Infectious Disease and Primary Care Research—What English General Practitioners Say They Need

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
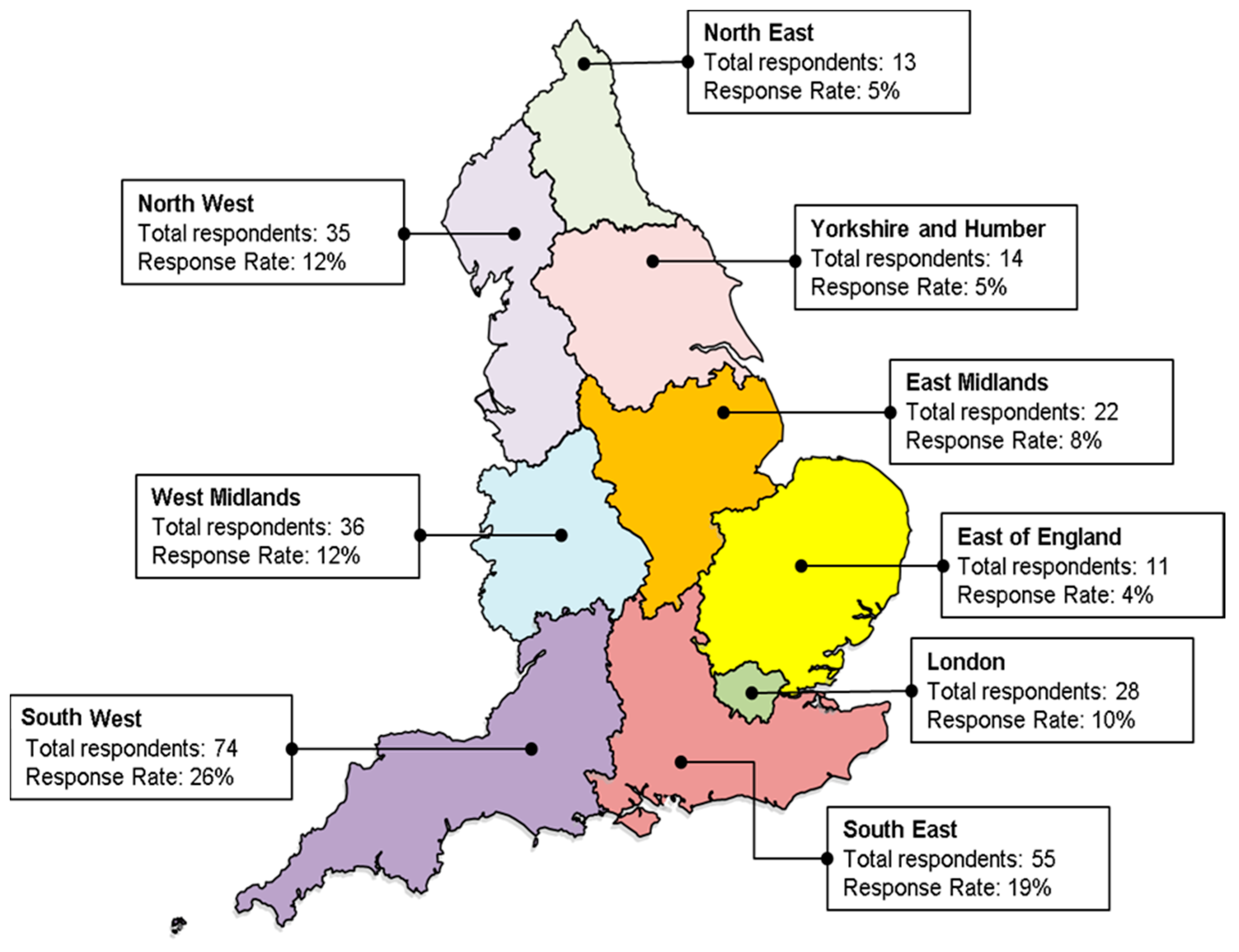
2.1. Response Rate
2.2. Representativeness of the Data
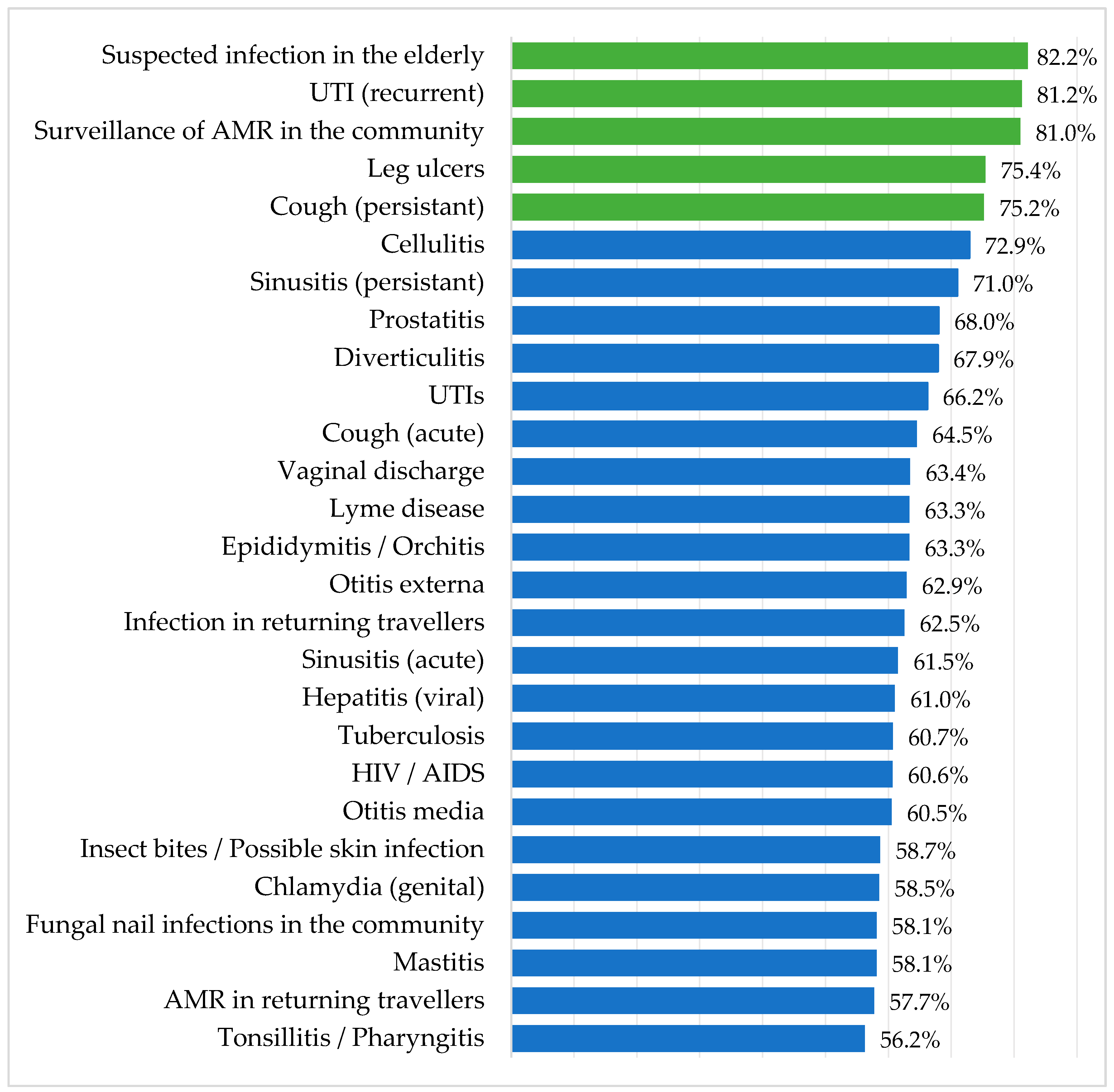
2.3. Condition Ranking
2.4. Top Three Illnesses/Conditions That Require Further Research, Evidence and Guidance
Other Conditions
2.5. Type of Evidence, Research and Guidance Needed
3. Discussion
3.1. Strengths and Limitations
3.2. Comparison with Existing Literature
4. Materials and Methods
- Participant rating of 27 named illnesses/conditions based on how much more evidence they perceive is required to support daily practice.
- Participant selection of the top three illnesses/conditions that they perceive require further research, evidence and guidance, with participant identification of where those improvements are required.
- Demographic data collection.
4.1. Survey Dissemination
4.2. Data Management
4.3. Representativeness of the GP Sample
4.4. Comparison of Importance of Research between GPs from Research and Non-Research Practices
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. GP Questionnaire Survey
Section 1
- On a scale of 1–5, please indicate how much more evidence you would like to see for each of the following conditions to support your daily clinical practice.
- (Tick one box for each statement. Please note that conditions are in alphabetical order)
- AMR in returning travellersCellulitisChlamydia GenitalCough AcuteCough PersistentDiverticulitisEpididymitis/OrchitisFungal nail infections in the communityHepatitis ViralHIV/AIDSInfection in Returning TravellersInsect Bites, possible skin infectionsLeg UlcersLyme DiseaseMastitisOtitis ExternaOtitis MediaProstatitisSinusitis AcuteSinusitis PersistentSurveillance of AMR in the communitySuspected Infection in The ElderlyTonsillitis/PharyngitisTuberculosisUTI RecurrentUTIsVaginal Discharge
