A Cluster of Candida auris Blood Stream Infections in a Tertiary Care Hospital in Oman from 2016 to 2019

 and
and
Abstract
:1. Introduction
2. Results
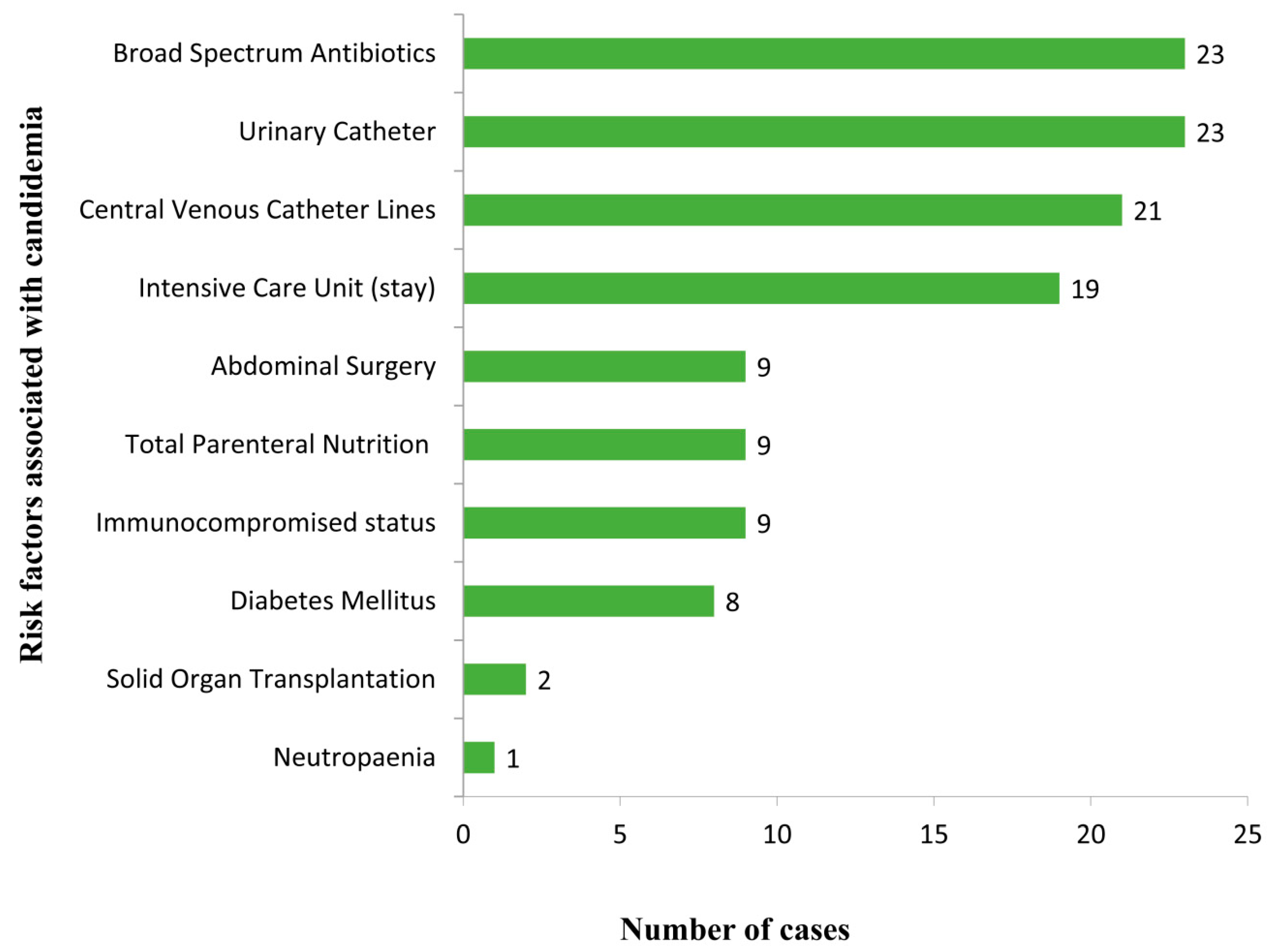
2.1. Clinical Characteristics and Manifestations
2.2. Microbiology
2.3. Treatment and Outcome
3. Discussion
4. Materials and Methods
4.1. Samples
4.2. Laboratory Investigations
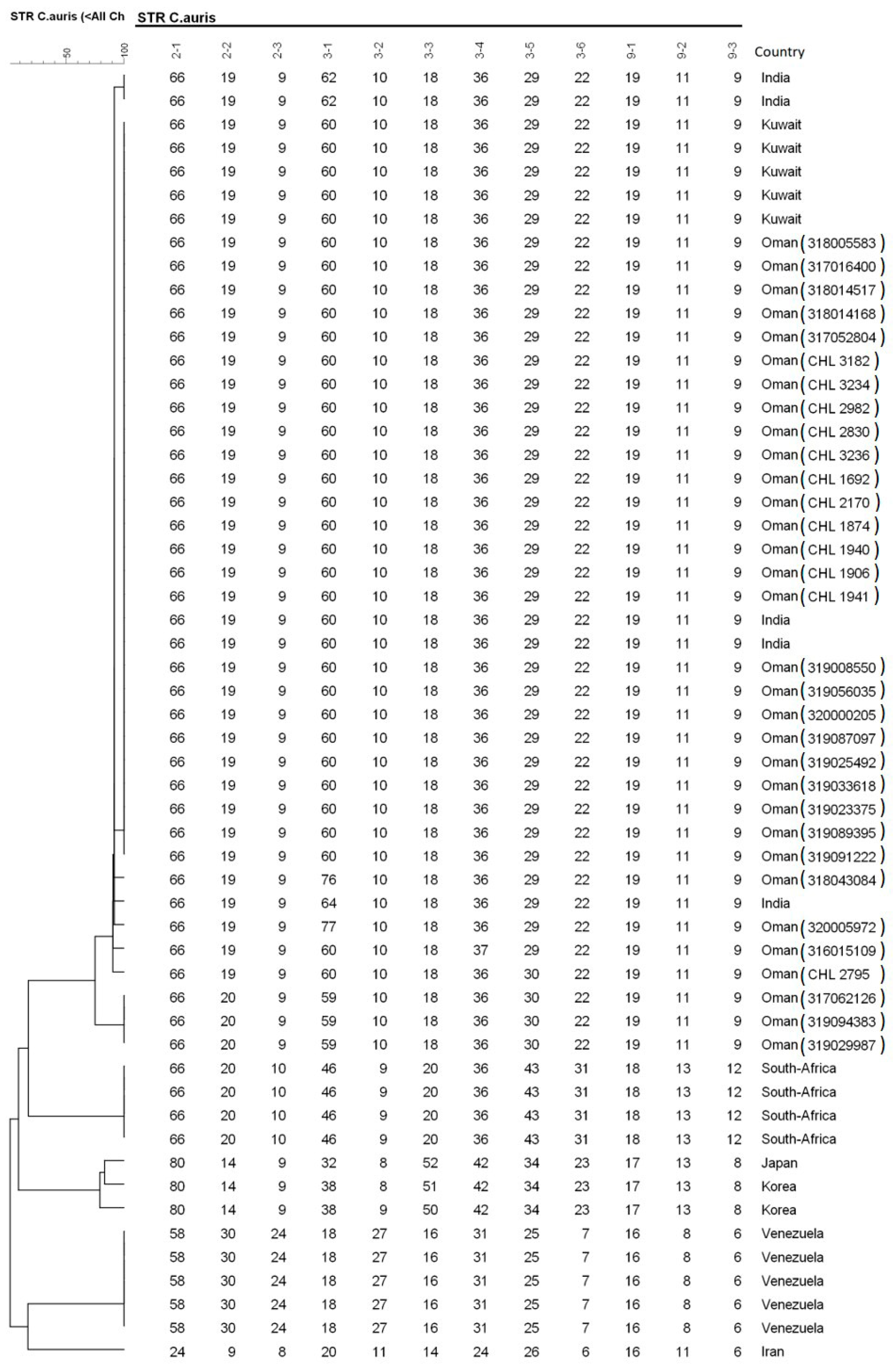
4.3. Molecular Identification Using ITS-Sequencing and STR-Genotyping
4.4. Antifungal Susceptibility Testing
4.5. Ethical Statement
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pfaller, M.; Diekema, D.J.; Turnidge, J.D.; Castanheira, M.; Jones, R.N. Twenty Years of the SENTRY Antifungal Surveillance Program: Results for Candida Species from 1997–2016. Open Forum Infect. Dis. 2019, 6, 79–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montagna, M.T.; Caggiano, G.; Lovero, G.; De Giglio, O.; Coretti, C.; Cuna, T.; Iatta, R.; Giglio, M.; Dalfino, L.; Bruno, F.; et al. Epidemiology of invasive fungal infections in the intensive care unit: Results of a multicenter Italian survey (AURORA Project). Infection 2013, 41, 645–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassetti, M.; Merelli, M.; Righi, E.; Diaz-Martin, A.; Rosello, E.M.; Luzzati, R.; Parra, A.; Trecarichi, E.M.; Sanguinetti, M.; Posteraro, B.; et al. Epidemiology, Species Distribution, Antifungal Susceptibility, and Outcome of Candidemia across Five Sites in Italy and Spain. J. Clin. Microbiol. 2013, 51, 4167–4172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klingspor, L.; Tortorano, A.M.; Pemán, J.; Willinger, B.; Hamal, P.; Sendid, B.; Velegraki, A.; Kibbler, C.; Meis, J.F.; Sabino, R.F.P.; et al. Invasive Candida infections in surgical patients in intensive care units: A prospective, multicentre survey initiated by the European Confederation of Medical Mycology (ECMM) (2006–2008). Clin. Microbiol. Infect. 2015, 21, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamoth, F.; Lockhart, S.R.; Berkow, E.L.; Calandra, T. Changes in the epidemiological landscape of invasive candidiasis. J. Antimicrob. Chemother. 2018, 73, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Kean, R.; Brown, J.L.; Gülmez, D.; Ware, A.; Ramage, G. Candida auris: A Decade of Understanding of an Enigmatic Pathogenic Yeast. J. Fungi 2020, 6, 30. [Google Scholar] [CrossRef] [Green Version]
