Antimicrobial Susceptibility Patterns and Wild-Type MIC Distributions of Anaerobic Bacteria at a German University Hospital: A Five-Year Retrospective Study (2015–2019)

 ,
,  , and
, and 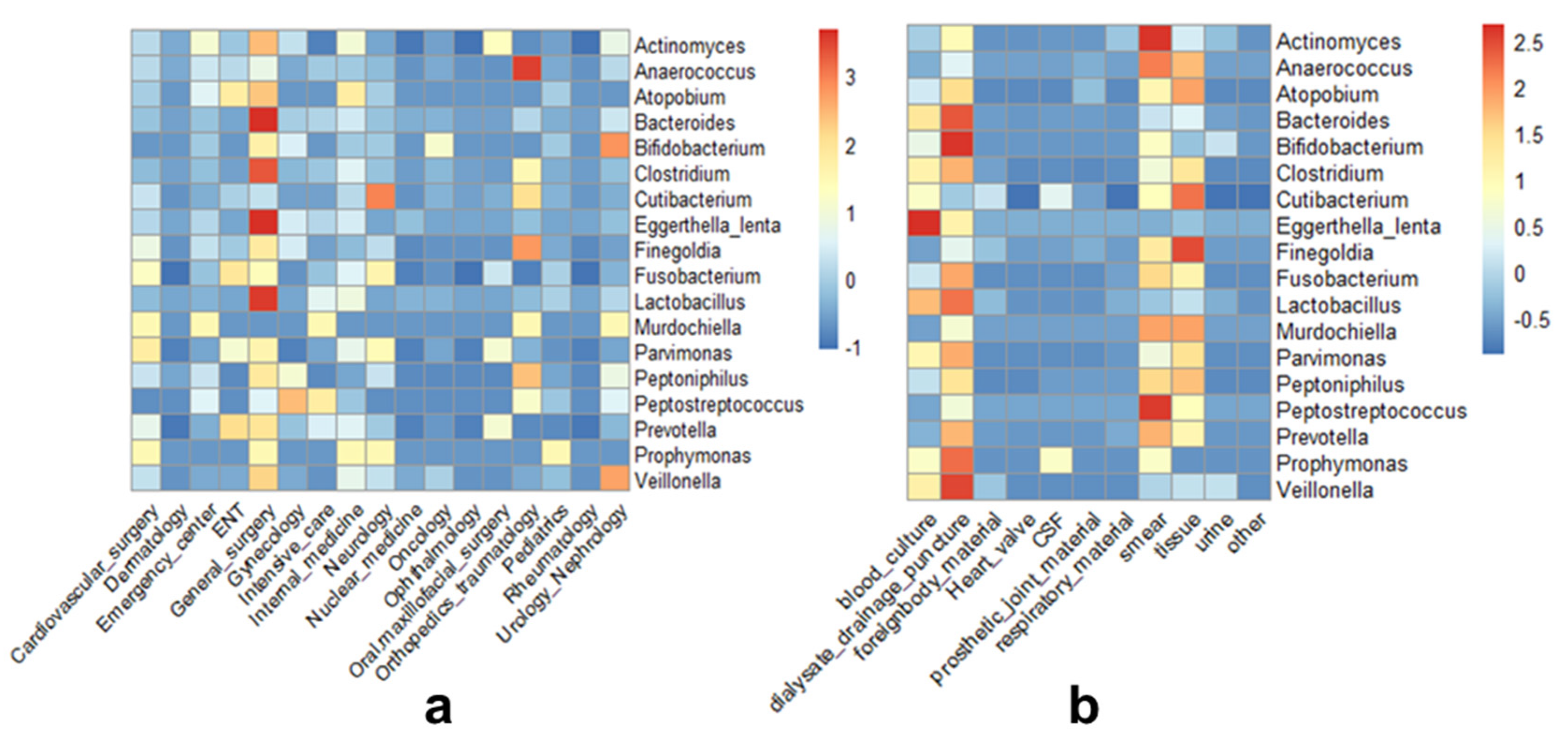{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Characterization of Isolated Anaerobic Bacteria
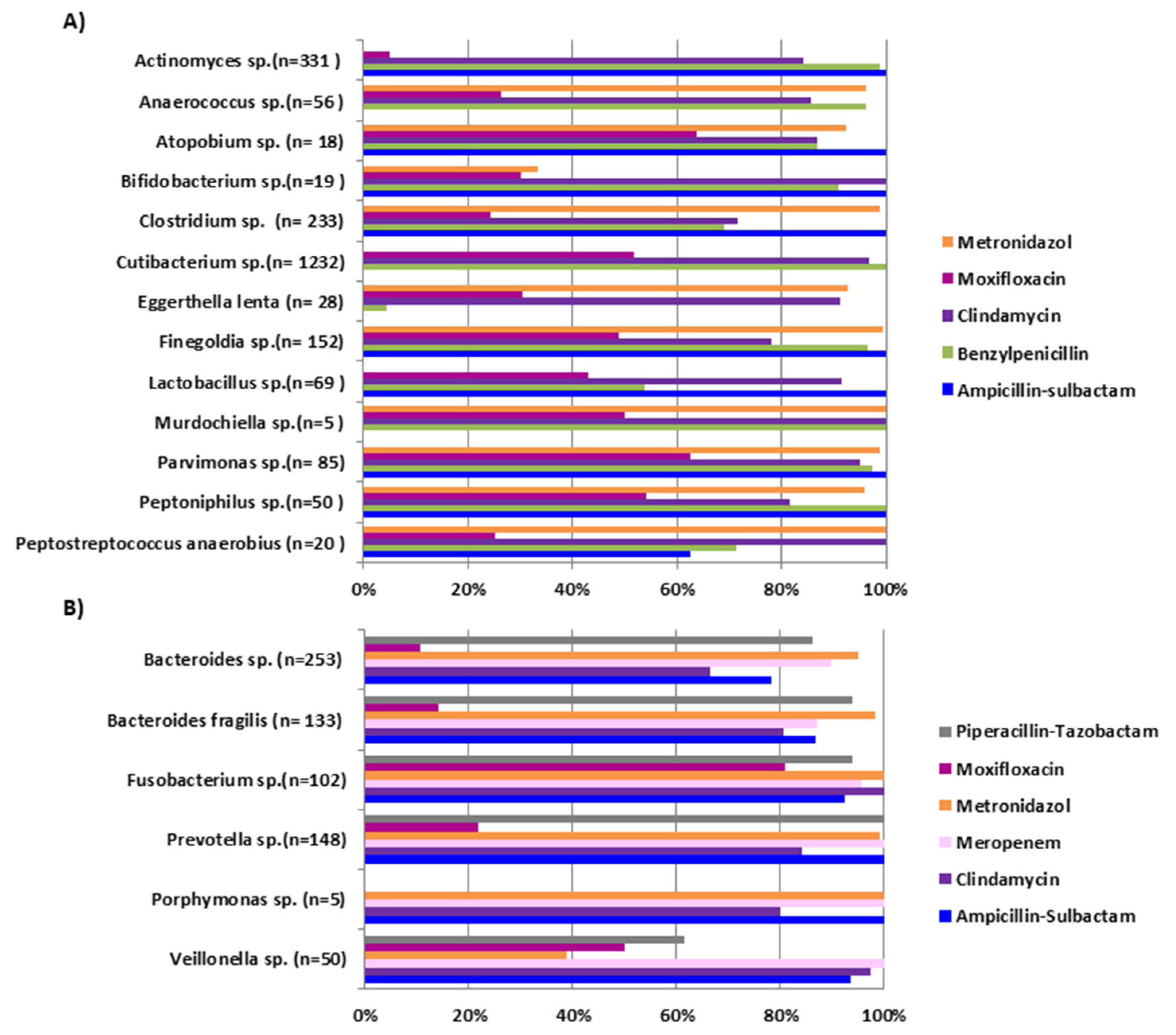
2.2. Antimicrobial Susceptibility Patterns
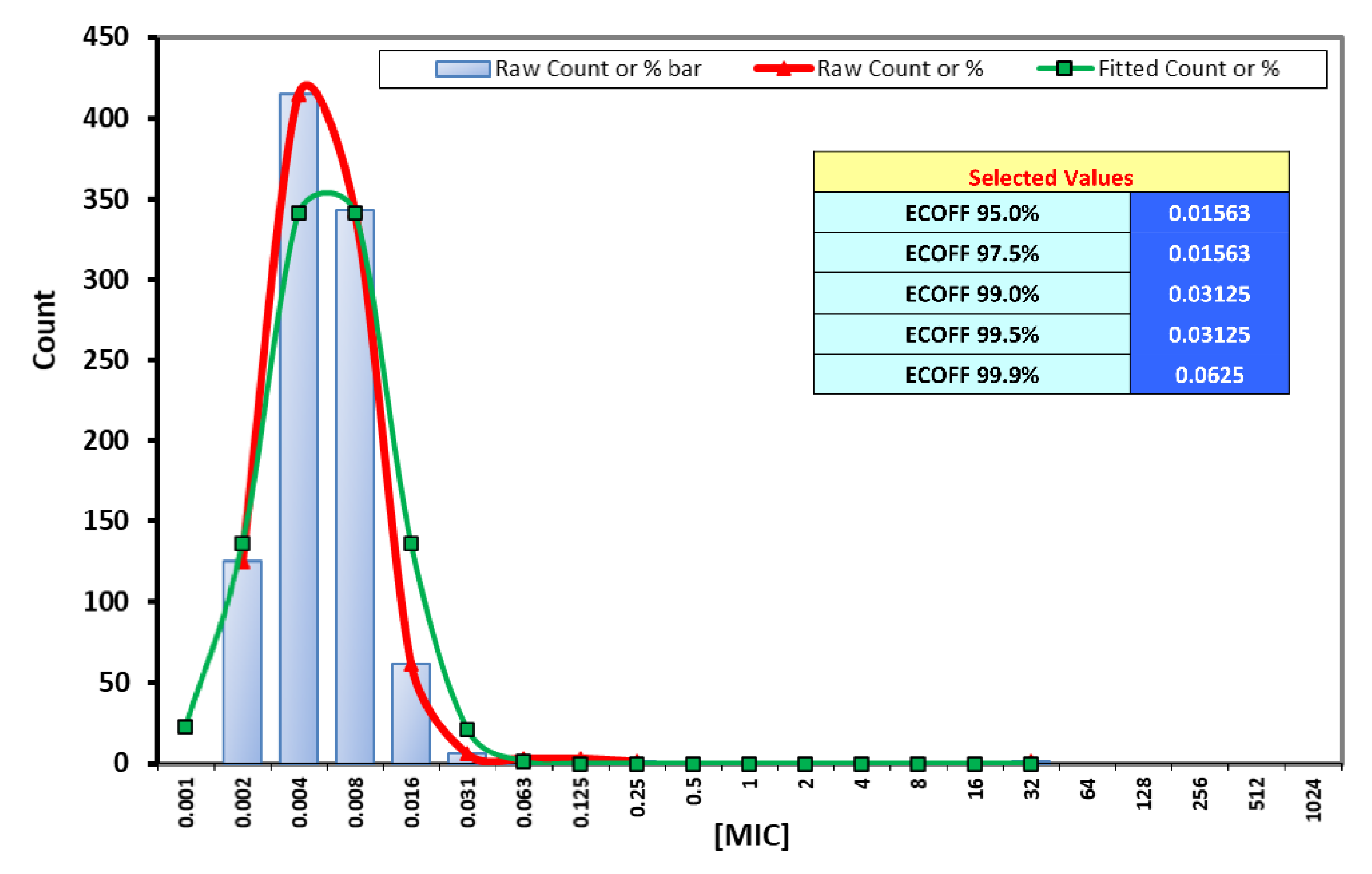
2.3. Wild-Type MIC Distributions
3. Discussion
4. Materials and Methods
4.1. Isolates Collection
4.2. Cultivation and Identification of Anaerobic Bacteria
4.3. Antimicrobial Susceptibility Testing
4.4. Determination of Wild-Type MIC Distributions and Cutoff Value
4.5. Demographic and Clinical Data
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Brook, I. Spectrum and treatment of anaerobic infections. J. Infect. Chemother. 2016, 22, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Shah, N.B.; Tande, A.J.; Patel, R.; Berbari, E.F. Anaerobic prosthetic joint infection. Anaerobe 2015, 36, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nagy, E. Anaerobic infections: Update on treatment considerations. Drugs 2010, 70, 841–858. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. Diagnosis and Management of Anaerobic Infections of the Head and Neck. Ann. Otol. Rhinol. Laryngol. Suppl. 1992, 155, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Boyanova, L.; Kolarov, R.; Mitov, I. Recent evolution of antibiotic resistance in the anaerobes as compared to previous decades. Anaerobe 2015, 31, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Ananth-Shenoy, P.; Vishwanath, S.; Targain, R.; Shetty, S.; Sunil-Rodrigues, G.; Mukhopadhyay, C.; Kiran, C. Anaerobic infections in surgical wards: A two year study. Iran. J. Microbiol. 2016, 8, 181–186. [Google Scholar]
