.M. Host modulation therapy with anti-inflammatory agents. Periodontology 2000 2018, 76, 131–149. [Google Scholar] [CrossRef]
- Acute Market Reports Global Periodontal Therapeutics Market Size, Market Share, Application Analysis, Regional Outlook, Growth Trends, Key Players, Competitive Strategies and Forecasts, 2017 to 2025. Available online: https://www.researchandmarkets.com/reports/4431610/global-periodontal-therapeutics-market-size (accessed on 1 December 2018).
- Collaborators, G. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet 2017, 389, 1885–1906. [Google Scholar]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri—Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, 162–170. [Google Scholar] [CrossRef]
- Greenstein, G.; Tonetti, M. The role of controlled drug delivery for periodontitis. The Research, Science and Therapy Committee of the American Academy of Periodontology. J. Periodontol. 2000, 71, 125–140. [Google Scholar]
- Rams, T.E.; Slots, J. Local delivery of antimicrobial agents in the periodontal pocket. Periodontology 2000 1996, 10, 139–159. [Google Scholar] [CrossRef]
- Pitcher, G.R.; Newman, H.N.; Strahan, J.D. Access to subgingival plaque by disclosing agents using mouthrinsing and direct irrigation. J. Clin. Periodontol. 1980, 7, 300–308. [Google Scholar] [CrossRef]
- Langer, R. New methods of drug delivery. Science 1990, 249, 1527–1533. [Google Scholar] [CrossRef]
- Division of Industry and Consumer Education Medical Device Overview. Available online: https://www.fda.gov/ForIndustry/ImportProgram/ImportBasics/RegulatedProducts/ucm510630.htm (accessed on 25 March 2019).
- Etienne, D. Locally delivered antimicrobials for the treatment of chronic periodontitis. Oral Dis. 2003, 9, 45–50. [Google Scholar] [CrossRef]
- Smiley, C.J.; Tracy, S.L.; Abt, E.; Michalowicz, B.S.; John, M.T.; Gunsolley, J.; Cobb, C.M.; Rossmann, J.; Harrel, S.K.; Forrest, J.L.; et al. Evidence-based clinical practice guideline on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J. Am. Dent. Assoc. 2015, 146, 525–535. [Google Scholar] [CrossRef]
- Matesanz-Pérez, P.; García-Gargallo, M.; Figuero, E.; Bascones-Martínez, A.; Sanz, M.; Herrera, D. A systematic review on the effects of local antimicrobials as adjuncts to subgingival debridement, compared with subgingival debridement alone, in the treatment of chronic periodontitis. J. Clin. Periodontol. 2013, 40, 227–241. [Google Scholar] [CrossRef]
- Drisko, C.L. Periodontal debridement: Still the treatment of choice. J. Evid. Based. Dent. Pract. 2014, 14, 33–41. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Cortellini, P.; Carnevale, G.; Cattabriga, M.; De Sanctis, M.; Pini Prato, G.P. A controlled multicenter study of adjunctive use of tetracycline periodontal fibers in mandibular class II furcations with persistent bleeding. J. Clin. Periodontol. 1998, 25, 728–736. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Lang, N.P.; Cortellini, P.; Suvan, J.E.; Eickholz, P.; Fourmousis, I.; Topoll, H.; Vangsted, T.; Wallkamm, B. Effects of a single topical doxycycline administration adjunctive to mechanical debridement in patients with persistent/recurrent periodontitis but acceptable oral hygiene during supportive periodontal therapy. J. Clin. Periodontol. 2012, 39, 475–482. [Google Scholar] [CrossRef]
- Chambrone, L.; Vargas, M.; Arboleda, S.; Serna, M.; Guerrero, M.; de Sousa, J.; Lafaurie, G.I. Efficacy of Local and Systemic Antimicrobials in the Non-Surgical Treatment of Smokers with Chronic Periodontitis: A Systematic Review. J. Periodontol. 2016, 87, 1320–1332. [Google Scholar] [CrossRef]
- Rovai, E.S.; Souto, M.L.S.; Ganhito, J.A.; Holzhausen, M.; Chambrone, L.; Pannuti, C.M. Efficacy of Local Antimicrobials in the Non-Surgical Treatment of Patients with Periodontitis and Diabetes: A Systematic Review. J. Periodontol. 2016, 87, 1406–1417. [Google Scholar] [CrossRef]
- John, M.T.; Michalowicz, B.S.; Kotsakis, G.A.; Chu, H. Network meta-analysis of studies included in the Clinical Practice Guideline on the nonsurgical treatment of chronic periodontitis. J. Clin. Periodontol. 2017, 44, 603–611. [Google Scholar] [CrossRef]
- Hanes, P.J.; Purvis, J.P. Local anti-infective therapy: Pharmacological agents. A systematic review. Ann. Periodontol. 2003, 8, 79–98. [Google Scholar] [CrossRef]
- Bonito, A.; Lux, L.; Lohr, K. Impact of Local Adjuncts to Scaling and Root Planing in Periodontal Disease Therapy: A Systematic Review. J. Periodontol. 2005, 76, 1227–1236. [Google Scholar] [CrossRef]
- The Cochrane Collaboration Review Manager (RevMan), version 5.3; The Nordic Cochrane Centre: Copenhagen, Denmark, 2014.
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Available online: http://handbook-5-1.cochrane.org/ (accessed on 29 June 2018).
