Time Trends and Factors Associated with Antibiotic Prescribing in Swiss Primary Care (2008 to 2020)

 ,
,  , and
, and
Abstract
:1. Introduction
2. Results
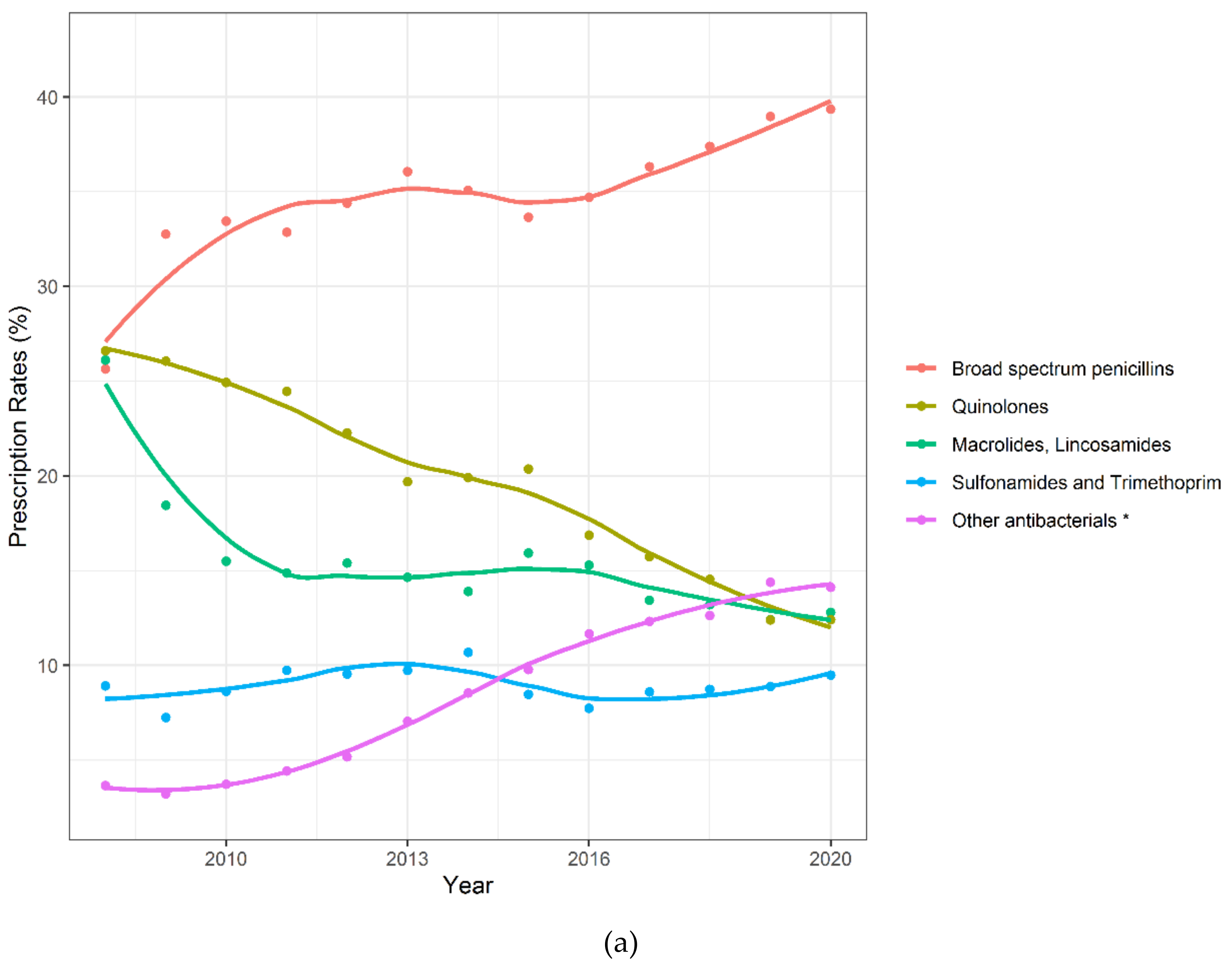
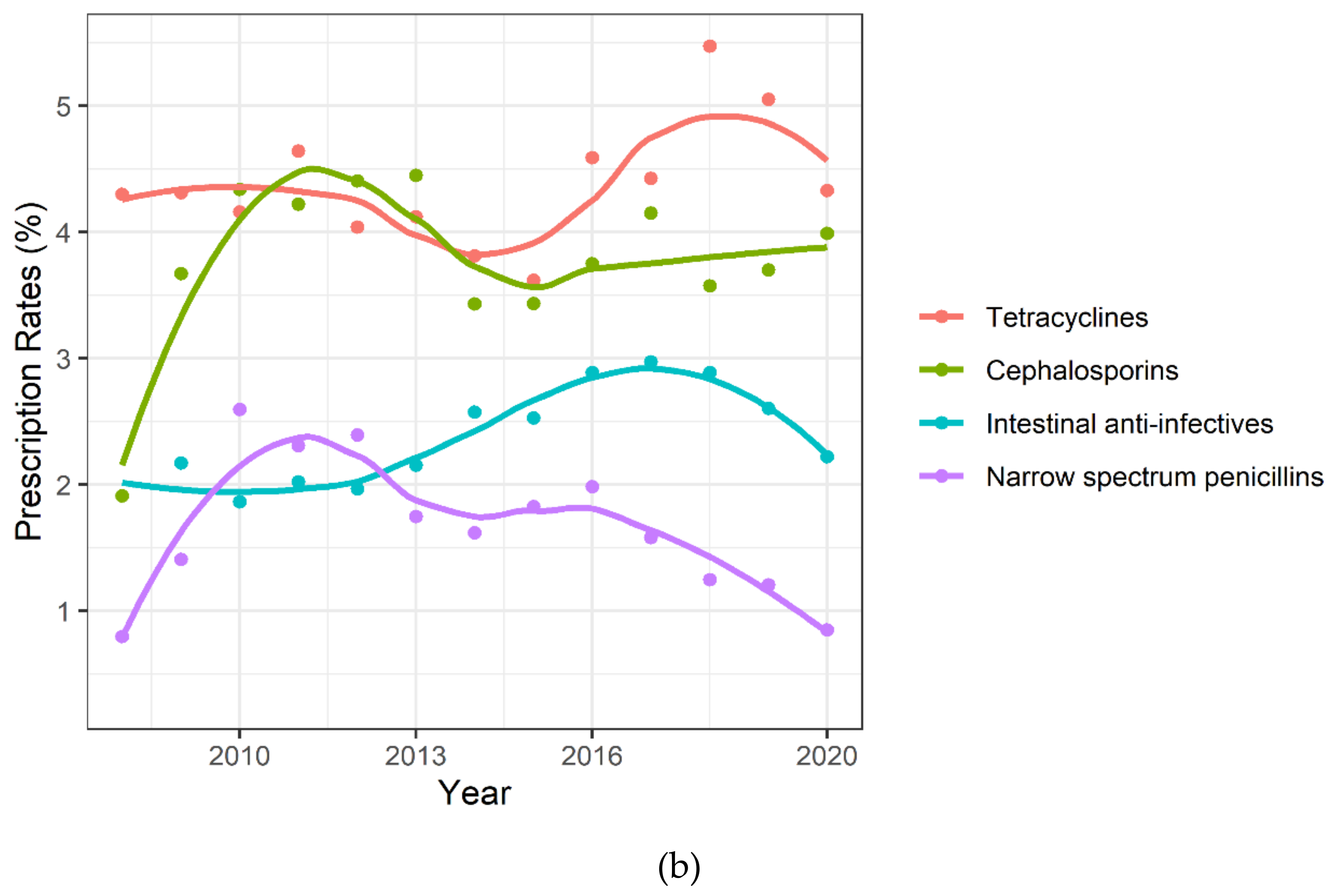
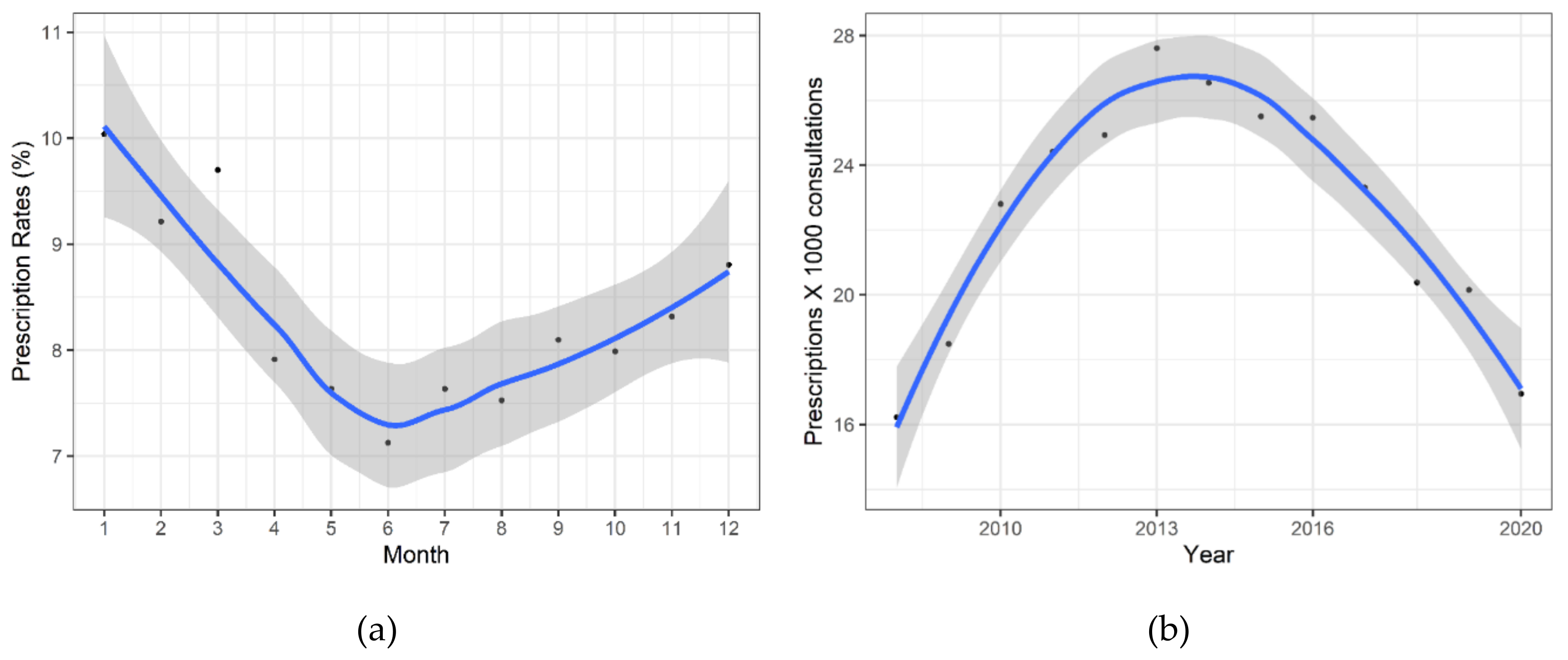
2.1. Patterns of Antibiotic Prescriptions
2.2. Subgroup Analysis
2.3. Multivariable and Sensitivity Analyses
3. Discussion
3.1. Factors Associated with Antibiotic Prescribing
3.2. Strengths and Limitations of the Study
3.3. Implications for Future Research, Policy and Practice
4. Materials and Methods
4.1. Study Design and Setting
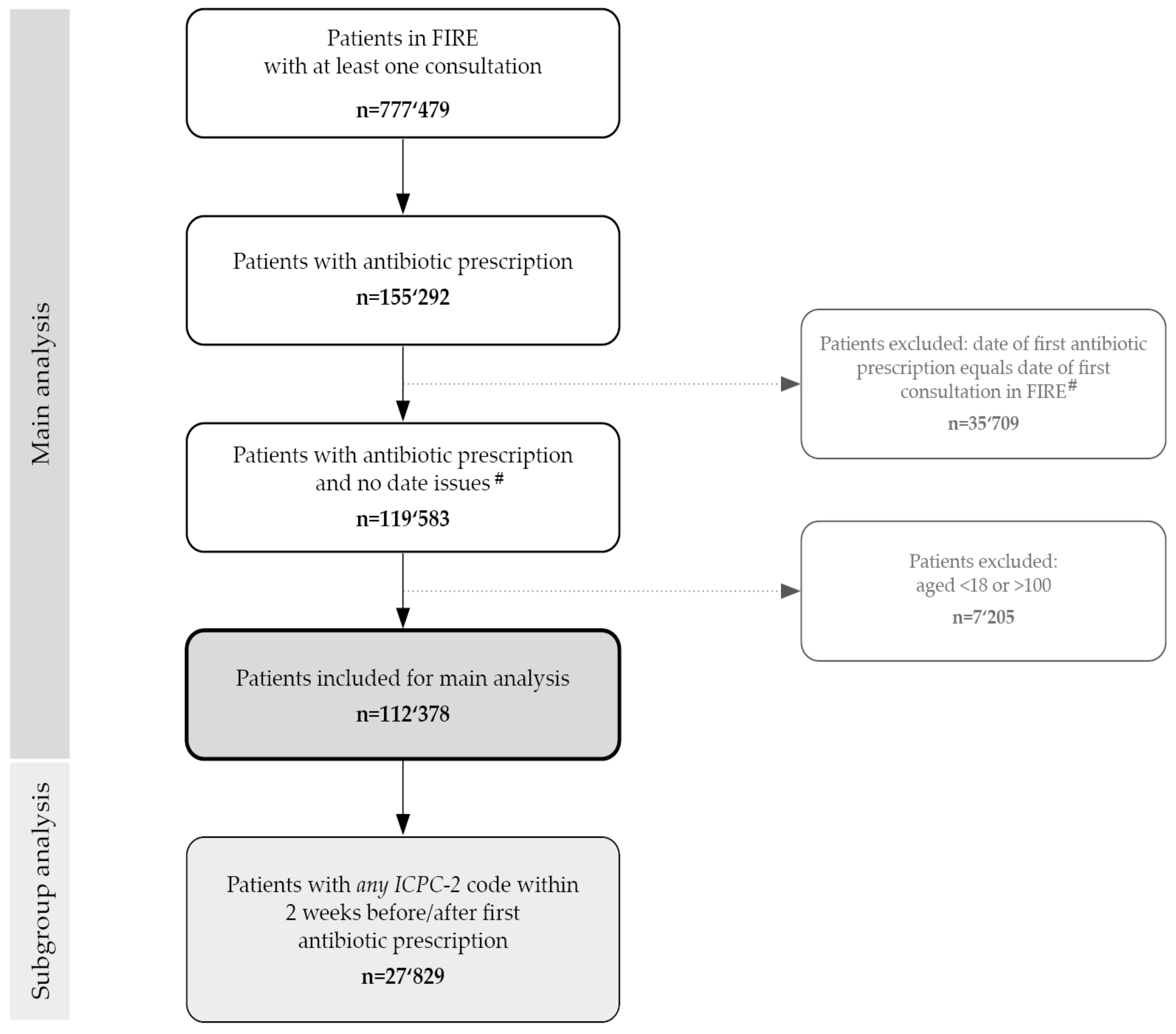
4.2. Participants’ Inclusion and Exclusion Criteria and Operational Definitions
4.3. Classification of Antibiotics and Diagnoses
4.4. Data Variables and Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the eu and the european economic area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, L.A.; Bartoces, M.G.; Roberts, R.M.; Suda, K.J.; Hunkler, R.J.; Taylor, T.H., Jr.; Schrag, S.J. Us outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clin. Infect. Dis. 2015, 60, 