- Please specify up to three conditions/illnesses not mentioned that you think require further research
- On a scale of 1–5, please indicate how much more evidence you would like to see for your chosen illness/condition to support your daily clinical practice. (Tick one box for each statement)
- Optional extra 1Optional extra 2Optional extra 3
Section 2
- From the list of illnesses/conditions you just rated, which top 3 illnesses/conditions do you feel require further research, evidence and guidance?
- Illness condition 1
- Illness condition 2
- Illness condition
- In relation to this illness/condition (respondents will only be shown their 3 selected illness/conditions), please indicate how important you feel improvements in each of the following areas are?
- Need for better evidence base for antibiotic treatment in primary care
- Need for better evidence base for self-care and non-antibiotic treatment in primary care
- Need for better near patient antibiotic resistance test in primary care
- Need for improved treatment guidelines for primary care staff
- Need for better clinical scores to help inform management in primary care
- Need for better point of care prognostic tests in primary care
Section 3
- How did you receive this questionnaire?
- Royal College of General Practitioners (RCGP)
- NIHR Clinical Research Network ((CRN) (Primary Care))
- Clinical Commissioning Group (CCG)
- Colleague
- Other, please specify
- Age (years)
- 20–30
- 31–40
- 41–50
- 51–60
- 60+
- Sex
- Male
- Female
- How many years have you been a practicing GP?
- 0–5
- 6 to 10
- 11 to 15
- 16–20
- 20+
- Did you carry out an antibiotic/infection audit in the past 12 months?
- Yes
- No
- Where are you a general practitioner?
- England
- Scotland
- Wales
- Northern Ireland
- Which region is your practice in?Please select one
- North East
- North West
- Yorkshire and Humber
- East Midlands
- West Midlands
- East of England
- London
- South East
- South West
- How would you describe your practice geographical location?
