Helicobacter pylori Primary and Secondary Genotypic Resistance to Clarithromycin and Levofloxacin Detection in Stools: A 4-Year Scenario in Southern Italy

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Results
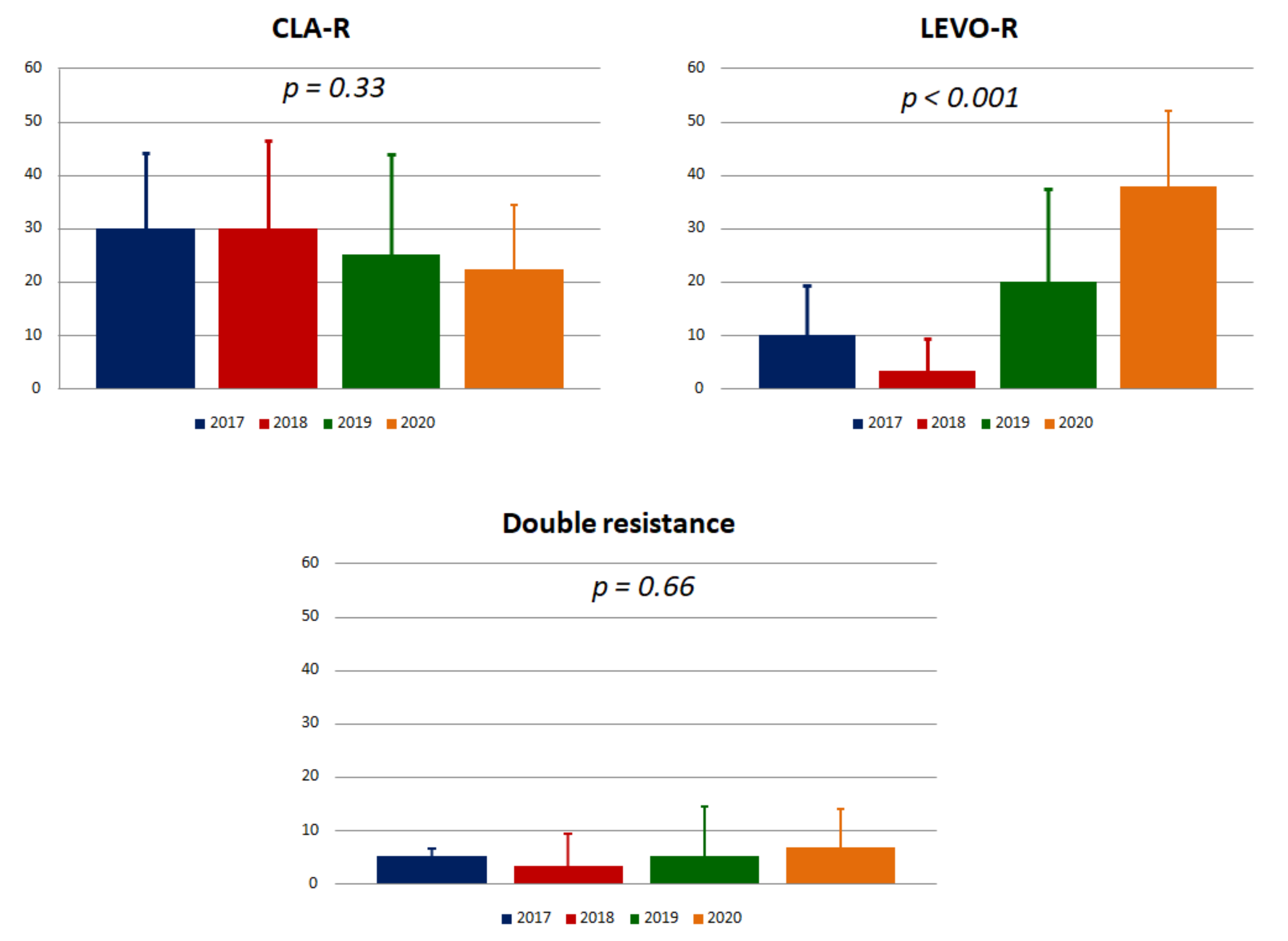
2.1. Naive Patients
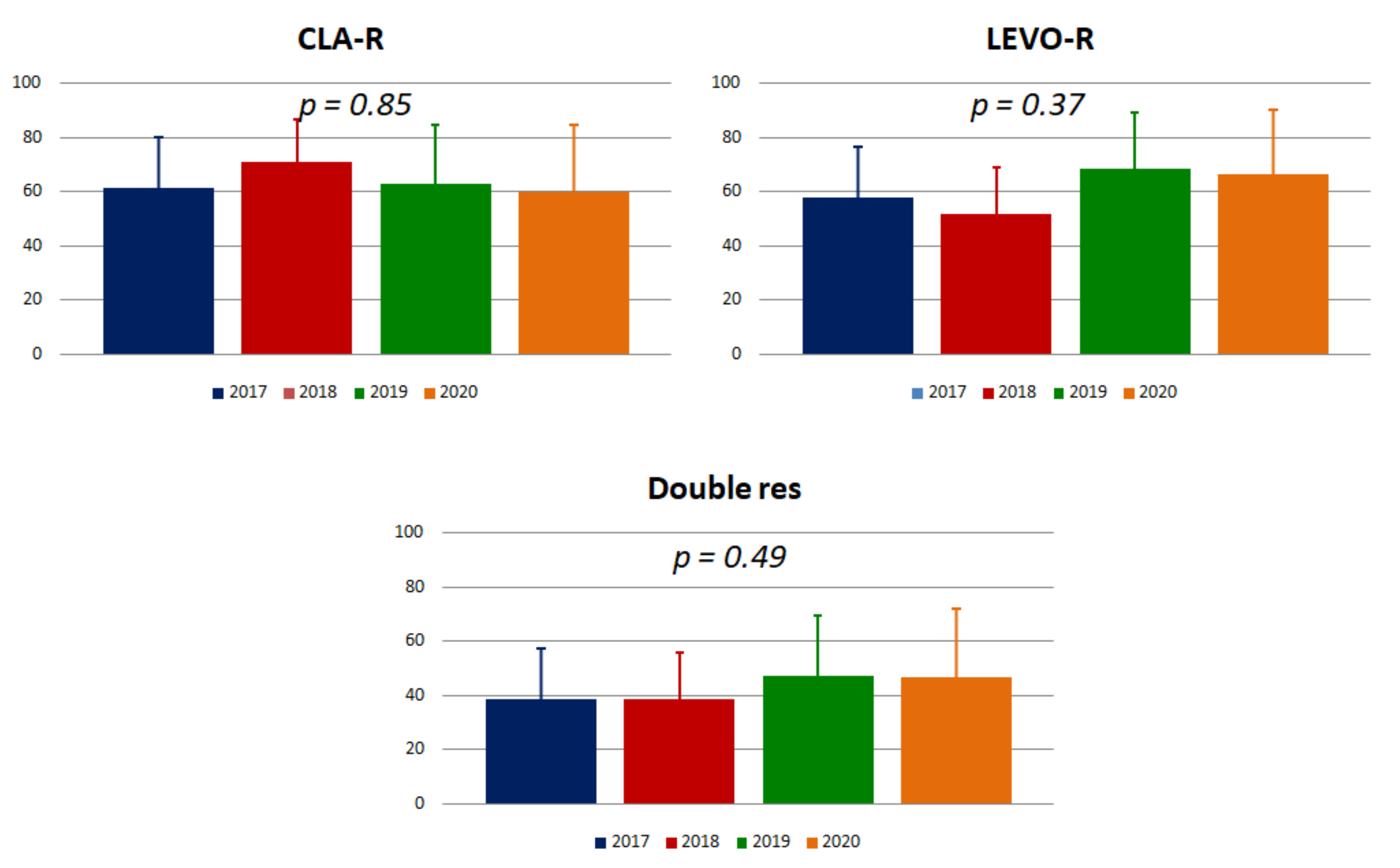
2.2. Secondary Resistance
3. Discussion
4. Materials and Methods
4.1. Patient Recruitment
4.2. Antibiotic Resistance Analysis
4.3. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- De Francesco, V.; Giorgio, F.; Hassan, C.; Manes, G.; Vannella, L.; Panella, C.; Ierardi, E.; Zullo, A. Worldwide H. pylori antibiotic resistance: A systematic review. J. Gastrointest. Liver Dis. 2010, 19, 409–414. [Google Scholar]
- Ierardi, E.; Giorgio, F.; Losurdo, G.; Di Leo, A.; Principi, M. How antibiotic resistances could change Helicobacter pylori treatment: A matter of geography? World J. Gastroenterol. 2013, 19, 8168–8180. [Google Scholar] [CrossRef] [PubMed]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 2016, 43, 514–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Francesco, V.; Margiotta, M.; Zullo, A.; Hassan, C.; Giorgio, F.; Burattini, O.; Stoppino, G.; Cea, U.; Pace, A.; Zotti, M.; et al. Prevalence of primary clarithromycin resistance in Helicobacter pylori strains over a 15 year period in Italy. J. Antimicrob. Chemother. 2007, 59, 783–785. [Google Scholar] [CrossRef] [PubMed]