- Citron, D.M.; Goldstein, E.J.C.; Merriam, C.V.; Lipsky, B.A.; Abramson, M.A. Bacteriology of Moderate-to-Severe Diabetic Foot Infections and In Vitro Activity of Antimicrobial Agents. J. Clin. Microbiol. 2007, 45, 2819–2828. [Google Scholar] [CrossRef] [Green Version]
- Byun, J.H.; Kim, M.; Lee, Y.; Lee, K.; Chong, Y. Antimicrobial Susceptibility Patterns of Anaerobic Bacterial Clinical Isolates From 2014 to 2016, Including Recently Named or Renamed Species. Ann. Lab. Med. 2019, 39, 190–199. [Google Scholar] [CrossRef] [Green Version]
- Lozupone, C.A.; Stombaugh, J.I.; Gordon, J.I.; Jansson, J.K.; Knight, R. Diversity, stability and resilience of the human gut microbiota. Nature 2012, 489, 220–230. [Google Scholar] [CrossRef] [Green Version]
- Walker, A.W.; Duncan, S.H.; Louis, P.; Flint, H.J. Phylogeny, culturing, and metagenomics of the human gut microbiota. Trends Microbiol. 2014, 22, 267–274. [Google Scholar] [CrossRef]
- Cobo, F.; Rodríguez-Granger, J.; Pérez-Zapata, I.; Sampedro, A.; Aliaga, L.; Navarro-Marí, J.M. Antimicrobial susceptibility and clinical findings of significant anaerobic bacteria in southern Spain. Anaerobe 2019, 59, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Shimura, S.; Watari, H.; Komatsu, M.; Kuchibiro, T.; Fukuda, S.; Nishio, H.; Kita, M.; Kida, K.; Oohama, M.; Toda, H.; et al. Antimicrobial susceptibility surveillance of obligate anaerobic bacteria in the Kinki area. J. Infect. Chemother. 2019, 25, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Marchand-Austin, A.; Rawte, P.; Toye, B.; Jamieson, F.B.; Farrell, D.J.; Patel, S.N. Antimicrobial Susceptibility of Clinical Isolates of Anaerobic Bacteria in Ontario, 2010–2011. Anaerobe 2014, 28, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-Joint Infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gueimonde, M.; Sánchez, B.; de los Reyes-Gavilán, C.G.; Margolles, A. Antibiotic resistance in probiotic bacteria. Front Microbiol. 2013, 4, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacqueline, C.; Caillon, J. Impact of bacterial biofilm on the treatment of prosthetic joint infections. J. Antimicrob. Chemother. 2014, 69 (Suppl. 1), i37–i40. [Google Scholar] [CrossRef] [Green Version]
