Extended-Spectrum β-Lactamase-Producing Enterobacterales Shedding by Dogs and Cats Hospitalized in an Emergency and Critical Care Department of a Veterinary Teaching Hospital

 ,
, 
Abstract
:1. Introduction
2. Results
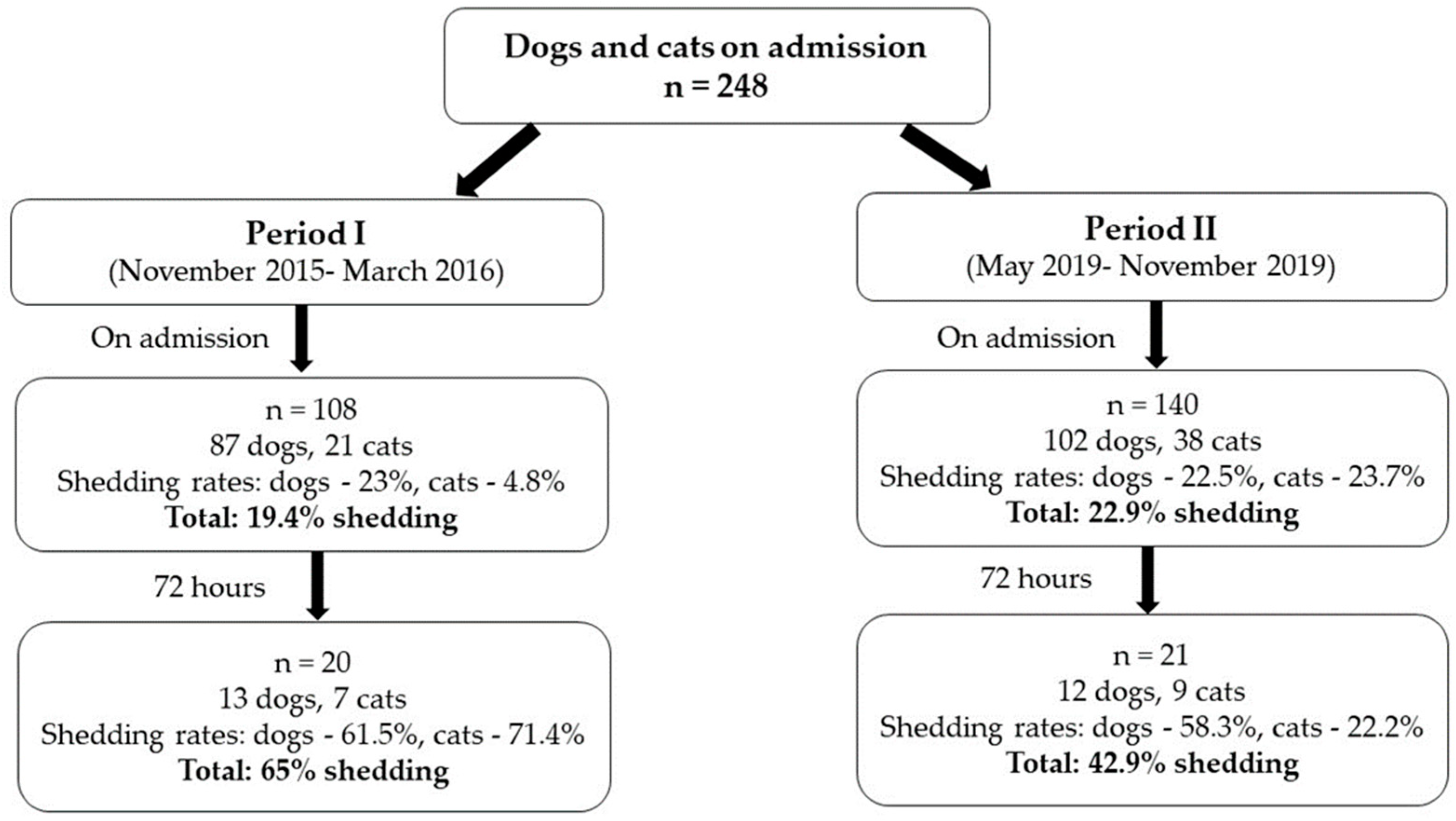
2.1. Population Characteristics
2.2. ESBL-PE Gut Shedding Rates
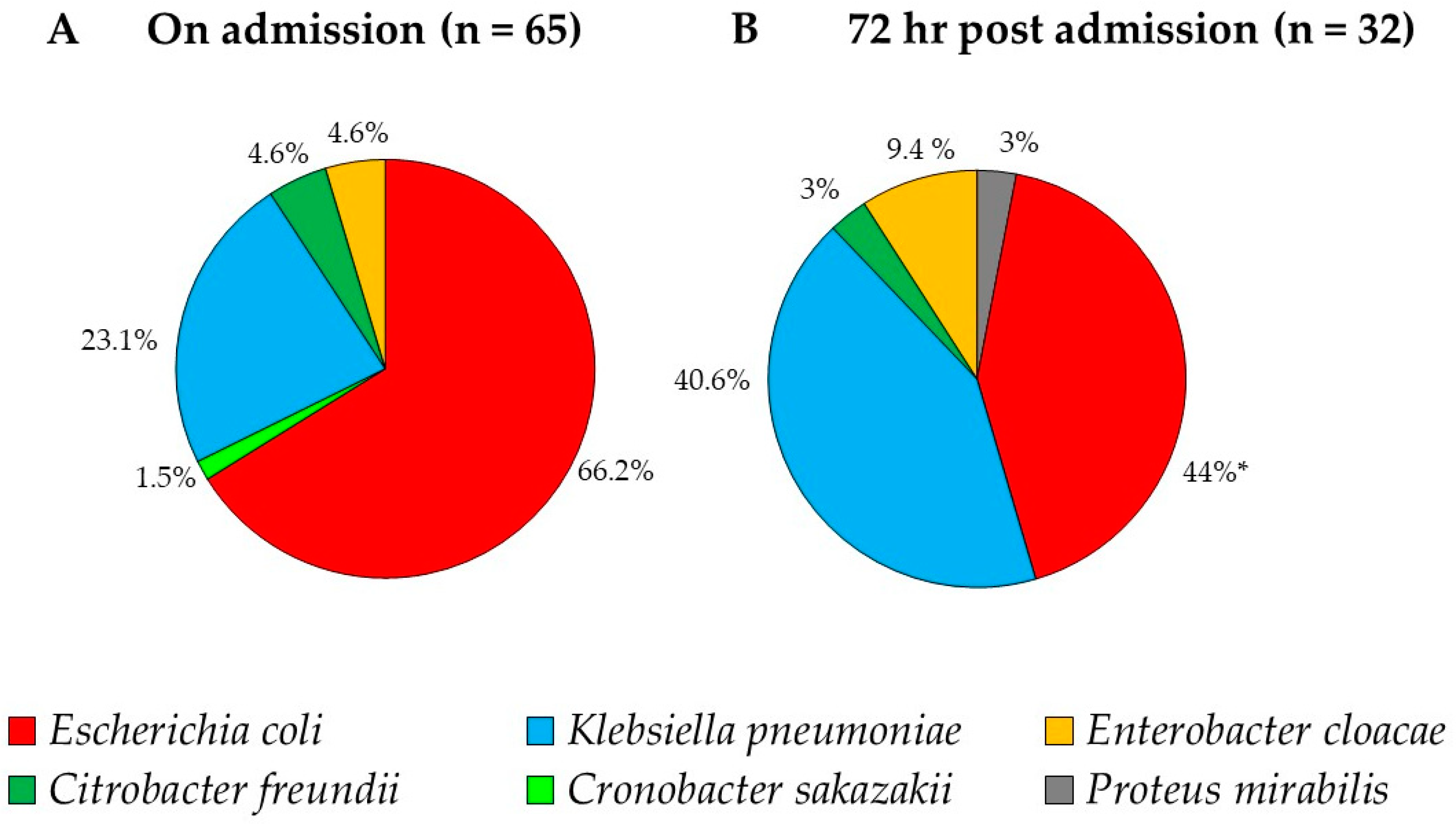
2.3. Distribution of the ESBL-PE Bacterial Species
2.3.1. On Admission
2.3.2. During Hospitalization
2.4. Susceptibility Patterns of the ESBL-PE Isolates
2.5. Risk Factor Analysis for ESBL-PE Gut Shedding
2.5.1. Period I
2.5.2. Period II
2.5.3. Periods I and II
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Isolation of ESBL-PE Gut Shedding and Species Identification
4.3. Demographic and Medical Data
4.4. Statistical and Risk Factor Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pitout, J.D.; Laupland, K.B. Extended-spectrum β-lactamase-producing Enterobacteriaceae: An emerging public-health concern. Lancet Infect. Dis. 2008, 8, 159–166. [Google Scholar] [CrossRef]
- Biehl, L.M.; Schmidt-Hieber, M.; Liss, B.; Cornely, O.A.; Vehreschild, M.J.G.T. Colonization and infection with extended spectrum beta-lactamase producing Enterobacteriaceae in high-risk patients—Review of the literature from a clinical perspective. Crit. Rev. Microbiol. 2016, 42, 1–16. [Google Scholar] [CrossRef]
- Dickstein, Y.; Temkin, E.; Ish Shalom, M.; Schwartz, D.; Carmeli, Y.; Schwaber, M.J. Trends in antimicrobial resistance in Israel, 2014–2017. Antimicrob. Resist. Infect. Control 2019, 8, 96. [Google Scholar] [CrossRef] [Green Version]
- Bert, F.; Larroque, B.; Paugam-Burtz, C.; Dondero, F.; Durand, F.; Marcon, E.; Belghiti, J.; Moreau, R.; Nicolas-Chanoine, M.-H. Pretransplant fecal carriage of extended-spectrum β-lactamase-producing Enterobacteriaceae and infection after liver transplant, France. Emerg. Infect. Dis. 2012, 18, 908–916. [Google Scholar] [CrossRef]
- Liss, B.J.; Vehreschild, J.J.; Cornely, O.A.; Hallek, M.; Fätkenheuer, G.; Wisplinghoff, H.; Seifert, H.; Vehreschild, M.J.G.T. Intestinal colonisation and blood stream infections due to vancomycin-resistant enterococci (VRE) and extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBLE) in patients with haematological and oncological malignancies. Infection 2012, 40, 613–619. [Google Scholar] [CrossRef]
- Martinez, A.E.; Widmer, A.; Frei, R.; Pargger, H.; Tuchscherer, D.; Marsch, S.; Egli, A.; Tschudin-Sutter, S. ESBL-colonization at ICU admission: Impact on subsequent infection, carbapenem-consumption, and outcome. Infect. Control Hosp. Epidemiol. 2019, 40, 408–413. [Google Scholar] [CrossRef]
