Effectiveness and Acceptance of Multimodal Antibiotic Stewardship Program: Considering Progressive Implementation and Complementary Strategies

Abstract
:1. Introduction
2. Results
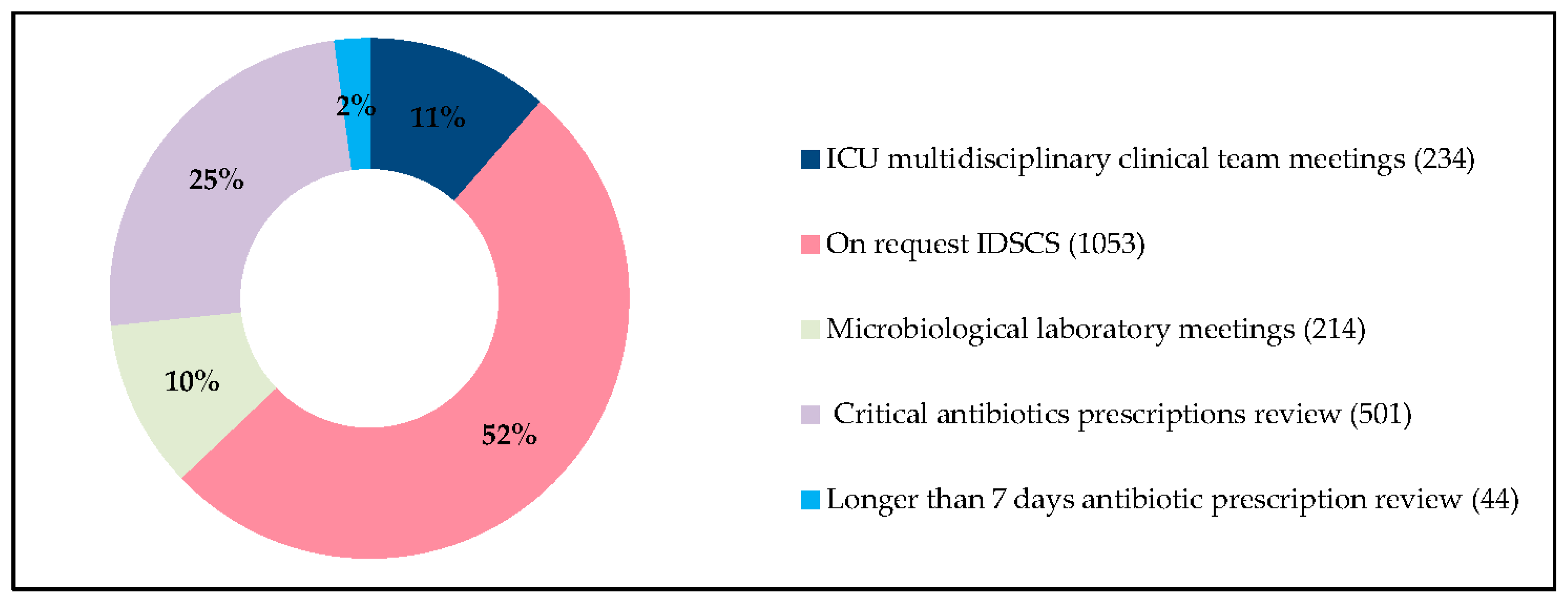
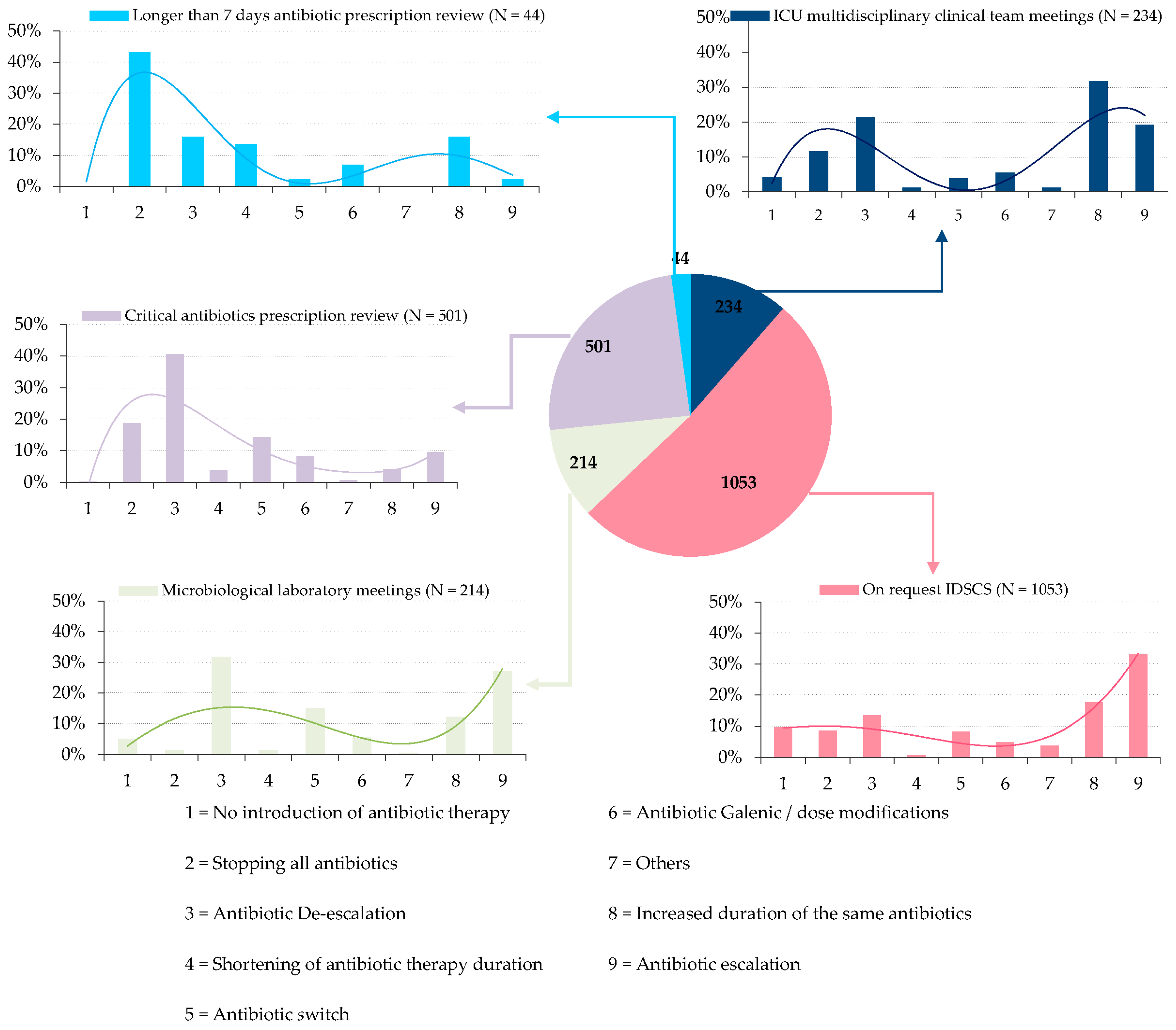
2.1. Interventions Complementarity
2.2. Impact on Mortality, 30-Day Readmission Rate, and Mean Length of Stay
2.3. Impact on Antibiotic Consumption
2.4. User Experience Assessment: Satisfaction Survey
3. Discussion
4. Materials and Methods
4.1. Study Setting and Interventions
4.2. Outcomes
4.3. User Experience Assessment
4.4. Statistical Approach
4.5. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Publications|AMR Review. Available online: https://amr-review.org/Publications.html (accessed on 29 August 2019).