- Megraud, F. H. pylori antibiotic resistance: prevalence, importance, and advances in testing. Gut 2004, 53, 1374–1384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Francesco, V.; Margiotta, M.; Zullo, A.; Hassan, C.; Troiani, L.; Burattini, O.; Stella, F.; Di Leo, A.; Russo, F.; Marangi, S.; et al. Clarithromycin-Resistant Genotypes and Eradication of Helicobacter pylori. Ann. Intern. Med. 2006, 144, 94–100. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, V.; Zullo, A.; Ierardi, E.; Giorgio, F.; Perna, F.; Hassan, C.; Panella, C.; Vaira, D. The A2143G Point Mutation of Clarithromycin Resistance Affects Helicobacter pylori Eradication. J. Clin. Gastroenterol. 2009, 43, 386. [Google Scholar] [CrossRef]
- De Francesco, V.; Zullo, A.; Ierardi, E.; Vaira, D. Minimal inhibitory concentration (MIC) values and different point mutations in the 23S rRNA gene for clarithromycin resistance in Helicobacter pylori. Dig. Liver Dis. 2009, 41, 610–611. [Google Scholar] [CrossRef]
- Federico, A.; Nardone, G.; Gravina, A.G.; Iovene, M.R.; Miranda, A.; Compare, D.; Pilloni, P.A.; Rocco, A.; Ricciardiello, L.; Marmo, R.; et al. Efficacy of 5-Day Levofloxacin-Containing Concomitant Therapy in Eradication of Helicobacter pylori Infection. Gastroenterol. 2012, 143, 55–61.e1. [Google Scholar] [CrossRef]
- Dang, N.Q.H.; Ha, T.M.T.; Nguyen, S.-T.; Le, N.D.K.; Nguyen, T.M.T.; Nguyen, T.H.; Pham, T.T.H.; Tran, V.H. High rates of clarithromycin and levofloxacin resistance of Helicobacter pylori in patients with chronic gastritis in the south east area of Vietnam. J. Glob. Antimicrob. Resist. 