- Paolantonio, M.; D’Ercole, S.; Pilloni, A.; D’Archivio, D.; Lisanti, L.; Graziani, F.; Femminella, B.; Sammartino, G.; Perillo, L.; Tetè, S.; et al. Clinical, Microbiologic, and Biochemical Effects of Subgingival Administration of a Xanthan-Based Chlorhexidine Gel in the Treatment of Periodontitis: A Randomized Multicenter Trial. J. Periodontol. 2009, 80, 1479–1492. [Google Scholar] [CrossRef]
- Kranti, K.; Seshan, H.; Sameer, Z. Clinical evaluation of topical subgingival application of biodegradable xanthan based 1.5% Chlorhexidine gel for treatment of periodontal pockets. J. Adv. Oral Res. 2010, 1, 47–54. [Google Scholar]
- Jain, M.; Dave, D.; Jain, P.; Manohar, B.; Yadav, B.; Shetty, N. Efficacy of xanthan based chlorhexidine gel as an adjunct to scaling and root planing in treatment of the chronic periodontitis. J. Indian Soc. Periodontol. 2013, 17, 439–443. [Google Scholar] [CrossRef]
- Matesanz, P.; Herrera, D.; Echeverría, A.; O’Connor, A.; González, I.; Sanz, M. A randomized clinical trial on the clinical and microbiological efficacy of a xanthan gel with chlorhexidine for subgingival use. Clin. Oral Investig. 2013, 17, 55–66. [Google Scholar] [CrossRef]
- Jeffcoat, M.K.; Bray, K.S.; Ciancio, S.G.; Dentino, A.R.; Fine, D.H.; Gordon, J.M.; Gunsolley, J.C.; Killoy, W.J.; Lowenguth, R.A.; Magnusson, N.I.; et al. Adjunctive Use of a Subgingival Controlled-Release Chlorhexidine Chip Reduces Probing Depth and Improves Attachment Level Compared with Scaling and Root Planing Alone. J. Periodontol. 1998, 69, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Grisi, D.C.; Salvador, S.L.; Figueiredo, L.C.; Souza, S.L.S.; Novaes, A.B.J.; Grisi, M.F.M. Effect of a controlled-release chlorhexidine chip on clinical and microbiological parameters of periodontal syndrome. J. Clin. Periodontol. 2002, 29, 875–881. [Google Scholar] [CrossRef]
- Carvalho, J.; Novak, M.J.; Mota, L.F. Evaluation of the Effect of Subgingival Placement of Chlorhexidine Chips as an Adjunct to Scaling and Root Planing. J. Periodontol. 2007, 78, 997–1001. [Google Scholar] [CrossRef]
- Reddy, S.; Bhowmick, N.; Singh, S.; Mgs, P.; Amir, A. A comparison of Chlorhexidine and Tetracycline local drug delivery systems in management of persistent periodontal pockets—A clinical study. Int. J. Appl. Dent. Sci. 2016, 2, 11–15. [Google Scholar]
- Cosyn, J.; Wyn, I.; De Rouck, T.; Sabzevar, M.M. Long-Term Clinical Effects of a Chlorhexidine Varnish Implemented Treatment Strategy for Chronic Periodontitis. J. Periodontol. 2006, 77, 406–415. [Google Scholar] [CrossRef]
- Bogren, A.; Teles, R.P.; Torresyap, G.; Haffajee, A.D.; Socransky, S.S.; Wennström, J.L. Locally Delivered Doxycycline During Supportive Periodontal Therapy: A 3-Year Study. J. Periodontol. 2008, 79, 827–835. [Google Scholar] [CrossRef]
- Buduneli, E.; Tünger, A.; Evrenosoglu, E.; Bilgiç, A. Comparative clinical and microbiological effects of subgingival metronidazole application in adult periodontitis; 12-months results. J. Int. Acad. Periodontol. 2001, 3, 81–86. [Google Scholar]
- Cortelli, J.R.; Aquino, D.R.; Cortelli, S.C.; Carvalho-Filho, J.; Roman-Torres, C.V.G.; Costa, F.O. A double-blind randomized clinical trial of subgingival minocycline for chronic periodontitis. J. Oral Sci. 2008, 50, 259–265. [Google Scholar] [CrossRef] [Green Version]
- Killeen, A.C.; Harn, J.A.; Jensen, J.; Yu, F.; Custer, S.; Reinhardt, R.A. Two-Year Randomized Clinical Trial of Adjunctive Minocycline Microspheres in Periodontal Maintenance. J. Dent. Hyg. 2018, 92, 51–58. [Google Scholar]
- Timmerman, M.F.; Van der Weijden, G.A.; Van Steenbergen, T.J.M.; Mantel, M.S.; de Graaff, J.; Van der Velden, U. Evaluation of the long-term efficacy and safety of locally-applied minocycline in adult periodontitis patients. J. Clin. Periodontol. 1996, 23, 707–716. [Google Scholar] [CrossRef]
- Mombelli, A.; Brochut, P.; Plagnat, D.; Casagni, F.; Giannopoulou, C. Enamel matrix proteins and systemic antibiotics as adjuncts to non-surgical periodontal treatment: Clinical effects. J. Clin. Periodontol. 2005, 32, 225–230. [Google Scholar] [CrossRef]
- Omer, B.; Satti, A.; Gismalla, B.; Hashim, N. The effect of local application of hyaluronan gel as an adjunctive to scaling and root planing in chronic periodontitis patients. Afr. J. Dent. 2018, 6, 163–170. [Google Scholar]
- Bevilacqua, L.; Eriani, J.; Serroni, I.; Liani, G.; Borelli, V.; Castronovo, G.; Di Lenarda, R. Effectiveness of adjunctive subgingival administration of amino acids and sodium hyaluronate gel on clinical and immunological parameters in the treatment of chronic periodontitis. Ann. Stomatol. 2012, 3, 75–81. [Google Scholar]
- Eick, S.; Renatus, A.; Heinicke, M.; Pfister, W.; Stratul, S.-I.; Jentsch, H. Hyaluronic acid as an adjunct after scaling and root planing: A prospective randomized clinical trial. J. Periodontol. 2013, 84, 941–949. [Google Scholar] [CrossRef]
- Engstrüm, P.-E.; Shi, X.-Q.; Tronje, G.; Larsson, A.; Welander, U.; Frithiof, L.; Engstrom, G.N. The Effect of Hyaluronan on Bone and Soft Tissue and Immune Response in Wound Healing. J. Periodontol. 2001, 72, 1192–1200. [Google Scholar] [CrossRef]
- Birang, R.; Shahaboui, M.; Kiani, S.; Shadmehr, E.; Naghsh, N. Effect of nonsurgical periodontal treatment combined with diode laser or photodynamic therapy on chronic periodontitis: A randomized controlled split-mouth clinical trial. J. Lasers Med. Sci. 2015, 6, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Monzavi, A.; Chinipardaz, Z.; Mousavi, M.; Fekrazad, R.; Moslemi, N.; Azaripour, A.; Bagherpasand, O.; Chiniforush, N. Antimicrobial photodynamic therapy using diode laser activated indocyanine green as an adjunct in the treatment of chronic periodontitis: A randomized clinical trial. Photodiagnosis Photodyn. Ther. 2016, 14, 93–97. [Google Scholar] [CrossRef]
