Sepsis—A Retrospective Cohort Study of Bloodstream Infections

 ,
,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Results
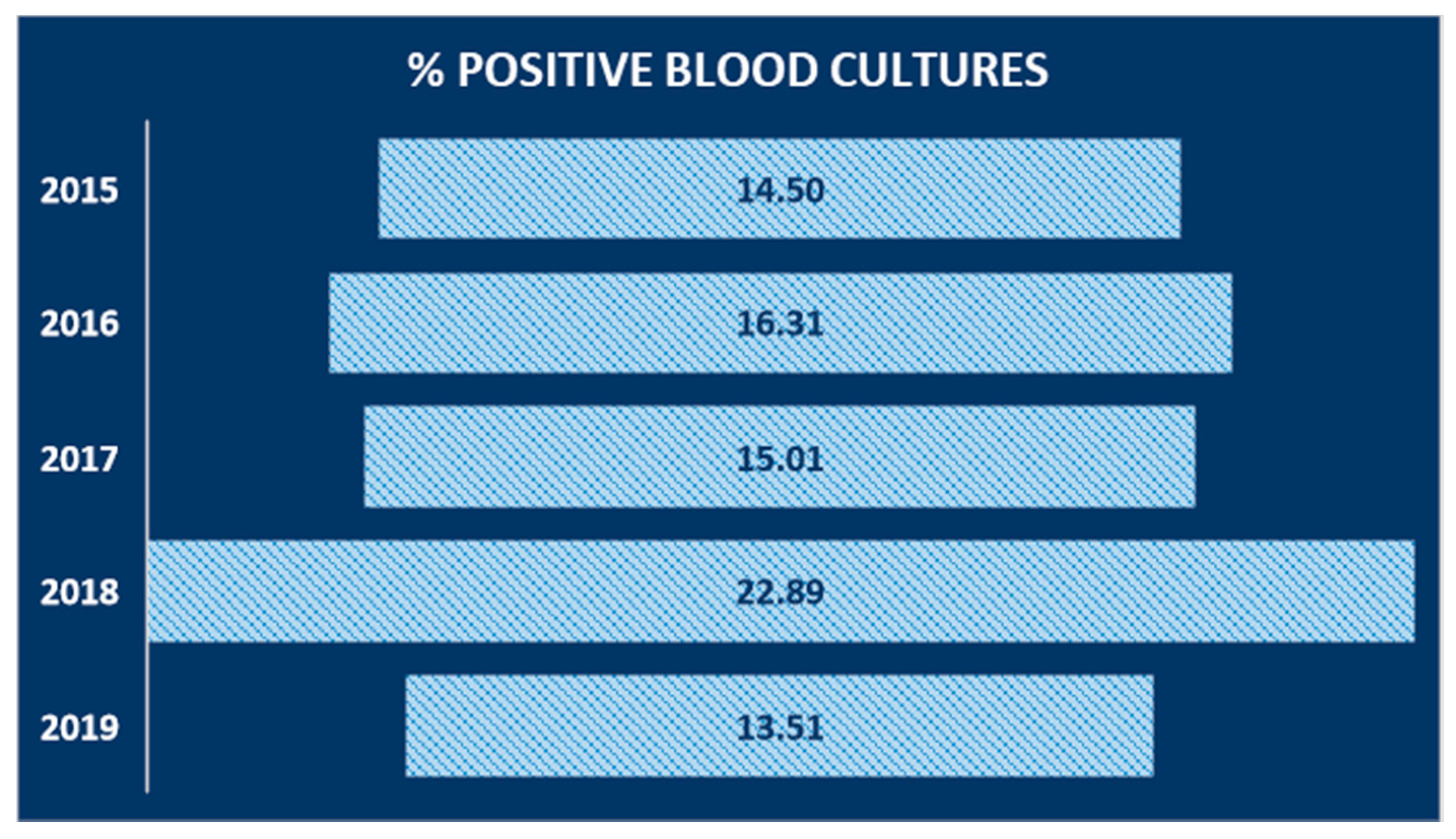
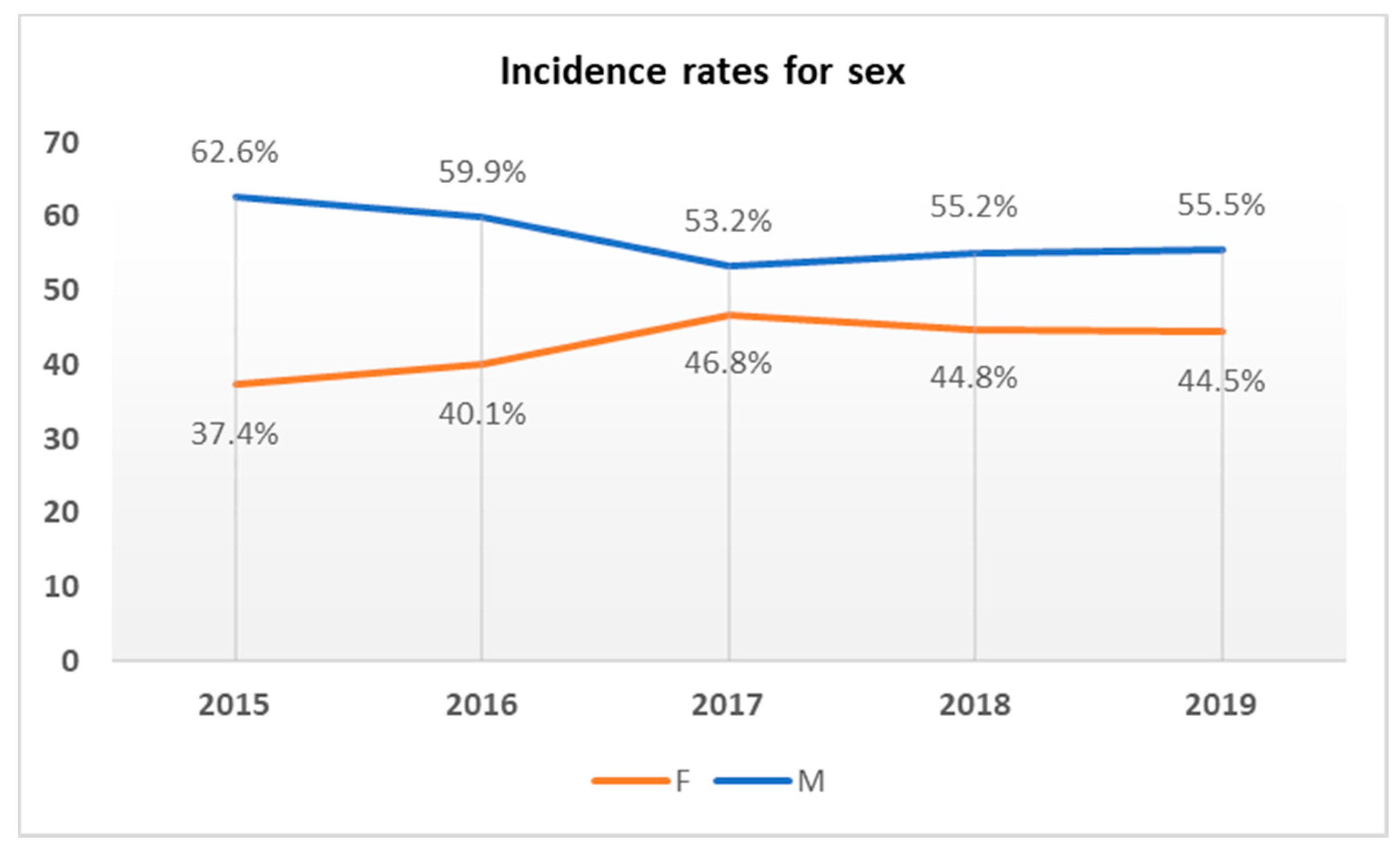
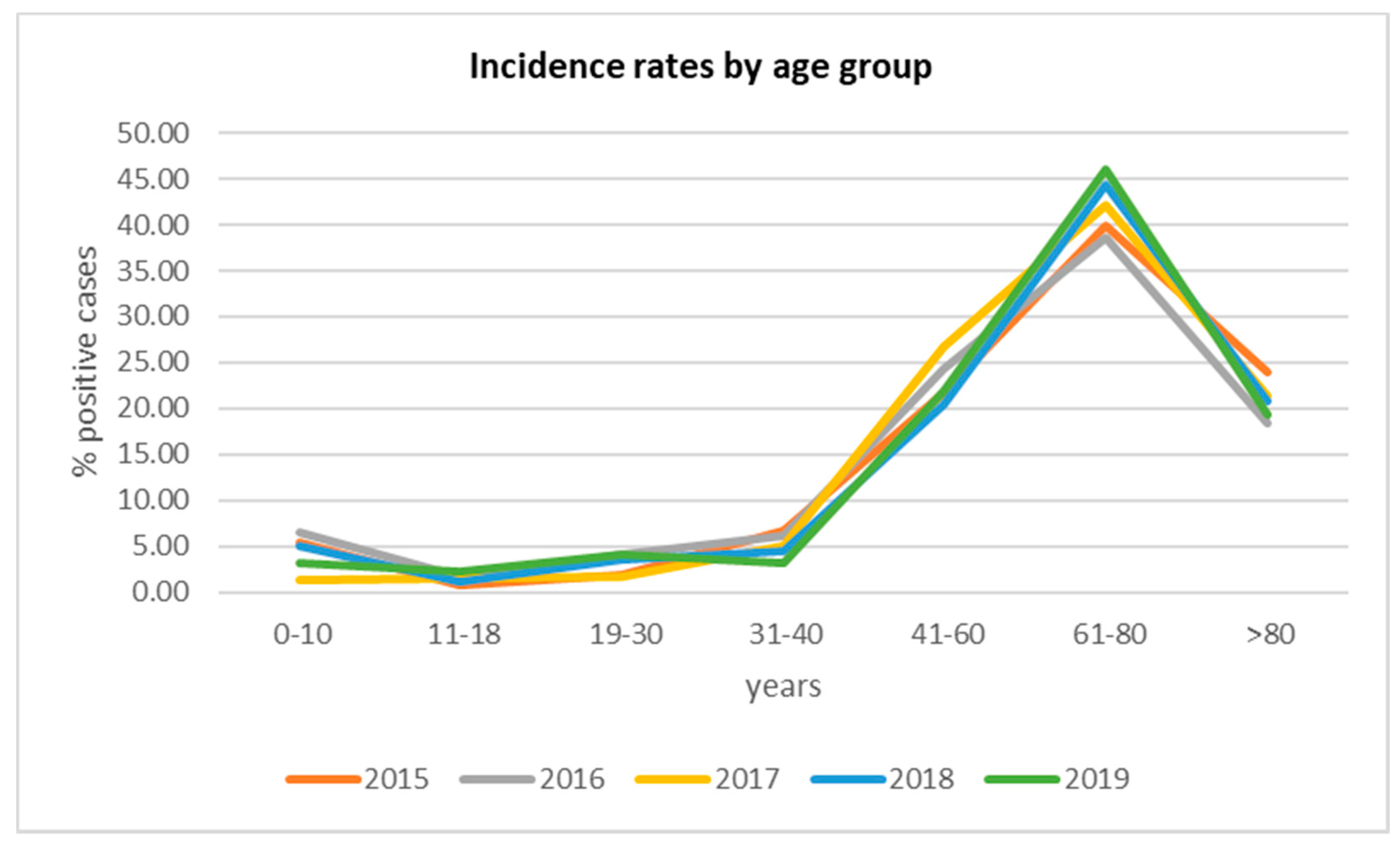
2.1. Incidence of BSIs in Studied Patients
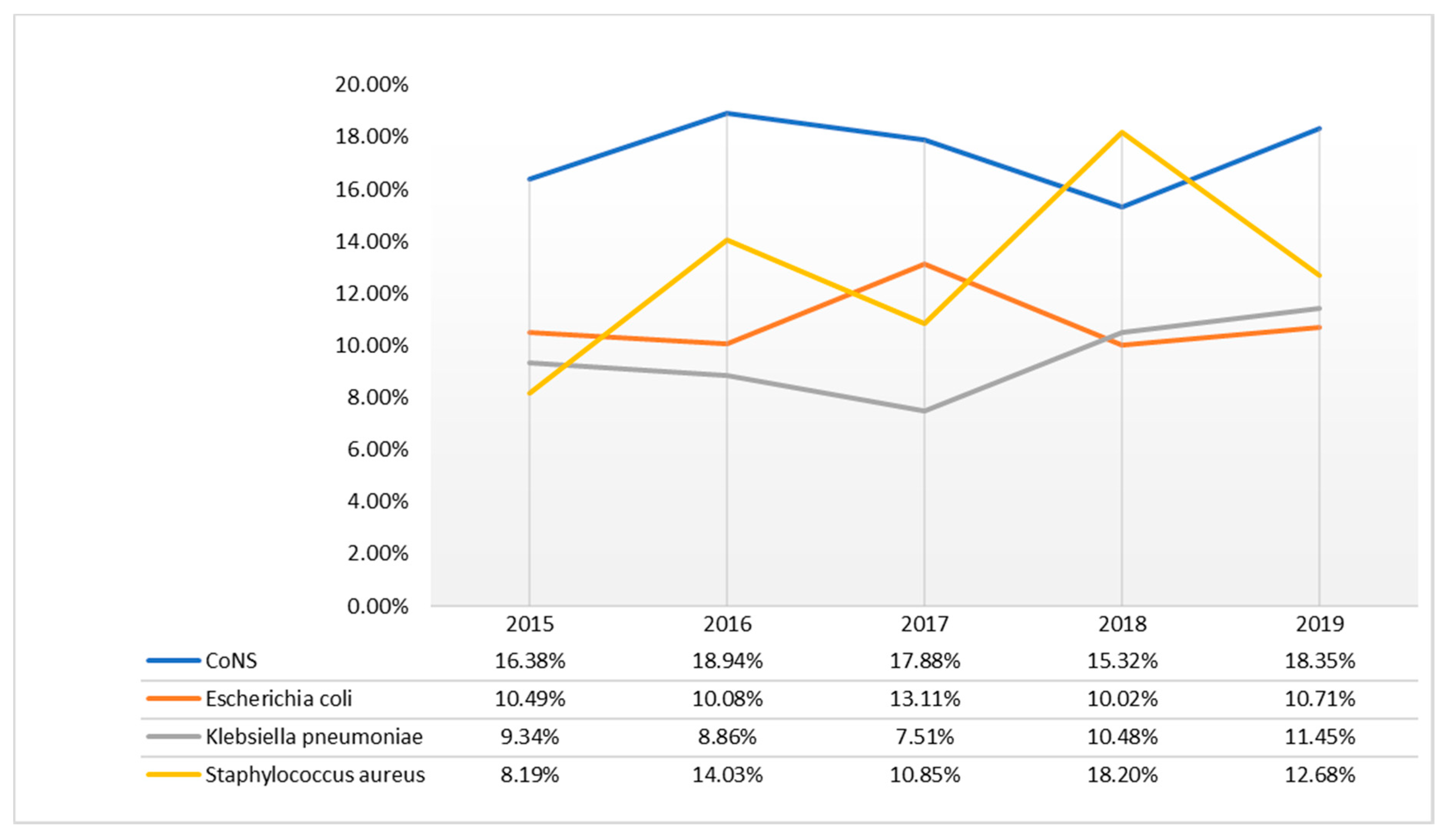
2.2. Isolated Bacteria
2.3. Prevalence of Antimicrobial Resistance among BSI Bacteria
3. Discussion
4. Materials and Methods
4.1. Samples Collection
4.2. Isolation, Identification and Antimicrobial Susceptibility Test for BSI Pathogens
4.3. Ethical Consideration Statement
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Timsit, J.-F.; Ruppé, E.; Barbier, F.; Tabah, A.; Bassetti, M. Bloodstream infections in critically ill patients: An expert statement. Intensiv. Care Med. 2020, 46, 266–284. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, M.C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Wisplinghoff, H.; Bischoff, T.; Tallent, S.M.; Seifert, H.; Wenzel, R.P.; Edmond, M.B. Nosocomial Bloodstream Infections in US Hospitals: Analysis of 24,179 Cases from a Prospective Nationwide Surveillance Study. Clin. Infect. Dis. 2004, 39, 309–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.-N.; Gan, T.-E.; Zhu, Y.-X.; Cao, J.-M.; Ji, C.-H.; Wu, Y.-H.; Lu, B. Epidemiology and microbiology of nosocomial bloodstream infections: Analysis of 482 cases from a retrospective surveillance study. J. Zhejiang Univ. Sci. B 2015, 16, 70–77. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, D.; Nahid, A.; Sami, A.B.; Halim, F.; Akter, N.; Sadique, T.; Rana, S.; Bin Elahi, S.; Rahman, M. Bacterial etiology of bloodstream infections and antimicrobial resistance in Dhaka, Bangladesh, 2005–2014. Antimicrob. Resist. Infect. Control. 2017, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- Kanoksil, M.; Jatapai, A.; Peacock, S.J.; Limmathurotsakul, D. Epidemiology, microbiology and mortality associated with community-acquired bacteremia in northeast Thailand: A multicenter surveillance study. PLoS ONE 2013, 8, e54714. [Google Scholar] [CrossRef]
- Vallés, J.; Palomar, M.; Alvárez-Lerma, F.; Rello, J.; Blanco, A.; Garnacho-Montero, J.; Martín-Loeches, I. Evolution Over a 15-Year Period of Clinical Characteristics and Outcomes of Critically Ill Patients With Community-Acquired Bacteremia. Crit. Care Med. 2013, 41, 76–83. [Google Scholar] [CrossRef]
- Kollef, M.H.; Zilberberg, M.D.; Shorr, A.F.; Vo, L.; Schein, J.; Micek, S.T.; Kim, M. Epidemiology, microbiology and outcomes of healthcare-associated and community-acquired bacteremia: A multicenter cohort study. J. Infect. 2011, 62, 130–135. [Google Scholar] [CrossRef]
- Søgaard, M.; Nørgaard, M.; Dethlefsen, C.; Schønheyder, H.C. Temporal Changes in the Incidence and 30-Day Mortality associated with Bacteremia in Hospitalized Patients from 1992 through 2006: A Population-based Cohort Study. Clin. Infect. Dis. 2011, 52, 61–69. [Google Scholar] [CrossRef]
