Current Antibiotic Resistance Trends of Uropathogens in Central Europe: Survey from a Tertiary Hospital Urology Department 2011–2019


Abstract
:1. Introduction
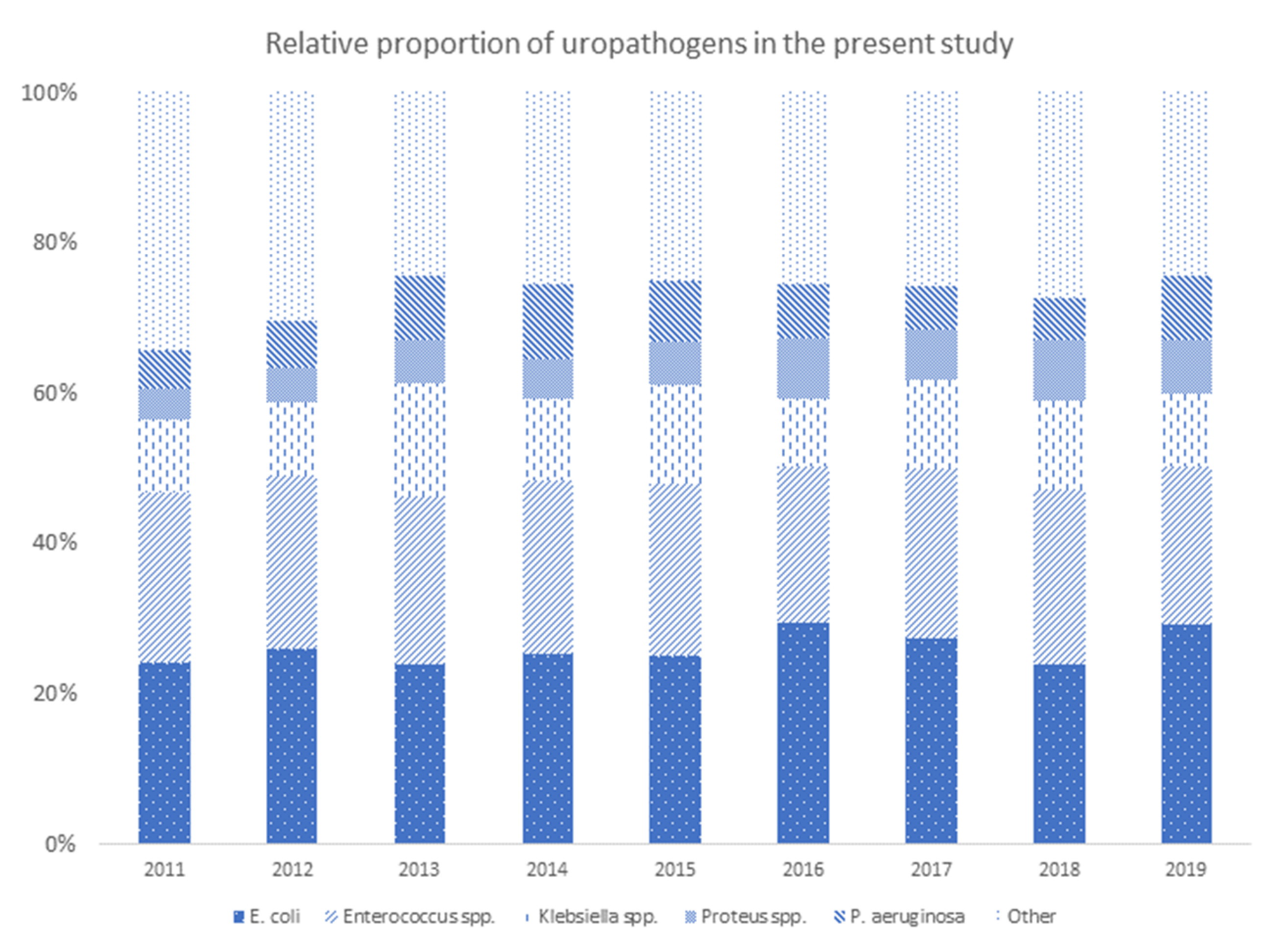
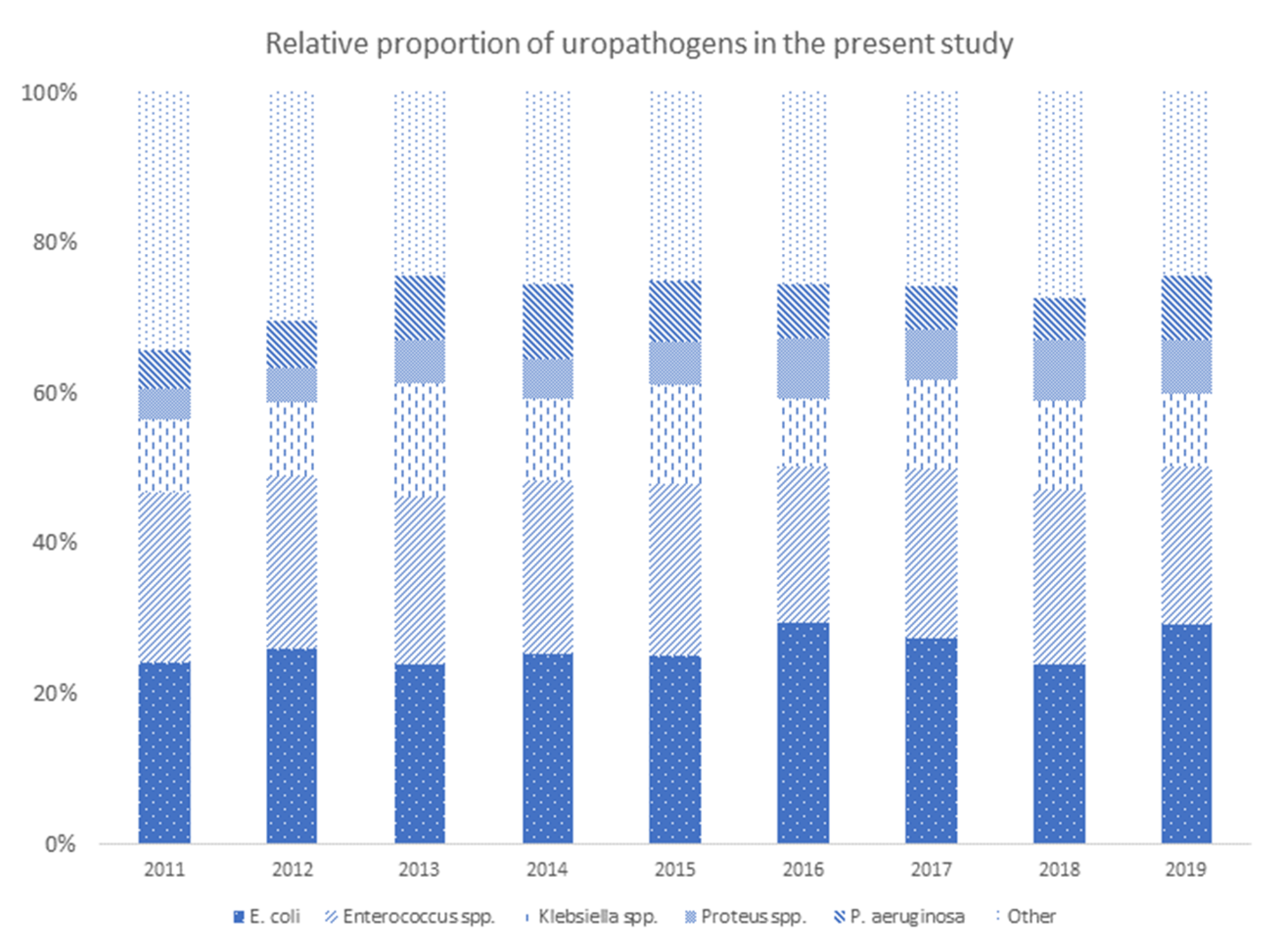
2. Results
2.1. Penicillin Derivatives
2.2. Cephalosporines
2.3. Fluoroquinolones
2.4. Aminoglycosides
2.5. Carbapenems
2.6. Co-Trimoxazole and Nitrofurantoin
2.7. Vancomycin and Colistin
3. Discussion
4. Materials and Methods
Culture Methods and Susceptibility Testing
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Manyi-Loh, C.; Mamphweli, S.; Meyer, E.; Okoh, A. Antibiotic use in agriculture and its consequential resistance in environmental sources: Potential public health implications. Molecules 2018, 23, 795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonkat, G.; Müller, G.; Braissant, O.; Frei, R.; Tschudin-Suter, S.; Rieken, M.; Wyler, S.; Gasser, T.C.; Bachmann, A.; Widmer, A.F. Increasing prevalence of ciprofloxacin resistance in extended-spectrum-beta-lactamase-producing Escherichia coli urinary isolates. World J. Urol. 2013, 31, 1427–1432. [Google Scholar] [CrossRef] [PubMed]
- Iacchini, S.; Sabbatucci, M.; Gagliotti, C.; Rossolini, G.M.; Moro, M.L.; Iannazzo, S.; D’Ancona, F.; Pezzotti, P.; Pantosti, A. Bloodstream infections due to carbapenemas eproducing Enterobacteriaceae in Italy: Results from nationwide surveillance, 2014 to 2017. Eurosurveillance 2019, 24, 1800159. [Google Scholar] [CrossRef]