2020, 22, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Zou, Y.; Qian, X.; Liu, X.; Song, Y.; Song, C.; Wu, S.; An, Y.; Yuan, R.; Wang, Y.; Xie, Y. The effect of antibiotic resistance on Helicobacter pylori eradication efficacy: A systematic review and meta-analysis. Helicobacter 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Zullo, A.; Hassan, C.; Lorenzetti, R.; Winn, S.; Morini, S. A clinical practice viewpoint: to culture or not to culture Helicobacter pylori? Dig. Liver Dis. 2003, 35, 357–361. [Google Scholar] [CrossRef]
- Monno, R.; Giorgio, F.; Carmine, P.; Soleo, L.; Cinquepalmi, V.; Ierardi, E. Helicobacter pylori clarithromycin resistance detected by Etest and TaqMan real-time polymerase chain reaction: A comparative study. APMIS 2012, 120, 712–717. [Google Scholar] [CrossRef]
- De Francesco, V.; Zullo, A.; Ierardi, E.; Giorgio, F.; Perna, F.; Hassan, C.; Morini, S.; Panella, C.; Vaira, D. Phenotypic and genotypic Helicobacter pylori clarithromycin resistance and therapeutic outcome: Benefits and limits. J. Antimicrob. Chemother. 2009, 65, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Ierardi, E.; Giorgio, F.; Iannone, A.; Losurdo, G.; Principi, M.; Barone, M.; Pisani, A.; Di Leo, A. Noninvasive molecular analysis of Helicobacter pylori: Is it time for tailored first-line therapy? World J. Gastroenterol. 2017, 23, 2453–2458. [Google Scholar] [CrossRef]
- Iannone, A.; Giorgio, F.; Russo, F.; Riezzo, G.; Girardi, B.; Pricci, M.; Palmer, S.C.; Barone, M.; Principi, M.; Strippoli, G.F.; et al. New fecal test for non-invasive Helicobacter pylori detection: A diagnostic accuracy study. World J. Gastroenterol. 2018, 24, 3021–3029. [Google Scholar] [CrossRef]