- Valles, J.; Rello, J.; Ochagavia, A.; Garnacho, J.; Alcala, M.A. Community-acquired bloodstream infection in critically ill adult patients: Impact of shock and inappropriate antibiotic therapy on survival. Chest 2003, 123, 1615–1624. [Google Scholar] [CrossRef]
- Kilgore, M.L.; Brossette, S. Cost of bloodstream infections. Am. J. Infect. Control. 2008, 36, S172.e1–S172.e3. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Moldawer, L.L.; Opal, S.M.; Reinhart, K.; Turnbull, I.R.; Vincent, J.L. Sepsis and septic shock. Nat. Rev. Dis. Primers 2016, 2, 16045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathur, P.; Varghese, P.; Tak, V.; Gunjiyal, J.; Lalwani, S.; Kumar, S.; Misra, M.C. Epidemiology of Blood Stream Infections at a Level-1 Trauma Care Center of India. J. Lab. Physicians 2014, 6, 022–027. [Google Scholar] [CrossRef] [PubMed]
- Kwiecińska-Piróg, J.; Skowron, K.; Gospodarek-Komkowska, E. Primary and Secondary Bacteremia Caused by Proteus spp.: Epidemiology, Strains Susceptibility and Biofilm Formation. Pol. J. Microbiol. 2018, 67, 471–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegman-Igra, Y.; Fourer, B.; Orni-Wasserlauf, R.; Golan, Y.; Noy, A.; Schwartz, D.; Giladi, M.; Yardena, S.-I.; Boaz, F.; Ruth, O.-W.; et al. Reappraisal of Community-Acquired Bacteremia: A Proposal of a New Classification for the Spectrum of Acquisition of Bacteremia. Clin. Infect. Dis. 2002, 34, 1431–1439. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Wang, Q.; Zhu, F.; An, Y. Epidemiology, species distribution, antifungal susceptibility and mortality risk factors of candidemia among critically ill patients: A retrospective study from 2011 to 2017 in a teaching hospital in China. Antimicrob. Resist. Infect. Control. 2019, 8, 89. [Google Scholar] [CrossRef]
- Tian, L.; Zhang, Z.; Sun, Z. Antimicrobial resistance trends in bloodstream infections at a large teaching hospital in China: A 20-year surveillance study (1998-2017). Antimicrob. Resist. Infect. Control. 2019, 8, 86. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.-L. The Clinical Challenge of Sepsis Identification and Monitoring. PLoS Med. 2016, 13, e1002022. [Google Scholar] [CrossRef] [Green Version]
- Seifert, H. The Clinical Importance of Microbiological Findings in the Diagnosis and Management of Bloodstream Infections. Clin. Infect. Dis. 2009, 48, 238–245. [Google Scholar] [CrossRef]
- Dailey, P.J.; Osborn, J.; Ashley, E.A.; Baron, E.J.; Dance, D.A.B.; Fusco, D.; Fanello, C.; Manabe, Y.C.; Mokomane, M.; Newton, P.N.; et al. Defining System Requirements for Simplified Blood Culture to Enable Widespread Use in Resource-Limited Settings. Diagnostics 2019, 9, 10. [Google Scholar] [CrossRef] [Green Version]