- Tacconelli, E.; Cataldo, M.A.; Dancer, S.J.; De Angelis, G.; Falcone, M.; Frank, U.; Kahlmeter, G.; Pan, A.; Petrosillo, N.; Rodríguez-Baño, J.; et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clin. Microbiol. Infect. 2014, 20, 1–55. [Google Scholar] [CrossRef] [Green Version]
- Bortolami, A.; Zendri, F.; Maciuca, E.I.; Wattret, A.; Ellis, C.; Schmidt, V.; Pinchbeck, G.; Timofte, D. Diversity, Virulence, and Clinical Significance of Extended-Spectrum β-Lactamase- and pAmpC-Producing Escherichia coli From Companion Animals. Front. Microbiol. 2019, 10, 1260. [Google Scholar] [CrossRef] [Green Version]
- Zogg, A.L.; Simmen, S.; Zurfluh, K.; Stephan, R.; Schmitt, S.N.; Nüesch-Inderbinen, M. High Prevalence of Extended-Spectrum β-Lactamase Producing Enterobacteriaceae Among Clinical Isolates From Cats and Dogs Admitted to a Veterinary Hospital in Switzerland. Front. Vet. Sci. 2018, 5, 62. [Google Scholar] [CrossRef] [Green Version]
- Piccolo, F.L.; Belas, A.; Foti, M.; Fisichella, V.; Marques, C.; Pomba, C. Detection of multidrug resistance and extended-spectrum/plasmid-mediated AmpC beta-lactamase genes in Enterobacteriaceae isolates from diseased cats in Italy. J. Feline Med. Surg. 2020, 22, 613–622. [Google Scholar] [CrossRef]
- Karkaba, A.; Hill, K.; Benschop, J.; Pleydell, E.; Grinberg, A. Carriage and population genetics of extended spectrum β-lactamase-producing Escherichia coli in cats and dogs in New Zealand. Vet. Microbiol. 2019, 233, 61–67. [Google Scholar] [CrossRef]
- Umeda, K.; Hase, A.; Matsuo, M.; Horimoto, T.; Ogasawara, J. Prevalence and genetic characterization of cephalosporin-resistant Enterobacteriaceae among dogs and cats in an animal shelter. J. Med. Microbiol. 2019, 68, 339–345. [Google Scholar] [CrossRef]
- Melo, L.C.; Oresco, C.; Leigue, L.; Netto, H.M.; Melville, P.A.; Benites, N.R.; Saras, E.; Haenni, M.; Lincopan, N.; Madec, J.-Y. Prevalence and molecular features of ESBL/pAmpC-producing Enterobacteriaceae in healthy and diseased companion animals in Brazil. Vet. Microbiol. 2018, 221, 59–66. [Google Scholar] [CrossRef]
- Zhang, P.L.C.; Shen, X.; Chalmers, G.; Reid-Smith, R.J.; Slavic, D.; Dick, H.; Boerlin, P. Prevalence and mechanisms of extended-spectrum cephalosporin resistance in clinical and fecal Enterobacteriaceae isolates from dogs in Ontario, Canada. Vet. Microbiol. 2018, 213, 82–88. [Google Scholar] [CrossRef]
- Marques, C.; Belas, A.; Aboim, C.; Cavaco-Silva, P.; Trigueiro, G.; Gama, L.T.; Pomba, C. Evidence of Sharing of Klebsiella pneumoniae Strains between Healthy Companion Animals and Cohabiting Humans. J. Clin. Microbiol. 2019, 57, e01537-18. [Google Scholar] [CrossRef] [Green Version]