- Lulic, M.; Leiggener Görög, I.; Salvi, G.E.; Ramseier, C.A.; Mattheos, N.; Lang, N.P. One-year outcomes of repeated adjunctive photodynamic therapy during periodontal maintenance: A proof-of-principle randomized-controlled clinical trial. J. Clin. Periodontol. 2009, 36, 661–666. [Google Scholar] [CrossRef]
- Alwaeli, H.A.; Al-Khateeb, S.N.; Al-Sadi, A. Long-term clinical effect of adjunctive antimicrobial photodynamic therapy in periodontal treatment: A randomized clinical trial. Lasers Med. Sci. 2015, 30, 801–807. [Google Scholar] [CrossRef]
- Petelin, M.; Perkič, K.; Seme, K.; Gašpirc, B. Effect of repeated adjunctive antimicrobial photodynamic therapy on subgingival periodontal pathogens in the treatment of chronic periodontitis. Lasers Med. Sci. 2015, 30, 1647–1656. [Google Scholar] [CrossRef]
- Tabenski, L.; Moder, D.; Cieplik, F.; Schenke, F.; Hiller, K.-A.; Buchalla, W.; Schmalz, G.; Christgau, M. Antimicrobial photodynamic therapy vs. local minocycline in addition to non-surgical therapy of deep periodontal pockets: A controlled randomized clinical trial. Clin. Oral Investig. 2017, 21, 2253–2264. [Google Scholar] [CrossRef] [PubMed]
- Berakdar, M.; Callaway, A.; Fakhr Eddin, M.; Roß, A.; Willershausen, B. Comparison between scaling-root-planing (SRP) and SRP/photodynamic therapy: Six-month study. Head Face Med. 2012, 8, 2–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller Campanile, V.S.; Giannopoulou, C.; Campanile, G.; Cancela, J.A.; Mombelli, A. Single or repeated antimicrobial photodynamic therapy as adjunct to ultrasonic debridement in residual periodontal pockets: Clinical, microbiological, and local biological effects. Lasers Med. Sci. 2015, 30, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goh, E.X.; Tan, K.S.; Chan, Y.H.; Lim, L.P. Effects of root debridement and adjunctive photodynamic therapy in residual pockets of patients on supportive periodontal therapy: A randomized split-mouth trial. Photodiagnosis Photodyn. Ther. 2017, 18, 342–348. [Google Scholar] [CrossRef]
- Goodson, J.M.; Haffajee, A.; Socransky, S.S. Periodontal therapy by local delivery of tetracycline. J. Clin. Periodontol. 1979, 6, 83–92. [Google Scholar] [CrossRef]
- Stabholz, A.; Kettering, J.; Aprecio, R.; Zimmerman, G.; Baker, P.J.; Wikesjö, U.M.E. Retention of Antimicrobial Activity by Human Root Surfaces after in Situ Subgingival Irrigation with Tetracycline HCl or Chlorhexidine. J. Periodontol. 1993, 64, 137–141. [Google Scholar] [CrossRef]
- Tonetti, M.; Cugini, M.A.; Goodson, J.M. Zero-order delivery with periodontal placement of tetracycline-loaded ethylene vinyl acetate fibers. J. Periodontal Res. 1990, 25, 243–249. [Google Scholar] [CrossRef]
- Christersson, L.A.; Norderyd, O.M.; Puchalsky, C.S. Topical application of tetracycline-HCl in human periodontitis. J. Clin. Periodontol. 1993, 20, 88–95. [Google Scholar] [CrossRef]
- Tonetti, M.S. Local delivery of tetracycline: From concept to clinical application. J. Clin. Periodontol. 1998, 25, 969–977. [Google Scholar] [CrossRef]
- Gordon, J.M.; Walker, C.B.; Murphy, J.C.; Goodson, J.M.; Socransky, S.S. Tetracycline: Levels Achievable in Gingival Crevice Fluid and in Vitro Effect on Subgingival Organisms: Part I. Concentrations in Crevicular Fluid After Repeated Doses. J. Periodontol. 1981, 52, 609–612. [Google Scholar] [CrossRef]
- Norkiewicz, D.S.; Breault, L.G.; Wonderlich, S.T.; Malone, K.H. The Use of Chemotherapeutic Agents in Localized Periodontal Pockets. Mil. Med. 2001, 166, 940–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandekerckhove, B.N.A.; Quirynen, M.; van Steenberghe, D. The Use of Tetracycline-Containing Controlled-Release Fibers in the Treatment of Refractory Periodontitis. J. Periodontol. 1997, 68, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.G.; McGuire, M.K.; Greenstein, G.; Nunn, M. Tetracycline Fibers Plus Scaling and Root Planing Versus Scaling and Root Planing Alone: Similar Results After 5 Years. J. Periodontol. 1997, 68, 1029–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=050653 (accessed on 2 August 2018).
- Goodson, J.M.; Haffajee, A.D.; Socransky, S.S.; Kent, R.; Teles, R.; Hasturk, H.; Bogren, A.; Van Dyke, T.; Wennstrom, J.; Lindhe, J. Control of periodontal infections: A randomized controlled trial I. The primary outcome attachment gain and pocket depth reduction at treated sites. J. Clin. Periodontol. 2012, 39, 526–536. [Google Scholar] [CrossRef]
- Sinha, S.; Kumar, S.; Dagli, N.; Dagli, R.J. Effect of tetracycline HCl in the treatment of chronic periodontitis—A clinical study. J. Int. Soc. Prev. Community Dent. 2014, 4, 149. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, F.; Starosta, A.L.; Arenz, S.; Sohmen, D.; Dönhöfer, A.; Wilson, D.N. Tetracycline antibiotics and resistance mechanisms. Biol. Chem. 2014, 395, 559–575. [Google Scholar] [CrossRef]
- Stoller, N.H.; Johnson, L.R.; Trapnell, S.; Harrold, C.Q.; Garrett, S. The Pharmacokinetic Profile of a Biodegradable Controlled-Release Delivery System Containing Doxycycline Compared to Systemically Delivered Doxycycline in Gingival Crevicular Fluid, Saliva, and Serum. J. Periodontol. 1998, 69, 1085–1091. [Google Scholar] [CrossRef]
- Polson, A.M.; Garrett, S.; Stoller, N.H.; Bandt, C.L.; Hanes, P.J.; Killoy, W.J.; Southard, G.L.; Duke, S.P.; Bogle, G.C.; Drisko, C.H.; et al. Multi-Center Comparative Evaluation of Subgingivally Delivered Sanguinarine and Doxycycline in the Treatment of Periodontitis. II. Clinical Results. J. Periodontol. 1997, 68, 119–126. [Google Scholar] [CrossRef]
- Vanderkerckhove, B.N.A.; Quirynen, M.; Van Steenberghe, D. The use of locally-delivered minocycline in the treatment of chronic periodontitis. A review of the literature. J. Clin. Periodontol. 1998, 25, 964–968. [Google Scholar] [CrossRef]