- Cullen, I.M.; Manecksha, R.P.; Mccullagh, E.; Ahmad, S.; O’Kelly, F.; Flynn, R.J.; McDermott, T.; Murphy, P.; Grainger, R.; Fennell, J.P.; et al. The changing pattern of antimicrobial resistance within 42 033 Escherichia coli isolates from nosocomial, community and urology patient-specific urinary tract infections, Dublin, 1999–2009. BJUI Int. 2011, 109, 1198–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lob, S.H.; Nicolle, L.E.; Hoban, D.J.; Kazmierczak, K.M.; Badal, R.E.; Sahm, D.F. Susceptibility patterns and ESBL rates of Escherichia coli from urinary tract infections in Canada and the United States, SMART 2010–2014. Diagn. Microbiol. Infect. Dis. 2016, 85, 459–465. [Google Scholar] [CrossRef]
- Guyomard-Rabenirina, S.; The Laboratory Working Group; Malespine, J.; Ducat, C.; Sadikalay, S.; Falord, M.; Harrois, D.; Richard, V.; Dozois, C.; Breurec, S.; et al. Temporal trends and risks factors for antimicrobial resistant Enterobacteriaceae urinary isolates from outpatients in Guadeloupe. BMC Microbiol. 2016, 16, 121. [Google Scholar] [CrossRef] [Green Version]
- Sierra-Díaz, E.; Hernández-ríos, C.J.; Bravo-cuellar, A. Antibiotic resistance: Microbiological profile of urinary tract infections in Mexico. Cir. Cir. 2019, 87, 176–182. [Google Scholar] [CrossRef]