- Peker, N.; Couto, N.; Sinha, B.; Rossen, J.W.A. Diagnosis of bloodstream infections from positive blood cultures and directly from blood samples: Recent developments in molecular approaches. Clin. Microbiol. Infect. 2018, 24, 944–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sader, H.S.; Castanheira, M.; Streit, J.M.; Carvalhaes, C.G.; Mendes, R.E. Frequency and antimicrobial susceptibility of bacteria causing bloodstream infections in pediatric patients from United States (US) medical centers (2014–2018): Therapeutic options for multidrug-resistant bacteria. Diagn. Microbiol. Infect. Dis. 2020, 98, 115108. [Google Scholar] [CrossRef] [PubMed]
- Hattori, H.; Maeda, M.; Nagatomo, Y.; Takuma, T.; Niki, Y.; Naito, Y.; Sasaki, T.; Ishino, K. Epidemiology and risk factors for mortality in bloodstream infections: A single-center retrospective study in Japan. Am. J. Infect. Control. 2018, 46, e75–e79. [Google Scholar] [CrossRef] [PubMed]
- Buetti, N.; Atkinson, A.; Marschall, J.; Kronenberg, A.; Anresis, T.S.C.F.A.R. Incidence of bloodstream infections: A nationwide surveillance of acute care hospitals in Switzerland 2008–2014. BMJ Open 2017, 7, e013665. [Google Scholar] [CrossRef] [Green Version]
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef] [Green Version]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Hall, K.K.; Lyman, J.A. Updated Review of Blood Culture Contamination. Clin. Microbiol. Rev. 2006, 19, 788–802. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.ecdc.europa.eu/en/publications-data/point-prevalence-survey-healthcare-associated-infections-and-antimicrobial-use-0 (accessed on 4 July 2013).