- Williams, R.C.; Paquette, D.W.; Offenbacher, S.; Adams, D.F.; Armitage, G.C.; Bray, K.; Caton, J.; Cochran, D.L.; Drisko, C.H.; Fiorellini, J.P.; et al. Treatment of Periodontitis by Local Administration of Minocycline Microspheres: A Controlled Trial. J. Periodontol. 2001, 72, 1535–1544. [Google Scholar] [CrossRef]
- Jenkins, S.; Addy, M.; Wade, W. The mechanism of action of chlorhexidine. A study of plaque growth on enamel inserts in vivo. J. Clin. Periodontol. 1988, 15, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Rindom Schiostt, C. Effect of chlorhexidine on the microflora of the oral cavity. J. Periodontal Res. 1973, 8, 7–10. [Google Scholar] [CrossRef]
- Tomás, I.; García-Caballero, L.; López-Alvar, E.; Suárez, M.; Diz, P.; Seoane, J. In Situ Chlorhexidine Substantivity on Saliva and Plaque-Like Biofilm: Influence of Circadian Rhythm. J. Periodontol. 2013, 84, 1–15. [Google Scholar] [CrossRef]
- Hallmon, W.W.; Rees, T.D. Local Anti-Infective Therapy: Mechanical and Physical Approaches. A Systematic Review. Ann. Periodontol. 2003, 8, 99–114. [Google Scholar] [CrossRef] [PubMed]
- Goodson, J.M. Gingival crevice fluid flow. Periodontology 2000 2003, 31, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Hjeljord, L.G.; Rolla, G.; Bonesvoll, P. Chlorhexidine-protein interactions. J. Periodontal Res. 1973, 8, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Rolla, G.; Loe, H.; Rindom Schiott, C. The affinity of chlorhexidine for hydroxyapatite and salivary mucins. J. Periodontal Res. 1970, 5, 90–95. [Google Scholar] [CrossRef]
- Spijkervet, F.K.L.; van Saene, J.J.M.; van Saene, H.K.F.; Panders, A.K.; Vermey, A.; Fidler, V. Chlorhexidine inactivation by saliva. Oral Surg. Oral Med. Oral Pathol. 1990, 69, 444–449. [Google Scholar] [CrossRef]
- Soskolne, W.A.; Chajek, T.; Flashner, M.; Landau, I.; Stabholtz, A.; Kolatch, B.; Lerner, E.I. An in vivo study of the chlorhexidine release profile of the PerioChip in the gingival crevicular fluid, plasma and urine. J. Clin. Periodontol. 1998, 25, 1017–1021. [Google Scholar] [CrossRef]
- John, P.; Lazarus, F.; George, J.P.; Selvam, A.; Prabhuji, M.L.V. Adjunctive Effects of a Piscean Collagen-Based Controlled-Release Chlorhexidine Chip in the Treatment of Chronic Periodontitis: A Clinical and. J. Clin. Diagn. Res. 2015, 9, ZC70–ZC74. [Google Scholar] [CrossRef]
- Needleman, I.G.; Smales, F.C.; Martin, G.P. An investigation of bioadhesion for periodontal and oral mucosal drug delivery. J. Clin. Periodontol. 1997, 24, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Manthena, S.; Ramesh, A.; Srikanth, A.; Ramoji Rao, M.V.; Preethi, P.L.; Samatha, Y.P. Comparative evaluation of subgingivally delivered chlorhexidine varnish and chlorhexidine gel in reducing microbial count after mechanical periodontal therapy. J. Basic Clin. Pharm. 2015, 6, 24–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manikandan, D.; Balaji, V.R.; Niazi, T.M.; Rohini, G.; Karthikeyan, B.; Jesudoss, P. Chlorhexidine varnish implemented treatment strategy for chronic periodontitis: A clinical and microbial study. J. Pharm. Bioallied Sci. 2016, 8, S133–S137. [Google Scholar] [PubMed]
- Sachdeva, S.; Grover, V.; Malhotra, R.; Kapoor, A.; Mohanty, K. Comparison of clinical effectiveness of single and multiple applications of 1% chlorhexidine varnish (Cervitec Plus) along with scaling and root planing in patients with chronic periodontitis. J. Indian Soc. Periodontol. 2018, 22, 523–528. [Google Scholar]
- Brogden, R.N.; Heel, R.C.; Speight, T.M.; Avery, G.S. Metronidazole in Anaerobic Infections. Drugs 1978, 16, 387–417. [Google Scholar] [CrossRef]
- Norling, T.; Lading, P.; Engström, S.; Larsson, K.; Krog, N.; Nissen, S.S. Formulation of a drug delivery system based on a mixture of monoglycerides and triglycerides for use in the treatment of periodontal disease. J. Clin. Periodontol. 1992, 19, 687–692. [Google Scholar] [CrossRef]
- Stoltze, K. Concentration of metronidazole in periodontal pockets after application of a metronidazole 25% dental gel. J. Clin. Periodontol. 1992, 19, 698–701. [Google Scholar] [CrossRef]
- Stoltze, K.; Stellfeld, M. Systemic absorption of metronidazole after application of a metronidazole 25% dental gel. J. Clin. Periodontol. 1992, 19, 693–697. [Google Scholar] [CrossRef]
- Greenstein, G. Povidone-Iodine’s Effects and Role in the Management of Periodontal Diseases: A Review. J. Periodontol. 1999, 70, 1397–1405. [Google Scholar] [CrossRef]
- Sahrmann, P.; Puhan, M.A.; Attin, T.; Schmidlin, P.R. Systematic review on the effect of rinsing with povidone-iodine during nonsurgical periodontal therapy. J. Periodontal Res. 2010, 45, 153–164. [Google Scholar] [CrossRef] [Green Version]
- Berkelman, R.L.; Holland, B.W.; Anderson, R.L. Increased bactericidal activity of dilute preparations of povidone-iodine solutions. J. Clin. Microbiol. 1982, 15, 635–639. [Google Scholar] [PubMed]
- Ribeiro, É.D.P.; Bittencourt, S.; Ambrosano, G.M.B.; Nociti, F.H.; Sallum, E.A.; Sallum, A.W.; Casati, M.Z. Povidone-Iodine Used as an Adjunct to Non-Surgical Treatment of Furcation Involvements. J. Periodontol. 2006, 77, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Zanatta, G.M.; Bittencourt, S.; Nociti, F.H.; Sallum, E.A.; Sallum, A.W.; Casati, M.Z. Periodontal debridement with povidone-iodine in periodontal treatment: Short-term clinical and biochemical observations. J. Periodontol. 2006, 77, 498–505. [Google Scholar] [CrossRef]
- Leonhardt, A.; Bergström, C.; Krok, L.; Cardaropoli, G. Healing following ultrasonic debridement and PVP-iodine in individuals with severe chronic periodontal disease: A randomized, controlled clinical study. Acta Odontol. Scand. 2006, 64, 262–266. [Google Scholar] [CrossRef]