- Kahlmeter, G.; Brown, D.F.J.; Goldstein, F.W.; MacGowan, A.P.; Mouton, J.W.; Österlund, A.; Rodloff, A.; Steinbakk, M.; Urbaskova, P.; Vatopoulos, A. European harmonization of MIC breakpoints for antimicrobial susceptibility testing of bacteria. J. Antimicrob. Chemother. 2003, 52, 145–148. [Google Scholar] [CrossRef] [Green Version]
- Behra-Miellet, J.; Dubreuil, L.; Jumas-Bilak, E. Antianaerobic activity of moxifloxacin compared with that of ofloxacin, ciprofloxacin, clindamycin, metronidazole and β-lactams. Int. J. Antimicrob. Agents 2002, 20, 366–374. [Google Scholar] [CrossRef]
- Zambrano, D. The role of anaerobic bacteria in human infections. Clin. Ther. 1993, 15, 244–260; discussion 215. [Google Scholar]
- Cobo, F.; Guillot, V.; Navarro-Marí, J.M. Breast Abscesses Caused by Anaerobic Microorganisms: Clinical and Microbiological Characteristics. Antibiotics 2020, 9, 341. [Google Scholar] [CrossRef]
- Lee, Y.; Park, Y.; Kim, M.S.; Yong, D.; Jeong, S.H.; Lee, K.; Chong, Y. Antimicrobial Susceptibility Patterns for Recent Clinical Isolates of Anaerobic Bacteria in South Korea. Antimicrob. Agents Chemother. 2010, 54, 3993–3997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Park, Y.-J.; Kim, M.-N.; Uh, Y.; Kim, M.S.; Lee, K. Multicenter Study of Antimicrobial Susceptibility of Anaerobic Bacteria in Korea in 2012. Ann. Lab. Med. 2015, 35, 479–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veloo, A.C.M.; Tokman, H.B.; Jean-Pierre, H.; Dumont, Y.; Jeverica, S.; Lienhard, R.; Novak, A.; Rodloff, A.; Rotimi, V.; Wybo, I.; et al. Antimicrobial susceptibility profiles of anaerobic bacteria, isolated from human clinical specimens, within different European and surrounding countries. A joint ESGAI study. Anaerobe 2020, 61, 102111. [Google Scholar] [CrossRef]