- Okeke, I.N.; Laxminarayan, R.; Bhutta, Z.A.; Duse, A.G.; Jenkins, P.; O’Brien, T.F.; Pablos-Mendez, A.; Klugman, K.P. AMR Resistance in developing countries. Lancet Infect. Dis. 2005, 5, 481–493. [Google Scholar] [CrossRef]
- Fasugba, O.; Mitchell, B.G.; Mnatzaganian, G.; Das, A.; Collignon, P.; Gardner, A. Five-Year Antimicrobial Resistance Patterns of Urinary Escherichia coli at an Australian Tertiary Hospital: Time Series Analyses of Prevalence Data. PLoS ONE 2016, 11, e0164306. [Google Scholar] [CrossRef] [Green Version]
- Hyun, M.; Noh, C.I.; Ryu, S.Y.; Kim, H.A. Changing trends in clinical characteristics and antibiotic susceptibility of Klebsiella pneumoniae bacteremia. Korean J. Intern. Med. 2018, 33, 595–603. [Google Scholar] [CrossRef] [Green Version]
- Karlowsky, J.A.; Hoban, D.J.; Hackel, M.A.; Lob, S.H.; Sahm, D.F. Antimicrobial susceptibility of Gram-negative ESKAPE pathogens isolated from hospitalized patients with intra-abdominal and urinary tract infections in Asia-Pacific countries: SMART 2013–2015. J. Med. Microbiol. 2017, 66, 61–69. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 2019 Antibacterial Agents in Clinical Development: An Analysis of the Antibacterial Clinical Development Pipeline; WHO: Geneva, Switzerland, 2019; Available online: https://www.who.int/medicines/areas/rational_use/antibacterial_agents_clinical_development/en/ (accessed on 24 April 2020).