- Van den Bunt, G.; Fluit, A.C.; Spaninks, M.P.; Timmerman, A.J.; Geurts, Y.; Kant, A.; Scharringa, J.; Mevius, D.; Wagenaar, J.A.; Bonten, M.J.M.; et al. Faecal carriage, risk factors, acquisition and persistence of ESBL-producing Enterobacteriaceae in dogs and cats and co-carriage with humans belonging to the same household. J. Antimicrob. Chemother. 2020, 75, 342–350. [Google Scholar] [CrossRef]
- Murk, J.-L.A.N.; Heddema, E.R.; Hess, D.L.J.; Bogaards, J.A.; Vandenbroucke-Grauls, C.M.J.E.; Debets-Ossenkopp, Y.J. Enrichment broth improved detection of extended-spectrum-beta-lactamase-producing bacteria in throat and rectal surveillance cultures of samples from patients in intensive care units. J. Clin. Microbiol. 2009, 47, 1885–1887. [Google Scholar] [CrossRef] [Green Version]
- Shnaiderman-Torban, A.; Navon-Venezia, S.; Dor, Z.; Paitan, Y.; Arielly, H.; Ahmad, W.A.; Kelmer, G.; Fulde, M.; Steinman, A. Extended-Spectrum β-lactamase-Producing Enterobacteriaceae Shedding in Farm Horses Versus Hospitalized Horses: Prevalence and Risk Factors. Animals 2020, 10, 282. [Google Scholar] [CrossRef] [Green Version]
- Ben-Ami, R.; Schwaber, M.J.; Navon-Venezia, S.; Schwartz, D.; Giladi, M.; Chmelnitsky, I.; Leavitt, A.; Carmeli, Y. Influx of Extended-Spectrum β-Lactamase—Producing Enterobacteriaceae into the Hospital. Clin. Infect. Dis. 2006, 42, 925–934. [Google Scholar] [CrossRef] [Green Version]
- Shitrit, P.; Reisfeld, S.; Paitan, Y.; Gottesman, B.-S.; Katzir, M.; Paul, M.; Chowers, M. Extended-spectrum beta-lactamase-producing Enterobacteriaceae carriage upon hospital admission: Prevalence and risk factors. J. Hosp. Infect. 2013, 85, 230–232. [Google Scholar] [CrossRef]
- Joosten, P.; Ceccarelli, D.; Odent, E.; Sarrazin, S.; Graveland, H.; Van Gompel, L.; Battisti, A.; Caprioli, A.; Franco, A.; Wagenaar, J.A.; et al. Antimicrobial Usage and Resistance in Companion Animals: A Cross-Sectional Study in Three European Countries. Antibiotics 2020, 9, 87. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, E.; Kruger, J.M.; Schall, W.; Beal, M.; Manning, S.D.; Kaneene, J.B. Acquisition and persistence of antimicrobial-resistant bacteria isolated from dogs and cats admitted to a veterinary teaching hospital. J. Am. Vet. Med. Assoc. 2013, 243, 990–1000. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.S.; Song, W.; Park, H.-M.; Oh, J.-Y.; Chae, J.-C.; Shin, S.; Jeong, S.H. Clonal Spread of Extended-Spectrum Cephalosporin-Resistant Enterobacteriaceae Between Companion Animals and Humans in South Korea. Front. Microbiol. 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- Gandolfi-Decristophoris, P.; Petrini, O.; Ruggeri-Bernardi, N.; Schelling, E. Extended-spectrum β-lactamase-producing Enterobacteriaceae in healthy companion animals living in nursing homes and in the community. Am. J. Infect. Control 2013, 41, 831–835. [Google Scholar] [CrossRef]