1308–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M. Outpatient antibiotic use in europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J.; Bartoces, M.; Enns, E.A.; File, T.M., Jr.; Finkelstein, J.A.; Gerber, J.S.; Hyun, D.Y.; Linder, J.A.; et al. Prevalence of inappropriate antibiotic prescriptions among us ambulatory care visits, 2010–2011. JAMA 2016, 315, 1864–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, e3463–e3470. [Google Scholar] [CrossRef] [Green Version]
- European Center for Disease Prevention and Control. Surveillance and disease data for antimicrobial consumption. Available online: https://www.Ecdc.Europa.Eu/en/antimicrobial-consumption/surveillance-and-disease-data (accessed on 17 September 2020).
- Interagency Coordination Group (IACG) on Antimicrobial Resistance. No time to wait: Securing the future from drug-resistant infections: Report to the secretary-general of the united nations. April 2019. Available online: https://www.Who.Int/docs/default-source/documents/no-time-to-wait-securing-the-future-from-drug-resistant-infections-en.Pdf?Sfvrsn=5b424d7_6 (accessed on 7 July 2020).
- World Health Organization. Global action plan on antimicrobial resistance; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Adriaenssens, N.; Coenen, S.; Versporten, A.; Muller, A.; Vankerckhoven, V.; Goossens, H. European surveillance of antimicrobial consumption (esac): Quality appraisal of antibiotic use in europe. J. Antimicrob. Chemother. 2011, 66, vi71–vi77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swiss Centre for Antibiotic Resistance—Anresis.ch. Meldungen Ausgewählter Multiresistenter Mikroorganismen in der Schweiz. Bern, Switzerland. In Informationsmagazin für Medizinische Fachpersonen und Medienschaffende; Bundesamt für Gesundheit BAG: Bern, Switzerland, 2020; pp. 8–9. Available online: http://www.anresis.ch (accessed on 11 August 2020).
- Centers for Disease Control and Prevention. Antibiotic use in outpatient settings, 2017: Antibiotic use by healthcare setting. Available online: https://www.Cdc.Gov/antibiotic-use/stewardship-report/outpatient.Html (accessed on 17 September 2020).
- King, L.M.; Fleming-Dutra, K.E.; Hicks, L.A. Advances in optimizing the prescription of antibiotics in outpatient settings. BMJ 2018, 363, k3047. [Google Scholar] [CrossRef]