- Chowdhary, A.; Sharma, C.; Meis, J.F. Candida auris: A rapidly emerging cause of hospital-acquired multidrug-resistant fungal infections globally. PLoS Pathog. 2017, 13, 1006290. [Google Scholar] [CrossRef]
- Calandra, T.; A Roberts, J.; Antonelli, M.; Bassetti, M.; Vincent, J.-L. Diagnosis and management of invasive candidiasis in the ICU: An updated approach to an old enemy. Crit. Care 2016, 20, 125. [Google Scholar] [CrossRef] [Green Version]
- Pristov, K.E.; Ghannoum, M. Resistance of Candida to azoles and echinocandins worldwide. Clin. Microbiol. Infect. 2019, 25, 792–798. [Google Scholar] [CrossRef]
- Jackson, B.R.; Chow, N.; Forsberg, K.; Litvintseva, A.P.; Lockhart, S.R.; Welsh, R.; Vallabhaneni, S.; Chiller, T. On the Origins of a Species: What Might Explain the Rise of Candida auris? J. Fungi 2019, 5, 58. [Google Scholar] [CrossRef] [Green Version]
- Borman, A.M.; Johnson, E.M. Candida auris in the UK: Introduction, dissemination, and control. PLoS Pathog. 2020, 16, e1008563. [Google Scholar] [CrossRef]
- Al Maani, A.; Paul, H.; Al-Rashdi, A.; Al Wahaibi, A.; Al-Jardani, A.; Abri, A.; Albalushi, M.A.H.; Al-Abri, S.; Al Reesi, M.; Al Maqbali, A.; et al. Ongoing Challenges with Healthcare-Associated Candida auris Outbreaks in Oman. J. Fungi 2019, 5, 101. [Google Scholar] [CrossRef] [Green Version]
- Benedict, K.; Roy, M.; Kabbani, S.; Anderson, E.J.; Farley, M.M.; Harb, S.; Harrison, L.H.; Bonner, L.; Wadu, V.L.; Marceaux, K.; et al. Neonatal and Pediatric Candidemia: Results from Population-Based Active Laboratory Surveillance in Four US Locations, 2009–2015. J. Pediatr. Infect. Dis. Soc. 2018, 7, 78–85. [Google Scholar] [CrossRef]
- Chowdhary, A.; Kumar, V.A.; Sharma, C.; Prakash, A.; Agarwal, K.; Babu, R.; Dinesh, K.R.; Karim, S.; Singh, S.K.; Hagen, F.; et al. Multidrug-resistant endemic clonal strain of Candida auris in India. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 33, 919–926. [Google Scholar] [CrossRef]