- rural
- urban
- suburban
- Is your practice a research practice?
- Yes
- No
Appendix B

{kind=link}
{kind=link}
| Condition | Responses | Non-Research | Research | Unadjusted | Adjusted | ||||
|---|---|---|---|---|---|---|---|---|---|
| Further Research is | (n) | (n) | |||||||
| AMR in returning travellers | Very Unimportant | 20 | 22 | OR 0.7 | [95% CI 0.48–1.01]; | p = 0.06 | OR 0.76 | [95% CI 0.50–1.14]; | p = 0.18 |
| Unimportant | 44 | 50 | |||||||
| Neutral | 55 | 48 | |||||||
| Important | 39 | 32 | |||||||
| Very important | 26 | 14 | |||||||
| Cellulitis | Very Unimportant | 6 | 10 | OR 0.99 | [95% CI 0.68–1.46]; | p = 0.98 | OR 0.96 | [95% CI 0.63–1.45]; | p = 0.8 |
| Unimportant | 19 | 16 | |||||||
| Neutral | 42 | 34 | |||||||
| Important | 70 | 72 | |||||||
| Very important | 42 | 38 | |||||||
| Chlamydia genital | Very Unimportant | 16 | 17 | OR 0.89 | [95% CI 0.61–1.31]; | p = 0.6 | OR 0.92 | [95% CI 0.61–1.40]; | p = 0.7 |
| Unimportant | 40 | 45 | |||||||
| Neutral | 75 | 58 | |||||||
| Important | 40 | 34 | |||||||
| Very important | 9 | 12 | |||||||
| Cough (acute) | Very Unimportant | 19 | 17 | OR 1.2 | [95% CI 0.82–1.74]; | p = 0.3 | OR 1.29 | [95% CI 0.88–1.90]; | p = 0.19 |
| Unimportant | 36 | 30 | |||||||
| Neutral | 47 | 43 | |||||||
| Important | 49 | 44 | |||||||
| Very important | 28 | 35 | |||||||
| Cough (persistent) | Very Unimportant | 8 | 6 | OR 1.2 | [95% CI 0.82–1.76]; | p = 0.3 | OR 1.31 | [95% CI 0.89–1.95]; | p = 0.17 * |
| Unimportant | 15 | 11 | |||||||
| Neutral | 42 | 35 | |||||||
| Important | 70 | 69 | |||||||
| Very important | 47 | 48 | |||||||
| Diverticulitis | Very Unimportant | 11 | 6 | OR 1.11 | [95% CI 0.76–1.63]; | p = 0.6 | OR 1.29 | [95% CI 0.85–1.95]; | p = 0.2 * |
| Unimportant | 23 | 29 | |||||||
| Neutral | 58 | 45 | |||||||
| Important | 63 | 62 | |||||||
| Very important | 23 | 25 | |||||||
| Epididymitis | Very Unimportant | 14 | 9 | OR 1.03 | [95% CI 0.70–1.51]; | p = 0.9 | 1 | [95% CI 0.66–1.51]; | p = 0.99 |
| Unimportant | 28 | 34 | |||||||
| Neutral | 70 | 63 | |||||||
| Important | 54 | 44 | |||||||
| Very important | 13 | 19 | |||||||
| Community fungal nail infection | Very Unimportant | 38 | 29 | OR 0.97 | [95% CI 0.67–1.40]; | p = 0.9 | OR 1.19 | [95% CI 0.80–1.78]; | p = 0.4 |
| Unimportant | 32 | 43 | |||||||
| Neutral | 40 | 37 | |||||||
| Important | 46 | 40 | |||||||
| Very important | 25 | 23 | |||||||
| Hepatitis viral | Very Unimportant | 16 | 11 | OR 0.98 | [95% CI 0.67–1.43]; | p = 0.9 | OR 0.98x | [95% CI 0.67–1.43x]; | p = 0.9 x |
| Unimportant | 38 | 42 | |||||||
| Neutral | 66 | 62 | |||||||
| Important | 45 | 31 | |||||||
| Very important | 17 | 22 | |||||||
| HIV/AIDS | Very Unimportant | 15 | 16 | OR 0.9 | [95% CI 0.61–1.31]; | p = 0.6 | OR 0.90x | [95% CI 0.61–1.31x]; | p = 0.6 x |
| Unimportant | 43 | 44 | |||||||
| Neutral | 64 | 56 | |||||||
| Important | 38 | 23 | |||||||
| Very important | 20 | 25 | |||||||
| Infection in returning travellers | Very Unimportant | 13 | 11 | OR 0.78 | [95% CI 0.53–1.13]; | p = 0.19 | OR 0.83 | [95% CI 0.55–1.25]; | p = 0.4 |
| Unimportant | 34 | 44 | |||||||
| Neutral | 60 | 56 | |||||||
| Important | 50 | 42 | |||||||
| Very important | 23 | 17 | |||||||
| Insect bites | Very Unimportant | 19 | 21 | OR 0.98 | [95% CI 0.68–1.43]; | p = 0.9 | OR 1.17 | [95% CI 0.78–1.76]; | p = 0.5 * |
| Unimportant | 43 | 44 | |||||||
| Neutral | 63 | 46 | |||||||
| Important | 43 | 45 | |||||||
| Very important | 12 | 13 | |||||||
| Leg ulcers | Very Unimportant | 5 | 7 | OR 1.12 | [95% CI 0.77–1.64]; | p = 0.5 | OR 1.11 | [95% CI 0.73–1.67]; | p = 0.6 * |
| Unimportant | 15 | 15 | |||||||
| Neutral | 38 | 35 | |||||||
| Important | 76 | 56 | |||||||
| Very important | 48 | 58 | |||||||
| Lyme disease | Very Unimportant | 16 | 13 | OR 0.91 | [95% CI 0.62–1.32]; | p = 0.6 | OR 1.03 | [95% CI 0.68–1.55]; | p = 0.9 |
| Unimportant | 32 | 44 | |||||||