- ANRESIS. Swiss Antibiotic Resistance Report 2018: Usage of Antibiotics and Occurrence of Antibiotic Resistance in Bacteria from Humans and Animals in Switzerland. Available online: https://www.Bundespublikationen.Admin.Ch/cshop_mimes_bbl/8c/8cdcd4590ee41ed8b9c944668445697e.Pdf (accessed on 17 September 2020).
- Federal Office of Public Health (FOPH). What is the Total Consumption of Antibiotics? Available online: https://www.Bag.Admin.Ch/bag/en/home/krankheiten/infektionskrankheiten-bekaempfen/antibiotikaresistenzen/wie-entwickelt-sich-die-antibiotikaresistenzlage-.Html (accessed on 7 July 2020).
- European Centre for Disease Prevention and Control (ECDC). Summary of the Latest Data on Antibiotic Consumption in the European Union. Esac-net surveillance data. Available online: https://www.Ecdc.Europa.Eu/en/publications-data/summary-latest-data-antibiotic-consumption-eu-2018 (accessed on 11 August 2020).
- Schweizerische Gesundheitsobservatorium (Obsan). Ärztinnen und Ärzte in Freier Praxis. Dichte der Ärztinnen und Ärzte in Freier Praxis—2017. Available online: Https://www.Obsan.Admin.Ch/de/indikatoren/aerztinnen-und-aerzte-freier-praxis (accessed on 11 August 2020).