- Liderot, K.; Ratcliffe, P.; Lüthje, P.; Thidholm, E.; Özenci, V. Microbiological diagnosis of Eggerthella lenta blood culture isolates in a Swedish tertiary hospital: Rapid identification and antimicrobial susceptibility profile. Anaerobe 2016, 38, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.-R.; Huang, Y.-T.; Liao, C.-H.; Chuang, T.-Y.; Wang, W.-J.; Lee, S.-W.; Lee, L.-N.; Hsueh, P.-R. Clinical and Microbiological Characteristics of Bacteremia Caused by Eggerthella, Paraeggerthella, and Eubacterium Species at a University Hospital in Taiwan from 2001 to 2010. J. Clin. Microbiol. 2012, 50, 2053–2055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardiner, B.J.; Tai, A.Y.; Kotsanas, D.; Francis, M.J.; Roberts, S.A.; Ballard, S.A.; Junckerstorff, R.K.; Korman, T.M. Clinical and Microbiological Characteristics of Eggerthella lenta Bacteremia. J. Clin. Microbiol. 2015, 53, 626–635. [Google Scholar] [CrossRef] [Green Version]
- Wybo, I.; Van den Bossche, D.; Soetens, O.; Vekens, E.; Vandoorslaer, K.; Claeys, G.; Glupczynski, Y.; Ieven, M.; Melin, P.; Nonhoff, C.; et al. Fourth Belgian multicentre survey of antibiotic susceptibility of anaerobic bacteria. J. Antimicrob. Chemother. 2014, 69, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Brazier, J.; Chmelar, D.; Dubreuil, L.; Feierl, G.; Hedberg, M.; Kalenic, S.; Könönen, E.; Lundgren, B.; Malamou-Ladas, H.; Nagy, E.; et al. European surveillance study on antimicrobial susceptibility of Gram-positive anaerobic cocci. Int. J. Antimicrob. Agents 2008, 31, 316–320. [Google Scholar] [CrossRef]
- Novak, A.; Rubic, Z.; Dogas, V.; Goic-Barisic, I.; Radic, M.; Tonkic, M. Antimicrobial susceptibility of clinically isolated anaerobic bacteria in a University Hospital Centre Split, Croatia in 2013. Anaerobe 2015, 31, 31–36. [Google Scholar] [CrossRef]
- Jeverica, S.; Kolenc, U.; Mueller-Premru, M.; Papst, L. Evaluation of the routine antimicrobial susceptibility testing results of clinically significant anaerobic bacteria in a Slovenian tertiary-care hospital in 2015. Anaerobe 2017, 47, 64–69. [Google Scholar] [CrossRef]