- Mohammadi, Z. Sodium hypochlorite in endodontics: An update review. Int. Dent. J. 2008, 58, 329–341. [Google Scholar] [CrossRef]
- Slots, J.; Jorgensen, M.G.M. Effective, safe, practical and affordable periodontal antimicrobial therapy: Where are we going, and are we there yet? Periodontology 2000 2002, 28, 298–312. [Google Scholar] [CrossRef]
- Bizzarro, S.; Van der Velden, U.; Loos, B.G. Local disinfection with sodium hypochlorite as adjunct to basic periodontal therapy: A randomized controlled trial. J. Clin. Periodontol. 2016, 43, 778–788. [Google Scholar] [CrossRef]
- Debnath, K.; Chatterjee, A.; Priya, V. Evaluation of Nano-Bio Fusion gel as an adjunct to scaling and root planing in chronic periodontitis: A clinico-microbiological study. J. Indian Soc. Periodontol. 2016, 20, 543. [Google Scholar]
- Hammarström, L.; Heijl, L.; Gestrelius, S. Periodontal regeneration in a buccal dehiscence model in monkeys after application of enamel matrix proteins. J. Clin. Periodontol. 1997, 24, 669–677. [Google Scholar] [CrossRef]
- Zetterstrom, O.; Andersson, C.; Eriksson, L.; Fredriksson, A.; Friskopp, J.; Heden, G.; Jansson, B.; Lundgren, T.; Nilveus, R.; Olsson, A.; et al. Clinical safety of enamel matrix derivative (EMDOGAIN) in the treatment of periodontal defects. J. Clin. Periodontol. 1997, 24, 697–704. [Google Scholar] [CrossRef]
- Heijl, L. Periodontal regeneration with enamel matrix derivative in one human experimental defect. A case report. J. Clin. Periodontol. 1997, 24, 693–696. [Google Scholar] [PubMed]
- Miron, R.J.; Sculean, A.; Cochran, D.L.; Froum, S.; Zucchelli, G.; Nemcovsky, C.; Donos, N.; Lyngstadaas, S.P.; Deschner, J.; Dard, M.; et al. Twenty years of enamel matrix derivative: The past, the present and the future. J. Clin. Periodontol. 2016, 43, 668–683. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Sculean, A.; Donos, N.; Lang, N.P. Pattern of mineralization after regenerative periodontal therapy with enamel matrix proteins. Eur. J. Oral Sci. 2006, 114, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Sculean, A.; Windisch, P.; Pjetursson, B.E.; Lang, N.P. Effects of enamel matrix proteins on tissue formation along the roots of human teeth. J. Periodontal Res. 2005, 40, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Windisch, P.; Keglevich, T.; Fabi, B.; Lundgren, E.; Lyngstadaas, P. Presence of an enamel matrix protein derivative on human teeth following periodontal surgery. Clin. Oral Investig. 2002, 6, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, M.A.; Mellonig, J.T.; Cochran, D.L. Evaluation of enamel matrix derivative as an adjunct to non-surgical periodontal therapy. J. Clin. Periodontol. 2003, 30, 739–745. [Google Scholar] [CrossRef]
- Graziani, F.; Gennai, S.; Petrini, M.; Bettini, L.; Tonetti, M. Enamel Matrix Derivative Stabilizes Blood Clot and Improves Clinical Healing in Deep Pockets After Flapless Periodontal Therapy: A Randomized Clinical Trial. J. Clin. Periodontol. 2019, 46, 231–240. [Google Scholar] [CrossRef]
- Rahemtulla, F. Proteoglycans of Oral Tissues. Crit. Rev. Oral Biol. Med. 1992, 3, 135–162. [Google Scholar] [CrossRef]
- Bartold, P.M. Proteoglycans of the periodontium: Structure, role and function. J. Periodontal Res. 1987, 22, 431–444. [Google Scholar] [CrossRef]
- Yamalik, N.; Kilinc, K.; Caglayan, F.; Eratalay, K.; Caglayan, G. Molecular size distribution analysis of human gingival proteoglycans and glycosaminoglycans in specific periodontal diseases. J. Clin. Periodontol. 1998, 25, 145–152. [Google Scholar] [CrossRef]
- Bartold, P.M.; Page, R.C. The effect of chronic inflammation on gingival connective tissue proteoglycans and hyaluronic acid. J. Oral Pathol. Med. 1986, 15, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Giannobile, W.V.; Al-Shammari, K.F.; Sarment, D.P. Matrix molecules and growth factors as indicators of periodontal disease activity. Periodontology 2000 2003, 31, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Y.J. Functions of hyaluronan in wound repair. Hyaluronan 2002, 2, 147–156. [Google Scholar]
- Moseley, R.; Waddington, R.J.; Embery, G. Hyaluronan and its Potential Role in Periodontal Healing. Dent. Update 2002, 29, 144–148. [Google Scholar] [CrossRef]
- Jentsch, H.; Pomowski, R.; Kundt, G.; Gocke, R. Treatment of gingivitis with hyaluronan. J. Clin. Periodontol. 2003, 30, 159–164. [Google Scholar] [CrossRef]
- Koshal, A.; Patel, P.; Bolt, R.; Bhupinder, D.; Galgut, P. A comparison in postoperative healing of sites receiving non-surgical debridement augmented with and without a single application of hyaluronan 0.8% gel. Prev. Dent. 2007, 2, 34–38. [Google Scholar]
- Soukos, N.S.; Goodson, J.M. Photodynamic therapy in the control of oral biofilms. Periodontology 2000 2011, 55, 143–166. [Google Scholar] [CrossRef]
- Macdonald, I.J.; Dougherty, T.J. Basic principles of photodynamic therapy. J. Porphyr. Phthalocyanines 2001, 5, 105–129. [Google Scholar] [CrossRef]
- Sarkar, S.; Wilson, M. Lethal photosensitization of bacteria in subgingival plaque from patients with chronic periodontitis. J. Periodontal Res. 1993, 28, 204–210. [Google Scholar] [CrossRef]
- Kömerik, N.; Wilson, M.; Poole, S. The Effect of Photodynamic Action on Two Virulence Factors of Gram-negative Bacteria. Photochem. Photobiol. 2007, 72, 676–680. [Google Scholar] [CrossRef]
- Chambrone, L.; Wang, H.; Romanos, G.E. Antimicrobial photodynamic therapy for the treatment of periodontitis and peri-implantitis: An American Academy of Periodontology best evidence review. J. Periodontol. 2018, 89, 783–803. [Google Scholar] [PubMed]