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance-the need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [Green Version]
- Rieg, S.; Küpper, M.F. Infectious diseases consultations can make the difference: A brief review and a plea for more infectious diseases specialists in Germany. Infection 2016, 44, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Carling, P.; Fung, T.; Killion, A.; Terrin, N.; Barza, M. Favorable impact of a multidisciplinary antibiotic management program conducted during 7 years. Infect. Control. Hosp. Epidemiol. 2003, 24, 699–706. [Google Scholar] [CrossRef]
- DiazGranados, C.A. Prospective audit for antimicrobial stewardship in intensive care: Impact on resistance and clinical outcomes. Am. J. Infect. Control. 2012, 40, 526–529. [Google Scholar] [CrossRef]
- Karanika, S.; Paudel, S.; Grigoras, C.; Kalbasi, A.; Mylonakis, E. Systematic Review and Meta-analysis of Clinical and Economic Outcomes from the Implementation of Hospital-Based Antimicrobial Stewardship Programs. Antimicrob. Agents Chemother. 2016, 60, 4840–4852. [Google Scholar] [CrossRef] [Green Version]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- Kim, J.; Joo, E.-J.; Ha, Y.E.; Park, S.Y.; Kang, C.-I.; Chung, D.R.; Song, J.-H.; Peck, K.R. Impact of a computerized alert system for bacteremia notification on the appropriate antibiotic treatment of Staphylococcus aureus bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 937–945. [Google Scholar] [CrossRef]
- Bai, A.D.; Showler, A.; Burry, L.; Steinberg, M.; Ricciuto, D.R.; Fernandes, T.; Chiu, A.; Raybardhan, S.; Science, M.; Fernando, E.; et al. Impact of Infectious Disease Consultation on Quality of Care, Mortality, and Length of Stay in Staphylococcus aureus Bacteremia: Results From a Large Multicenter Cohort Study. Clin. Infect. Dis. 2015, 60, 1451–1461. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, S.; McQuillen, D.P.; Nahass, R.; Martinelli, L.; Rubin, M.; Schwebke, K.; Petrak, R.; Ritter, J.T.; Chansolme, D.; Slama, T.; et al. Infectious diseases specialty intervention is associated with decreased mortality and lower healthcare costs. Clin. Infect. Dis. 2014, 58, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Cunha, C.B. The Pharmacoeconomic Aspects of Antibiotic Stewardship Programs. Med. Clin. North Am. 2018, 102, 937–946. [Google Scholar] [CrossRef]
- Abbara, S.; Pitsch, A.; Jochmans, S.; Hodjat, K.; Cherrier, P.; Monchi, M.; Vinsonneau, C.; Diamantis, S. Impact of a multimodal strategy combining a new standard of care and restriction of carbapenems, fluoroquinolones and cephalosporins on antibiotic consumption and resistance of Pseudomonas aeruginosa in a French intensive care unit. Int. J. Antimicrob. Agents 2019, 53, 416–422. [Google Scholar] [CrossRef]
- Dyar, O.J.; Tebano, G.; Pulcini, C.; ESGAP (ESCMID Study Group for Antimicrobial StewardshiP). Managing responsible antimicrobial use: Perspectives across the healthcare system. Clin. Microbiol. Infect. 2017, 23, 441–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parente, D.M.; Morton, J. Role of the Pharmacist in Antimicrobial Stewardship. Med. Clin. North Am. 2018, 102, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Carlet, J.; Le Coz, P. Proposals of the Special Working Group for Keeping Antibiotics Effective; ESCMID: Basel, Switzerland, 2015; 150p. [Google Scholar]
- Pulcini, C.; Morel, C.M.; Tacconelli, E.; Beovic, B.; de With, K.; Goossens, H.; Harbarth, S.; Holmes, A.; Howard, P.; Morris, A.M.; et al. Human resources estimates and funding for antibiotic stewardship teams are urgently needed. Clin. Microbiol. Infect. 2017, 23, 785–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amann, S.; Neef, K.; Kohl, S. Antimicrobial resistance (AMR). Eur. J. Hosp. Pharm. Sci. Prac. 2019, 26, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Binda, F.; Tebano, G.; Kallen, M.C.; Ten Oever, J.; Hulscher, M.E.; Schouten, J.A.; Pulcini, C. Nationwide survey of hospital antibiotic stewardship programs in France. Med. Mal. Infect. 2020, 50, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Dyar, O.J.; Nathwani, D.; Monnet, D.L.; Gyssens, I.C.; Stålsby Lundborg, C.; Pulcini, C.; ESGAP Student-PREPARE Working Group. Do medical students feel prepared to prescribe antibiotics responsibly? Results from a cross-sectional survey in 29 European countries. J. Antimicrob. Chemother. 2018, 73, 2236–2242. [Google Scholar] [CrossRef]