- Mohsin, J.; Hagen, F.; Al-Balushi, Z.A.M.; De Hoog, S.; Chowdhary, A.; Meis, J.F.; Al-Hatmi, A.M.S. The first cases of Candida auris candidaemia in Oman. Mycoses 2017, 60, 569–575. [Google Scholar] [CrossRef] [Green Version]
- Al-Siyabi, T.; Al Busaidi, I.; Balkhair, A.; Al-Muharrmi, Z.; Al-Salti, M.; Al’Adawi, B. First report of Candida auris in Oman: Clinical and microbiological description of five candidemia cases. J. Infect. 2017, 75, 373–376. [Google Scholar] [CrossRef]
- Eyre, D.W.; Sheppard, A.E.; Madder, H.; Moir, I.; Moroney, R.; Quan, T.P.; Griffiths, D.; George, S.; Butcher, L.; Morgan, M.; et al. A Candida auris Outbreak and Its Control in an Intensive Care Setting. N. Engl. J. Med. 2018, 379, 1322–1331. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Berkow, E.L.; Chow, N.; Welsh, R.M. Candida auris for the clinical microbiology laboratory: Not your grandfather’s Candida species. Clin. Microbiol. Newsl. 2017, 39, 99–103. [Google Scholar] [CrossRef] [Green Version]
- Astvad, K.; Johansen, H.K.; Røder, B.L.; Rosenvinge, F.S.; Knudsen, J.D.; Lemming, L.; Schønheyder, H.C.; Hare, R.K.; Kristensen, L.; Nielsen, L.; et al. Update from a twelve-year nationwide fungaemia surveillance: Increasing intrinsic and acquired resistance causes concern. J. Clin. Microbiol. 2018, 56, 107–119. [Google Scholar]
- Shastri, P.; Shankarnarayan, S.A.; Oberoi, J.; Rudramurthy, S.M.; Wattal, C.; Chakrabarti, A. Candida auris candidaemia in an intensive care unit—Prospective observational study to evaluate epidemiology, risk factors, and outcome. J. Crit. Care 2020, 57, 42–48. [Google Scholar] [CrossRef]
- Rudramurthy, S.M.; Chakrabarti, A.; Paul, R.A.; Sood, P.; Kaur, H.; Capoor, M.R.; Kindo, A.J.; Marak, R.S.K.; Arora, A.; Sardana, R.; et al. Candida auris candidaemia in Indian ICUs: Analysis of risk factors. J. Antimicrob. Chemother. 2017, 72, 1794–1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piedrahita, C.T.; Cadnum, J.L.; Jencson, A.L.; Shaikh, A.A.; Ghannoum, M.A.; Donskey, C.J. Environmental Surfaces in Healthcare Facilities are a Potential Source for Transmission ofCandida aurisand OtherCandidaSpecies. Infect. Control. Hosp. Epidem. 2017, 38, 1107–1109. [Google Scholar] [CrossRef] [Green Version]