- Azaripour, A.; Dittrich, S.; Van Noorden, C.J.F.; Willershausen, B. Efficacy of photodynamic therapy as adjunct treatment of chronic periodontitis: A systematic review and meta-analysis. Lasers Med. Sci. 2018, 33, 407–423. [Google Scholar] [CrossRef] [PubMed]
- Akram, Z.; Hyder, T.; Al-Hamoudi, N.; Binshabaib, M.S.; Alharthi, S.S.; Hanif, A. Efficacy of photodynamic therapy versus antibiotics as an adjunct to scaling and root planing in the treatment of periodontitis: A systematic review and meta-analysis. Photodiagnosis Photodyn. Ther. 2017, 19, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Aoki, A.; Romanos, G.; Schwarz, F.; Miron, R.J.; Cosgarea, R. Is Photodynamic Therapy an Effective Treatment for Periodontal and Peri-Implant Infections? Dent. Clin. N. Am. 2015, 59, 831–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, B.C.; Patterson, M.S. The physics, biophysics and technology of photodynamic therapy. Phys. Med. Biol. 2008, 53, R61–R109. [Google Scholar] [CrossRef]
- Hopp, M.; Biffar, R. Photodynamic therapies–blue versus green. Laser 2013, 1, 10–25. [Google Scholar]
- Van der Weijden, G.A.; Timmerman, M.F. A systematic review on the clinical efficacy of subgingival debridement in the treatment of chronic periodontitis. J. Clin. Periodontol. 2002, 29, 55–71. [Google Scholar] [CrossRef]
- Vitt, A.; Gustafsson, A.; Ramberg, P.; Slizen, V.; Kazeko, L.A.; Buhlin, K. Polyhexamethylene guanidine phosphate irrigation as an adjunctive to scaling and root planing in the treatment of chronic periodontitis. Acta Odontol. Scand. 2019, 77, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Denez, E.M.; Toma, S.; Lasserre, J.F.; Brecx, M.C. Evaluation of a unique subgingival irrigation with 10% povidone-iodine after scaling and root planing: A randomized clinical trial. Quintessence Int. 2016, 47, 549–558. [Google Scholar]
- Kinane, D.F.; Radvar, M. A Six-Month Comparison of Three Periodontal Local Antimicrobial Therapies in Persistent Periodontal Pockets. J. Periodontol. 2005, 70, 1–7. [Google Scholar] [CrossRef]
- Gupta, R.; Pandit, N.; Aggarwal, S.; Verma, A. Comparative evaluation of subgingivally delivered 10% doxycycline hyclate and xanthan-based chlorhexidine gels in the treatment of chronic periodontitis. J. Contemp Dent. Pract. 2008, 9, 25–32. [Google Scholar] [PubMed]
- Radvar, M.; Pourtaghi, N.; Kinane, D.F. Comparison of 3 Periodontal Local Antibiotic Therapies in Persistent Periodontal Pockets. J. Periodontol. 1996, 67, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Lie, T.; Bruun, G.; Böe, O.E. Effects of Topical Metronidazole and Tetracycline in Treatment of Adult Periodontitis. J. Periodontol. 1998, 69, 819–827. [Google Scholar] [CrossRef]
- Keestra, J.A.J.; Grosjean, I.; Coucke, W.; Quirynen, M.; Teughels, W. Non-surgical periodontal therapy with systemic antibiotics in patients with untreated aggressive periodontitis: A systematic review and meta-analysis. J. Periodontal Res. 2015, 50, 689–706. [Google Scholar] [CrossRef]
- Armitage, G.C. Development of a Classification System for Periodontal Diseases and Conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef]
- Mombelli, A.; Cionca, N.; Almaghlouth, A. Does adjunctive antimicrobial therapy reduce the perceived need for periodontal surgery? Periodontology 2000 2011, 55, 205–216. [Google Scholar] [CrossRef] [Green Version]
- Chatzopoulos, G.-S.; Doufexi, A.-E. Photodynamic therapy in the treatment of aggressive periodontitis: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e192–e200. [Google Scholar] [CrossRef]
- Vohra, F.; Akram, Z.; Safii, S.H.; Vaithilingam, R.D.; Ghanem, A.; Sergis, K.; Javed, F. Role of antimicrobial photodynamic therapy in the treatment of aggressive periodontitis: A systematic review. Photodiagnosis Photodyn. Ther. 2016, 13, 139–147. [Google Scholar] [CrossRef]
- Souza, E.; Medeiros, A.C.; Gurgel, B.C.; Sarmento, C. Antimicrobial photodynamic therapy in the treatment of aggressive periodontitis: A systematic review and meta-analysis. Lasers Med. Sci. 2016, 31, 187–196. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Lang, N.P. Surgical and nonsurgical periodontal therapy. Learned and unlearned concepts. Periodontology 2000 2013, 62, 218–231. [Google Scholar] [CrossRef]
- Quirynen, M.; Teenberghe, W.; Soete, M.; Steenberghe, D. Topical antiseptics and antibiotics in the initial therapy of chronic adult periodontitis: Microbiological aspects. Periodontology 2000 2002, 28, 72–90. [Google Scholar] [CrossRef] [PubMed]
- Mager, D.L.; Ximenez-Fyvie, L.A.; Haffajee, A.D.; Socransky, S.S. Distribution of selected bacterial species on intraoral surfaces. J. Clin. Periodontol. 2003, 30, 644–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faveri, M.; Feres, M.; Shibli, J.A.; Hayacibara, R.F.; Hayacibara, M.M.; de Figueiredo, L.C. Microbiota of the Dorsum of the Tongue After Plaque Accumulation: An Experimental Study in Humans. J. Periodontol. 2006, 77, 1539–1546. [Google Scholar] [CrossRef] [PubMed]
- Feres, M.; Figueiredo, L.C.; Soares, G.M.S.; Faveri, M. Systemic antibiotics in the treatment of periodontitis. Periodontology 2000 2015, 67, 131–186. [Google Scholar] [CrossRef] [PubMed]
- Meinberg, T.A.; Barnes, C.M.; Dunning, D.G.; Reinhardt, R.A. Comparison of Conventional Periodontal Maintenance Versus Scaling and Root Planing with Subgingival Minocycline. J. Periodontol. 2002, 73, 167–172. [Google Scholar] [CrossRef]
- Hussein, I.; Ranka, M.; Gilbert, A.; Davey, K. Locally Delivered Antimicrobials in the Management of Periodontitis: A Critical Review of the Evidence for their Use in Practice. Dent. Update 2007, 34, 494–506. [Google Scholar] [CrossRef]
- Oral Health Division Ministry of Health Malaysia CPG. Management of Chronic Periodontitis, 2nd ed. 2012. Available online: http://www.moh.gov.my/moh/attachments/CPG%202014/Management_Orthodontic.pdf (accessed on 16 December 2019).