- Zweigner, J.; Meyer, E.; Gastmeier, P.; Schwab, F. Rate of antibiotic prescriptions in german outpatient care—Are the guidelines followed or are they still exceeded? GMS Hyg. Infect. Control 2018, 13, Doc04. [Google Scholar]
- Edelstein, M.; Agbebiyi, A.; Ashiru-Oredope, D.; Hopkins, S. Trends and patterns in antibiotic prescribing among out-of-hours primary care providers in England, 2010–14. J. Antimicrob. Chemother. 2017, 72, 3490–3495. [Google Scholar] [CrossRef]
- Plate, A.; Kronenberg, A.; Risch, M.; Mueller, Y.; Di Gangi, S.; Rosemann, T.; Senn, O. Treatment of urinary tract infections in swiss primary care: Quality and determinants of antibiotic prescribing. BMC Fam. Pract. 2020, 21, 125. [Google Scholar] [CrossRef] [PubMed]
- Glinz, D.; Leon Reyes, S.; Saccilotto, R.; Widmer, A.F.; Zeller, A.; Bucher, H.C.; Hemkens, L.G. Quality of antibiotic prescribing of swiss primary care physicians with high prescription rates: A nationwide survey. J. Antimicrob. Chemother. 2017, 72, 3205–3212. [Google Scholar] [CrossRef] [PubMed]
- Streit, S.; Frey, P.; Singer, S.; Bollag, U.; Meli, D.N. Clinical and haematological predictors of antibiotic prescribing for acute cough in adults in swiss practices—An observational study. BMC Fam. Pract. 2015, 16, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achermann, R.; Suter, K.; Kronenberg, A.; Gyger, P.; Muhlemann, K.; Zimmerli, W.; Bucher, H.C. Antibiotic use in adult outpatients in switzerland in relation to regions, seasonality and point of care tests. Clin. Microbiol. Infect. 2011, 17, 855–861. [Google Scholar] [CrossRef] [Green Version]
- Briel, M.; Young, J.; Tschudi, P.; Hersberger, K.E.; Hugenschmidt, C.; Langewitz, W.; Bucher, H.C. Prevalence and influence of diagnostic tests for acute respiratory tract infections in primary care. Swiss Med. Wkly. 2006, 136, 248–253. [Google Scholar]
- Chmiel, C.; Bhend, H.; Senn, O.; Zoller, M.; Rosemann, T. The fire project: A milestone for research in primary care in switzerland. Swiss Med. Wkly. 2011, 140, w13142. [Google Scholar]
- European Center for Disease Prevention and Control. Surveillance Report: Antimicrobial Consumption in the eu/eea, Annual Epidemiological Report for 2018: Distribution by Antimicrobiall Group. Available online: https://www.Ecdc.Europa.Eu/en/antimicrobial-consumption/database/distribution-by-antimicrobial-group (accessed on 20 September 2020).
- World Health Organisation. Aware—A New Who Tool to Help Countries Improve Antibiotic Treatment, Increase Access and Reduce Resistance. 2019. Available online: https://adoptaware.Org/ (accessed on 11 August 2020).
- European Center for Disease Prevention and Control. Surveillance Report: Antimicrobial Consumption in the eu/eea, Annual Epidemiological Report for 2018: Trend of Antimicrobial Consumption by Country. Available online: https://www.Ecdc.Europa.Eu/en/antimicrobial-consumption/database/trend-country (accessed on 17 September 2020).
- Public Health England. English Surveillance Programme for Antimicrobial Utilisation and Resistance (espaur). Report 2018–2019. Available online: https://www.Gov.Uk/government/publications/english-surveillance-programme-antimicrobial-utilisation-and-resistance-espaur-report (accessed on 20 September 2020).
- Selby, K.; Gaspoz, J.-M.; Rodondi, N.; Neuner-Jehle, S.; Perrier, A.; Zeller, A.; Cornuz, J. Creating a list of low-value health care activities in swiss primary care. JAMA Intern. Med. 2015, 175, 640–642. [Google Scholar] [CrossRef] [Green Version]
- Federal Office of Public Health and Federal Food Safety and Veterinary Office and the Strategy on Antibiotic Resistance (StAR). Swiss Antibiotic Resistance Report 2018. Usage of antibiotics And Occurrence of Antibiotic Resistance in Bacteria from Humans and Animals in Switzerland. 2018. Available online: http://www.Anresis.Ch/files/pdf/bag_swiss_antibiotic_resistance_report_2016_web.pdf (accessed on 11 August 2020).
- Shively, N.R.; Buehrle, D.J.; Clancy, C.J.; Decker, B.K. Prevalence of inappropriate antibiotic prescribing in primary care clinics within a veterans affairs health care system. Antimicrob. Agents Chemother. 2018, 62, e00337-18. [Google Scholar] [CrossRef] [Green Version]
- Petersen, I.; Hayward, A.C. Antibacterial prescribing in primary care. J. Antimicrob. Chemother. 2007, 60, i43–i47. [Google Scholar] [CrossRef] [Green Version]
- DemoSCOPE. Survey on Antimicrobial Resistance Commissioned by the Federal Office of Public Health. September 2016. Available online: https://www.Star.Admin.Ch/star/en/home/star/brennpunkte/brennpunkt-zwei.Html (accessed on 7 June 2020).