- Frost, I.; Van Boeckel, T.P.; Pires, J.; Craig, J.; Laxminarayan, R. Global geographic trends in antimicrobial resistance: The role of international travel. J. Travel Med. 2019, 26, taz036. [Google Scholar] [CrossRef] [PubMed]
- Zowawi, H.M.; Harris, P.N.A.; Roberts, M.J.; Tambyah, P.A.; Schembri, M.A.; Pezzani, M.D.; Williamson, D.A.; Paterson, D. The emerging threat of multidrug-resistant Gram-negative bacteria in urology. Nat. Rev. Urol. 2015, 12, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, A.; Schaeffer, E. Infections of the urinary tract. In Campbell-Walsh Urology, 10th ed.; Wein, A., Kavoussi, L., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2012; pp. 258–260. [Google Scholar]
- François, M.; Hanslik, T.; Dervaux, B.; Le Strat, Y.; Souty, C.; Vaux, S.; Maugat, S.; Rondet, C.; Sarazin, M.; Heym, B.; et al. The economic burden of urinary tract infections in women visiting general practices in France: A cross-sectional survey. BMC Health Serv. Res. 2016, 16, 365. [Google Scholar] [CrossRef]
- Vallejo-Torres, L.; Pujol, M.; Shaw, E.; Wiegand, I.; Vigo, J.M.; Stoddart, M.; Grier, S.; Gibbs, J.; Vank, C.; Cuperus, N.; et al. Cost of hospitalised patients due to complicated urinary tract infections: A retrospective observational study in countries with high prevalence of multidrug-resistant Gram-negative bacteria: The COMBACTE-MAGNET, RESCUING study. BMJ Open 2018, 8, e020251. [Google Scholar] [CrossRef]
- Stapleton, P.J.; Lundon, D.J.; McWade, R.; Scanlon, N.; Hannan, M.M.; O’Kelly, F.; Lynch, M. Antibiotic resistance patterns of Escherichia coli urinary isolates and comparison with antibiotic consumption data over 10 years, 2005–2014. Ir. J. Med. Sci. 2017, 186, 733–741. [Google Scholar] [CrossRef]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [Green Version]
- Kandil, H.; Cramp, E.; Vaghela, T. Trends in Antibiotic Resistance in Urologic Practice. Eur. Urol. Focus 2016, 2, 363–373. [Google Scholar] [CrossRef]
- Adriaenssens, N.; Coenen, S.; Versporten, A.; Muller, A.; Minalu, G.; Faes, C.; Vankerckhoven, V.; Aerts, M.; Hens, N.; Molenberghs, G.; et al. European Surveillance of Antimicrobial Consumption (ESAC): Outpatient antibiotic use in Europe (1997–2009). J. Antimicrob. Chemother. 2011, 66, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Durkin, M.J.; Keller, M.; Butler, A.M.; Kwon, J.H.; Dubberke, E.R.; Miller, A.C.; Polgreen, P.M.; Olsen, M.A. An assessment of inappropriate antibiotic use and guideline adherence for uncomplicated urinary tract infections. Open Forum Infect. Dis. 2018, 5, ofy198. [Google Scholar] [CrossRef]