- Jakab, E.; Zbinden, R.; Gubler, J.; Ruef, C.; von Graevenitz, A.; Krause, M. Severe infections caused by Propionibacterium acnes: An underestimated pathogen in late postoperative infections. Yale J. Biol. Med. 1996, 69, 477–482. [Google Scholar] [PubMed]
- Crane, J.K.; Hohman, D.W.; Nodzo, S.R.; Duquin, T.R. Antimicrobial Susceptibility of Propionibacterium acnes Isolates from Shoulder Surgery. Antimicrob. Agents Chemother. 2013, 57, 3424–3426. [Google Scholar] [CrossRef] [Green Version]
- Khassebaf, J.; Hellmark, B.; Davidsson, S.; Unemo, M.; Nilsdotter-Augustinsson, Å.; Söderquist, B. Antibiotic susceptibility of Propionibacterium acnes isolated from orthopaedic implant-associated infections. Anaerobe 2015, 32, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Chow, A.W.; Patten, V.; Guze, L.B. Comparative Susceptibility of Anaerobic Bacteria to Minocycline, Doxycycline, and Tetracycline. Antimicrob. Agents Chemother. 1975, 7, 46–49. [Google Scholar] [CrossRef] [Green Version]
- Wexler, H.M. Bacteroides: The Good, the Bad, and the Nitty-Gritty. Clin. Microbiol. Rev. 2007, 20, 593–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagy, E.; Urbán, E.; Nord, C.E. Antimicrobial susceptibility of Bacteroides fragilis group isolates in Europe: 20 years of experience. Clin. Microbiol. Infect. 2011, 17, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlowsky, J.A.; Walkty, A.J.; Adam, H.J.; Baxter, M.R.; Hoban, D.J.; Zhanel, G.G. Prevalence of antimicrobial resistance among clinical isolates of Bacteroides fragilis group in Canada in 2010-2011: CANWARD surveillance study. Antimicrob. Agents Chemother. 