| Neutral | 62 | 50 | |||||||
| Important | 43 | 38 | |||||||
| Very important | 24 | 25 | |||||||
| Mastitis | Very Unimportant | 19 | 21 | OR 0.91 | [95% CI 0.62–1.32]; | p = 0.6 | OR 0.91x | [95% CI 0.62–1.32x]; | p = 0.6 x |
| Unimportant | 40 | 41 | |||||||
| Neutral | 74 | 60 | |||||||
| Important | 38 | 38 | |||||||
| Very important | 11 | 9 | |||||||
| Otitis external | Very Unimportant | 17 | 21 | OR 0.91 | [95% CI 0.64–1.36]; | p = 0.7 | OR 0.99 | [95% CI 0.67–1.47]; | p = 0.97 * |
| Unimportant | 37 | 36 | |||||||
| Neutral | 51 | 40 | |||||||
| Important | 55 | 45 | |||||||
| Very important | 22 | 25 | |||||||
| Otitis media | Very Unimportant | 19 | 20 | OR 0.96 | [95% CI 0.66–1.39]; | p = 0.8 | OR 1.06 | [95% CI 0.70–1.59]; | p = 0.8 * |
| Unimportant | 46 | 41 | |||||||
| Neutral | 51 | 46 | |||||||
| Important | 46 | 48 | |||||||
| Very important | 22 | 16 | |||||||
| Prostatitis | Very Unimportant | 11 | 3 | OR 1.6 | [95% CI 1.09–2.34]; | p = 0.02 | OR 1.53 | 1.02–2.32]; | p = 0.04 * |
| Unimportant | 21 | 22 | |||||||
| Neutral | 77 | 54 | |||||||
| Important | 52 | 60 | |||||||
| Very important | 21 | 30 | |||||||
| Sinusitis (acute) | Very Unimportant | 22 | 19 | OR 0.99 | [95% CI 0.68–1.44]; | p = 0.9 | OR 1.12 | [95% CI 0.75–1.69]; | p = 0.6 |
| Unimportant | 39 | 38 | |||||||
| Neutral | 49 | 45 | |||||||
| Important | 43 | 49 | |||||||
| Very important | 26 | 18 | |||||||
| Sinusitis (persistent) | Very Unimportant | 9 | 8 | OR 0.96 | [95% CI 0.66–1.42]; | p = 0.8 | OR 1.19 | [95% CI 0.78–1.82]; | p = 0.4 |
| Unimportant | 20 | 17 | |||||||
| Neutral | 43 | 45 | |||||||
| Important | 75 | 67 | |||||||
| Very important | 31 | 28 | |||||||
| Surveillance of AMR in community | Very Unimportant | 5 | 7 | OR 1.16 | [95% CI 0.79–1.72]; | p = 0.4 | OR 1.31 | [95% CI 0.86–2.02]; | p = 0.2 |
| Unimportant | 15 | 12 | |||||||
| Neutral | 22 | 19 | |||||||
| Important | 58 | 46 | |||||||
| Very important | 81 | 85 | |||||||
| Suspected infection in elderly | Very Unimportant | 6 | 1 | OR 1.19 | [95% CI 0.81–1.76]; | p = 0.4 | OR 1.4 | [95% CI 0.91–2.16]; | p = 0.13 * |
| Unimportant | 8 | 7 | |||||||
| Neutral | 23 | 19 | |||||||
| Important | 74 | 71 | |||||||
| Very important | 72 | 71 | |||||||
| Tonsillitis | Very Unimportant | 25 | 30 | OR 0.89 | [95% CI 0.61–1.29]; | p = 0.5 | OR 0.94 | [95% CI 0.62–1.41]; | p = 0.8 |
| Unimportant | 49 | 44 | |||||||
| Neutral | 52 | 48 | |||||||
| Important | 43 | 34 | |||||||
| Very important | 12 | 14 | |||||||
| Tuberculosis | Very Unimportant | 18 | 19 | OR 0.82 | [95% CI 0.56–1.19]; | p = 0.3 | 0.85 | [95% CI 0.57–1.29]; | p = 0.5 |
| Unimportant | 36 | 41 | |||||||
| Neutral | 58 | 56 | |||||||
| Important | 54 | 31 | |||||||
| Very important | 15 | 21 | |||||||
| UTI (recurrent) | Very Unimportant | 4 | 5 | 1.22 | [95% CI 0.83–1.79]; | p = 0.3 | 1.38 | [95% CI 0.91–2.12]; | p = 0.13 * |
| Unimportant | 6 | 6 | |||||||
| Neutral | 34 | 23 | |||||||
| Important | 74 | 70 | |||||||
| Very important | 64 | 68 | |||||||
| UTIs | Very Unimportant | 13 | 12 | 1.05 | [95% CI 0.72–1.54]; | p = 0.8 | 1.2 | [95% CI 0.79–1.80]; | p = 0.4 |
| Unimportant | 33 | 28 | |||||||
| Neutral | 53 | 55 | |||||||
| Important | 58 | 38 | |||||||
| Very important | 26 | 34 | |||||||
| Vaginal discharge | Very Unimportant | 10 | 10 | 1 | [95% CI 0.68–1.46]; | p = 0.98 | 1.19 | [95% CI 0.78–1.80]; | p = 0.4 * |
| Unimportant | 32 | 32 | |||||||
| Neutral | 64 | 61 | |||||||
| Important | 55 | 43 | |||||||
| Very important | 15 | 21 | |||||||
References
- Baird, B.; Charles, A.; Honeyman, M.; Maguire, D.; Das, P. Understanding Pressures in General Practice; The King’s Fund: London, UK, 2016. [Google Scholar]
- NHS Digital. GP Appointments. Comparison to Other Collections. 2018. Available online: https://files.digital.nhs.uk/3E/2BC49E/Appointments_GP_QResearch_Comparison_Corrected.pdf (accessed on 19 May 2020).