- Schelenz, S.; Hagen, F.; Rhodes, J.; Abdolrasouli, A.; Chowdhary, A.; Hall, A.; Ryan, L.; Shackleton, J.; Trimlett, R.; Meis, J.F.; et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob. Resist. Infect. Control. 2016, 5, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Gaitán, A.; Moret, A.M.; Tasias-Pitarch, M.; Aleixandre-Lopez, A.I.; Martínez-Morel, H.; Calabuig, E.; Salavert-Lletí, M.; Ramírez, P.; Hontangas, J.L.L.; Hagen, F.; et al. An outbreak due to Candida auris with prolonged colonisation and candidaemia in a tertiary care European hospital. Mycoses 2018, 61, 498–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welsh, R.M.; Bentz, M.L.; Shams, A.; Houston, H.; Lyons, A.; Rose, L.J.; Litvintseva, A.P. Survival, Persistence, and Isolation of the Emerging Multidrug-Resistant Pathogenic Yeast Candida auris on a Plastic Health Care Surface. J. Clin. Microbiol. 2017, 55, 2996–3005. [Google Scholar] [CrossRef] [Green Version]
- Forsberg, K.; Woodworth, K.; Walters, M.; Berkow, E.L.; Jackson, B.; Chiller, T.; Vallabhaneni, S. Candida auris: The recent emergence of a multidrug-resistant fungal pathogen. Med Mycol. 2018, 57, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Tsay, S.; Welsh, R.M.; Adams, E.H.; Chow, N.A.; Gade, L.; Berkow, E.L.; Poirot, E.; Lutterloh, E.; Quinn, M.; Chaturvedi, S.; et al. Notes from the field: Ongoing transmission of Candida auris in health care facilities—United States, June 2016–May 2017. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 514. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. 2017. Candida Auris, Case Count Updated: 15 May 2020. Available online: https://www.cdc.gov/fungal/diseases/candidiasis/candida-auris.html (accessed on 4 July 2020).
- Sekyere, J.O. Candida auris: A systematic review and meta-analysis of current updates on an emerging multidrug-resistant pathogen. Microbiology 2019, 8, e00901. [Google Scholar] [CrossRef] [Green Version]
- Jeffery-Smith, A.; Taori, S.K.; Schelenz, S.; Jeffery, K.; Johnson, E.M.; Borman, A.M.; Manuel, R.; Brown, C.S. Candida auris: A Review of the Literature. Clin. Microbiol. Rev. 2017, 31, e00029-17. [Google Scholar] [CrossRef] [Green Version]