- Havers, F.P.; Hicks, L.A.; Chung, J.R.; Gaglani, M.; Murthy, K.; Zimmerman, R.K.; Jackson, L.A.; Petrie, J.G.; McLean, H.Q.; Nowalk, M.P.; et al. Outpatient antibiotic prescribing for acute respiratory infections during influenza seasons. JAMA Netw. Open 2018, 1, e180243. [Google Scholar] [CrossRef]
- Dekker, A.R.; Verheij, T.J.; van der Velden, A.W. Inappropriate antibiotic prescription for respiratory tract indications: Most prominent in adult patients. Fam. Pract. 2015, 32, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Schroeck, J.L.; Ruh, C.A.; Sellick, J.A., Jr.; Ott, M.C.; Mattappallil, A.; Mergenhagen, K.A. Factors associated with antibiotic misuse in outpatient treatment for upper respiratory tract infections. Antimicrob. Agents Chemother. 2015, 59, 3848–3852. [Google Scholar] [CrossRef] [Green Version]
- Gebeyehu, E.; Bantie, L.; Azage, M. Inappropriate use of antibiotics and its associated factors among urban and rural communities of bahir dar city administration, northwest ethiopia. PLoS ONE 2015, 10, e0138179. [Google Scholar] [CrossRef] [PubMed]
- Elseviers, M.M.; Ferech, M.; Vander Stichele, R.H.; Goossens, H. Antibiotic use in ambulatory care in europe (esac data 1997–2002): Trends, regional differences and seasonal fluctuations. Pharmacoepidemiol. Drug Saf. 2007, 16, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Ferech, M.; Coenen, S.; Malhotra-Kumar, S.; Dvorakova, K.; Hendrickx, E.; Suetens, C.; Goossens, H. European surveillance of antimicrobial consumption (esac): Outpatient antibiotic use in europe. J. Antimicrob. Chemother. 2006, 58, 401–407. [Google Scholar] [CrossRef]
- Suda, K.J.; Hicks, L.A.; Roberts, R.M.; Hunkler, R.J.; Taylor, T.H. Trends and seasonal variation in outpatient antibiotic prescription rates in the united states, 2006 to 2010. Antimicrob. Agents Chemother. 2014, 58, 2763–2766. [Google Scholar] [CrossRef] [Green Version]
- Curtis, H.J.; Walker, A.J.; Mahtani, K.R.; Goldacre, B. Time trends and geographical variation in prescribing of antibiotics in england 1998–2017. J. Antimicrob. Chemother. 2018, 74, 242–250. [Google Scholar] [CrossRef]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.A.; Laxminarayan, R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- Jones, B.E.; Sauer, B.; Jones, M.M.; Campo, J.; Damal, K.; He, T.; Ying, J.; Greene, T.; Goetz, M.B.; Neuhauser, M.M.; et al. Variation in outpatient antibiotic prescribing for acute respiratory infections in the veteran population: A cross-sectional study. Ann. Intern. Med. 2015, 163, 73–80. [Google Scholar] [CrossRef]
- Gjelstad, S.; Straand, J.; Dalen, I.; Fetveit, A.; Strøm, H.; Lindbæk, M. Do general practitioners’ consultation rates influence their prescribing patterns of antibiotics for acute respiratory tract infections? J. Antimicrob. Chemother. 2011, 66, 2425–2433. [Google Scholar] [CrossRef] [Green Version]
- Akkerman, A.E.; Kuyvenhoven, M.M.; van der Wouden, J.C.; Verheij, T.J. Prescribing antibiotics for respiratory tract infections by gps: Management and prescriber characteristics. Br. J. Gen. Pract. 2005, 55, 114–118. [Google Scholar] [PubMed]
- Cadieux, G.; Tamblyn, R.; Dauphinee, D.; Libman, M. Predictors of inappropriate antibiotic prescribing among primary care physicians. Cmaj. 2007, 177, 877–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selby, K.; Cornuz, J.; Cohidon, C.; Gaspoz, J.-M.; Senn, N. How do swiss general practitioners agree with and report adhering to a top-five list of unnecessary tests and treatments? Results of a cross-sectional survey. Eur. J. Gen. Pract. 2018, 24, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Saliba-Gustafsson, E.A.; Dunberger Hampton, A.; Zarb, P.; Orsini, N.; Borg, M.A.; Stålsby Lundborg, C. Factors associated with antibiotic prescribing in patients with acute respiratory tract complaints in malta: A 1-year repeated cross-sectional surveillance study. BMJ Open 2019, 9, e032704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haeseker, M.B.; Dukers-Muijrers, N.H.T.M.; Hoebe, C.J.P.A.; Bruggeman, C.A.; Cals, J.W.L.; Verbon, A. Trends in antibiotic prescribing in adults in dutch general practice. PLoS ONE 2012, 7, e51860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, G.C.; Reveles, K.R.; Attridge, R.T.; Lawson, K.A.; Mansi, I.A.; Lewis, J.S.; Frei, C.R. Outpatient antibiotic prescribing in the united states: 2000 to 2010. BMC Med. 2014, 12, 96. [Google Scholar] [CrossRef] [Green Version]
- Dallas, A.; Magin, P.; Morgan, S.; Tapley, A.; Henderson, K.; Ball, J.; Scott, J.; Spike, N.; McArthur, L.; van Driel, M. Antibiotic prescribing for respiratory infections: A cross-sectional analysis of the recent study exploring the habits of early-career doctors in primary care. Fam. Pract. 2014, 32, 49–55. [Google Scholar] [CrossRef] [Green Version]
- The White House. National Action Plan for Combating Antibiotic-Resistant Bacteria. 2015: Washington. Available online: https://obamawhitehouse.Archives.Gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.Pdf (accessed on 11 August 2020).
