Validating Use of Electronic Health Data to Identify Patients with Urinary Tract Infections in Outpatient Settings

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Algorithm Development
2.3. Data Validation
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Durkin, M.J.; Keller, M.; Butler, A.M.; Kwon, J.H.; Dubberke, E.R.; Miller, A.C.; Polgreen, P.M.; Olsen, M.A. An Assessment of Inappropriate Antibiotic Use and Guideline Adherence for Uncomplicated Urinary Tract Infections. Open Forum Infect. Dis. 2018, 5, ofy198. [Google Scholar] [CrossRef] [PubMed]
- Germanos, G.J.; Trautner, B.W.; Zoorob, R.J.; Salemi, J.L.; Drekonja, D.; Gupta, K.; Grigoryan, L. No Clinical Benefit to Treating Male Urinary Tract Infection Longer Than Seven Days: An Outpatient Database Study. Open Forum Infect. Dis. 2019, 6, ofz216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, M.; Shapiro, D.J.; Hersh, A.L.; Sanchez, G.V.; Hicks, L.A. Outpatient Antibiotic Prescribing Practices for Uncomplicated Urinary Tract Infection in Women in the United States, 2002–2011. Open Forum Infect. Dis. 2016, 3, ofw159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landers, T.; Apte, M.; Hyman, S.; Furuya, Y.; Glied, S.; Larson, E. A Comparison of Methods to Detect Urinary Tract Infections Using Electronic Data. Jt. Comm. J. Qual. Patient Saf. 2010, 36, 411–417. [Google Scholar] [CrossRef] [Green Version]
- Matt, V.; Matthew, H. The retrospective chart review: Important methodological considerations. J. Educ. Eval. Health Prof. 2013, 10, 12. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC3853868/ (accessed on 12 March 2020).
- Parsons, A.; McCullough, C.; Wang, J.; Shih, S. Validity of electronic health record-derived quality measurement for performance monitoring. J. Am. Med. Inform. Assoc. 2012, 19, 604–609. [Google Scholar] [CrossRef] [Green Version]
- Gavrielov-Yusim, N.; Friger, M. Use of administrative medical databases in population-based research. J. Epidemiol Community Health 2014, 68, 283–287. [Google Scholar] [CrossRef]
- Chan, K.S.; Fowles, J.B.; Weiner, J.P. Review: Electronic health records and the reliability and validity of quality measures: A review of the literature. Med. Care Res. Rev. 2010, 67, 503–527. [Google Scholar] [CrossRef]
- Kerr, E.A.; Smith, D.M.; Hogan, M.M.; Krein, S.L.; Pogach, L.; Hofer, T.P.; Hayward, R.A. Comparing Clinical Automated, Medical Record, and Hybrid Data Sources for Diabetes Quality Measures. Jt. Comm. J. Qual. Improv. 2002, 28, 555–565. [Google Scholar] [CrossRef]
- Grigoryan, L.; Zoorob, R.; Wang, H.; Trautner, B.W. Low Concordance with Guidelines for Treatment of Acute Cystitis in Primary Care. Open Forum Infect. Dis. 2015, 2, ofv159. [Google Scholar] [CrossRef]