- Slots, J.; Pallasch, T.J. Dentists’ Role in Halting Antimicrobial Resistance. J. Dent. Res. 1996, 75, 1338–1341. [Google Scholar] [CrossRef]
- Walker, C.B.; Godowski, K.C.; Borden, L.; Lennon, J.; Nangó, S.; Stone, C.; Garrett, S. The Effects of Sustained Release Doxycycline on the Anaerobic Flora and Antibiotic-Resistant Patterns in Subgingival Plaque and Saliva. J. Periodontol. 2000, 71, 768–774. [Google Scholar] [CrossRef]
- Goodson, J.M.; Tanner, A. Antibiotic resistance of the subgingival microbiota following local tetracycline therapy. Oral Microbiol. Immunol. 1992, 7, 113–117. [Google Scholar] [CrossRef]
- Larsen, T. Occurrence of doxycycline resistant bacteria in the oral cavity after local administration of doxycycline in patients with periodontal disease. Scand. J. Infect. Dis. 1991, 23, 89–95. [Google Scholar] [CrossRef]
- Killoy, W. The clinical significance of local chemotherapies. J. Clin. Periodontol. 2002, 29, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J.; Giordano, J.; Soehren, S.; Hutchinson, R.; Rau, C.F.; Walsh, L.; Schork, M.A. Nonsurgical treatment of patients with periodontal disease. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1996, 81, 533–543. [Google Scholar] [CrossRef]
- Henke, C.J.; Genco, R.J.; Killoy, W.J.; Miller, D.P.; Evans, C.J.; Finkelmam, R.D. An economic evaluation of a chlorhexidine chip for treating chronic periodontitis: The CHIP (chlorhexidine in periodontitis) study. J. Am. Dent. Assoc. 2001, 132, 1557–1569. [Google Scholar] [CrossRef] [PubMed]
- Niederman, R.; Abdelshehid, G.; Goodson, J.M. Periodontal therapy using local delivery of antimicrobial agents. Dent. Clin. N. Am. 2002, 46, 665–677. [Google Scholar] [CrossRef]
- Wennstrom, J.L.; Newman, H.N.; MacNeill, S.R.; Killoy, W.J.; Griffiths, G.S.; Gillam, D.G.; Krok, L.; Needleman, I.G.; Weiss, G.; Garrett, S.; et al. Utilisation of locally delivered doxycycline in non-surgical treatment of chronic periodontitis. A comparative multi-centre trial of 2 treatment approaches. J. Clin. Periodontol. 2001, 28, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Braegger, U. Cost-benefit, cost-effectiveness and cost-utility analyses of periodontitis prevention. J. Clin. Periodontol. 2005, 32, 301–313. [Google Scholar] [CrossRef]
- Heasman, P.A.; Vernazza, C.R.; Gaunt, F.L.; Pennington, M.W. Cost-effectiveness of adjunctive antimicrobials in the treatment of periodontitis. Periodontology 2000 2011, 55, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Valentine, J.C.; Pigott, T.D.; Rothstein, H.R. How many studies do you need? A primer on statistical power for meta-analysis. J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Active Agent | Brand | Manufacturer | Dosage | Delivery Vehicle | Application and Duration (per Manufacturer/Study Design) | Longest Follow-Up Study | Authors | Study Design | Sample Size |
|---|---|---|---|---|---|---|---|---|---|
| Chlorhexidine | Chlo-Site® | Ghimas Company, Italy | 1.5% CHX | Gel | 1 application 15 days treatment | 6 months | Paolantonio et al. 2009 [41] | Split-mouth | 98 |
| Kranti et al. 2010 [42] | Split-mouth | 10 | |||||||
| Jain et al. 2013 [43] | Split-mouth | 30 | |||||||
| Matesanz et al. 2013 [44] | Parallel | 22 | |||||||
| Periochip® | Perio Products Ltd., Jerusalem, Israel | 2.5 mg CHX gluconate | Chip | 1 application 7 days treatment | 9 months | Jeffcoat et al. 1998 [45] | Parallel * | 419 | |
| Grisi et al. 2002 [46] | Parallel * | 20 | |||||||
| Carvalho et al. 2007 [47] | Split-mouth * | 28 | |||||||
| PerioCol®-CG | Eucare Pharmaceuticals Ltd., Chennai, India | 2.5 mg CHX gluconate | Chip | 1 application 7 days treatment | 12 months | Reddy et al. 2016 [48] | Parallel | 48 | |
| EC40® | Biodent BV, Nijmegen, The Netherlands | 35% CHX diacetate | Varnish | 1 application 7 days treatment | 9 months | Cosyn et al. 2006 [49] | Parallel | 26 | |
| Doxycycline | Atridox® | Atrix Laboratories, Fort Collins, CO, USA | 10% DOXY hyclate | Gel | 1 application 7 days treatment | 36 months | Bogren et al. 2008 [50] | Parallel * | 132 |
| Metronidazole | Elyzol® | Dumex, Copenhagen, Denmark | 25% MET benzoate | Gel | 2 applications 7 days treatment | 12 months | Buduneli et al. 2001 [51] | Split-mouth | 18 |
| Minocycline | Arestin® | OraPharma, Inc., Warminster, PA, USA | 1 mg MINO hydrochloride | Micro-spheres | 1 application 14 days treatment | 24 months | Cortelli et al. 2008 [52] | Parallel * | 30 |
| Killeen et al. 2018 [53] | Parallel * | 55 | |||||||
| Dentomycin® | Lederle Dental Division, Gosport, Hampshire, UK | 2% MINO hydrochloride | Ointment | 3–4 applications 14 days treatment | 18 months | Timmerman et al. 1996 [54] | Parallel * | 20 | |
| Periocline® | Sunstar Corp., Tokyo, Japan | ||||||||
| Tetracycline | Periodontal Plus ABTM | Advanced Biotech Products, Chennai, India | 2 mg TET hydrochloride | 1 application 7 days treatment | 12 months | Reddy et al. 2016 [48] | Parallel | 48 | |
| Enamel matrix derivative | Emdogain® | Institute Straumann AG, Basel, Switzerland | 30 mg/mL porcine enamel matrix derivative | Gel | 1 application | 12 months | Mombelli et al. 2005 [55] | Split-mouth | 16 |