- Shnaiderman-Torban, A.; Paitan, Y.; Arielly, H.; Kondratyeva, K.; Tirosh-Levy, S.; Abells-Sutton, G.; Navon-Venezia, S.; Steinman, A. Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae in Hospitalized Neonatal Foals: Prevalence, Risk Factors for Shedding and Association with Infection. Animals 2019, 9, 600. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, F.A.; Fox, L.; Fox, B.; Viviano, K. Diagnostic and therapeutic challenges for dogs with urinary tract infections caused by extended-spectrum β-lactamase-producing Escherichia coli. J. Am. Vet. Med Assoc. 2018, 253, 850–856. [Google Scholar] [CrossRef]
- Gardiner, B.J.; Stewardson, A.J.; Abbott, I.J.; Peleg, A.Y. Nitrofurantoin and fosfomycin for resistant urinary tract infections: Old drugs for emerging problems. Aust. Prescr. 2019, 42, 14–19. [Google Scholar] [CrossRef]
- FarajzadehSheikh, A.; Veisi, H.; Shahin, M.; Getso, M.; Farahani, A. Frequency of quinolone resistance genes among extended-spectrum β-lactamase (ESBL)-producing Escherichia coli strains isolated from urinary tract infections. Trop. Med. Health 2019, 47, 19. [Google Scholar] [CrossRef] [Green Version]
- Wiener, E.S.; Heil, E.L.; Hynicka, L.M.; Johnson, J.K. Are Fluoroquinolones Appropriate for the Treatment of Extended-Spectrum β-Lactamase-Producing Gram-Negative Bacilli? J. Pharm. Technol. 2016, 32, 16–21. [Google Scholar] [CrossRef]
- Tacão, M.; Moura, A.; Correia, A.; Henriques, I. Co-resistance to different classes of antibiotics among ESBL-producers from aquatic systems. Water Res. 2014, 48, 100–107. [Google Scholar] [CrossRef]
- Ekakoro, J.E.; Okafor, C.C. Antimicrobial use practices of veterinary clinicians at a veterinary teaching hospital in the United States. Vet. Anim. Sci. 2019, 7, 100038. [Google Scholar] [CrossRef]
- Kiddee, A.; Assawatheptawee, K.; Na-udom, A.; Boonsawang, P.; Treebupachatsakul, P.; Walsh, T.R.; Niumsup, P.R. Risk Factors for Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae Carriage in Patients Admitted to Intensive Care Unit in a Tertiary Care Hospital in Thailand. Microb. Drug Resist. 2019, 25, 1182–1190. [Google Scholar] [CrossRef]
- Massart, N.; Camus, C.; Benezit, F.; Moriconi, M.; Fillatre, P.; Le Tulzo, Y. Incidence and risk factors for acquired colonization and infection due to extended-spectrum beta-lactamase-producing Gram-negative bacilli: A retrospective analysis in three ICUs with low multidrug resistance rate. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 889–895. [Google Scholar] [CrossRef]