- Fleming-Dutra, K.; Hersh, A.L.; Shapiro, D.J. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010–2011. JAMA 2016, 315, 1865–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chardavoyne, P.C.; Kasmire, K.E. Appropriateness of Antibiotic Prescriptions for Urinary Tract Infections. West. J. Emerg. Med. 2020, 21, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Palagin, I.; Brunelli, R.; Cipelli, R.; Pellini, E.; Truzzi, J.C.; Van Bruwaene, S. Office-based approach to urinary tract infections in 50,000 patients: Results from the REWIND study. Int. J. Antimicrob. Agents 2020, 56, 105966. [Google Scholar] [CrossRef] [PubMed]
- Luepke, K.H.; Luepke, K.H.; Boucher, H.; Russo, R.L.; Bonney, M.W.; Hunt, T.D.; Mohr, J.F. Past, Present, and Future of Antibacterial Economics: Increasing Bacterial Resistance, Limited Antibiotic Pipeline, and Societal Implications. Pharmacotherapy 2017, 37, 71–84. [Google Scholar] [CrossRef]
- Theuretzbacher, U.; Bush, K.; Harbarth, S.; Paul, M.; Rex, J.H.; Tacconelli, E.; Thwaites, G.E. Critical analysis of antibacterial agents in clinical development. Nat. Rev. Microbiol. 2020, 18, 286–298. [Google Scholar] [CrossRef] [Green Version]
- Theuretzbacher, U.; Piddock, L.J.V. Non-traditional antibacterial therapeutic options and challenges. Cell Host Microbe 2019, 26, 61–72. [Google Scholar] [CrossRef]
- Tiwari, V.; Mishra, N.; Gadani, K.; Solanki, P.S.; Shah, N.A.; Tiwari, M. Mechanism of anti-bacterial activity of zinc oxide nanoparticle against Carbapenem-Resistant Acinetobacter baumannii. Front. Microbiol. 2018, 9, 1218. [Google Scholar] [CrossRef] [Green Version]
- Abdelhamid, A.G.; Esaam, A.; Hazaa, M.M. Cell free preparations of probiotics exerted antibacterial and antibiofilm activities against multidrug resistant E. coli. Saudi Pharm. J. 2018, 26, 603–607. [Google Scholar] [CrossRef]
- Iseppi, R.; Di Cerbo, A.; Aloisi, P.; Manelli, M.; Pellesi, V.; Provenzano, C.; Camellini, S.; Messi, P.; Sabia, C. In vitro activity of essential oils against planktonic and biofilm cells of extended-spectrum β-lactamase (ESBL)/carbapenamase-producing gram-negative bacteria involved in human nosocomial infections. Antibiotics 2020, 9, 272. [Google Scholar] [CrossRef]
- Sybesma, W.; Zbinden, R.; Chanishvili, N.; Kutateladze, M.; Chkhotua, A.; Ujmajuridze, A.; Mehnert, U.; Kessler, T.M. Bacteriophages as Potential Treatment for Urinary Tract Infections. Front. Microbiol. 2016, 7, 465. [Google Scholar] [CrossRef]
- Magyar, A.; Koves, B.; Nagy, K.; Dobák, A.; Arthanareeswaran, V.K.A.; Bálint, P.; Wagenlehner, F.; Tenke, P. Spectrum and antibiotic resistance of uropathogens between 2004 and 2015 in a tertiary care hospital in Hungary. J. Med. Microbiol. 2017, 66, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Toner, L.; Papa, N.; Aliyu, S.H.; Dev, H.; Lawrentschuk, N.; Al-Hayek, S. Extended-spectrum beta-lactamase-producing Enterobacteriaceae in hospital urinary tract infections: Incidence and antibiotic susceptibility profile over 9 years. World J. Urol. 2016, 34, 1031–1037. [Google Scholar] [CrossRef] [PubMed]