- Sante, L.; Aguirre-Jaime, A.; Miguel, M.A.; Ramos, M.J.; Pedroso, Y.; Lecuona, M. Epidemiological study of secondary bloodstream infections: The forgotten issue. J. Infect. Public Heal. 2019, 12, 37–42. [Google Scholar] [CrossRef]
- Panday, R.S.N.; Wang, S.; Van De Ven, P.M.; Hekker, T.A.M.; Alam, N.; Nanayakkara, P.W.B. Evaluation of blood culture epidemiology and efficiency in a large European teaching hospital. PLoS ONE 2019, 14, e0214052. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, S.; Nielsen, J.; Voldstedlund, M.; Kristensen, B.; Schonheyder, H.C.; Vandenbroucke-Grauls, C.; Arpi, M.; Björnsdóttir, M.; Knudsen, J.D.; Dessau, R.B.; et al. Utilization of blood cultures in Danish hospitals: A population-based descriptive analysis. Clin. Microbiol. Infect. 2015, 21, 344.e13–344.e21. [Google Scholar] [CrossRef] [Green Version]
- Uslan, D.Z.; Crane, S.J.; Steckelberg, J.M.; Cockerill, F.R., 3rd; St Sauver, J.L.; Wilson, W.R.; Baddour, L.M. Age- and sex-associated trends in bloodstream infection: A population-based study in Olmsted County, Minnesota. Arch. Intern. Med. 2007, 167, 834–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlowsky, J.A.; Jones, M.E.; Draghi, D.C.; Thornsberry, C.; Sahm, D.F.; Volturo, G.A. Prevalence and antimicrobial susceptibilities of bacteria isolated from blood cultures of hospitalized patients in the United States in 2002. Ann. Clin. Microbiol. Antimicrob. 2004, 3, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakur, S.; Thakur, K.; Sood, A.; Chaudhary, S. Bacteriological profile and antibiotic sensitivity pattern of neonatal septicaemia in a rural tertiary care hospital in North India. Indian J. Med Microbiol. 2016, 34, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Gohel, K.; Jojera, A.; Soni, S.; Gang, S.; Sabnis, R.; Desai, M. Bacteriological Profile and Drug Resistance Patterns of Blood Culture Isolates in a Tertiary Care Nephrourology Teaching Institute. BioMed Res. Int. 2014, 2014, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Pignataro, D.; Foglia, F.; Della Rocca, M.T.; Melardo, C.; Santella, B.; Folliero, V.; Shinde, S.; Pafundi, P.C.; Sasso, F.; Iovene, M.R.; et al. Methicillin-resistant Staphylococcus aureus: Epidemiology and antimicrobial susceptibility experiences from the University Hospital ‘Luigi Vanvitelli’ of Naples. Pathog. Glob. Heal. 2020, 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Choo, E.J.; Chambers, H.G. Treatment of Methicillin-Resistant Staphylococcus aureus Bacteremia. Infect. Chemother. 2016, 48, 267–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidhu, S.K.; Malhotra, S.; Devi, P.; Tuli, A.K. Significance of coagulase negative Staphylococcus from blood cultures: Persisting problems and partial progress in resource constrained settings. Iran. J. Microbiol. 2016, 8, 366–371. [Google Scholar]
- Saber, H.; Jasni, A.S.; Jamaluddin, T.Z.M.T.; Ibrahim, R. A Review of Staphylococcal Cassette Chromosome mec (SCCmec) Types in Coagulase-Negative Staphylococci (CoNS) Species. Malays. J. Med Sci. 2017, 24, 7–18. [Google Scholar] [CrossRef]
- Camins, B.C.; Marschall, J.; De Vader, S.R.; Maker, D.E.; Hoffman, M.W.; Fraser, V.J. The clinical impact of fluoroquinolone resistance in patients with E coli bacteremia. J. Hosp. Med. 2011, 6, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Rawat, D.; Nair, D. Extended-spectrum beta-lactamases in Gram Negative Bacteria. J. Glob. Infect. Dis. 2010, 2, 263–274. [Google Scholar] [CrossRef]