- Razazi, K.; Rosman, J.; Phan, A.-D.; Carteaux, G.; Decousser, J.-W.; Woerther, P.L.; de Prost, N.; Brun-Buisson, C.; Dessap, A.M. Quantifying risk of disease due to extended-spectrum β-lactamase producing Enterobacteriaceae in patients who are colonized at ICU admission. J. Infect. 2020, 80, 504–510. [Google Scholar] [CrossRef]
- Otter, J.A.; Natale, A.; Batra, R.; Auguet, O.T.; Dyakova, E.; Goldenberg, S.D.; Edgeworth, J.D. Individual- and community-level risk factors for ESBL Enterobacteriaceae colonization identified by universal admission screening in London. Clin. Microbiol. Infect. 2019, 25, 1259–1265. [Google Scholar] [CrossRef]
- Detsis, M.; Karanika, S.; Mylonakis, E. ICU Acquisition Rate, Risk Factors, and Clinical Significance of Digestive Tract Colonization With Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae: A Systematic Review and Meta-Analysis. Crit. Care Med. 2017, 45, 705–714. [Google Scholar] [CrossRef]
- Birgand, G.; Armand-Lefevre, L.; Lolom, I.; Ruppe, E.; Andremont, A.; Lucet, J.-C. Duration of colonization by extended-spectrum β-lactamase-producing Enterobacteriaceae after hospital discharge. Am. J. Infect. Control 2013, 41, 443–447. [Google Scholar] [CrossRef]
- Li, B.; Zhong, Y.; Fu, X.; Qiu, Y.; Wang, S.; Yang, A.J.; Huang, X. Duration of Stool Colonization in Healthy Medical Students with Extended-Spectrum-β-Lactamase-Producing Escherichia coli. Antimicrob. Agents Chemother. 2012, 56, 4558–4559. [Google Scholar] [CrossRef] [Green Version]
- Nordberg, V.; Jonsson, K.; Giske, C.G.; Iversen, A.; Aspevall, O.; Jonsson, B.; Camporeale, A.; Norman, M.; Navér, L. Neonatal intestinal colonization with extended-spectrum β-lactamase–producing Enterobacteriaceae—A 5-year follow-up study. Clin. Microbiol. Infect. 2018, 24, 1004–1009. [Google Scholar] [CrossRef] [Green Version]
- Baede, V.O.; Wagenaar, J.A.; Broens, E.M.; Duim, B.; Dohmen, W.; Nijsse, R.; Timmerman, A.J.; Hordijk, J. Longitudinal Study of Extended-Spectrum-β-Lactamase- and AmpC-Producing Enterobacteriaceae in Household Dogs. Antimicrob. Agents Chemother. 2015, 59, 3117–3124. [Google Scholar] [CrossRef] [Green Version]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing, 26th ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2016. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing, 29th ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2019. [Google Scholar]
- Falagas, M.E.; Karageorgopoulos, D.E. Pandrug resistance (PDR), extensive drug resistance (XDR), and multidrug resistance (MDR) among Gram-negative bacilli: Need for international harmonization in terminology. Clin. Infect. Dis. 2008, 46, 1121–1122. [Google Scholar] [CrossRef] [Green Version]
- Gilliver, S.; Valveny, N. How to interpret and report the results from multivariable analyses. MEW 2016, 25, 37–42. [Google Scholar]