- Adam, R.D.; Revathi, G.; Okinda, N.; Fontaine, M.; Shah, J.; Kagotho, E.; Castanheira, M.; Pfaller, M.A.; Maina, D. Analysis of Candida auris fungemia at a single facility in Kenya. Int. J. Infect. Dis. 2019, 85, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous Emergence of Multidrug-Resistant Candida auris on 3 Continents Confirmed by Whole-Genome Sequencing and Epidemiological Analyses. Clin. Infect. Dis. 2016, 64, 134–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfouzan, W.; Dhar, R.; Albarrag, A.; Al-Abdely, H. The emerging pathogen Candida auris: A focus on the Middle-Eastern countries. J. Infect. Public Heal. 2019, 12, 451–459. [Google Scholar] [CrossRef]
- Ahmad, S.; Khan, Z.; Al-Sweih, N.; Alfouzan, W.; Joseph, L. Candida auris in various hospitals across Kuwait and their susceptibility and molecular basis of resistance to antifungal drugs. Mycoses 2019, 63, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Almaghrabi, R.S.; AlBalawi, R.; Mutabagani, M.; Atienza, E.; Aljumaah, S.; Gade, L.; Forsberg, K.; Litvintseva, A.; Althawadi, S. Molecular characterisation and clinical outcomes of Candida auris infection: Single-centre experience in Saudi Arabia. Mycoses 2020, 63, 452–460. [Google Scholar] [CrossRef]
- De Hoog, G.S.; Guarro, J.; Gené, J.; Ahmed, S.; Al-Hatmi, A.M.S.; Figueras, M.J.; Vitale, R.G. Atlas of Clinical Fungi, 4th ed.; Westerdijk Institute, Universitat Rovira i Virgili: Utrecht, The Netherlands, 2019. [Google Scholar]
- Lone, S.A.; Ahmad, A. Candida auris—The growing menace to global health. Mycoses 2019, 62, 620–637. [Google Scholar] [CrossRef] [Green Version]
- Chow, N.A.; de Groot, T.; Badali, H.; Abastabar, M.; Chiller, T.M.; Meis, J.F. Potential fifth clade of Candida auris, Iran, 2018. Emerg. Infect. Dis. 2019, 25, 1780–1781. [Google Scholar]
- De Groot, T.; Puts, Y.; Berrio, I.; Chowdhary, A.; Meis, J.F. Development of Candida auris Short Tandem Repeat Typing and Its Application to a Global Collection of Isolates. mBio 2020, 11, e02971-19. [Google Scholar] [CrossRef] [Green Version]