2011, 56, 1247–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yunoki, T.; Matsumura, Y.; Yamamoto, M.; Tanaka, M.; Hamano, K.; Nakano, S.; Noguchi, T.; Nagao, M.; Ichiyama, S.; Fujita, N.; et al. Genetic identification and antimicrobial susceptibility of clinically isolated anaerobic bacteria: A prospective multicenter surveillance study in Japan. Anaerobe 2017, 48, 215–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittelkötter, U. Antimicrobial Prophylaxis for Abdominal Surgery: Is There a Need for Metronidazole? J. Chemother. 2001, 13 (Suppl. 4), 27–34. [Google Scholar]
- Tan, T.Y.; Ng, L.S.Y.; Kwang, L.L.; Rao, S.; Eng, L.C. Clinical characteristics and antimicrobial susceptibilities of anaerobic bacteremia in an acute care hospital. Anaerobe 2017, 43, 69–74. [Google Scholar] [CrossRef]
- Veloo, A.C.M.; van Winkelhoff, A.J. Antibiotic susceptibility profiles of anaerobic pathogens in The Netherlands. Anaerobe 2015, 31, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Jamal, W.; Shahin, M.; Rotimi, V.O. Surveillance and trends of antimicrobial resistance among clinical isolates of anaerobes in Kuwait hospitals from 2002 to 2007. Anaerobe 2010, 16, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Cobo, F.; Borrego, J.; Gómez, E.; Casanovas, I.; Calatrava, E.; Foronda, C.; Navarro-Marí, J.M. Clinical Findings and Antimicrobial Susceptibility of Anaerobic Bacteria Isolated in Bloodstream Infections. Antibiotics 2020, 9, 345. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, M.P.; Towns, M.L.; Quartey, S.M.; Mirrett, S.; Reimer, L.G.; Parmigiani, G.; Reller, L.B. The Clinical Significance of Positive Blood Cultures in the 1990s: A Prospective Comprehensive Evaluation of the Microbiology, Epidemiology, and Outcome of Bacteremia and Fungemia in Adults. Clin. Infect. Dis. 1997, 24, 584–602. [Google Scholar] [CrossRef]
- EUCAST. Clinical Breakpoints and Dosing of Antibiotics. Available online: https://eucast.org/clinical_breakpoints/ (accessed on 4 November 2020).
- Tyson, G.H.; Li, C.; Ayers, S.; McDermott, P.F.; Zhao, S. Using whole-genome sequencing to determine appropriate streptomycin epidemiological cutoffs for Salmonella and Escherichia coli. FEMS Microbiol. Lett. 2016, 363, fnw009. [Google Scholar] [CrossRef] [Green Version]