- Giorgio, F.; Ierardi, E.; Sorrentino, C.; Principi, M.; Barone, M.; Losurdo, G.; Iannone, A.; Giangaspero, A.; Monno, R.; Di Leo, A. Helicobacter pylori DNA isolation in the stool: an essential pre-requisite for bacterial noninvasive molecular analysis. Scand. J. Gastroenterol. 2016, 51, 1429–1432. [Google Scholar] [CrossRef]
- Khadangi, F.; Yassi, M.; Kerachian, M.A. Review: Diagnostic accuracy of PCR-based detection tests for Helicobacter pylori in stool samples. Helicobacter 2017, 22, e12444. [Google Scholar] [CrossRef]
- Losurdo, G.; Leandro, G.; Principi, M.; Giorgio, F.; Montenegro, L.; Sorrentino, C.; Ierardi, E.; Di Leo, A. Sequential vs. prolonged 14-day triple therapy for Helicobacter pylori eradication: the meta-analysis may be influenced by ‘geographical weighting’. Int. J. Clin. Pr. 2015, 69, 1112–1120. [Google Scholar] [CrossRef]
- De Francesco, V.; Giorgio, F.; Ierardi, E.; Zotti, M.; Neri, M.; Milano, A.; Varasano, V.; Luzza, F.; Suraci, E.; Marmo, R.; et al. Primary clarithromycin resistance in Helicobacter pylori: The Multicentric Italian Clarithromycin Resistance Observational (MICRO) study. J. Gastrointest. Liver Dis. 2011, 20, 235–239. [Google Scholar]
- Saleem, Z.; Saeed, H.; Hassali, M.A.; Godman, B.; Asif, U.; Yousaf, M.; Ahmed, Z.; Riaz, H.; Raza, S.A. Pattern of inappropriate antibiotic use among hospitalized patients in Pakistan: A longitudinal surveillance and implications. Antimicrob. Resist. Infect. Control. 2019, 8, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antibiotici Chinolonici e Fluorochinolonici per Uso Sistemico e Inalatorio. Available online: https://www.aifa.gov.it/sites/default/files/NII_fluorochinoloni_08.04.2019.pdf (accessed on 24 July 2020).