- Mehta, J.M.; Haynes, K.; Wileyto, E.P.; Gerber, J.S.; Timko, D.R.; Morgan, S.C.; Binkley, S.; Fishman, N.O.; Lautenbach, E.; Zaoutis, T.; et al. Comparison of prior authorization and prospective audit with feedback for antimicrobial stewardship. Infect. Control. Hosp. Epidemiol. 2014, 35, 1092–1099. [Google Scholar] [CrossRef] [Green Version]
- Cosgrove, S.E.; Seo, S.K.; Bolon, M.K.; Sepkowitz, K.A.; Climo, M.W.; Diekema, D.J.; Speck, K.; Gunaseelan, V.; Noskin, G.A.; Herwaldt, L.A.; et al. Evaluation of postprescription review and feedback as a method of promoting rational antimicrobial use: A multicenter intervention. Infect. Control. Hosp. Epidemiol. 2012, 33, 374–380. [Google Scholar] [CrossRef]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Pollack, L.A.; Srinivasan, A. Core elements of hospital antibiotic stewardship programs from the Centers for Disease Control and Prevention. Clin. Infect. Dis. 2014, 59 (Suppl. 3), S97–S100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulcini, C.; Binda, F.; Lamkang, A.S.; Trett, A.; Charani, E.; Goff, D.A.; Harbarth, S.; Hinrichsen, S.L.; Levy-Hara, G.; Mendelson, M.; et al. Developing core elements and checklist items for global hospital antimicrobial stewardship programmes: A consensus approach. Clin. Microbiol. Infect. 2019, 25, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Buckel, W.R.; Veillette, J.J.; Vento, T.J.; Stenehjem, E. Antimicrobial Stewardship in Community Hospitals. Med. Clin. N. Am. 2018, 102, 913–928. [Google Scholar] [CrossRef] [PubMed]
- Bishop, B.M. Antimicrobial Stewardship in the Emergency Department: Challenges, Opportunities, and a Call to Action for Pharmacists. J. Pharm. Prac. 2016, 29, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Morrill, H.J.; Gaitanis, M.M.; LaPlante, K.L. Antimicrobial stewardship program prompts increased and earlier infectious diseases consultation. Antimicrob. Resist. Infect. Control. 2014, 3, 12. [Google Scholar] [CrossRef] [Green Version]
- Tamma, P.D.; Avdic, E.; Keenan, J.F.; Zhao, Y.; Anand, G.; Cooper, J.; Dezube, R.; Hsu, S.; Cosgrove, S.E. What is the More Effective Antibiotic Stewardship Intervention: Preprescription Authorization or Postprescription Review with Feedback? Clin. Infect. Dis. 2017, 64, 537–543. [Google Scholar] [CrossRef]
- Vaughn, V.M.; Gandhi, T.; Conlon, A.; Chopra, V.; Malani, A.N.; Flanders, S.A. The Association of Antibiotic Stewardship With Fluoroquinolone Prescribing in Michigan Hospitals: A Multi-hospital Cohort Study. Clin. Infect. Dis. 2019, 69, 1269–1277. [Google Scholar] [CrossRef] [Green Version]
- Sasikumar, M.; Boyer, S.; Remacle-Bonnet, A.; Ventelou, B.; Brouqui, P. The value of specialist care-infectious disease specialist referrals-why and for whom? A retrospective cohort study in a French tertiary hospital. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 625–633. [Google Scholar] [CrossRef]
- Pulcini, C.; Gyssens, I.C. How to educate prescribers in antimicrobial stewardship practices. Virulence 2013, 4, 192–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Baño, J.; Pérez-Moreno, M.A.; Peñalva, G.; Garnacho-Montero, J.; Pinto, C.; Salcedo, I.; Fernández-Urrusuno, R.; Neth, O.; Gil-Navarro, M.V.; Pérez-Milena, A.; et al. Outcomes of the PIRASOA programme, an antimicrobial stewardship programme implemented in hospitals of the Public Health System of Andalusia, Spain: An ecologic study of time-trend analysis. Clin. Microbiol. Infect. 2020, 26, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Weber, B.R.; Noble, B.N.; Bearden, D.T.; Crnich, C.J.; Ellingson, K.D.; McGregor, J.C.; Furuno, J.P. Antibiotic Prescribing upon Discharge from the Hospital to Long-Term Care Facilities: Implications for Antimicrobial Stewardship Requirements in Post-Acute Settings. Infect. Control. Hosp. Epidemiol. 2019, 40. [Google Scholar] [CrossRef] [Green Version]