- Ismail, N.A.; Omar, S.V.; Joseph, L.; Govender, N.; Blows, L.; Ismail, F.; Koornhof, H.; Dreyer, A.W.; Kaniga, K.; Ndjeka, N. Defining Bedaquiline Susceptibility, Resistance, Cross-Resistance and Associated Genetic Determinants: A Retrospective Cohort Study. EBioMedicine 2018, 28, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Turnidge, J.; Kahlmeter, G.; Kronvall, G. Statistical characterisation of bacterial wild-type MIC value distributions and the determination of epidemiological cut-off values. Clin. Microbiol. Infect. 2006, 12, 418–425. [Google Scholar] [CrossRef]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009. [Google Scholar]
- Kolde, R. pheatmap: Pretty Heatmaps. 2019. Available online: https://CRAN.R-project.org/package=pheatmap (accessed on 15 September 2020).




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badr, M.T.; Blümel, B.; Baumgartner, S.; Komp, J.M.A.; Häcker, G. Antimicrobial Susceptibility Patterns and Wild-Type MIC Distributions of Anaerobic Bacteria at a German University Hospital: A Five-Year Retrospective Study (2015–2019). Antibiotics 2020, 9, 823. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9110823
Badr MT, Blümel B, Baumgartner S, Komp JMA, Häcker G. Antimicrobial Susceptibility Patterns and Wild-Type MIC Distributions of Anaerobic Bacteria at a German University Hospital: A Five-Year Retrospective Study (2015–2019). Antibiotics. 2020; 9(11):823. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9110823
Chicago/Turabian StyleBadr, Mohamed Tarek, Benjamin Blümel, Sandra Baumgartner, Johanna M. A. Komp, and Georg Häcker. 2020. "Antimicrobial Susceptibility Patterns and Wild-Type MIC Distributions of Anaerobic Bacteria at a German University Hospital: A Five-Year Retrospective Study (2015–2019)" Antibiotics 9, no. 11: 823. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9110823