- Hecker, M.T.; Fox, C.J.; Son, A.H.; Cydulka, R.K.; Siff, J.E.; Emerman, C.L.; Sethi, A.K.; Muganda, C.P.; Donskey, C.J. Effect of a Stewardship Intervention on Adherence to Uncomplicated Cystitis and Pyelonephritis Guidelines in an Emergency Department Setting. PLoS ONE 2014, 9, e87899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niska, R.; Bhuiya, F.; Xu, J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Natl. Health Stat. Rep. 2010, 6, 1–31. [Google Scholar]
- Shapiro, D.J.; Hicks, L.A.; Pavia, A.T.; Hersh, A.L. Antibiotic prescribing for adults in ambulatory care in the USA, 2007-09. J. Antimicrob. Chemother. 2014, 69, 234–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, K.; Grigoryan, L.; Trautner, B. Urinary Tract Infection. Ann. Intern. Med. 2017, 167, ITC49–ITC64. [Google Scholar] [CrossRef] [PubMed]
- Colgan, R.; Keating, K.; Dougouih, M. Survey of Symptom Burden in Women with Uncomplicated Urinary Tract Infections. Clin. Drug Investig. 2004, 24, 55–60. [Google Scholar] [CrossRef]
- Foxman, B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am. J. Med. 2002, 113, 5–13. [Google Scholar] [CrossRef]
- Grigoryan, L.; Zoorob, R.; Wang, H.; Horsfield, M.; Gupta, K.; Trautner, B.W. Less workup, longer treatment, but no clinical benefit observed in women with diabetes and acute cystitis. Diabetes Res. Clin. Pract. 2017, 129, 197–202. [Google Scholar] [CrossRef]
- Jhung, M.A.; Banerjee, S.N. Administrative Coding Data and Health Care–Associated Infections. Clin. Infect. Dis. 2009, 49, 949–955. [Google Scholar] [CrossRef] [Green Version]
- Skove, S.L.; Howard, L.E.; Senechal, J.; Hoedt, A.D.; Bresee, C.; Cunningham, T.J.; Barbour, K.E.; Kim, J.; Freedland, S.J.; Anger, J.T. The misdiagnosis of interstitial cystitis/bladder pain syndrome in a VA population. Neurourol. Urodyn. 2019, 38, 1966–1972. [Google Scholar] [CrossRef]
- Tieder, J.S.; Hall, M.; Auger, K.A.; Hain, P.D.; Jerardi, K.E.; Myers, A.L.; Rahman, S.S.; Williams, D.J.; Shah, S.S. Accuracy of Administrative Billing Codes to Detect Urinary Tract Infection Hospitalizations. Pediatrics 2011, 128, 323–330. [Google Scholar] [CrossRef]
- Klompas, M.; Yokoe, D.S. Automated Surveillance of Health Care–Associated Infections. Clin. Infect. Dis. 2009, 48, 1268–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motheral, B.; Brooks, J.; Clark, M.A.; Crown, W.H.; Davey, P.; Hutchins, D.; Martin, B.C.; Stang, P. A Checklist for Retrospective Database Studies—Report of the ISPOR Task Force on Retrospective Databases. Value Health 2003, 6, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livorsi, D.J.; Linn, C.M.; Alexander, B.; Heintz, B.H.; Tubbs, T.A.; Perencevich, E.N. The Value of Electronically Extracted Data for Auditing Outpatient Antimicrobial Prescribing. Infect. Control Hosp. Epidemiol. 2018, 39, 64–70. [Google Scholar] [CrossRef]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trevethan, R. Sensitivity, Specificity, and Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Health 2017, 5, 307. [Google Scholar] [CrossRef]
- Foxman, B. Urinary tract infection syndromes: Occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clin. N. Am. 2014, 28, 1–13. [Google Scholar] [CrossRef]