- Tamma, P.D.; Miller, M.A.; Cosgrove, S.E. Rethinking how antibiotics are prescribed: Incorporating the 4 moments of antibiotic decision making into clinical practice. JAMA 2019, 321, 139–140. [Google Scholar] [CrossRef]
- Guideline: Akute Bakterielle Sinusitis (d). Available online: https://ssi.Guidelines.Ch/guideline/2410 (accessed on 17 September 2020).
- Guideline: Pharyngitis (d). Available online: https://ssi.Guidelines.Ch/guideline/240 (accessed on 20 September 2020).
- Patel, A.; Pfoh, E.R.; Misra Hebert, A.D.; Chaitoff, A.; Shapiro, A.; Gupta, N.; Rothberg, M.B. Attitudes of high versus low antibiotic prescribers in the management of upper respiratory tract infections: A mixed methods study. J. Gen. Intern. Med. 2020, 35, 1182–1188. [Google Scholar] [CrossRef]
- Smith, D.R.M.; Dolk, F.C.K.; Smieszek, T.; Robotham, J.V.; Pouwels, K.B. Understanding the gender gap in antibiotic prescribing: A cross-sectional analysis of english primary care. BMJ Open 2018, 8, e020203. [Google Scholar] [CrossRef] [Green Version]
- WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for the Anatomical Therapeutic Chemical Classification (atc) and Defined Daily Doses (ddd) Assignment 2020; WHO Collaborating Centre for Drug Statistics Methodology: Oslo, Norway, 2019. [Google Scholar]
- Who International Classification of Primary Care, Second Edition (icpc-2). Available online: http://www.Who.Int/classifications/icd/adaptations/icpc2/en/ (accessed on 9 May 2020).
- Lorenz, M.O. Methods of measuring the concentration of wealth. Publ. Am. Stat. Assoc. 1905, 9, 209–219. [Google Scholar] [CrossRef]
- Luebnker, M. Inequality, Income Shares and Poverty: The Practical Meaning of Gini Coefficients. In Travail Policy Brief no. 3. June 2010. Conditions of Work and Employment Programme (Travail), International Labour Office. Available online: https://www.Ilo.Org/wcmsp5/groups/public/-ed_protect--protrav/-travail/documents/publication/wcms_145695.Pdf (accessed on 20 September 2020).
- R core team. R: A language and environment for statistical computing. In R foundation for Statistical Computing, Editor; R core team: Vienna, Austria, 2018. [Google Scholar]
- Rachamin, Y.; Meier, R.; Grischott, T.; Rosemann, T.; Markun, S. General practitioners’ consultation counts and associated factors in swiss primary care—A retrospective observational study. PLoS ONE 2019, 14, e0227280. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class Number, n | Antibiotic Class | Prescriptions, n (%) |
|---|---|---|
| 1 | Broad spectrum penicillins | 75,534 (36.5) |
| 2 | Fluoroquinolones | 33,900 (16.4) |
| 3 | Macrolides, Lincosamides | 28,589 (13.8) |
| 4 | Other antibacterials 1 | 23,268 (11.3) |
| 5 | Sulfonamides and Trimethoprim | 18,380 (8.9) |
| 6 | Tetracyclines | 9670 (4.7) |
| 7 | Cephalosporins | 7886 (3.8) |
| 8 | Intestinal antiinfectives 2 | 5364 (2.6) |
| 9 | Narrow spectrum penicillins | 3160 (1.5) |
| 10 | Antimycobacterials | 732 (0.4) |
| 11 | Carbapenems | 53 (0.0) |
| 12 | Glycopeptides | 45 (0.0) |
| 13 | Aminoglycosides | 17 (0.0) |
| 14 | Monobactams | 1 (0.0) |
| Clinical Indications | ICPC-2 Code 1 | Prescriptions, n |
|---|---|---|
| Respiratory tract | 11,039 | |
| Upper respiratory tract infections | R74 | 2516 |
| Pneumonia | R81 | 1777 |
| Acute/chronic sinusitis | R75 | 1664 |
| Cough | R05 | 1404 |
| Acute Tonsillitis | R76 | 1271 |
| Acute Bronchitis / Bronchiolitis | R78 | 973 |
| Throat symptoms | R21 | 720 |