- Public Health England. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2018–2019; Public Health England: London, UK, 2019.
- Nugent, C.; Patterson, L.; Sartaj, M. Surveillance of Antimicrobial Use and Resistance in Northern Ireland, Annual Report 2018. Available online: https://www.publichealth.hscni.net/sites/default/files/2019-02/AMR%20annual%20report%20final%202018.pdf (accessed on 19 May 2020).
- Public Health Wales. Antibacterial Usage in Primary Care in Wales 2013/14–2017/18. Available online: http://www.wales.nhs.uk/sitesplus/documents/888/Antibacterial%20Usage%20in%20Primary%20Care%20in%20Wales%202013-2017%20%28financial%20years%29.pdf (accessed on 19 May 2020).
- Public Health England. Research Reveals Levels of Inappropriate Prescriptions in England; Public Health England: London, UK, 2018.
- Pouwels, K.B.; Dolk, F.C.K.; Smith, D.R.M.; Robotham, J.V.; Smieszek, T. Actual versus ‘ideal’ antibiotic prescribing for common conditions in English primary care. J. Antimicrob. Chemother. 2018, 73, 19–26. [Google Scholar] [CrossRef]
- Germeni, E.; Frost, J.; Garside, R.; Rogers, M.; Valderas, J.M.; Britten, N. Antibiotic prescribing for acute respiratory tract infections in primary care: An updated and expanded meta-ethnography. Br. J. Gen. Pract. 2018, 68, e633–e645. [Google Scholar] [CrossRef]
- McNulty, C.A.; Smith, G.E.; Graham, C. PHLS primary care consultation--infectious disease and primary care research and service development priorities. Commun. Dis. Public Health 2001, 4, 18–26. [Google Scholar]
- McNulty, C.A.; Thomas, M.D. PHLS laboratory services and primary care needs. Prescriber 2002, 13, 110–115. [Google Scholar]
- NHS Digital. General Practice Workforce, Final 30 September 2018, Experimental Statistics; NHS Digital: London, UK, 2019. [Google Scholar]
- Fryrear, A. What’s a Good Response Rate? Available online: https://www.surveygizmo.com/resources/blog/survey-response-rates/ (accessed on 4 June 2019).
- Porter, B. Tips and Tricks to Improve Survey Response Rate. Available online: https://www.surveymonkey.com/curiosity/improve-survey-response-rate/ (accessed on 3 June 2019).
- NHS Digital. General Practice Trends in the UK to 2017; NHS Digital: London, UK, 2018. [Google Scholar]
- McNulty, C.A.M.; Freeman, E.; Bowen, J.; Shefras, J.; Fenton, K.A. Diagnosis of genital chlamydia in primary care: An explanation of reasons for variation in chlamydia testing. Sex. Transm. Infect. 2004, 80, 207–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radcliffe, K.; Jusuf, I.; Cowan, F.; Fitzgerald, M.; Wilson, J. UK national guidelines on sexually transmitted infections and closely related conditions. Sex. Transm. Infect. 1999, 75, S2–S3. [Google Scholar]
- British Association for Sexual Health and HIV (BASHH). BASHH Guidelines. Available online: https://www.bashh.org/guidelines (accessed on 13 June 2019).
- National Chlamydia Screening Programme (NCSP). Information, Data, Guidance and Resources about the NCSP. Available online: https://www.gov.uk/government/collections/national-chlamydia-screening-programme-ncsp (accessed on 5 June 2019).