- Abramson, J.H. WINPEPI updated: Computer programs for epidemiologists, and their teaching potential. Epidemiol. Perspect. Innov. 2011, 8, 1. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Period | Animal | Antibiotic Therapy Within A Year Prior To Admission (% Valid Percentage) 1 | |||||
|---|---|---|---|---|---|---|---|
| Penicillins 2 | Amoxicillin-Clavulanate | Cephalosporins 3 | Quinolones | Doxycycline | Metronidazole | ||
| I | Dogs (n = 87) | 13.5 | 4.1 | 4.1 | 4.1 | 1.4 | 4.2 |
| Cats (n = 21) | 13.3 | 13.3 | 0 | 13.3 | 0 | 13.3 | |
| Total (n = 108) | 13.5 | 5.7 | 3.4 | 5.7 | 1.1 | 5.7 | |
| II | Dogs (n = 102) | 4.9 | 8.5 | 3.7 | 3.7 | 6.1 | 3.7 |
| Cats (n = 38) | 0 | 9.7 | 6.5 | 0 | 3.2 | 0 | |
| Total (n = 140) | 3.5 | 8.8 | 4.5 | 2.7 | 5.3 | 2.7 | |
| I & II | Dogs (n = 189) | 9 | 6.9 | 3.9 | 3.9 | 3.9 | 3.9 |
| Cats (n = 59) | 4.3 | 11.9 | 4.3 | 4.3 | 2.2 | 4.3 | |
| Total (n = 248) | 8 | 7.6 | 4.1 | 4 | 3.5 | 4.1 | |
| Period | Animal | ESBL Gut Shedding Rate | ||
|---|---|---|---|---|
| on Admission % (Frequency, 95% CI) | At 72 h % (Frequency, 95% CI) | p-Value 1 | ||
| I | Dogs (n = 87) | 23 (20/87, 14.6–33.3) | 61.5 (8/13, 31.6–86.1) | 0.007 * |
| Cats (n = 21) | 4.8 (1/21, 0.1–23.8) | 71.4 (5/7, 29–96.3) | 0.001 * | |
| Total (n = 108) | 19.4 (21/108, 12.5–28.2) | 65 (13/20, 40.8–84.6) | <0.001 * | |
| II | Dogs (n = 102) | 22.5(23/102, 14.9–31.9) | 58.3 (7/12, 27.7–84.8) | 0.014 * |
| Cats (n = 38) | 23.7 (9/38, 11.4–40.2) | 22.2 (2/9, 2.8–60) | 1 | |
| Total (n = 140) | 22.9 (32/140, 16.2–30.7) | 42.9 (9/21, 21.8–69.0) | 0.062 | |
| I & II | Dogs (n = 189) | 22.8 (43/189, 17–29.4) | 60 (15/25, 39.7–78.9) | <0.001 * |
| Cats (n = 59) | 16.9 (10/59, 8.4, 29) | 43.8 (7/16, 19.8–70.1) | 0.04 * | |
| Total (n = 248) | 21.4 (n = 53/248, 16.4–27.0) | 53.7 1 (n = 22/41, 37.4–69.3) | <0.001 * | |
| Period | Sampling (Number of Isolates) | AMC (95% CI) | OFL (95% CI) | AMK (95% CI) | GEN (95% CI) | TMS (95% CI) | NIT (95% CI) | MDR (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Period I | Admission (n = 26) | 100 (86.7–100) | 44 (24.4–65.1) | 3.8 (0.1–19.6) | 15.4 (4.4–34.9) | 65.4 (44.3–82.8) | 7.7 (0.9–25.13) | 69.2 (48.2–85.7) |
| 72 h post admission (n = 19) | 69.2 1 (38.6–90.9) | 87.5 3 (61.7–98.5) | 0 (0–17.7) | 41.2 (18.4–67.1) | 88.2 (63.6–98.5) | 5.9 (0.2–28.7) | 94.4 (72.7–99.9) | |
| Period II | Admission (n = 39) | 28.2 2 (15–44.9) | 53.9 (37.2–69.9) | 0 (0–9) | 38.5 (23.4–55.4) | 71.8 (55.1–85) | 17.95 (7.5–33.5) | 61.5 (44.6–77.6) |
| 72 h post admission (n = 13) | 46.2 (19.2–74.9) | 100 4 (73.5–100) | 0 (0–24.7) | 38.5 (13.9–68.4) | 84.6 (54.5–98.1) | 53.85 5,6 (25.2–80.8) | 92.3 7 (64–99.8) |