- Kenters, N.; Kiernan, M.; Chowdhary, A.; Denning, D.W.; Pemán, J.; Saris, K.; Schelenz, S.; Tartari, E.; Widmer, A.; Meis, J.F.; et al. Control of Candida auris in healthcare institutions: Outcome of an International Society for Antimicrobial Chemotherapy expert meeting. Int. J. Antimicrob. Agents 2019, 54, 400–406. [Google Scholar] [CrossRef]
- Caceres, D.H.; Forsberg, K.; Welsh, R.M.; Sexton, D.J.; Lockhart, S.R.; Jackson, B.R.; Chiller, T. Candida auris: A Review of Recommendations for Detection and Control in Healthcare Settings. J. Fungi 2019, 5, 111. [Google Scholar] [CrossRef] [Green Version]
- Arendrup, M.C.; Prakash, A.; Meletiadis, J.; Sharma, C.; Chowdhary, A. Comparison of EUCAST and CLSI Reference Microdilution MICs of Eight Antifungal Compounds for Candida auris and Associated Tentative Epidemiological Cutoff Values. Antimicrob. Agents Chemother. 2017, 61, e00485-17. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Sample No | MALDI-TOF/Sequencing | Age/Year | Sex | Duration of Treatment (Days) | Time of Candidemia Post Admission (Weeks) | MIC Values (mg/L) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AMB | FLC | ITC | VOR | POS | ISA | ANI | MICA | ||||||
| 317062126 | C. auris | 54 | M | 16 | 3 | 1 | >64 | 0.125 | 0.5 | 0.063 | 0.063 | 0.125 | 0.125 |
| 318005583 | C. auris | 50 | M | 28 | 2 | 1 | >64 | 0.125 | 0.5 | 0.063 | 0.031 | 0.5 | 0.25 |
| 317078724 | C. auris | 78 | F | 24 | 12 | 2 | 32 | 0.25 | 1 | 0.016 | 0.5 | 0.25 | 0.25 |
| 317052804 | C. auris | 69 | M | 14 | 1 | 0.5 | 64 | 0.063 | 0.25 | 0.016 | 0.125 | 0.25 | 0.125 |
| 318014168 | C. auris | 63 | F | 14 | 8 | 1 | 32 | 0.063 | 0.5 | 0.063 | 0.5 | 0.125 | 0.25 |
| 318014517 | C. auris | 30 | M | 4 | NA | 1 | 64 | 0.031 | 1 | 0.031 | 0.063 | 0.5 | 0.25 |
| 318028905 | C. auris | 76 | F | 10 | 16 | 1 | >64 | 0.125 | 1 | 0.063 | 0.031 | 0.25 | 0.25 |
| 318043084 | C. auris | 2 | M | 16 | 1 | 1 | >64 | 0.125 | 0.5 | 0.063 | 0.5 | 0.125 | 0.125 |
| 318066628 | C. auris | 0.5 | M | 15 | 4 | 2 | 64 | 0.5 | 0.5 | 0.031 | 0.063 | 0.5 | 0.25 |
| 318071689 | C. auris | 83 | M | NA | NA | 0.5 | 32 | 0.25 | 1 | 0.125 | 0.031 | 0.5 | 0.125 |