- Zagari, R.M.; Romano, M.; Ojetti, V.; Stockbrugger, R.; Gullini, S.; Annibale, B.; Farinati, F.; Ierardi, E.; Maconi, G.; Rugge, M.; et al. Guidelines for the management of Helicobacter pylori infection in Italy: The III Working Group Consensus Report 2015. Dig. Liver Dis. 2015, 47, 903–912. [Google Scholar] [CrossRef] [PubMed]
- De Palma, G.Z.; Mendiondo, N.; Wonaga, A.; Viola, L.; Ibarra, D.; Campitelli, E.; Salim, N.; Corti, R.; Goldman, C.; Catalano, M. Occurrence of Mutations in the Antimicrobial Target Genes Related to Levofloxacin, Clarithromycin, and Amoxicillin Resistance in Helicobacter pylori Isolates from Buenos Aires City. Microb. Drug Resist. 2016, 23, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.-H. Distribution of gyrA mutations in fluoroquinolone-resistant Helicobacter pylori strains. World J. Gastroenterol. 2010, 16, 2272–2277. [Google Scholar] [CrossRef]
- Glocker, E.; Kist, M. Rapid Detection of Point Mutations in the gyrA Gene of Helicobacter pylori Conferring Resistance to Ciprofloxacin by a Fluorescence Resonance Energy Transfer-Based Real-Time PCR Approach. J. Clin. Microbiol. 2004, 42, 2241–2246. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Naive Patients (n = 135) | Failure Patients (n = 91) | p | |
|---|---|---|---|
| Age (mean ± SD) | 42.1 ± 12.8 | 43.2 ± 13.5 | 0.54 |
| Sex M/F | 54/81 | 41/50 | 0.49 |
| Smokers, n (%) | 32 (23.7%) | 21 (23.1%) | 1 |
| Endoscopic picture, n | (n = 106) | (n = 72) | 0.11 |
| Normal | 16 (15.1%) | 6 (8.3%) | |
| Antral erosions | 36 (34.0%) | 21 (29.2%) | |
| Mucosal hyperemia | 51 (48.1%) | 43 (59.4%) | |
| PUD | 3 (2.8%) | 2 (2.8%) |
| One Failure N = 56 | Two Failures N = 35 | p | |
|---|---|---|---|
| CLA-R, n (%) | 34 (60.7%) | 25 (71.4%) | 0.37 |
| LEVO-R, n (%) | 23 (41.1%) | 31 (88.6%) | <0.001 |
| Double resistance, n (%) | 18 (32.1%) | 20 (57.1%) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Losurdo, G.; Giorgio, F.; Pricci, M.; Girardi, B.; Russo, F.; Riezzo, G.; Martulli, M.; Piazzolla, M.; Cocomazzi, F.; Abbruzzi, F.; et al. Helicobacter pylori Primary and Secondary Genotypic Resistance to Clarithromycin and Levofloxacin Detection in Stools: A 4-Year Scenario in Southern Italy. Antibiotics 2020, 9, 723. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9100723
Losurdo G, Giorgio F, Pricci M, Girardi B, Russo F, Riezzo G, Martulli M, Piazzolla M, Cocomazzi F, Abbruzzi F, et al. Helicobacter pylori Primary and Secondary Genotypic Resistance to Clarithromycin and Levofloxacin Detection in Stools: A 4-Year Scenario in Southern Italy. Antibiotics. 2020; 9(10):723. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9100723
Chicago/Turabian StyleLosurdo, Giuseppe, Floriana Giorgio, Maria Pricci, Bruna Girardi, Francesco Russo, Giuseppe Riezzo, Manuela Martulli, Mariano Piazzolla, Francesco Cocomazzi, Francesco Abbruzzi, and et al. 2020. "Helicobacter pylori Primary and Secondary Genotypic Resistance to Clarithromycin and Levofloxacin Detection in Stools: A 4-Year Scenario in Southern Italy" Antibiotics 9, no. 10: 723. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9100723