| Period | Period I | Period II | Period I & II | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables (p-Value) | Dogs | Cats | Dogs & Cats | Dogs | Cats | Dogs & Cats | Dogs | Cats | Dogs & Cats | |
| Demographics | Species 1 | 0.07 6 | 0.89 | 0.38 | ||||||
| Gender 2 | 0.52 | 0.41 | 0.42 | 0.29 | 0.41 | 0.7 | 0.87 | 0.23 | 0.98 | |
| Breed | 0.82 | 1 | 0.62 | 0.63 | 0.64 | 0.62 | 0.75 | 0.78 | 0.77 | |
| Age | 0.87 | NI 5 | 0.94 | 0.36 | 0.27 | 0.74 | 0.44 | 0.23 | 0.81 | |
| Weight | 0.8 | 0.57 | 0.45 | 0.01 *,6 | 0.08 | 0.03 *,6 | 0.04 *,6 | 0.19 6 | 0.048 *,6 | |
| Medical background | Previous admission to a veterinary clinic 3 | 0.26 | 1 | 0.22 | 1 | 0.03 *,6 | 0.16 6 | 0.52 | 0.17 6 | 0.89 |
| Previous hospitalization 3 | 1 | 1 | 1 | 0.24 | 0.03 *,6 | 0.02 *,6 | 0.313 | 0.02 *,6 | 0.035 *,6 | |
| Length of illness before admission | 0.4 | NI | 0.35 | 0.88 | 0.77 | 0.93 | 0.66 | 0.77 | 0.49 | |
| Previous antibiotic treatments 3 | Antibiotic treatment (yes/no) | 0.73 | 0.4 | 0.54 | 0.92 | 1 | 0.74 | 0.85 | 1 | 0.92 |
| Penicillins 4 | 0.66 | 0.13 | 0.37 | 1 | NI | 1 | 1 | 0.28 | 0.51 | |
| Amoxicillin-clavulanate | 0.42 | 0.13 | 0.16 | 0.19 6 | 1 | 0.12 6 | 0.69 | 1 | 0.74 | |
| Cephalosporines | 1 | NI | 1 | 1 | 1 | 0.59 | 0.6 | 1 | 0.36 | |
| Quinolones | 0.42 | 0.13 | 0.16 | 0.55 | NI | 0.53 | 0.35 | 0.28 | 0.18 | |
| Doxycycline | 1 | NI | 1 | 0.33 | 1 | 0.61 | 0.35 | 1 | 0.62 | |
| Metronidazole | 0.43 | 1 | 1 | 0.55 | NI | 0.53 | 0.35 | 1 | 0.652 | |
| Clinical syndrome on admission | Neurological disease | 0.73 | 1 | 1 | 0.56 | 0.63 | 0.4 | 0.4 | 1 | 0.45 |
| Injury | 1 | 1 | 1 | 0.45 | 0.31 | 0.12 6 | 0.57 | 0.19 6 | 0.11 6 | |
| Cardiovascular disease | 0.07 6 | 1 | 0.21 | 1 | 0.66 | 0.76 | 0.22 | 0.67 | 0.58 | |
| Hematologic disease | 0.68 | 0.053 | 1 | 0.028 *,6 | 1 | 0.14 6 | 0.25 | 0.51 | 0.27 | |
| Gastro-intestinal disease | 0.54 | 1 | 0.59 | 0.49 | 1 | 0.46 | 0.37 | 1 | 0.4 | |
| Endocrinopathy | NI | NI | NI | 1 | 1 | 0.57 | 1 | 1 | 0.58 | |
| Hepatic disease | 0.046 *,6 | 1 | 0.09 6 | 0.57 | 1 | 0.68 | 0.62 | 1 | 0.72 | |
| Reproduction related disease | 1 | NI | 1 | 0.59 | NI | 0.59 | 0.2 | NI | 0.21 | |
| Respiratory | 0.02 *,6 | 1 | 0.055 6 | 0.04 *,6 | 1 | 0.04 *,6 | 0.82 | 0.67 | 0.8 | |
| Orthopedic | 0.68 | 1 | 1 | 1 | 0.56 | 0.3 | 0.53 | 0.58 | 0.26 | |
| Intoxication | 1 | NI | 1 | 0.41 | 1 | 0.54 | 0.66 | 1 | 0.68 | |
| Ophthalmological | 1 | 1 | 1 | 0.57 | 0.22 | 1 | 0.6 | 0.3 | 1 | |
| Tumor | 0.29 | NI | 0.46 | 0.59 | 0.56 | 0.95 | 0.62 | 1 | 0.55 | |
| Urinary-tract disease | 1 | 1 | 0.73 | 1 | 0.37 | 0.56 | 0.8 | 0.42 | 0.94 | |
| Outcomes | Hospital discharge (yes/no) | 0.73 | 0.08 | 0.75 | 0.76 | 0.37 | 0.8 | 0.55 | 1 | 0.78 |