- Sbiti, M.; Lahmadi, K.; Louzi, L. Profil épidémiologique des entérobactéries uropathogènes productrices de bêta-lactamases à spectre élargi. Pan Afr. Med. J. 2017, 28, 29. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.H.; Jung, S.I.; Chung, H.S.; Yu, H.S.; Hwang, E.C.; Kim, S.-O.; Kang, T.W.; Kwon, D.D.; Park, K. Antimicrobial susceptibilities of extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae in health care-associated urinary tract infection: Focus on susceptibility to fosfomycin. Int. Urol. Nephrol. 2015, 47, 1059–1066. [Google Scholar] [CrossRef]
- Fajfr, M.; Louda, M.; Paterová, P.; Ryskova, L.; Pacovský, J.; Košina, J.; Žemličková, H.; Brodak, M. The susceptibility to fosfomycin of Gram-negative bacteria isolates from urinary tract infection in the Czech Republic: Data from a unicentric study. BMC Urol. 2017, 17, 33. [Google Scholar] [CrossRef]
- van der Donk, C.F.M.; Beisser, P.S.; Hoogkamp-Korstanje, J.A.A.; Bruggeman, C.A.; Stobberingh, E.E. A 12 year (1998–2009) antibiotic resistance surveillance of Klebsiella pneumoniae collected from intensive care and urology patients in 14 Dutch hospitals. J. Antimicrob. Chemother. 2011, 66, 855–858. [Google Scholar] [CrossRef]
- Gajdács, M.; Urbán, E. Comparative Epidemiology and Resistance Trends of Proteae in Urinary Tract Infections of Inpatients and Outpatients: A 10-Year Retrospective Study. Antibiotics 2019, 8, 91. [Google Scholar] [CrossRef] [Green Version]
- Lupo, A.; Haenni, M.; Madec, J.-Y. Antimicrobial Resistance in Acinetobacter spp. and Pseudomonas spp. Microbiol. Spectr. 2018, 6. [Google Scholar] [CrossRef]
- Tolker-Nielsen, T.I.M.; Brinch, U.C.; Ragas, P.C.; Andersen, J.B.O.; Jacobsen, C.S.; Molin, S. Development and Dynamics of Pseudomonas sp. Biofilms. J. Bacteriol. 2000, 182, 6482–6489. [Google Scholar] [CrossRef] [Green Version]
- EMEA. Disabling and Potentially Permanent Side Effects Lead to Suspension or Restrictions of Quinolone and Fluoroquinolone Antibiotics. Available online: https://www.ema.europa.eu/en/news/disabling-potentially-permanent-side-effects-lead-suspension-restrictions-quinolone-fluoroquinolone (accessed on 12 April 2020).
- Bonkat, G.; Wagenlehner, F. In the Line of Fire: Should Urologists Stop Prescribing Fluoroquinolones as Default ? Eur. Urol. 2019, 75, 205–207. [Google Scholar] [CrossRef]
- Toner, L.; Papa, N.; Aliyu, S.H.; Dev, H.; Lawrentschuk, N.; Al-Hayek, S. Vancomycin resistant enterococci in urine cultures: Antibiotic susceptibility trends over a decade at a tertiary hospital in the United Kingdom. Investig. Clin. Urol. 2016, 57, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Bonkat, G.; Bartoletti, R.; Bruyère, F.; Cai, T.; Geerlings, S.; Köves, B.; Schubert, S.; Wagenlehner, F. Urological Infections. 2020. Available online: https://uroweb.org/guideline/urological-infections/ (accessed on 17 September 2020).