- Lewis, J.; White, P.J. Changes in chlamydia prevalence and duration of infection estimated from testing and diagnosis rates in England: A model-based analysis using surveillance data, 2000-15. Lancet Public Health 2018, 3, e271–e278. [Google Scholar] [CrossRef]
- Finch, R.G.; Low, D.E. A critical assessment of published guidelines and other decision-support systems for the antibiotic treatment of community-acquired respiratory tract infections. Clin. Microbiol. Infect. 2002, 8 (Suppl. 2), 69–91. [Google Scholar] [CrossRef] [Green Version]
- Spurling, G.K.P.; Del Mar, C.B.; Dooley, L.; Foxlee, R.; Farley, R. Delayed antibiotic prescriptions for respiratory infections. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [Green Version]
- Hay, A.D.; Redmond, N.M.; Turnbull, S.; Christensen, H.; Thornton, H.; Little, P.; Thompson, M.; Delaney, B.; Lovering, A.M.; Muir, P.; et al. Development and internal validation of a clinical rule to improve antibiotic use in children presenting to primary care with acute respiratory tract infection and cough: A prognostic cohort study. Lancet Respir. Med. 2016, 4, 902–910. [Google Scholar] [CrossRef] [Green Version]
- Centor, R.M.; Witherspoon, J.M.; Dalton, H.P.; Brody, C.E.; Link, K. The diagnosis of strep throat in adults in the emergency room. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 1981, 1, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Little, P.; Hobbs, F.D.; Moore, M.; Mant, D.; Williamson, I.; McNulty, C.; Cheng, Y.E.; Leydon, G.; McManus, R.; Kelly, J.; et al. Clinical score and rapid antigen detection test to guide antibiotic use for sore throats: Randomised controlled trial of PRISM (primary care streptococcal management). BMJ 2013, 347, f5806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, B.; Gaveikaite, V.; Bianchi, C.; Puhan, M.A. Prediction models for exacerbations in patients with COPD. Eur. Respir. Rev. 2017, 26, 160061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundberg, T.; Hellstrom, S.; Sandstrom, H. Development and validation of a new grading scale for otitis media. Pediatric Infect. Dis. J. 2013, 32, 341–345. [Google Scholar] [CrossRef]
- Jones, L.F.; Hawking, M.K.D.; Owens, R.; Lecky, D.; Francis, N.A.; Butler, C.; Gal, M.; McNulty, C.A.M. An evaluation of the TARGET (Treat Antibiotics Responsibly; Guidance, Education, Tools) Antibiotics Toolkit to improve antimicrobial stewardship in primary care—Is it fit for purpose? Fam. Pract. 2017. [Google Scholar] [CrossRef] [Green Version]
- Finch, R.G.; Metlay, J.P.; Davey, P.G.; Baker, L.J. Educational interventions to improve antibiotic use in the community: Report from the International Forum on Antibiotic Resistance (IFAR) colloquium, 2002. Lancet Infect. Dis. 2004, 4, 44–53. [Google Scholar] [CrossRef]
- Tan, M.K.H.; Luo, R.; Onida, S.; Maccatrozzo, S.; Davies, A.H. Venous Leg Ulcer Clinical Practice Guidelines: What is AGREEd? Eur. J. Vasc. Endovasc. Surg. 2019, 57, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. Guidance: Managing Common Infections: Guidance for Primary Care. Available online: https://www.gov.uk/government/publications/managing-common-infections-guidance-for-primary-care (accessed on 7 January 2020).
- National Institute for Health and Care Excellence. Leg Ulcer Infection: Antimicrobial Prescribing. NICE Guideline [NG152]. Available online: https://www.nice.org.uk/guidance/ng152 (accessed on 23 March 2020).
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology 2012, 50, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Head, K.; Chong, L.Y.; Piromchai, P.; Hopkins, C.; Philpott, C.; Schilder, A.G.M.; Burton, M.J. Systemic and topical antibiotics for chronic rhinosinusitis. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [Green Version]
- Rudmik, L.; Soler, Z.M. Medical Therapies for Adult Chronic Sinusitis: A Systematic Review. JAMA 2015, 314, 926–939. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Sinusitis (Acute): Antimicrobial Prescribing NICE Guideline [NG79]. Available online: https://www.nice.org.uk/guidance/ng79 (accessed on 18 January 2020).
- NHS England. Reducing Gram Negative Blood Stream Infections (BSI) across the Whole Health Economy. Available online: https://www.england.nhs.uk/publication/part-a-reducing-gram-negative-blood-stream-infections-bsi-across-the-whole-health-economy/ (accessed on 13 January 2020).
- National Institute for Health and Care Excellence. Antimicrobial Prescribing Guidelines. Available online: https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/antimicrobial-prescribing-guidelines (accessed on 30 January 2020).
- HM Government. Tackling Antimicrobial Resistance 2019–2024. The UK’s Five-Year National Action Plan. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/784894/UK_AMR_5_year_national_action_plan.pdf (accessed on 5 June 2019).
- HM Government. Contained and Controlled. The UK’s 20-Year Vision for Antimicrobial Resistance. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/773065/uk-20-year-vision-for-antimicrobial-resistance.pdf (accessed on 5 June 2019).
- Public Health England. Tuberculosis in England: 2018 Presenting Data to End of 2017. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/774091/TB_Annual_Report_2018_2.pdf (accessed on 3 June 2019).
- National Institute for Health and Care Excellence. Prostatitis (Acute): Antimicrobial Prescribing NICE Guideline [NG110]. Available online: https://www.nice.org.uk/guidance/ng110/history (accessed on 18 January 2020).
- National Institute for Health and Care Excellence. Diverticular Disease: Antimicrobial Prescribing. Available online: https://www.nice.org.uk/guidance/ng147/resources/visual-summary-pdf-6968965213 (accessed on 19 May 2020).
- Kline, K.A.; Bowdish, D.M. Infection in an aging population. Curr. Opin. Microbiol. 2016, 29, 63–67. [Google Scholar] [CrossRef]
- Storey, A. Living Longer: How Our Population Is Changing and Why It Matters; Office for National Statistics, Ed.; 2018. Available online: https://www.ons.gov.uk/releases/livinglongerhowourpopulationischangingandwhyitmatters (accessed on 19 May 2020).