| ESBL-PE gut shedding 72 h post admission | 1 | 1 | 1 | 0.24 | 0.17 | 0.03 * | 0.23 | 0.6 | 1 | |
| Length of stay | 0.48 | 0.56 | 0.45 | 0.14 7 | 0.9 | 0.23 | 0.44 | 1 | 0.55 | |
| Length of stay excluding dead | 0.52 | 8 | 0.27 | 0.28 | 0.57 | 0.57 | 0.96 | |||
| Period | Period I | Period II | Periods I & II | ||||
|---|---|---|---|---|---|---|---|
| Variable (p-Value, OR, 95% CI) | Dogs | Dogs & Cats | Dogs | Cats | Dogs & Cats | Cats | Dogs & Cats |
| Species 1 | NI 3 | 0.09 OR = 0.16 0.02–1.35 | NI | NI | NI | NI | NI |
| Previous admission to a veterinary clinic 2 | NI | NI | NI | 0.999 | 0.14 OR = 0.19 95% CI 0.03–1.47 | 0.774 OR = 0.7 95% CI 0.6–7.6 | NI |
| Previous hospital admission 2 | NI | NI | NI | 0.92 OR = 0.76 0.002–232 | 0.095 OR = 5.82 1.28–7.27 | 0.56 OR = 0.7 95% CI 0.6–7.6 | 0.01 * OR = 3.05 1.28–7.27 |
| Amoxicillin-clavulanate before admission 2 | NI | NI | >0.99 | NI | 0.999 | NI | NI |
| Injury on admission | NI | NI | NI | NI | 0.999 | 0.999 | 0.4 OR = 0.51 0.11–2.4 |
| Cardiovascular disease on admission | 0.42 OR = 2.05 0.36–11.74 | NI | NI | NI | NI | NI | NI |
| Hematologic disease on admission | NI | NI | 0.12 OR = 4.35 0.68–27.84 | NI | 0.35 OR = 2.54 0.36–17.86 | NI | NI |
| Hepatic disease on admission | 1 | 0.069 | NI | NI | NI | NI | NI |
| Respiratory disease on admission | 0.08 OR = 3.43 0.87–13.49 | 0.029 * OR = 3.63 1.15–11.5 | >0.99 | 0.99 | 0.998 | NI | NI |
| Weight (Kg) | NI | NI | 0.014 * OR = 1.07 1.01–1.13 | 0.07 OR = 3.69 0.89–15.26 | 0.011 * OR = 1.1 1.02–1.19 | 0.3 OR = 1.33 0.78–2.25 | 0.07 OR = 1.02 0.99–1.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shnaiderman-Torban, A.; Navon-Venezia, S.; Kelmer, E.; Cohen, A.; Paitan, Y.; Arielly, H.; Steinman, A. Extended-Spectrum β-Lactamase-Producing Enterobacterales Shedding by Dogs and Cats Hospitalized in an Emergency and Critical Care Department of a Veterinary Teaching Hospital. Antibiotics 2020, 9, 545. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090545
Shnaiderman-Torban A, Navon-Venezia S, Kelmer E, Cohen A, Paitan Y, Arielly H, Steinman A. Extended-Spectrum β-Lactamase-Producing Enterobacterales Shedding by Dogs and Cats Hospitalized in an Emergency and Critical Care Department of a Veterinary Teaching Hospital. Antibiotics. 2020; 9(9):545. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090545
Chicago/Turabian StyleShnaiderman-Torban, Anat, Shiri Navon-Venezia, Efrat Kelmer, Adar Cohen, Yossi Paitan, Haya Arielly, and Amir Steinman. 2020. "Extended-Spectrum β-Lactamase-Producing Enterobacterales Shedding by Dogs and Cats Hospitalized in an Emergency and Critical Care Department of a Veterinary Teaching Hospital" Antibiotics 9, no. 9: 545. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090545