| Hyaluronic acid | Aftamed® | BioPlax Limited, London, UK | 240 mg/100 g sodium hyaluronate | Gel | 1 application | 6 weeks | Omer at el. 2018 [56] | Split-mouth | 33 |
| Aminogam® | Errekappa Euroterapici, Spa, Italy | Sodium hyaluronate, amino acids | 1 application | 3 months | Bevilacqua et al. 2012 [57] | Split-mouth * | 11 | ||
| Gengigel® | Ricerfarma, Italy | 0.2% and 0.8% Sodium hyaluronate | 1 application | 6 months | Eick et al. 2013 [58] | Parallel * | 42 | ||
| Healon GV® | Pharmacia and Upjohn, Uppsala, Sweden. | 14 mg/mL sodium hyaluronate | 3 applications 27 days treatment | 12 months | Engstrüm et al. 2001 [59] | Split-mouth * | 9 | ||
| Photosensitiser | EmunDo® | A.R.C. laser GmbH, Germany | Indocyanine green (iodide-free) | Dye Solution | 2–4 applications 14–27 days treatment | 3 months | Birang et al. 2015 [60] | Split-mouth | 20 |
| Monzavi et al. 2016 [61] | Split-mouth * | 25 | |||||||
| HELBO® | Bredent Medical, Germany | Phenothiazine chloride | 1 application | 12 months | Lulic et al. 2009 [62] | Parallel | 10 | ||
| Alwaeli et al. 2015 [63] | Split-mouth * | 21 | |||||||
| Petelin et al. 2015 [64] | Parallel * | 27 | |||||||
| Tabenski et al. 2017 [65] | Parallel | 48 | |||||||
| PeriowaveTM | Periowave Dental Technologies Inc, Canada | Methylene blue | 1–3 applications | 6 months | Berakdar et al. 2012 [66] | Split-mouth | 22 | ||
| Müller Campanile et al. 2015 [67] | Split-mouth * | 28 | |||||||
| Fotosan® | CMS Dental, Copenhagen, Denmark | Toluidine blue/tolonium chloride | 1–3 applications | 6 months | Goh et al. 2017 [68] | Split-mouth | 27 |
| Author and Year (Ref.) | Study Period | Types of Studies | Treatment Arms | Weighted Mean Differences (WMD) (mm) [95% Confidence Interval (CI)] | Main Outcomes and Conclusion | |
|---|---|---|---|---|---|---|
| Probing Pocket Depth (PPD) | Clinical Attachment Level (CAL) * | |||||
| Hanes and Purvis [37] | ≥3 months | 28 RCT, 2 CCT, 2 cohort | 1. CHX, 2.5 mg in gelatin matrix | 0.35 [n/a] | 0.16 [n/a] |
|
| 2. MINO, 2% gel or ointment; microencapsulated powder | 0.36; 0.26 (micro) [n/a] | 0.39; −0.40 (micro) [n/a] | ||||
| 3. DOXY, 8.5% in biodegradable matrix; 15% | 0.51 [n/a] | 0.34 [n/a] | ||||
| 4. MET, 5%; 25% gel | 0.06 [n/a] | 0.07 [n/a] | ||||
| 5. TET, 25% fiber | 0.21 [n/a] | −0.17 [n/a] | ||||
| 6. Sanguinarine, 5% gel | n/a | n/a | ||||
| 7. CHX, 2%, 12%, and 0.2% irrigation; ethyl cellulose | n/a | n/a | ||||
| Bonito et al. [38] | No minimum duration | 50 RCT | 1. TET | 0.47 [0.22, 0.72] | 0.24 [0.07, 0.42] |
|
| 2. MINO | 0.49 [0.40, 0.58] | 0.46 [0.32, 0.60] | ||||
| 3. MET | 0.32 [0.20, 0.44] | 0.12 [0.01, 0.24] | ||||
| 4. CHX | 0.24 [0.13, 0.35] | 0.16 [0.04, 0.28] | ||||
| 5. Other antibiotics (DOXY; ofloxacin) | n/a | n/a | ||||
| 6. Other antimicrobials (amine fluoride; stannous fluoride; triclosan; hydrogen peroxide; povidone iodine; tetra-potassium peroxy-diphosphate) | n/a | n/a | ||||
| Matesanz-Pérez et al. [30] | No minimum duration | 52 RCT | 1. CHX chip | 0.328 [0.447, 0.209] | 0.218 [0.329, 0.107] |
|
| 2. CHX varnish | 0.413 [0.655, 0.170] | 0.029 [0.550, −0.492] | ||||
| 3. CHX xanthan gel | n/a | 0.891 [0.914, 0.867] | ||||
| 4. DOXY | 0.573 [0.778, 0.367] | 0.218 [0.260, 0.176] | ||||
| 5. MET | 0.157 [0.303, 0.011] | −0.008 [0.091, −0.107] | ||||
| 6. MINO | 0.472 [0.520, 0.424] | 0.189 [0.251, 0.126] | ||||
| 7. TET fiber | 0.727 [0.759, 0.695] | 0.327 [0.552, 0.101] | ||||
| 8. TET strip | n/a | 0.463 [0.401, 0.163] | ||||
| Smiley et al. [29] | ≥6 months | 72 RCT | 1. SDD | n/a | 0.35 [0.15, 0.56] |
|
| 2. Systemic antimicrobials | 0.35 [0.20, 0.51] | |||||
| 3. CHX chips | 0.40 [0.24, 0.56] | |||||
| 4. DOXY hyclate gel | 0.64 [0.00, 1.28] | |||||
| 5. MINO microspheres | 0.24 [−0.06, 0.55] | |||||
| 6. PDT with diode laser | 0.53 [0.06, 1.00] | |||||
| 7. Diode laser | 0.21 [−0.23, 0.64] | |||||
| 8. Nd:YAG lasers | 0.41 [−0.12, 0.94] | |||||
| 9. Erbium lasers | 0.18 [−0.63, 0.98] | |||||
| John et al. [36] # | 61 RCT | n/a | n/a |
| ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, O.L.; Safii, S.H.; Razali, M. Commercial Local Pharmacotherapeutics and Adjunctive Agents for Nonsurgical Treatment of Periodontitis: A Contemporary Review of Clinical Efficacies and Challenges. Antibiotics 2020, 9, 11. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9010011
Tan OL, Safii SH, Razali M. Commercial Local Pharmacotherapeutics and Adjunctive Agents for Nonsurgical Treatment of Periodontitis: A Contemporary Review of Clinical Efficacies and Challenges. Antibiotics. 2020; 9(1):11. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9010011
Chicago/Turabian StyleTan, Oi Leng, Syarida Hasnur Safii, and Masfueh Razali. 2020. "Commercial Local Pharmacotherapeutics and Adjunctive Agents for Nonsurgical Treatment of Periodontitis: A Contemporary Review of Clinical Efficacies and Challenges" Antibiotics 9, no. 1: 11. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9010011