- Dolk, F.; Pouwels, K.; Smith, D.; Robotham, J.; Smieszek, T. Antibiotics in primary care in England: Which antibiotics are prescribed and for which conditions? J. Antimicrob. Chemother. 2018, 73, ii2–ii10. [Google Scholar] [CrossRef]
- Hayward, G.N.; Moore, A.; McKelvie, S.; Lasserson, D.S.; Croxson, C. Antibiotic prescribing for the older adult: Beliefs and practices in primary care. J. Antimicrob. Chemother. 2019, 74, 791–797. [Google Scholar] [CrossRef]
- Poolman, J.T.; Anderson, A.S. Escherichia coli and Staphylococcus aureus: Leading bacterial pathogens of healthcare associated infections and bacteremia in older-age populations. Expert Rev. Vaccines 2018, 17, 607–618. [Google Scholar] [CrossRef]


| Variable | Survey (a)(b) | England (c)(d) [11] * | ||
|---|---|---|---|---|
| Number | Percent of GPs | Number | Percent of GPs | |
| Age (p = 0.260) | n = 367 | n = 44,047 | ||
| 20–30 | 17 | 5% | 2110 | 5% |
| 31–40 | 106 | 29% | 10,363 | 31% |
| 41–50 | 103 | 28% | 9629 | 28% |
| 51–60 | 110 | 30% | 8677 | 24% |
| 60+ | 31 | 8% | 2677 | 8% |
| Unknown | - | 1485 | 3% | |
| Sex (p = 0.183) | n = 363 | n = 43,966 | ||
| Male | 150 | 41% | 19,213 | 44% |
| Female | 213 | 59% | 23,659 | 54% |
| Unknown | 1094 | 2% | ||
| Research Practice (p = 0.019) | n = 361 | n = 7840 | ||
| Yes | 174 | 48% | 3293 | 42% |
| No | 187 | 52% | 4547 | 58% |
| Years in practice | n = 362 | |||
| 0–5 | 75 | 21% | - | - |
| 6–10 | 59 | 16% | - | - |
| 11–15 | 59 | 16% | - | - |
| 16–20 | 45 | 12% | - | - |
| 20+ | 124 | 34% | - | - |
| Region * (p =< 0.05) | n = 288 | n = 44,737 | ||
| North East | 13 | 4% | 2159 | 5% |
| North West | 35 | 12% | 5878 | 13% |
| Yorkshire and Humber | 14 | 5% | 4364 | 10% |
| East Midlands | 22 | 8% | 3490 | 8% |
| West Midlands | 36 | 12% | 4634 | 10% |
| East of England | 11 | 4% | 4463 | 10% |
| London | 28 | 10% | 7175 | 16% |
| South East | 55 | 19% | 7417 | 17% |
| South West | 74 | 26% | 4354 | 10% |
| Unknown | 803 | 2% | ||
| Locality | n = 360 | |||
| urban | 166 | 46% | - | - |
| suburban | 140 | 39% | - | - |
| rural | 54 | 15% | - | - |
| Order of Importance for Evidence to Support Daily Practice | Condition/Illness | Top 3 Ranked by the Need for More Research, Evidence and Guidance | |||
|---|---|---|---|---|---|
| Number of Respondents | Rank | Rank (19998) | Rank | Number of Respondents | |
| 415 | 1 | - | Suspected infection in the elderly | 1 | 115 |
| 417 | 2 | 18 | UTI (recurrent) | 2 | 107 |
| 413 | 3 | 3 | Surveillance of AMR in the community | 1 | 115 |
| 418 | 4 | 5 | Leg ulcers | 5 | 70 |
| 413 | 5 | 17 | Cough (persistent) | 3 | 94 |
| 414 | 6 | 28 | Cellulitis | 4 | 89 |
| 404 | 7 | 6 | Sinusitis (persistent) | 9 | 28 |
| 412 | 8 | - | Prostatitis | 7 | 36 |
| 408 | 9 | - | Diverticulitis | 8 | 30 |
| 412 | 10 | 18 | UTIs | 10 | 25 |
| 409 | 11 | 17 | Cough (acute) | 6 | 47 |
| 406 | 12 | 4 | Vaginal discharge | 8 | 18 |
| 409 | 13 | 1 | Lyme disease | 9 | 28 |
| 411 | 14 | - | Epididymitis/Orchitis | 13 | 20 |
| 411 | 15 | 7 | Otitis externa | 12 | 22 |
| 413 | 16 | 11 | Infection in returning travelers | 11 | 23 |
| 410 | 17 | 6 | Sinusitis (acute) | 17 | 13 |
| 414 | 18 | 24 | Hepatitis viral | 14 | 19 |
| 411 | 19 | 19 | Tuberculosis | 18 | 8 |
| 406 | 20 | 14 | HIV/AIDS | 15 | 16 |
| 418 | 21 | 7 | Otitis media | 16 | 15 |
| 413 | 22 | - | Insect Bites, possible skin infections | 16 | 15 |
| 408 | 23 | 1 | Chlamydia genital | 20 | 4 |
| 415 | 24 | 26 | Fungal nail infections in the community | 22 | 23 |
| 415 | 25 | - | Mastitis | 19 | 7 |
| 415 | 26 | - | AMR in returning travelers | 10 | 25 |
| 414 | 27 | 10 | Tonsillitis/Pharyngitis | 19 | 7 |