- Apondi, O.E.; Oduor, O.C.; Gye, B.K.; Kipkoech, M.K. High Prevalence of Multi-Drug Resistant Klebsiella Pneumoniae in A Tertiary Teaching Hospital in Western Kenya. Afr. J. Infect. Dis. 2016, 10, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuner, E.A.; Yeh, J.-Y.; Hall, G.S.; Sekeres, J.; Endimiani, A.; Bonomo, R.A.; Shrestha, N.K.; Fraser, T.G.; Van Duin, D. Treatment and outcomes in carbapenem-resistant Klebsiella pneumoniae bloodstream infections. Diagn. Microbiol. Infect. Dis. 2011, 69, 357–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sydnor, E.R.M.; Perl, T.M. Hospital Epidemiology and Infection Control in Acute-Care Settings. Clin. Microbiol. Rev. 2011, 24, 141–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Belkum, A.; Bachmann, T.T.; Ludke, G.; Lisby, J.G.; Kahlmeter, G.; Mohess, A.; Becker, K.; Hays, J.P.; Woodford, N.; Mitsakakis, K.; et al. Developmental roadmap for antimicrobial susceptibility testing systems. Nat. Rev. Microbiol. 2019, 17, 51–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fair, R.J.; Tor, Y. Antibiotics and Bacterial Resistance in the 21st Century. Perspect. Med. Chem. 2014, 6, 25–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.-R.; Cho, I.H.; Jeong, B.C.; Lee, S.H. Strategies to Minimize Antibiotic Resistance. Int. J. Environ. Res. Public Heal. 2013, 10, 4274–4305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zannella, C.; Shinde, S.; Vitiello, M.; Falanga, A.; Galdiero, E.; Fahmi, A.; Santella, B.; Nucci, L.; Gasparro, R.; Galdiero, M.; et al. Antibacterial Activity of Indolicidin-Coated Silver Nanoparticles in Oral Disease. Appl. Sci. 2020, 10, 1837. [Google Scholar] [CrossRef] [Green Version]
- Retamar, P.; Portillo, M.M.; López-Prieto, M.D.; Rodríguez-López, F.; De Cueto, M.; García, M.V.; Gómez, M.J.; Del Arco, A.; Muñoz, A.; Sánchez-Porto, A.; et al. Impact of Inadequate Empirical Therapy on the Mortality of Patients with Bloodstream Infections: A Propensity Score-Based Analysis. Antimicrob. Agents Chemother. 2012, 56, 472–478. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | 2015 | 2016 | 2017 | 2018 | 2019 | Total |
|---|---|---|---|---|---|---|
| Positive | 696 | 734 | 839 | 868 | 812 | 3949 |
| Negative | 4104 | 3766 | 4752 | 2924 | 5199 | 20,745 |
| Total | 4800 | 4500 | 5591 | 3792 | 6011 | 24,694 |
| St. aureus | 2015 | 2016 | 2017 | 2018 | 2019 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Antibiotic | n. Assays | R % | n. Assays | R % | n. Assays | R % | n. Assays | R % | n. Assays | R % |
| Fusidic acid | 60 | 0 | 103 | 1.9 | 91 | 5.5 | 158 | 4.4 | 103 | 4.9 |
| Clindamycin | 60 | 36.7 | 103 | 27.2 | 91 | 39.6 | 158 | 39.9 | 103 | 35.9 |
| Daptomycin | 60 | 0 | 103 | 1.0 | 91 | 5.5 | 158 | 5.1 | 103 | 3.9 |
| Erythromycin | 60 | 43.3 | 103 | 49.5 | 91 | 50.5 | 158 | 53.2 | 103 | 42.7 |
| Gentamicin | 60 | 13.3 | 103 | 13.6 | 91 | 9.9 | 158 | 10.8 | 103 | 7.8 |
| Levofloxacin | 57 | 33.3 | 79 | 35.4 | 77 | 53.2 | 116 | 41.4 | 90 | 27.8 |
| Linezolid | 60 | 0 | 103 | 0 | 91 | 4.4 | 158 | 4.4 | 103 | 2.9 |
| Oxacillin | 60 | 26.7 | 103 | 50.5 | 91 | 53.8 | 158 | 50.6 | 103 | 36.9 |
| Penicillin G | 60 | 86.7 | 102 | 85.3 | 91 | 84.6 | 158 | 86.7 | 103 | 68.9 |
| Rifampicin | 57 | 7.0 | 79 | 12.7 | 77 | 0 | 116 | 3.4 | 90 | 7.8 |
| Teicoplanin | 60 | 0 | 103 | 1.9 | 91 | 5.5 | 157 | 5.7 | 103 | 7.8 |
| Tetracycline | 60 | 9.6 | 103 | 9.8 | 91 | 8.8 | 158 | 3.2 | 103 | 9.8 |
| Tigecycline | 58 | 0 | 103 | 0 | 91 | 4.4 | 157 | 2.5 | 103 | 1.0 |
| Trimethoprim/Sulfam. | 60 | 1.7 | 103 | 2.0 | 91 | 5.5 | 157 | 1.9 | 103 | 4.9 |
| Vancomycin | 60 | 0 | 103 | 1.9 | 91 | 4.4 | 158 | 4.4 | 103 | 3.9 |
| CoNS | 2015 | 2016 | 2017 | 2018 | 2019 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Antibiotic | n. Assays | R % | n. Assays | R % | n. Assays | R % | n. Assays | R % | n. Assays | R % |