- Foxman, B.; Gillespie, B.; Koopman, J.; Zhang, L.; Palin, K.; Tallman, P.; Marsh, J.V.; Spear, S.; Sobel, J.D.; Marty, M.J.; et al. Risk Factors for Second Urinary Tract Infection among College Women. Am. J. Epidemiol. 2000, 151, 1194–1205. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Demographic Factors and Identification Algorithms | Overall n = 1087 | Medicine 1 n = 927 | Urology n = 160 | p-Value 2 |
|---|---|---|---|---|
| Age, mean years ± SD | 52.1 ± 17.3 | 51.0 ± 17.1 | 58.5 ± 16.9 | <0.001 |
| Race, n (%) | <0.001 | |||
| White | 611 (56.2) | 491 (53.0) | 120 (75.0) | |
| Black | 244 (22.5) | 229 (24.7) | 15 (9.4) | |
| Hispanic | 59 (5.4) | 48 (5.2) | 11 (6.9) | |
| Other | 67 (6.2) | 65 (7.0) | 2 (1.3) | |
| Unknown | 106 (9.8) | 94 (10.1) | 12 (7.5) | |
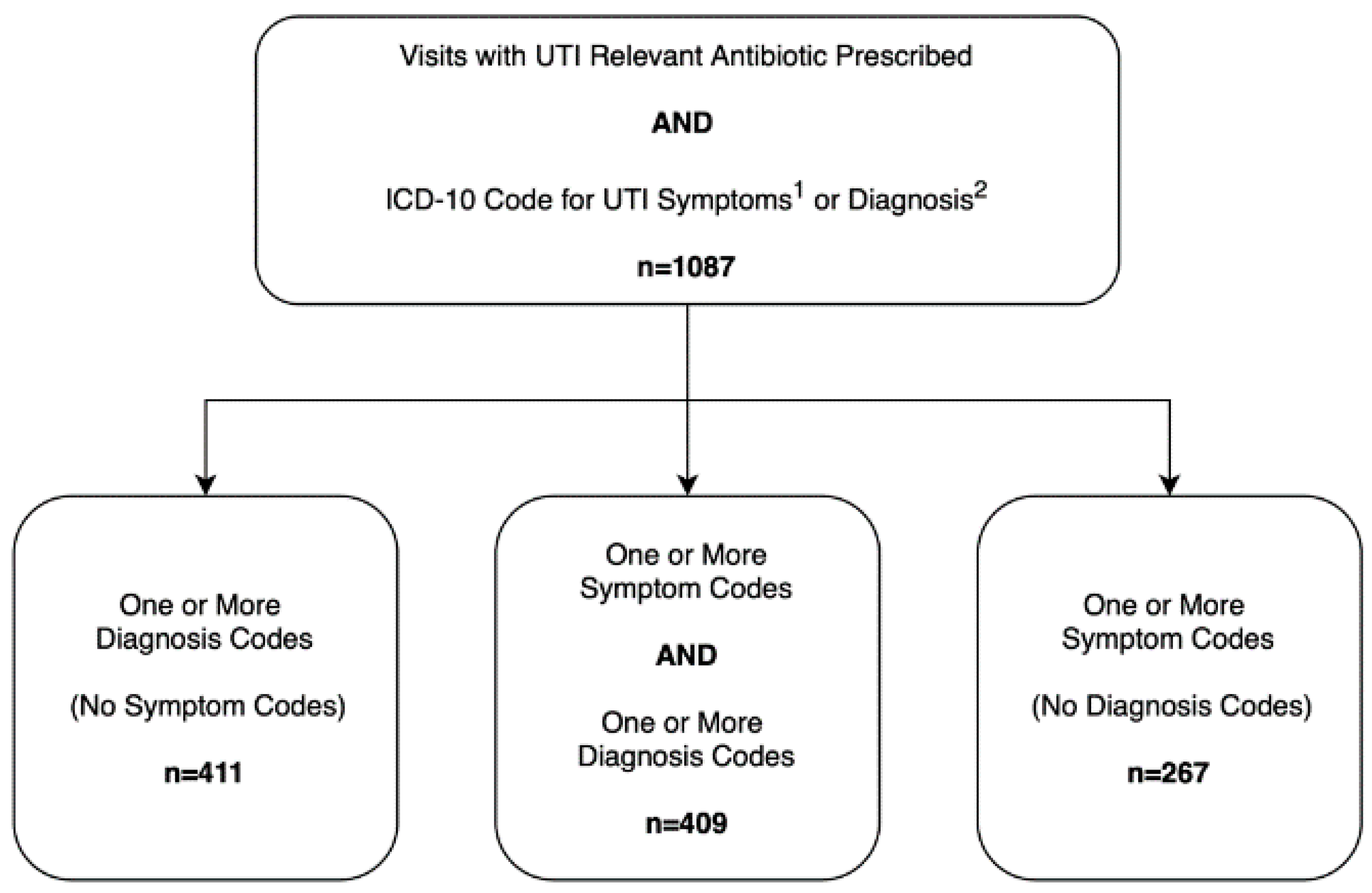
| ICD-10 Identification Algorithm, n (%) | <0.001 | |||
| ICD-10 Symptom Code Only (%) | 267 (24.6) | 251 (27.1) | 16 (10.0) | |
| ICD-10 Diagnosis Code Only (%) | 411 (37.8) | 274 (29.6) | 137 (85.6) | |
| ICD-10 Symptom and Diagnosis Code (%) | 409 (37.6) | 402 (43.4) | 7 (4.4) |
| Uti Identification Criteria | Algorithm-Identified Encounters | Chart-Confirmed Utis | Ppv (%) 95% CI |
|---|---|---|---|
| Overall | |||
| Symptom codes only | 267 | 148 | 55.4 (49.3–61.5%) |
| Diagnosis codes only | 411 | 349 | 84.9 (81.1–88.2%) |
| Symptom and Diagnosis codes | 409 | 394 | 96.3 (94.5–97.9%) |
| Internal and Family Medicine Only | |||
| Symptom codes only | 251 | 147 | 58.6 (52.2–64.7%) |
| Diagnosis codes only | 274 | 258 | 94.2 (90.7–96.6%) |
| Symptom and Diagnosis codes | 402 | 391 | 97.3 (95.2–98.6%) |
| Urology Only | |||
| Symptom codes only | 16 | 1 | 6.3 (0.0–30.2%) |
| Diagnosis codes only | 137 | 91 | 66.4 (57.9–74.3%) |
| Symptom and Diagnosis codes | 7 | 3 | 42.9 (9.9–81.6%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Germanos, G.; Light, P.; Zoorob, R.; Salemi, J.; Khan, F.; Hansen, M.; Gupta, K.; Trautner, B.; Grigoryan, L. Validating Use of Electronic Health Data to Identify Patients with Urinary Tract Infections in Outpatient Settings. Antibiotics 2020, 9, 536. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090536
Germanos G, Light P, Zoorob R, Salemi J, Khan F, Hansen M, Gupta K, Trautner B, Grigoryan L. Validating Use of Electronic Health Data to Identify Patients with Urinary Tract Infections in Outpatient Settings. Antibiotics. 2020; 9(9):536. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090536
Chicago/Turabian StyleGermanos, George, Patrick Light, Roger Zoorob, Jason Salemi, Fareed Khan, Michael Hansen, Kalpana Gupta, Barbara Trautner, and Larissa Grigoryan. 2020. "Validating Use of Electronic Health Data to Identify Patients with Urinary Tract Infections in Outpatient Settings" Antibiotics 9, no. 9: 536. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090536