| Streptococci pharyngitis | R72 | 714 |
| Urinary tract infection | U71 | 5898 |
| Skin infection | S76 | 1000 |
| Diverticulosis / Diverticulitis | D92 | 971 |
| Abdominal Pain | D06 | 599 |
| Fever | A03 | 571 |
| Insect bite | S12 | 550 |
| Acute otitis media | H71 | 549 |
| Infectious Diseases | ICPC Category 1 | Overall Prescriptions, n | Overall Prescriptions, % |
|---|---|---|---|
| 21,021 | 100 | ||
| Respiratory | R71-83 | 9968 | 47.4 |
| Urological | U70-72 | 6514 | 31.0 |
| Skin | S03,09-11,70-76, 84, 95 | 1409 | 6.7 |
| Ear | H70-74 | 926 | 4.4 |
| Digestive system | D70-73 | 847 | 4.0 |
| Male genital | Y70-76 | 503 | 2.4 |
| General and unspecified | A70-78 | 467 | 2.2 |
| Eye | F70-73 | 169 | 0.8 |
| Musculoskeletal | L70 | 78 | 0.4 |
| Female genital | X70-74, 90-92 | 80 | 0.4 |
| Blood, Blood Forming Organs and Immune Mechanism | B70-71 | 29 | 0.1 |
| Cardiovascular | K70-71 | 16 | 0.1 |
| Neurological | N70-73 | 11 | 0.1 |
| Endocrine/Metabolic and Nutritional | T70 | 4 | 0.0 |
| Predictor (Reference, Where Applicable) | Univariable Analysis | Multivariable Analysis n = 26,589, GPs = 240 | |||
|---|---|---|---|---|---|
| Prescriptions and GPs, n | Estimates (95% CI) | p | Estimates (95% CI) | p | |
| GP Characteristics | ICC = 0.09 | ||||
| Age | n = 26,595, GP = 240 | 0.005 (−0.001, 0.011) | 0.080 | ||
| N. consultations ≥ 6000 (<6000) | n = 26,595, GP = 240 | 0.355 (0.252, 0.457) | <0.001 | 0.281 (0.163, 0.398) | <0.001 |
| Female gender (male) | n = 26,595, GP = 240 | −0.205 (−0.316, −0.094) | <0.001 | −0.079 (−0.199, 0.042) | 0.204 |
| Years in practice | n = 22,808, GP = 204 | 0.006 (−0.0004, 0.012 ) | 0.068 | ||
| Self-Employed (employee) | n = 24,604, GP = 216 | 0.089 (−0.035, 0.213) | 0.161 | ||
| Employment level (100%) | n = 26,595, GP = 240 | ||||
| <50% | −0.483 (−0.694, −0.266) | <0.001 | −0.279 (−0.507, −0.051) | 0.017 | |
| 50–79% | −0.271 (−0.400, −0.143) | <0.001 | −0.100 (−0.247, 0.047) | 0.183 | |
| 80–99% | −0.096 (−0.235, 0.044) | 0.179 | −0.058 (−0.193, 0.077) | 0.402 | |
| Practice Characteristics | |||||
| Type of practice (single practice) | n = 26,595, GP = 240 | ||||
| Double practice | −0.136 (−0.451, 0.179) | 0.399 | |||
| Group practice | −0.086 (−0.247, 0.075) | 0.297 | |||
| Patient Characteristics | |||||
| Age | n = 26,595, GP = 240 | 0.002 (0.001, 0.003) | <0.001 | 0.002 (0.001, 0.003) | <0.001 |
| Male gender (female) * | n = 26,589, GP = 240 | −0.231 (−0.270, −0.193) | <0.001 | −0.234 (−0.272, −0.196) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-González, N.A.; Di Gangi, S.; Pichierri, G.; Neuner-Jehle, S.; Senn, O.; Plate, A. Time Trends and Factors Associated with Antibiotic Prescribing in Swiss Primary Care (2008 to 2020). Antibiotics 2020, 9, 837. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9110837
Martínez-González NA, Di Gangi S, Pichierri G, Neuner-Jehle S, Senn O, Plate A. Time Trends and Factors Associated with Antibiotic Prescribing in Swiss Primary Care (2008 to 2020). Antibiotics. 2020; 9(11):837. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9110837
Chicago/Turabian StyleMartínez-González, Nahara Anani, Stefania Di Gangi, Giuseppe Pichierri, Stefan Neuner-Jehle, Oliver Senn, and Andreas Plate. 2020. "Time Trends and Factors Associated with Antibiotic Prescribing in Swiss Primary Care (2008 to 2020)" Antibiotics 9, no. 11: 837. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9110837