| Fusidic acid | 212 | 28.3 | 257 | 36.6 | 274 | 27.0 | 230 | 31.7 | 242 | 33.1 |
| Clindamycin | 216 | 62.5 | 257 | 57.2 | 272 | 55.1 | 232 | 54.3 | 243 | 51.4 |
| Daptomycin | 211 | 0.5 | 257 | 1.2 | 269 | 2.2 | 229 | 0.9 | 243 | 2.9 |
| Linezolid | 200 | 0 | 237 | 0 | 258 | 0.4 | 231 | 6.9 | 243 | 3.3 |
| Oxacillin | 206 | 81.1 | 233 | 77.3 | 249 | 72.7 | 229 | 78.6 | 243 | 77.8 |
| Rifampicin | 207 | 28.0 | 233 | 31.8 | 250 | 32.4 | 201 | 37.3 | 201 | 34.3 |
| Vancomycin | 216 | 0.5 | 257 | 0.4 | 273 | 1.1 | 232 | 0.4 | 242 | 3.7 |
| Klebsiella pneumoniae | 2015 | 2016 | 2017 | 2018 | 2019 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Antibiotic | n. Assays | R % | n. Assays | R % | n. Assays | R % | n. Assays | R % | n. Assays | R % |
| Amoxicillin/A. Clav. | 67 | 77.6 | 60 | 76.7 | 53 | 79.2 | 62 | 82.3 | 116 | 94.8 |
| Cefotaxime | 67 | 85.1 | 65 | 73.8 | 63 | 87.3 | 91 | 81.3 | 92 | 92.4 |
| Ceftazidime | 67 | 79.1 | 65 | 73.8 | 63 | 85.7 | 91 | 84.6 | 93 | 92.5 |
| Ciprofloxacin | 67 | 86.6 | 65 | 73.8 | 63 | 85.7 | 91 | 76.9 | 93 | 89.2 |
| Colistin | 66 | 21.2 | 63 | 27.0 | 55 | 16.4 | 75 | 12.3 | 88 | 26.1 |
| Ertapenem | 59 | 62.7 | 65 | 64.6 | 63 | 77.8 | 91 | 54.9 | 93 | 65.6 |
| Fosfomycin | 67 | 22.4 | 60 | 28.3 | 53 | 20.7 | 63 | 14.3 | 68 | 38.2 |
| Meropenem | 67 | 64.2 | 65 | 64.6 | 63 | 74.6 | 91 | 54.9 | 93 | 65.6 |
| Piperacillin/Tazobactam | 67 | 79.1 | 65 | 70.8 | 63 | 82.5 | 91 | 81.3 | 93 | 79.6 |
| Trimethoprim/Sulf. | 67 | 77.6 | 65 | 69.2 | 63 | 88.9 | 91 | 70.3 | 93 | 58.1 |
| Escherichia coli | 2015 | 2016 | 2017 | 2018 | 2019 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Antibiotic | n. Assays | R % | n. Assays | R % | n. Assays | R % | n. Assays | R % | n. Assays | R % |
| Amoxicillin/A. Clav. | 70 | 50.0 | 66 | 56.1 | 103 | 39.8 | 84 | 51.2 | 110 | 68.2 |
| Cefotaxime | 73 | 53.5 | 74 | 54.1 | 110 | 52.7 | 87 | 57.5 | 83 | 54.2 |
| Ciprofloxacin | 73 | 61.6 | 74 | 68.9 | 110 | 66.3 | 87 | 67.8 | 87 | 71.3 |
| Ertapenem | 73 | 1.4 | 74 | 0 | 110 | 0 | 87 | 2.3 | 87 | 2.3 |
| Fosfomycin | 70 | 0 | 66 | 0 | 103 | 4.9 | 84 | 0 | 70 | 0 |
| Gentamicin | 73 | 34.2 | 74 | 40.5 | 110 | 27.3 | 87 | 27.6 | 87 | 31.0 |
| Imipenem | 73 | 0 | 74 | 0 | 110 | 0 | 74 | 0 | 23 | 0 |
| Meropenem | 73 | 0 | 74 | 0 | 110 | 0 | 87 | 2.3 | 87 | 2.2 |
| Piperacillin/tazobactam | 72 | 15.3 | 74 | 10.8 | 110 | 18.2 | 86 | 12.8 | 85 | 14.1 |
| Tigecycline | 72 | 0 | 73 | 0 | 109 | 0 | 85 | 0 | 81 | 1.2 |
| Trimethoprim/Sulf. | 73 | 41.1 | 74 | 43.2 | 110 | 45.5 | 87 | 52.9 | 87 | 55.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santella, B.; Folliero, V.; Pirofalo, G.M.; Serretiello, E.; Zannella, C.; Moccia, G.; Santoro, E.; Sanna, G.; Motta, O.; De Caro, F.; et al. Sepsis—A Retrospective Cohort Study of Bloodstream Infections. Antibiotics 2020, 9, 851. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9120851
Santella B, Folliero V, Pirofalo GM, Serretiello E, Zannella C, Moccia G, Santoro E, Sanna G, Motta O, De Caro F, et al. Sepsis—A Retrospective Cohort Study of Bloodstream Infections. Antibiotics. 2020; 9(12):851. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9120851
Chicago/Turabian StyleSantella, Biagio, Veronica Folliero, Gerarda Maria Pirofalo, Enrica Serretiello, Carla Zannella, Giuseppina Moccia, Emanuela Santoro, Giuseppina Sanna, Oriana Motta, Francesco De Caro, and et al. 2020. "Sepsis—A Retrospective Cohort Study of Bloodstream Infections" Antibiotics 9, no. 12: 851. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9120851