- Scarpato, S.J.; Timko, D.R.; Cluzet, V.C.; Dougherty, J.P.; Nunez, J.J.; Fishman, N.O.; Hamilton, K.W.; CDC Prevention Epicenters Program. An Evaluation of Antibiotic Prescribing Practices upon Hospital Discharge. Infect. Control. Hosp. Epidemiol. 2017, 38, 353–355. [Google Scholar] [CrossRef]
- Morquin, D.; Ologeanu-Taddei, R.; Koumar, Y.; Reynes, J. Tele-Expertise System Based on the Use of the Electronic Patient Record to Support Real-Time Antimicrobial Use. Int. J. Technol. Assess. Health Care 2018, 34, 156–162. [Google Scholar] [CrossRef]
- Boussat, S.; Demoré, B.; Lozniewski, A.; Aissa, N.; Rabaud, C. How to improve the collection and analysis of hospital antibiotic consumption: Preliminary results of the ConsoRes software experimental implementation. Med. Mal. Infect. 2012, 42, 154–160. [Google Scholar] [CrossRef]
- Howard, P.; Pulcini, C.; Levy Hara, G.; West, R.M.; Gould, I.M.; Harbarth, S.; Nathwani, D.; ESCMID Study Group for Antimicrobial Policies (ESGAP); ISC Group on Antimicrobial Stewardship. An international cross-sectional survey of antimicrobial stewardship programmes in hospitals. J. Antimicrob. Chemother. 2015, 70, 1245–1255. [Google Scholar] [CrossRef] [Green Version]
- Perozziello, A.; Lescure, F.X.; Truel, A.; Routelous, C.; Vaillant, L.; Yazdanpanah, Y.; Lucet, J.C.; CEFECA Study Group. Prescribers’ experience and opinions on antimicrobial stewardship programmes in hospitals: A French nationwide survey. J. Antimicrob. Chemother. 2019, 74, 2451–2458. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Implementation | After Implementation | p-Value | |
|---|---|---|---|
| 1/1/2016 to 31/5/2017 | 1/1/2018 to 31/5/2019 | ||
| Number of stays | 3561 | 3839 | |
| Gender | |||
| Female | 1646 (46%) | 1848 (48%) | |
| Male | 1915 (54%) | 1991 (52%) | |
| Age (years) | |||
| Mean (Min–Max) | 73.13 (17–108) | 73.30 (17–103) | |
| ICU stays | |||
| 600 (17%) | 567 (15%) | 0.015 | |
| Pre-existing medical conditions | |||
| Solid organ transplant | 7 (0.2%) | 14 (0.4%) | 0.25 |
| Immunomodulatory therapy | 1 (0.03%) | 9 (0.2%) | 0.036 |
| End stages renal disease (IV–V) | 30 (0.8%) | 72 (1.9%) | 0.0002 |
| Chronic liver disease | 47 (1.3%) | 39 (1%) | 0.27 |
| Chronic respiratory failure | 187 (5.3%) | 250 (6.5%) | 0.025 |
| Agranulocytosis | 10 (0.3%) | 15 (0.4%) | 0.54 |
| Chemotherapy during the stay | 2 (0.06%) | 9 (0.2%) | 0.09 |
| Diabetes | 724 (20%) | 874 (23%) | 0.01 |
| HIV | 33 (0.9%) | 24 (0.6%) | 0.18 |
| Infection types | |||
| Pyelonephritis | 1124 | 1013 | |
| Intra-abdominal infections | 651 | 673 | |
| Cellulitis and skin abscess | 233 | 253 | |
| Meningitis | 5 | 7 | |
| Endocarditis | 9 | 10 | |
| Pulmonary infection | 1834 | 1809 | |
| Osteomyelitis and prosthetic joint infection | 62 | 70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bouchet, F.; Le Moing, V.; Dirand, D.; Cros, F.; Lienard, A.; Reynes, J.; Giraudon, L.; Morquin, D. Effectiveness and Acceptance of Multimodal Antibiotic Stewardship Program: Considering Progressive Implementation and Complementary Strategies. Antibiotics 2020, 9, 848. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9120848
Bouchet F, Le Moing V, Dirand D, Cros F, Lienard A, Reynes J, Giraudon L, Morquin D. Effectiveness and Acceptance of Multimodal Antibiotic Stewardship Program: Considering Progressive Implementation and Complementary Strategies. Antibiotics. 2020; 9(12):848. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9120848
Chicago/Turabian StyleBouchet, Flavien, Vincent Le Moing, Delphine Dirand, François Cros, Alexi Lienard, Jacques Reynes, Laurent Giraudon, and David Morquin. 2020. "Effectiveness and Acceptance of Multimodal Antibiotic Stewardship Program: Considering Progressive Implementation and Complementary Strategies" Antibiotics 9, no. 12: 848. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9120848