| 318095154 | C. auris | 70 | F | 17 | 3 | 1 | 64 | 0.125 | 1 | 0.063 | 0.063 | 0.125 | 0.25 |
| 319008550 | C. auris | 54 | M | 30 | 9 | 2 | >64 | 0.25 | 0.5 | 0.063 | 0.125 | 0.25 | 0.125 |
| 319056035 | C. auris | 62 | M | 2 | 2 | 2 | >64 | 0.063 | 0.5 | 0.063 | 0.25 | 0.125 | 0.125 |
| 320000205 | C. auris | 51 | M | 14 | 3 | 1 | 32 | 0.031 | 0.5 | 0.016 | 0.25 | 0.5 | 0.25 |
| 319087097 | C. auris | 62 | M | 2 | 5 | 1 | 64 | 0.125 | 1 | 0.031 | 0.063 | 0.5 | 0.25 |
| 319025492 | C. auris | 50 | M | 48 | 15 | 0.5 | >64 | 0.125 | 0.5 | 0.016 | 0.016 | 0.5 | 0.125 |
| 319033618 | C. auris | 47 | F | 16 | 2 | 1 | 32 | 0.125 | 0.25 | 0.016 | 0.016 | 0.5 | 0.25 |
| 319023375 | C. auris | 62 | M | 14 | 15 | 2 | >64 | 0.25 | 0.5 | 0.063 | 0.125 | 0.25 | 0.25 |
| 319089395 | C. auris | 49 | F | 11 | 5 | 1 | 32 | 0.063 | 0.5 | 0.016 | 0.125 | 0.5 | 0.25 |
| 319091222 | C. auris | 54 | M | 14 | 6 | 1 | 64 | 0.063 | 1 | 0.25 | 0.031 | 0.25 | 0.125 |
| 320005972 | C. auris | 31 | M | 14 | 1 | 1 | >64 | 0.5 | 1 | 0.125 | 0.5 | 0.25 | 0.125 |
| 319094383 | C. auris | 47 | M | 14 | 2 | 1 | 64 | 0.125 | 1 | 0.031 | 0.031 | 0.25 | 0.125 |
| 319029987 | C. auris | 64 | F | 17 | 2 | 1 | 64 | 0.125 | 1 | 0.25 | 0.031 | 0.25 | 0.125 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohsin, J.; Weerakoon, S.; Ahmed, S.; Puts, Y.; Al Balushi, Z.; Meis, J.F.; Al-Hatmi, A.M.S. A Cluster of Candida auris Blood Stream Infections in a Tertiary Care Hospital in Oman from 2016 to 2019. Antibiotics 2020, 9, 638. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9100638
Mohsin J, Weerakoon S, Ahmed S, Puts Y, Al Balushi Z, Meis JF, Al-Hatmi AMS. A Cluster of Candida auris Blood Stream Infections in a Tertiary Care Hospital in Oman from 2016 to 2019. Antibiotics. 2020; 9(10):638. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9100638
Chicago/Turabian StyleMohsin, Jalila, Sanjeewani Weerakoon, Sarah Ahmed, Ynze Puts, Zainab Al Balushi, Jacques F. Meis, and Abdullah M.S. Al-Hatmi. 2020. "A Cluster of Candida auris Blood Stream Infections in a Tertiary Care Hospital in Oman from 2016 to 2019" Antibiotics 9, no. 10: 638. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9100638