| Condition | Need for Better Evidence Base for Antibiotic Treatment in Primary Care | Need for Better Evidence Base for Self-Care and Non-Antibiotic Treatment in Primary Care | Need for Better Near Patient Antibiotic Resistance Test in Primary Care | Need for Improved Treatment Guidelines for Primary Care Staff | Need for Better Clinical Scores to Help Inform Management in Primary Care | Need For Better Point of Care Prognostic Tests In Primary Care | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rank | Mean | Rank | Mean | Rank | Mean | Rank | Mean | Rank | Mean | Rank | Mean | |
| Suspected infection in the elderly | 1 | 4.58 | 4 | 4.25 | 5 | 4.16 | 2 | 4.46 | 6 | 4.15 | 3 | 4.38 |
| UTI (recurrent) | 2 | 4.50 | 1 | 4.53 | 5 | 4.15 | 3 | 4.37 | 6 | 3.94 | 4 | 4.16 |
| Surveillance of AMR in the community | 1 | 4.64 | 2 | 4.60 | 4 | 4.25 | 5 | 4.21 | 6 | 3.98 | 3 | 4.27 |
| Leg Ulcers | 2 | 4.46 | 3 | 4.43 | 5 | 3.92 | 1 | 4.52 | 4 | 4.03 | 6 | 3.91 |
| Cough (persistent) | 3 | 4.31 | 1 | 4.43 | 6 | 3.76 | 2 | 4.42 | 5 | 4.02 | 4 | 4.05 |
| Cellulitis | 1 | 4.61 | 3 | 4.28 | 6 | 3.92 | 2 | 4.37 | 4 | 4.09 | 5 | 4.03 |
| Sinusitis (persistent) | 3 | 4.17 | 1 | 4.54 | 6 | 3.33 | 2 | 4.42 | 4 | 3.87 | 5 | 3.52 |
| Prostatitis | 1 | 4.65 | 3 | 3.94 | 5 | 3.53 | 2 | 4.38 | 3 | 3.94 | 4 | 3.74 |
| Diverticulitis | 1 | 4.48 | 3 | 4.40 | 6 | 3.33 | 2 | 4.41 | 4 | 4.07 | 5 | 3.70 |
| UTIs | 2 | 4.54 | 1 | 4.67 | 4 | 4.33 | 3 | 4.39 | 5 | 4.08 | 6 | 4.00 |
| Cough (acute) | 2 | 4.44 | 1 | 4.57 | 6 | 3.90 | 4 | 4.24 | 5 | 4.02 | 3 | 4.26 |
| Vaginal Discharge | 2 | 4.57 | 3 | 4.17 | 4 | 3.86 | 1 | 4.71 | 6 | 3.57 | 5 | 3.71 |
| Lyme Disease | 2 | 4.50 | 5 | 3.71 | 6 | 3.08 | 1 | 4.54 | 4 | 3.85 | 3 | 3.92 |
| Epididymitis/Orchitis | 1 | 4.42 | 3 | 4.05 | 5 | 3.74 | 2 | 4.37 | 4 | 3.88 | 6 | 3.68 |
| Otitis Externa | 2 | 4.20 | 2 | 4.20 | 5 | 3.25 | 1 | 4.42 | 3 | 3.95 | 4 | 3.60 |
| Infection In Returning Travellers | 1 | 4.57 | 3 | 4.20 | 6 | 4.00 | 2 | 4.48 | 5 | 4.05 | 4 | 4.19 |
| Sinusitis (acute) | 2 | 4.50 | 1 | 4.62 | 5 | 3.58 | 3 | 4.00 | 4 | 3.85 | 3 | 4.00 |
| Hepatitis (viral) | 5 | 3.07 | 3 | 3.64 | 6 | 2.53 | 1 | 4.21 | 2 | 4.20 | 3 | 3.67 |
| Tuberculosis | 1 | 4.43 | 5 | 3.57 | 4 | 3.86 | 1 | 4.43 | 2 | 4.14 | 3 | 4.00 |
| HIV/AIDS | 4 | 3.93 | 2 | 4.14 | 5 | 3.57 | 1 | 4.36 | 4 | 3.93 | 3 | 4.00 |
| Otitis Media | 2 | 4.58 | 1 | 4.67 | 6 | 3.92 | 3 | 4.50 | 4 | 4.25 | 5 | 4.00 |
| Insect Bites, possible skin infections | 2 | 4.29 | 1 | 4.50 | 5 | 3.57 | 3 | 3.93 | 4 | 3.79 | 3 | 3.93 |
| Chlamydia (genital) | 2 | 4.00 | 4 | 2.33 | 1 | 4.33 | 3 | 3.00 | 4 | 2.33 | 2 | 4.00 |
| Fungal nail infections in the community | 3 | 3.84 | 1 | 4.47 | 5 | 3.16 | 2 | 4.37 | 4 | 3.32 | 4 | 3.32 |
| Mastitis | 2 | 4.20 | 3 | 3.75 | 6 | 2.80 | 1 | 4.40 | 4 | 3.67 | 5 | 3.40 |
| AMR in returning travellers | 2 | 4.36 | 3 | 4.25 | 3 | 4.25 | 1 | 4.42 | 4 | 4.09 | 5 | 4.04 |
| Tonsillitis/Pharyngitis | 2 | 4.50 | 1 | 4.67 | 5 | 3.33 | 3 | 4.17 | 3 | 4.17 | 4 | 3.83 |
| Overall scoring | 1 | 4.35 | 3 | 4.21 | 5 | 3.68 | 2 | 4.31 | 4 | 3.90 | 4 | 3.90 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lecky, D.M.; Granier, S.; Allison, R.; Verlander, N.Q.; Collin, S.M.; McNulty, C.A.M. Infectious Disease and Primary Care Research—What English General Practitioners Say They Need. Antibiotics 2020, 9, 265. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9050265
Lecky DM, Granier S, Allison R, Verlander NQ, Collin SM, McNulty CAM. Infectious Disease and Primary Care Research—What English General Practitioners Say They Need. Antibiotics. 2020; 9(5):265. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9050265
Chicago/Turabian StyleLecky, Donna M., Steve Granier, Rosalie Allison, Neville Q. Verlander, Simon M. Collin, and Cliodna A. M. McNulty. 2020. "Infectious Disease and Primary Care Research—What English General Practitioners Say They Need" Antibiotics 9, no. 5: 265. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9050265