- Wagenlehner, F.M.; Tandoğdu, Z.; Bartoletti, R.; Cai, T.; Cek, M.; Kulchavenya, E.V.; Koves, B.; Naber, K.; Perepanova, T.S.; Tenke, P.; et al. The global prevalence of infections in urology study: A long-term, worldwide surveillance study on urological infections. Pathogens 2016, 5, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Uropathogen | Antimicrobial Agent | |||||||
|---|---|---|---|---|---|---|---|---|
| Ampicillin | Amoxicillin/clavulanic acid | Piperacillin/tazobactam | ||||||
| n/N | n/N | n/N | ||||||
| E. coli | 641/1149 | 55.8% | 163/1138 | 14.3% | 50/358 | 14.0% | ||
| Klebsiella spp. | 522/522 | 100.0% | 191/492 | 38.8% | 129/245 | 52.7% | ||
| P. aeruginosa | NT | NT | 55/180 | 30.6% | ||||
| Proteus spp. | 138/241 | 57.3% | 30/239 | 12.6% | 1/113 | 0.9% | ||
| Enterococcus spp. | 80/756 | 10.6% | NT | NT | ||||
| Cefuroxime | Cefotaxime | Ceftazidime | Cefepime | |||||
| n/N | n/N | n/N | n/N | |||||
| E. coli | 143/1143 | 12.5% | 108/1135 | 9.5% | 100/1131 | 8.8% | 86/367 | 23.4% |
| Klebsiella spp. | 219/523 | 41.9% | 173/505 | 34.3% | 180/503 | 35.8% | 151/260 | 58.1% |
| P. aeruginosa | NT | NT | 47/252 | 18.7% | 56/178 | 31.5% | ||
| Proteus spp. | 38/242 | 15.7% | 14/240 | 5.8% | 7/240 | 2.9% | 8/109 | 7.3% |
| Enterococcus spp. | NT | NT | NT | NT | ||||
| Ciprofloxacin | Ofloxin | |||||||
| n/N | n/N | |||||||
| E. coli | 161/382 | 42.1% | 267/1015 | 26.3% | ||||
| Klebsiella spp. | 191/278 | 68.7% | 183/460 | 39.8% | ||||
| P. aeruginosa | 99/260 | 38.1% | 12/12 | 100.0% | ||||
| Proteus spp. | 55/113 | 48.7% | 107/210 | 51.0% | ||||
| Enterococcus spp. | NT | NT | ||||||
| Gentamicin | Amikacin | |||||||
| n/N | n/N | |||||||
| E. coli | 82/1149 | 7.1% | 5/381 | 1.3% | ||||
| Klebsiella spp. | 170/521 | 32.6% | 7/278 | 2.5% | ||||
| P. aeruginosa | 81/258 | 31.4% | 24/258 | 9.3% | ||||
| Proteus spp. | 70/242 | 28.9% | 0/112 | 0.0% | ||||
| Enterococcus spp. | NT | NT | ||||||
| Ertapenem | Meropenem | Imipenem | ||||||
| n/N | n/N | n/N | ||||||
| E. coli | 1/377 | 0.3% | 0/388 | 0.0% | 0/385 | 0.0% | ||
| Klebsiella spp. | 9/276 | 3.3% | 0/283 | 0.0% | 0/282 | 0.0% | ||
| P. aeruginosa | NT | 54/170 | 31.8% | 21/135 | 15.6% | |||
| Proteus spp. | 0/112 | 0.0% | 0/114 | 0.0% | 1/114 | 0.9% | ||
| Enterococcus spp. | NT | NT | NT | |||||
| Vancomycin | Colistin | Nitrofurantoin | Cotrimoxazole | |||||
| n/N | n/N | n/N | n/N | |||||
| E. coli | NT | 1/123 | 0.8% | 47/973 | 4.8% | 398/1150 | 34.6% | |
| Klebsiella spp. | NT | 2/100 | 2.0% | 144/313 | 46.0% | 248/522 | 47.5% | |
| P. aeruginosa | NT | 0/260 | 0.0% | NT | NT | |||
| Proteus spp. | NT | NT | 173/173 | 100.0% | 162/242 | 66.9% | ||
| Enterococcus spp. | 8/796 | 1.0% | NT | 34/711 | 4.8% | NT | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hrbacek, J.; Cermak, P.; Zachoval, R. Current Antibiotic Resistance Trends of Uropathogens in Central Europe: Survey from a Tertiary Hospital Urology Department 2011–2019. Antibiotics 2020, 9, 630. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090630
Hrbacek J, Cermak P, Zachoval R. Current Antibiotic Resistance Trends of Uropathogens in Central Europe: Survey from a Tertiary Hospital Urology Department 2011–2019. Antibiotics. 2020; 9(9):630. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090630
Chicago/Turabian StyleHrbacek, Jan, Pavel Cermak, and Roman Zachoval. 2020. "Current Antibiotic Resistance Trends of Uropathogens in Central Europe: Survey from a Tertiary Hospital Urology Department 2011–2019" Antibiotics 9, no. 9: 630. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090630